
Cytotoxic Influence of Khat (Catha edulis (Vahl) Forssk. ex Endl) on Oral Fibroblasts, Squamous Carcinoma Cells, and Expression of α Smooth Muscle Actin

 ,
,  ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Khat Preparation
2.2. Culture of NOFs and SCC4 Cells
2.2.1. Cell Lines and Culturing
2.2.2. Cell Growth Medium
2.2.3. Thawing and Seeding Cell Lines
2.2.4. Adherent Cell Sub-Culturing and Passaging
2.3. MTT Assay
2.3.1. Seeding Cells in 96 Well Plates
2.3.2. Khat Exposure
2.3.3. Determination of Cytotoxicity/Metabolic Activity
2.4. Effect of Khat on Fibroblast Phenotype
2.4.1. Immunostaining Preparation
2.4.2. Immunofluorescence for SMA
3. Results
3.1. MTT Assay
3.1.1. NOF 316
3.1.2. NOF 26
3.1.3. NOF 319
3.1.4. NOF 18
3.1.5. Cytotoxicity of Different NOF’s
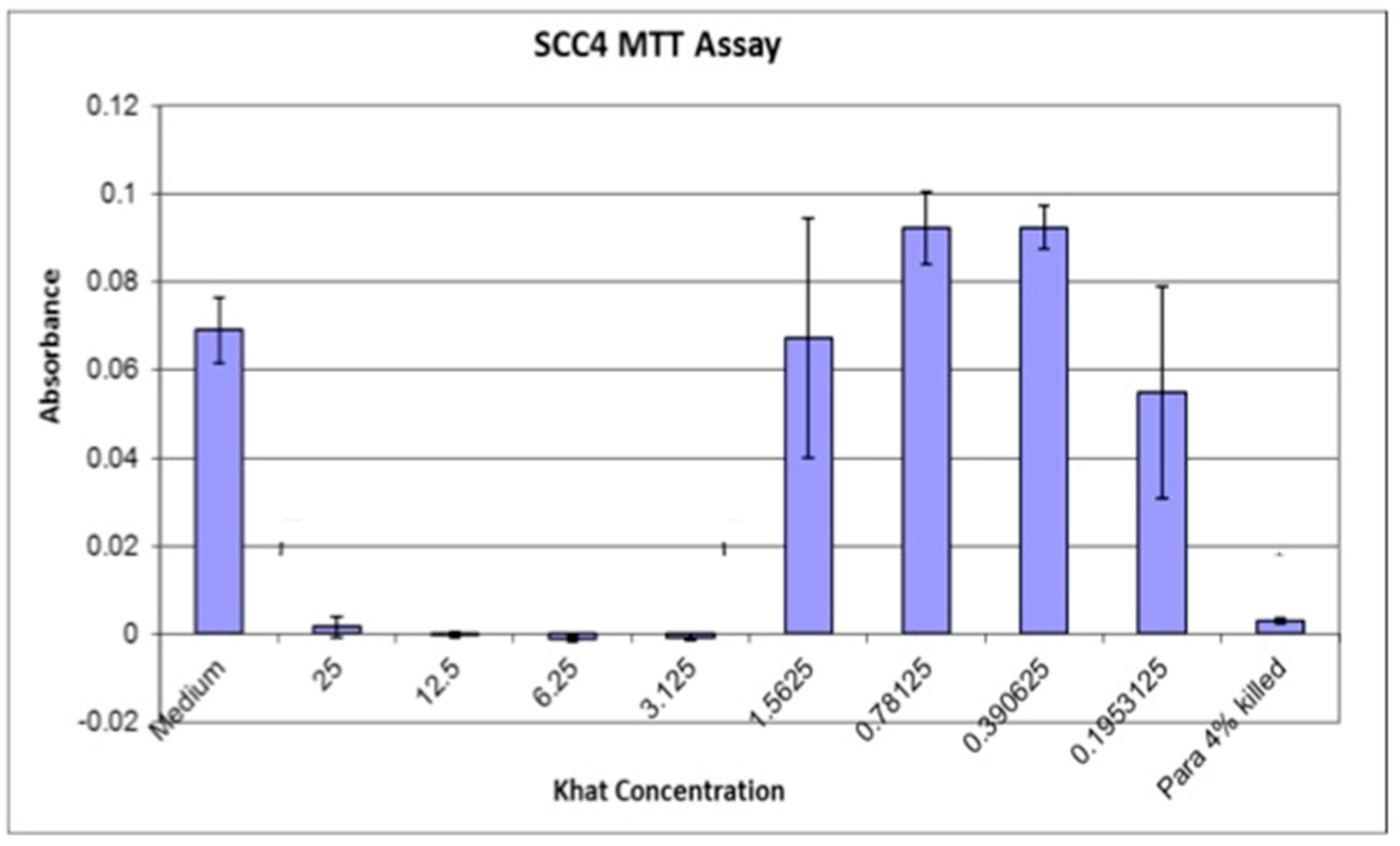
3.2. SCC4 Cells
SCC4 (Late Passage)
3.3. Comparison of NOF’s and SCC4 Assays
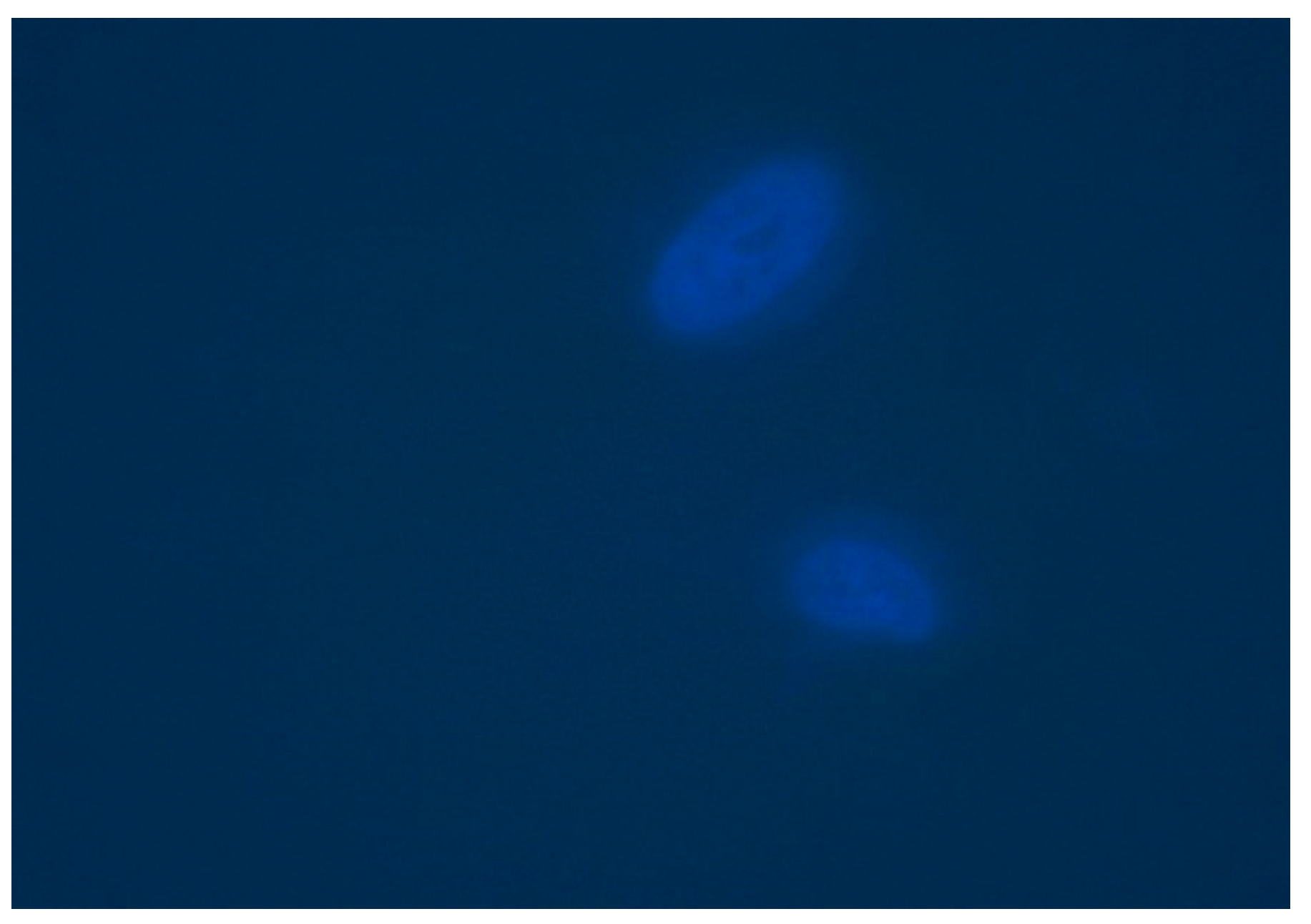
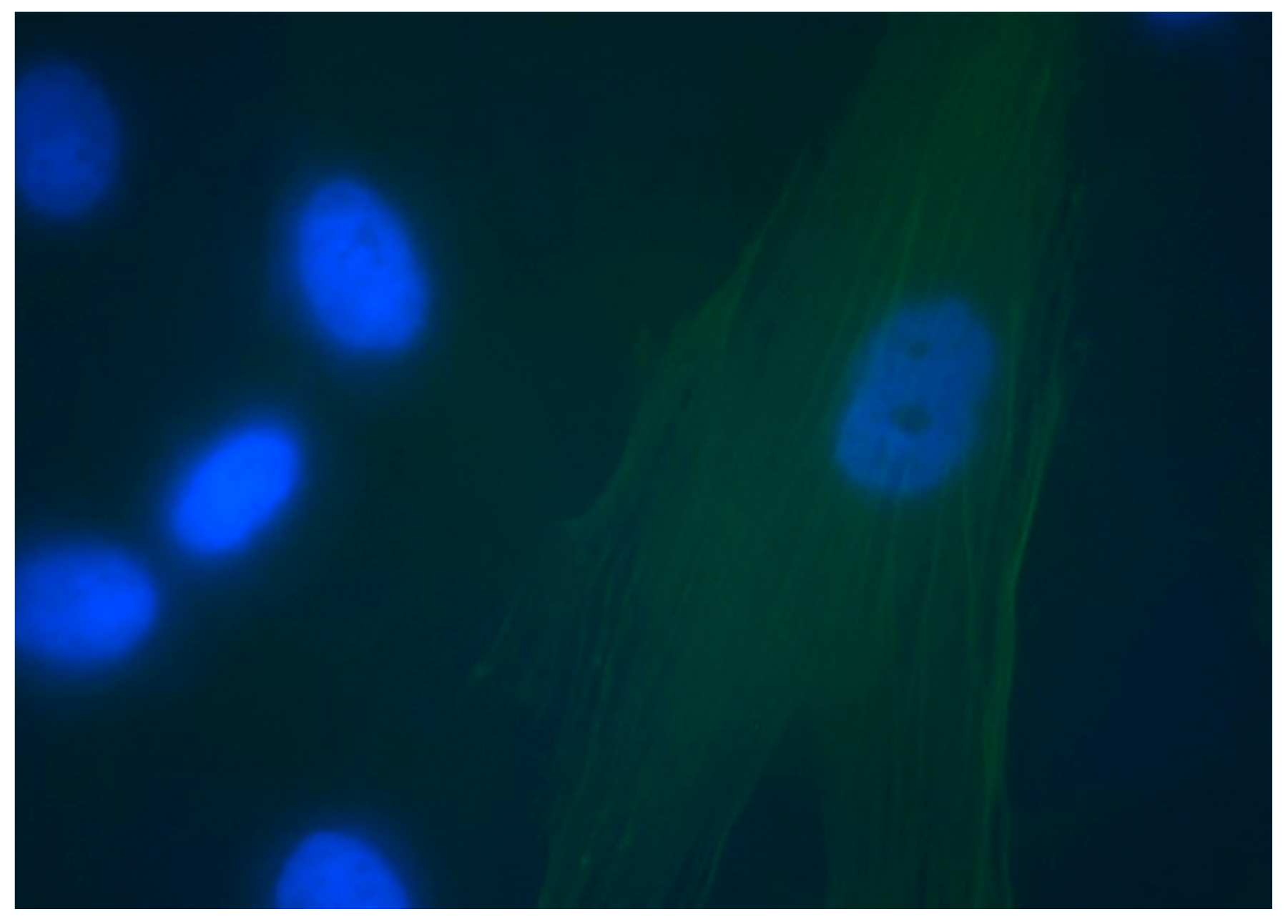
3.4. Detection of α-SMA
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials/Equipment | Company |
|---|---|
| Dulbecco’s Modified Eagles Medium, Cell culture medium | Gibco by Life technologies Invitrogen |
| PBS solution (without Ca2+ and Mg2+) | Sigma Aldrich |
| Trypsin/EDTA | Invitrogen |
| Acidified Isopropanol | Fisher Scientific, Leicestershire, UK |
| MTT, Thiazolyl Blue Tetrazolium Bromide | Sigma Aldrich |
| Galaxy R CO2 Incubator | Brunswick lab, (UK) |
| MSE Harrier 18/80 Refrigerated Centrifuge | MSE, UK |
| 25 cm2 and 75 cm2 tissue culture flasks (Cellstar®) | Greiner Bio-One Ltd. (Gloucestershire, UK) |
