
Design and Evaluation of Large-Scale IoT-Enabled Healthcare Architecture



Abstract
:1. Introduction
- the proposal of IoT-enabled healthcare architecture,
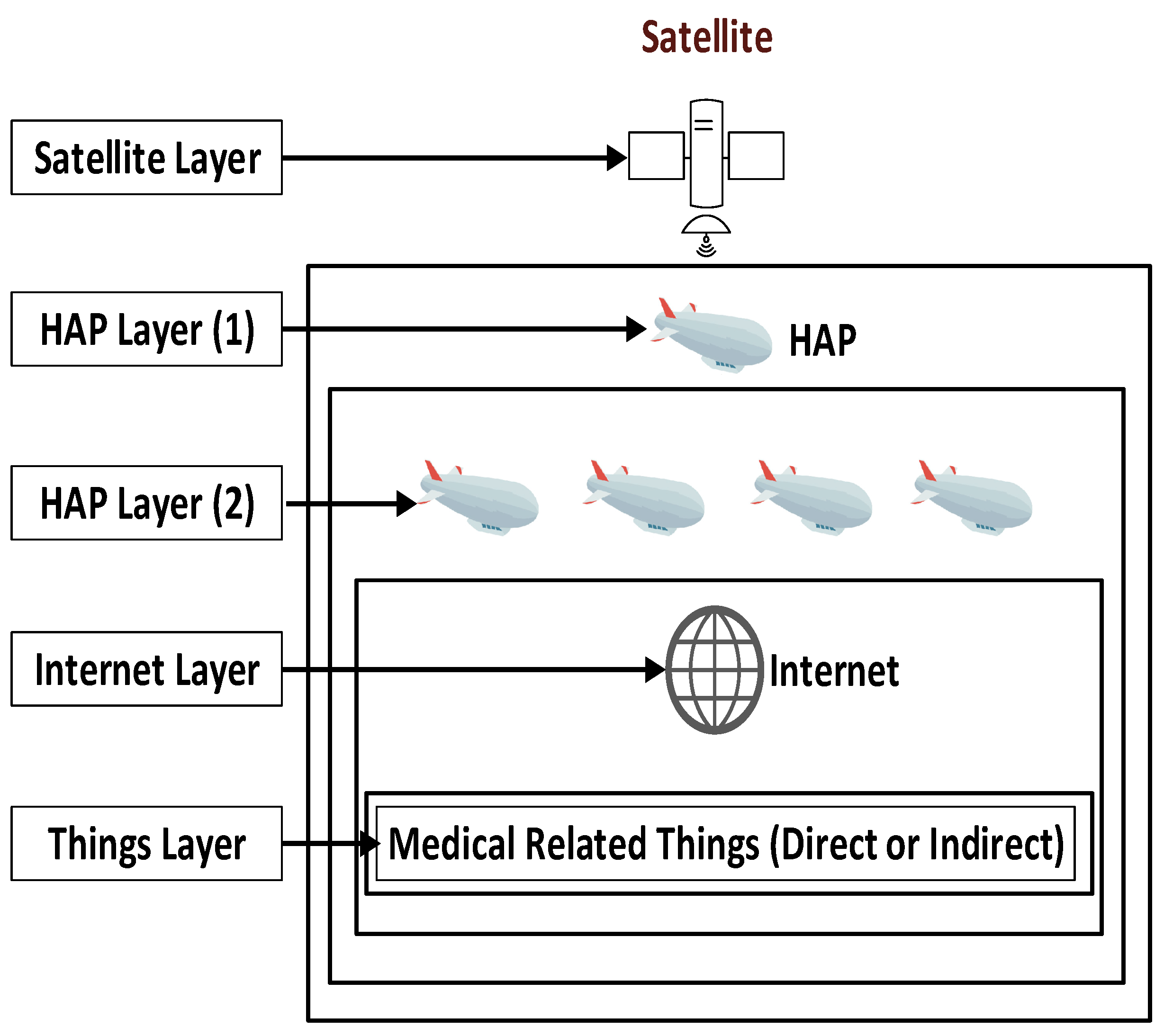
- applying a large-scale coverage scheme to guarantee communication between healthcare devices,
- usage of clustering and prioritization methodologies in the proposed IoT-enabled healthcare architecture,
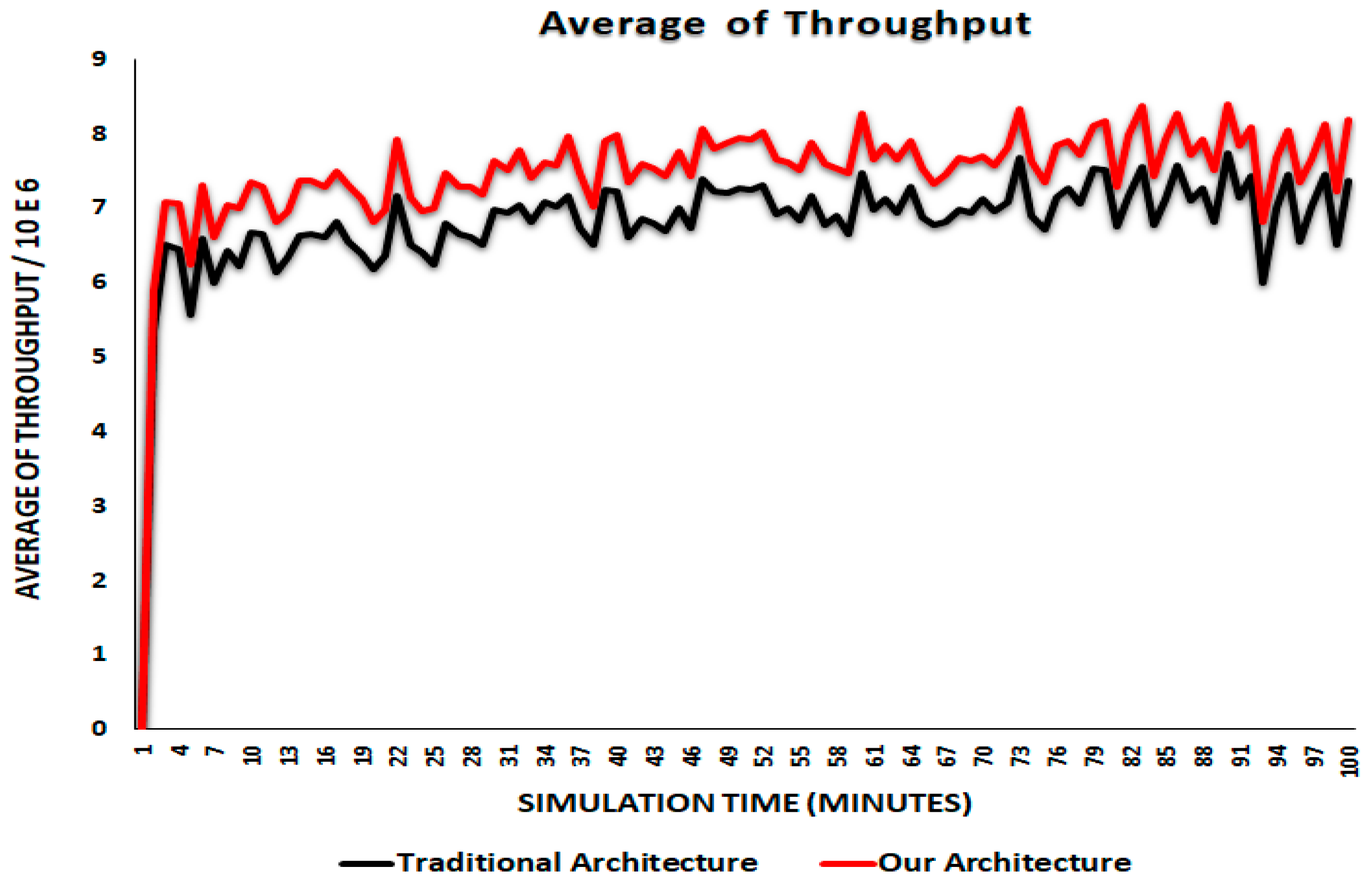