| 96 well tissue culture plates | Fisher Scientific UK Ltd. (Loughborough, UK) |
| Integra Biosciences PIPETBOYpro | Thermo Scientific, UK Ltd. |
| Disposable sterile pipettes (Costar®) | Corning Incorporated (USA) |
| Micropipettes | Thermo Scientific and Gilson lab (UK) |
| Labpette pipettes | Manufactured by Labnet (NJ, USA) |
| Pipette tips | STARLAB, Ltd. and Gilson. (UK) |
| Universal containers | SARSTEDT Ltd. (Leicester, UK) & Sterilin UK |
| Manual Desktop Counter | Ryman, UK |
| Cell counting chamber slides/Haemocytometer | Invitrogen |
| Zeiss Axiovert 200 M inverted microscope | Carl Zeiss Ltd. (Hertfordshire, UK) |
| Syringe and Its filter units | Millex®GP, Ireland |
| Eppendorf centrifuge tubes | Eppendorf, UK |
| 24 well tissue culture plates | Fisher Scientific UK Ltd. (Loughborough, UK) |
| Glass slides | Thermo, UK |
| Axioplan 2 Imagin software | Operated by University of Sheffield |
| Spectrophotometer plate reader, Infinite M200 | Tecan, UK |
| Magellan™ data analysis software | Tecan, UK |
| 100% Methanol | Provided by tissue culture lab, Dental School, University of Sheffield |
| Sodium deoxycholate | Provided by tissue culture lab, Dental School, University of Sheffield |
| Bovine Serum Albumin (BSA) | Sigma Aldrich, UK |
| Monoclonal Anti-Actin, α-Smooth Muscle - FITC antibody produced in mouse clone 1A4, purified immunoglobulin, buffered aqueous solution | C2 Sigma Aldrich, UK |
| DAPI nuclear stain | Life Technologies, Invitrogen |
| Monoclonal Anti-Human IgG1−FITC antibody produced in mouse | Sigma Aldrich, UK |