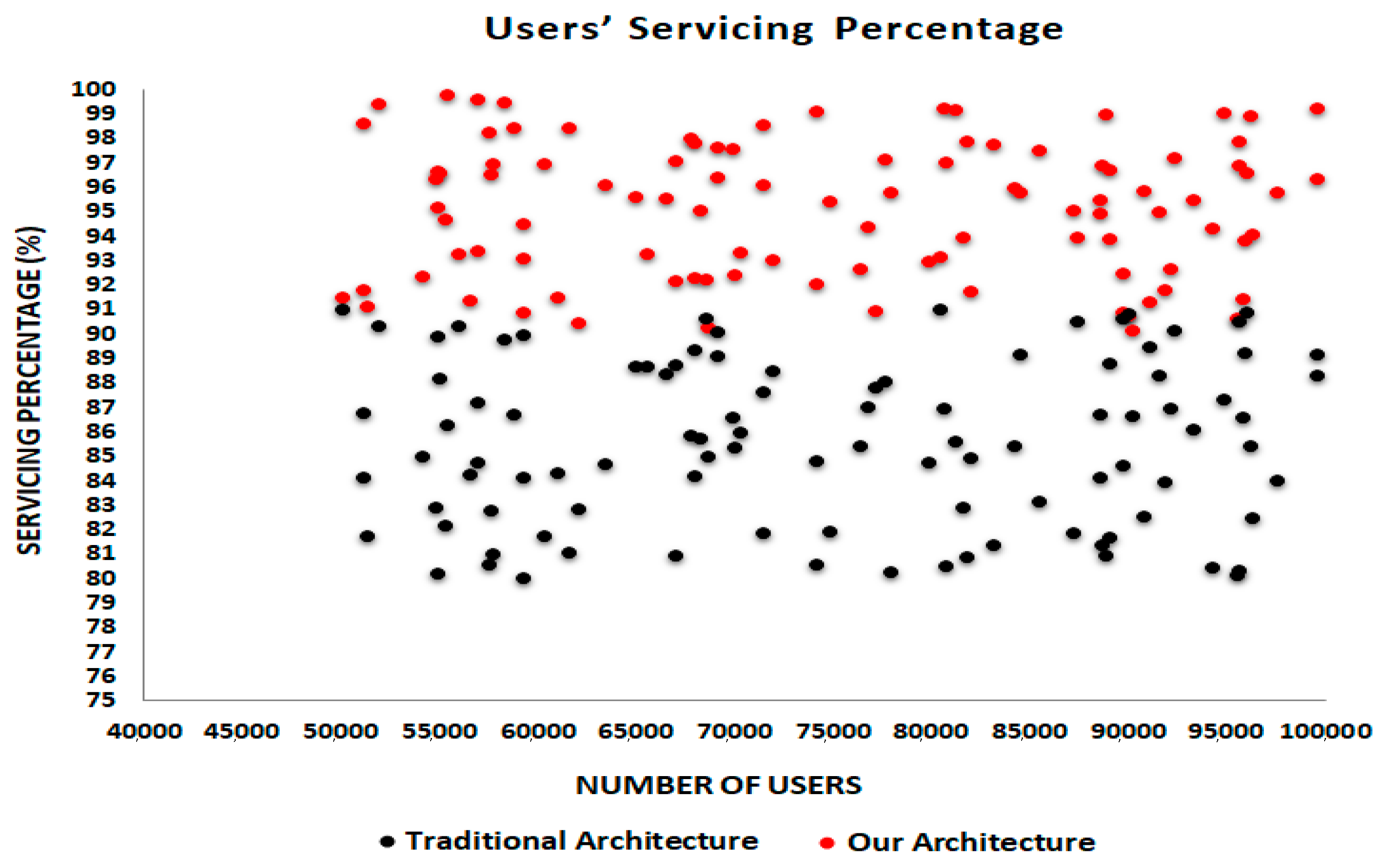
- a simulated environment to measure the performance of the proposed IoT-enabled healthcare architecture, and
- discussion of the simulation results and recommendations.