| TGF-β | Sigma Aldrich, UK |
References
- Gharat, S.A.; Momin, M.; Bhavsar, C. Oral Squamous Cell Carcinoma: Current Treatment Strategies and Nanotechnology-Based Approaches for Prevention and Therapy. Crit. Rev. Ther. Drug Carr. Syst. 2016, 33, 363–400. [Google Scholar] [CrossRef]
- Pires, F.R.; Ramos, A.B.; De Oliveira, J.B.C.; Tavares, A.S.; Da Luz, P.S.R.; Dos Santos, T.C.R.B. Oral squamous cell carcinoma: Clinicopathological features from 346 cases from a single Oral Pathology service during an 8-year period. J. Appl. Oral Sci. 2013, 21, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.-Q.; Liu, K.; Huo, Z.-J.; Li, X.-C.; Wang, M.; Liu, P.; Pang, B.; Wang, S.-J. A cell-targeted chemotherapeutic nanomedicine strategy for oral squamous cell carcinoma therapy. J. Nanobiotechnol. 2015, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Al-Maweri, S.A.; Warnakulasuriya, S.; Samran, A. Khat (Catha edulis) and its oral health effects: An updated review. J. Investig. Clin. Dent. 2018, 9, e12288. [Google Scholar] [CrossRef] [PubMed]
- Yarom, N.; Epstein, J.; Levi, H.; Porat, D.; Kaufman, E.; Gorsky, M. Oral manifestations of habitual khat chewing: A case-control study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, e60–e66. [Google Scholar] [CrossRef]
- Abdelwahab, S.I.; Alsanosy, R.; Taha, M.M.E.; Mohan, S. Khat Induced Toxicity: Role on Its Modulating Effects on Inflammation and Oxidative Stability. BioMed Res. Int. 2018, 2018, 1–7. [Google Scholar] [CrossRef]