2. Related Work
3. Proposed IoT-Enabled Healthcare Architecture
3.1. Communicator
3.2. Manager
- Manage its cluster(s).
- Monitor the activities of each thing in its cluster(s).
- Update its cluster by deletion/addition of old/new thing(s).
- Predict the future events in its cluster(s).
- Control the message exchange process in its cluster(s).
- Gather information about the things in its cluster periodically.
- Send summarized report about its cluster to UM.
- Communicate with neighbor HMs.
- Select a computing center to process a specific data inside its cluster region.
- Manage the entire domain of the proposed IoT-based healthcare environment.
- Select additional HMs for a specific cluster (If required).
- Achieve the load balancing issue between clusters.
- Achieve the fault tolerance issue inside clusters.
- Achieve the communication between clusters’ HMs.
- Evaluate the clusters in the healthcare environment periodically.
- Exchange between the messages’ transmission strategies.
- Select a computing center to process a specific data outside a cluster region.
3.3. Prioritizer
3.4. How the Proposed Healthcare Architecture Works
3.5. Mathematical Analysis
3.6. Simple Use Case
4. Simulation Infrastructure
5. Results and Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roy, S.; Chowdhury, C. Remote health monitoring protocols for IoT-enabled healthcare infrastructure. In Healthcare Paradigms in the Internet of Things Ecosystem, 1st ed.; Balas, V., Pal, S., Eds.; Academic Press: Amsterdam, The Netherlands, 2021; pp. 163–188. [Google Scholar]
- Javaid, M.; Khan, I.H. Internet of Things (IoT) enabled healthcare helps to take the challenges of COVID-19 Pandemic. J. Oral Biol. Craniofacial Res. 2021, 11, 209–214. [Google Scholar] [CrossRef]
- Albahri, A.; Alwan, J.K.; Taha, Z.K.; Ismail, S.F.; Hamid, R.A.; Zaidan, A.; Zaidan, B.; Alamoodi, A.; Alsalem, M. IoT-based telemedicine for disease prevention and health promotion: State-of-the-Art. J. Netw. Comput. Appl. 2021, 173, 102873. [Google Scholar] [CrossRef]
- Yang, X.; Wang, X.; Li, X.; Gu, D.; Liang, C.; Li, K.; Zhang, G.; Zhong, J. Exploring emerging IoT technologies in smart health research: A knowledge graph analysis. BMC Med Inform. Decis. Mak. 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Wu, X.; Huang, W.; Wu, X.; Wang, S. Internet of things in health management systems: A review. Int. J. Commun. Syst. 2020, 34. [Google Scholar] [CrossRef]
- Alam, M.M.; Malik, H.; Khan, M.I.; Pardy, T.; Kuusik, A.; Le Moullec, Y. A Survey on the Roles of Communication Technologies in IoT-Based Personalized Healthcare Applications. IEEE Access 2018, 6, 36611–36631. [Google Scholar] [CrossRef]
- Paszkiel, S. Using BCI in IoT Implementation. In Studies in Computational Intelligence; Springer: Berlin/Heidelberg, Germany, 2020; Volume 852, pp. 111–128. [Google Scholar]
- Ilyas, M.; Saad, P.; Ahmad, M. A survey of analysis and classification of EEG signals for brain-computer interfaces. In Proceedings of the 2nd International Conference on Biomedical Engineering (ICoBE), Penang, Malaysia, 30–31 March 2015; pp. 1–6. [Google Scholar]
- Zhang, X.; Yao, L.; Zhang, S.; Kanhere, S.; Sheng, M.; Liu, Y. Internet of Things Meets Brain–Computer Interface: A Unified Deep Learning Framework for Enabling Human-Thing Cognitive Interactivity. IEEE Internet Things J. 2018, 6, 2084–2092. [Google Scholar] [CrossRef] [Green Version]