- Lukandu, O.M.; Bredholt, T.; Neppelberg, E.; Gjertsen, B.T.; Johannessen, A.C.; Vintermyr, O.K.; Costea, D.E. Early loss of mitochondrial inner transmembrane potential in khat-induced cell death of primary normal human oral cells. Toxicology 2009, 263, 108–116. [Google Scholar] [CrossRef]
- Al-Ahdal, M.N.; McGarry, T.J.; Hannan, M.A. Cytotoxicity of Khat (Catha edulis) extract on cultured mammalian cells: Effects on macromolecule biosynthesis. Mutat. Res. Toxicol. 1988, 204, 317–322. [Google Scholar] [CrossRef]
- Al-Akwa, A.A.; Shaher, M.; Al-Akwa, S.; Aleryani, S.L. Free radicals are present in human serum of Catha edulis Forsk (Khat) abusers. J. Ethnopharmacol. 2009, 125, 471–473. [Google Scholar] [CrossRef]
- Dimba, E.A.; Gjertsen, B.T.; Bredholt, T.; Fossan, K.O.; Costea, D.E.; Francis, G.W.; Johannessen, A.C.; Vintermyr, O.K. Khat (Catha edulis)-induced apoptosis is inhibited by antagonists of caspase-1 and -8 in human leukaemia cells. Br. J. Cancer 2004, 91, 1726–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, E.D.; Thompson, E.W. Epithelial mesenchymal plasticity in carcinoma metastasis. Clin. Exper. Metastasis 2015, 32, 188. [Google Scholar] [CrossRef]
- Daly, A.J.; McIlreavey, L.; Irwin, C.R. Regulation of HGF and SDF-1 expression by oral fibroblasts—Implications for invasion of oral cancer. Oral Oncol. 2008, 44, 646–651. [Google Scholar] [CrossRef]
- Lee, C.H.; Shah, B.; Moioli, E.K.; Mao, J.J. CTGF directs fibroblast differentiation from human mesenchymal stem/stromal cells and defines connective tissue healing in a rodent injury model. J. Clin. Investig. 2010, 120, 3340–3349. [Google Scholar] [CrossRef] [Green Version]
- Grotendorst, G.R.; Rahmanie, H.; Duncan, M.R. Combinatorial signaling pathways determine fibroblast proliferation and myofibroblast differentiation. FASEB J. 2004, 18, 469–479. [Google Scholar] [CrossRef] [Green Version]
- Karagiannis, G.S.; Poutahidis, T.; Erdman, S.E.; Kirsch, R.; Riddell, R.H.; Diamandis, E.P. Cancer-Associated Fibroblasts Drive the Progression of Metastasis through both Paracrine and Mechanical Pressure on Cancer Tissue. Mol. Cancer Res. MCR 2012, 10, 1403–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aziz, K.H.; Peh, Y.T.-O. Research & Clinical Practice, Undefined 2011, Herbal Delivery System for Treatment of Obesity Administration of Encapsulated Khat-Extracts on Body Weight of Rats, Elsevier. (n.d.). Available online: https://www.sciencedirect.com/science/article/pii/S1871403X11000159?casa_token=uYkaq5-2G3kAAAAA:UuoMUGEn2084syGHl66wrIy191u1_XAyt76GNQCYWbFuwfmic63JFuCumGXiU75wgLyxLBUJk2g (accessed on 1 February 2021).
- Macedo, A.L.; da Silva, D.P.; Moreira, D.L.; de Queiroz, L.N.; Vasconcelos, T.R.; Araujo, G.F.; Kaplan, M.A.C.; Pereira, S.S.; de Almeida, E.C.; Valverde, A.L.; et al. Cytotoxicity and selectiveness of Brazilian Piper species towards oral carcinoma cells. Biomed. Pharmacother. 2019, 110, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Paul, B.D.; Cole, K.A. Cathinone (Khat) and Methcathinone (CAT)in Urine Specimens: A Gas Chromatographic-Mass Spec-trometric Detection Procedure*. 2001. Available online: https://academic.oup.com/jat/article/25/7/525/729486 (accessed on 27 January 2021).