- Haghi, M.; Neubert, S.; Geissler, A.; Fleischer, H.; Stoll, N.; Stoll, R.; Thurow, K. A Flexible and Pervasive IoT-Based Healthcare Platform for Physiological and Environmental Parameters Monitoring. IEEE Internet Things J. 2020, 7, 5628–5647. [Google Scholar] [CrossRef]
- Kumar, A.; Krishnamurthi, R.; Nayyar, A.; Sharma, K.; Grover, V.; Hossain, E. A Novel Smart Healthcare Design, Simulation, and Implementation Using Healthcare 4.0 Processes. IEEE Access 2020, 8, 118433–118471. [Google Scholar] [CrossRef]
- Min, M.; Wan, X.; Xiao, L.; Chen, Y.; Xia, M.; Wu, D.; Dai, H. Learning-Based Privacy-Aware Offloading for Healthcare IoT With Energy Harvesting. IEEE Internet Things J. 2018, 6, 4307–4316. [Google Scholar] [CrossRef]
- Chanak, P.; Banerjee, I. Congestion Free Routing Mechanism for IoT-Enabled Wireless Sensor Networks for Smart Healthcare Applications. IEEE Trans. Consum. Electron. 2020, 66, 223–232. [Google Scholar] [CrossRef]
- Aujla, G.; Jindal, A. A Decoupled Blockchain Approach for Edge-Envisioned IoT-Based Healthcare Monitoring. IEEE J. Sel. Areas Commun. 2020, 39, 491–499. [Google Scholar] [CrossRef]
- Wu, T.; Wu, F.; Qiu, C.; Redoute, J.-M.; Yuce, M.R. A Rigid-Flex Wearable Health Monitoring Sensor Patch for IoT-Connected Healthcare Applications. IEEE Internet Things J. 2020, 7, 6932–6945. [Google Scholar] [CrossRef]
- Bharathi, R.; Abirami, T.; Dhanasekaran, S.; Gupta, D.; Khanna, A.; Elhoseny, M.; Shankar, K. Energy efficient clustering with disease diagnosis model for IoT based sustainable healthcare systems. Sustain. Comput. Inform. Syst. 2020, 28, 100453. [Google Scholar] [CrossRef]
- Akkaş, M.A.; Sokullu, R.; Çetin, H.E. Healthcare and patient monitoring using IoT. Internet Things 2020, 11, 100173. [Google Scholar] [CrossRef]
- Ni, J.-C.; Yang, C.-S.; Huang, J.-K.; Shiu, L.C. Combining Non-Invasive Wearable Device and Intelligent Terminal in HealthCare IoT. Procedia Comput. Sci. 2019, 154, 161–166. [Google Scholar] [CrossRef]
- Anand, L.V.; Kotha, M.K.; Kannan, N.S.; Kumar, S.; Meera, M.; Shawl, R.Q.; Ray, A.P. Design and development of IoT based health monitoring system for military applications. Mater. Today Proc. 2020. [Google Scholar] [CrossRef]
- Kadhim, K.T.; Alsahlany, A.M.; Wadi, S.M.; Kadhum, H.T. An Overview of Patient’s Health Status Monitoring System Based on Internet of Things (IoT). Wirel. Pers. Commun. 2020, 114, 2235–2262. [Google Scholar] [CrossRef]
- Misra, D.; Das, G.; Das, D. An IoT based building health monitoring system supported by cloud. J. Reliab. Intell. Environ. 2020, 6, 141–152. [Google Scholar] [CrossRef]
- Campioni, F.; Choudhury, S.; Al-Turjman, F. Scheduling RFID networks in the IoT and smart health era. J. Ambient. Intell. Humaniz. Comput. 2019, 10, 4043–4057. [Google Scholar] [CrossRef]
- Usak, M.; Kubiatko, M.; Shabbir, M.S.; Dudnik, O.V.; Jermsittiparsert, K.; Rajabion, L. Health care service delivery based on the Internet of things: A systematic and comprehensive study. Int. J. Commun. Syst. 2020, 33, e4179. [Google Scholar] [CrossRef]
- Kumar, P.; Silambarasan, K. Enhancing the Performance of Healthcare Service in IoT and Cloud Using Optimized Techniques. IETE J. Res. 2019, 1–10. [Google Scholar] [CrossRef]
- Jeyaraj, P.R.; Nadar, E.R.S. Smart-Monitor: Patient Monitoring System for IoT-Based Healthcare System Using Deep Learning. IETE J. Res. 2019, 1–8. [Google Scholar] [CrossRef]