- Alsanosy, R.; Alhazmi, H.A.; Sultana, S.; Abdalla, A.N.; Ibrahim, Y.; Al Bratty, M.; Banji, D.; Khardali, I.; Khalid, A. Phytochemical Screening and Cytotoxic Properties of Ethanolic Extract of Young and Mature Khat Leaves. J. Chem. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Lukandu, O.M.; Costea, D.E.; Neppelberg, E.; Johannessen, A.C.; Vintermyr, O.K. Khat (Catha edulis) Induces Reactive Oxygen Species and Apoptosis in Normal Human Oral Keratinocytes and Fibroblasts. Toxicol. Sci. 2008, 103, 311–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atlabachew, M.; Chandravanshi, B.; Redi-Abshiro, M.; Torto, N.; Chigome, S.; Pule, B. Evaluation of the effect of various drying techniques on the composition of the psychoactive phenylpropylamino alkaloids of khat (Catha edulis Forsk) chewing leaves. Bull. Chem. Soc. Ethiop. 2013, 27, 347–358. [Google Scholar] [CrossRef]
- Al-Habori, M. The potential adverse effects of habitual use of Catha edulis (khat). Expert Opin. Drug Saf. 2005, 4, 1145–1154. [Google Scholar] [CrossRef]
- Abderrahman, S.M.; Modallal, N. Genotoxic Effects of Catha edulis (Khat) Extract on Mice Bone Marrow Cells. Jordan J. Biol. Sci. 2008, 1, 165–172. [Google Scholar]
- Lukandu, O.; Neppelberg, E.; Vintermyr, O.; Johannessen, A.; Costea, D. Khat Alters the Phenotype of in vitro-reconstructed Human Oral Mucosa. J. Dent. Res. 2009, 89, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Nyongesa, A.W.; Oduma, J.A.; Nakajima, M.; Odongo, H.O.; Adoyo, P.A.; Al’Absi, M. Dose-response inhibitory effects of purified cathinone from khat (Catha edulis) on cortisol and prolactin release in vervet monkeys (Chlorocebus aethiops). Metab. Brain Dis. 2013, 29, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Hinz, B.; Dugina, V.; Ballestrem, C.; Wehrle-Haller, B.; Chaponnier, C. α-smooth muscle actin is crucial for focal adhesion mat-uration in myofibroblasts. Mol. Biol. Cell 2003, 14, 2508–2519. [Google Scholar] [CrossRef] [Green Version]
- Biela, S.A.; Su, Y.; Spatz, J.P.; Kemkemer, R. Different sensitivity of human endothelial cells, smooth muscle cells and fibroblasts to topography in the nano–micro range. Acta Biomater. 2009, 5, 2460–2466. [Google Scholar] [CrossRef] [PubMed]
- Giannoni, E.; Bianchini, F.; Masieri, L.; Serni, S.; Torre, E.; Calorini, L.; Chiarugi, P. Reciprocal activation of prostate cancer cells and cancer-associated fibroblasts stimulates epithelial-mesenchymal transition and cancer stemness. Cancer Res. 2010, 70, 6945–6956. [Google Scholar] [CrossRef] [Green Version]
- Gold, L.I. The role for transforming growth factor-β (TGF-β) in human cancer. Crit. Rev. Oncog. 1999, 10, 303–360. Available online: https://europepmc.org/article/med/10654929 (accessed on 27 January 2021).
- Cunningham, J.L.; Tsolakis, A.V.; Jacobson, A.; Janson, E.T. Connective tissue growth factor expression in endocrine tumors is associated with high stromal expression of α-smooth muscle actin. Eur. J. Endocrinol. 2010, 163, 691–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etemad-Moghadam, S.; Khalili, M.; Tirgary, F.; Alaeddini, M. Evaluation of myofibroblasts in oral epithelial dysplasia and squamous cell carcinoma. J. Oral Pathol. Med. 2009, 38, 639–643. [Google Scholar] [CrossRef]
- Alan, H.; Ağaçayak, S.; Kavak, G.; Özcan, A. Verrucous carcinoma and squamous cell papilloma of the oral cavity: Report of two cases and review of literature. Eur. J. Dent. 2015, 9, 453–456. [Google Scholar] [CrossRef] [Green Version]
- Nasr, A.H.; Khatri, M.L. Head and neck squamous cell carcinoma in Hajjah, Yemen. Saudi Med. J. 2000, 21, 565–568. [Google Scholar] [PubMed]
- Cicciù, M.; Cervino, G.; Fiorillo, L.; D’Amico, C.; Oteri, G.; Troiano, G.; Zhurakivska, K.; Muzio, L.L.; Herford, A.S.; Crimi, S.; et al. Early Diagnosis on Oral and Potentially Oral Malignant Lesions: A Systematic Review on the VELscope® Fluorescence Method. Dent. J. 2019, 7, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]











| Cell Line | Type | Origin |
|---|---|---|
| NOF 18 | Primary cells | Normal Oral Fibroblasts |
| NOF 26 | Primary cells | Normal Oral Fibroblasts |
| NOF 316 | Primary cells | Normal Oral Fibroblasts |
| NOF 319 | Primary cells | Normal Oral Fibroblasts |
| SCC4 | Cell line | Squamous Cell Carcinoma |
| Composition | Volume | Remarks |
|---|---|---|
| Dulbecco’s Modified Eagles Medium (DMEM) supplemented by 4500 mg/L glucose, GlutaMAX™ I and Sodium Pyruvate | 450 mL | Invitrogen, UK lot- 1250148 lot- 1122288 lot- 1369047 |
| 10% Fetal Bovine Serum (FBS) | 50 mL | Biosera, East Sussex, UK |
| Pen/Strep (Antibiotics) | 5 mL 100 IU/mL Penicillin, 100 µg/mL Streptomycin | Sigma Aldrich, Dorset, UK |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syed, A.U.Y.; Ahmed, M.A.; AlSagob, E.I.; Al-Askar, M.; AlMubarak, A.M.; Jouhar, R.; Ahmed, A.R.; Mokeem, S.A.; Aldahiyan, N.; Vohra, F.; et al. Cytotoxic Influence of Khat (Catha edulis (Vahl) Forssk. ex Endl) on Oral Fibroblasts, Squamous Carcinoma Cells, and Expression of α Smooth Muscle Actin. Appl. Sci. 2021, 11, 3524. https://doi.org/10.3390/app11083524
Syed AUY, Ahmed MA, AlSagob EI, Al-Askar M, AlMubarak AM, Jouhar R, Ahmed AR, Mokeem SA, Aldahiyan N, Vohra F, et al. Cytotoxic Influence of Khat (Catha edulis (Vahl) Forssk. ex Endl) on Oral Fibroblasts, Squamous Carcinoma Cells, and Expression of α Smooth Muscle Actin. Applied Sciences. 2021; 11(8):3524. https://doi.org/10.3390/app11083524
Chicago/Turabian StyleSyed, Azeem Ul Yaqin, Muhammad A. Ahmed, Eman I. AlSagob, Mansour Al-Askar, Abdulrahman M. AlMubarak, Rizwan Jouhar, Abdul R. Ahmed, Sameer A. Mokeem, Nada Aldahiyan, Fahim Vohra, and et al. 2021. "Cytotoxic Influence of Khat (Catha edulis (Vahl) Forssk. ex Endl) on Oral Fibroblasts, Squamous Carcinoma Cells, and Expression of α Smooth Muscle Actin" Applied Sciences 11, no. 8: 3524. https://doi.org/10.3390/app11083524
APA StyleSyed, A. U. Y., Ahmed, M. A., AlSagob, E. I., Al-Askar, M., AlMubarak, A. M., Jouhar, R., Ahmed, A. R., Mokeem, S. A., Aldahiyan, N., Vohra, F., & Abduljabbar, T. (2021). Cytotoxic Influence of Khat (Catha edulis (Vahl) Forssk. ex Endl) on Oral Fibroblasts, Squamous Carcinoma Cells, and Expression of α Smooth Muscle Actin. Applied Sciences, 11(8), 3524. https://doi.org/10.3390/app11083524