- Asghari, P.; Rahmani, A.M.; Javadi, H.H.S. A medical monitoring scheme and health-medical service composition model in cloud-based IoT platform. Trans. Emerg. Telecommun. Technol. 2019, 30. [Google Scholar] [CrossRef]
- Chui, K.T.; Liu, R.W.; Lytras, M.D.; Zhao, M. Big data and IoT solution for patient behaviour monitoring. Behav. Inf. Technol. 2019, 38, 940–949. [Google Scholar] [CrossRef]
- Kavitha, D.; Ravikumar, S. IOT and context-aware learning-based optimal neural network model for real-time health monitoring. Trans. Emerg. Telecommun. Technol. 2021, 32. [Google Scholar] [CrossRef]
- Said, O.; Tolba, A. Performance Evaluation of a Dual Coverage System for Internet of Things Environments. Mob. Inf. Syst. 2016, 2016, 1–20. [Google Scholar] [CrossRef]
- Kumari, P. RFID technology in health-IoT. In Healthcare Paradigms in the Internet of Things Ecosystem; Balas, V., Pal, S., Eds.; Academic Press: Amsterdam, The Netherlands, 2021; pp. 223–250. [Google Scholar]
- Paniagua, C.; Eliasson, J.; Delsing, J. Efficient Device-to-Device Service Invocation Using Arrowhead Orchestration. IEEE Internet Things J. 2019, 7, 429–439. [Google Scholar] [CrossRef]
- Bello, O.; Zeadally, S. Intelligent Device-to-Device Communication in the Internet of Things. IEEE Syst. J. 2016, 10, 1172–1182. [Google Scholar] [CrossRef]
- Said, O.; Tolba, A. Design and performance evaluation of mixed multicast architecture for internet of things environment. J. Supercomput. 2018, 74, 3295–3328. [Google Scholar] [CrossRef]
- Said, O.; Tolba, A. DORS: A data overhead reduction scheme for hybrid networks in smart cities. Int. J. Commun. Syst. 2020, 33, e4435. [Google Scholar] [CrossRef]
- Said, O.; Al-Makhadmeh, Z.; Tolba, A. EMS: An Energy Management Scheme for Green IoT Environments. IEEE Access 2020, 8, 44983–44998. [Google Scholar] [CrossRef]
- El Kafhali, S.; Salah, K. Performance modelling and analysis of Internet of Things enabled healthcare monitoring systems. IET Netw. 2019, 8, 48–58. [Google Scholar] [CrossRef]
- Wang, C.; Zhu, X.; Hong, J.C.; Zheng, D. Artificial Intelligence in Radiotherapy Treatment Planning: Present and Future. Technol. Cancer Res. Treat. 2019, 18. [Google Scholar] [CrossRef] [PubMed]
- Said, O. Analysis, design and simulation of Internet of Things routing algorithm based on ant colony optimization. Int. J. Commun. Syst. 2016, 30, e3174. [Google Scholar] [CrossRef]
- Said, O.; Albagory, Y.; Nofal, M.; Al Raddady, F. IoT-RTP and IoT-RTCP: Adaptive Protocols for Multimedia Transmission over Internet of Things Environments. IEEE Access 2017, 5, 16757–16773. [Google Scholar] [CrossRef]
- Said, O.; Tolba, A. A Reliable and Scalable Internet of Military Things Architecture. Comput. Mater. Contin. 2021, 67, 3887–3906. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group # | Type | Description |
|---|---|---|
| First | Guidance | Used by UM to determine HM status (active/sleep/off). |
| Stop | Used to break the connection between HM and its cluster. | |
| Inform | Used to send regular information to managers. | |
| Second | Status | Used to describe the clusters status. |
| Threshold | Used when an element of the healthcare system reaches one of its indicators (power or processing unit) threshold. | |
| Sudden | Used in case of an unexpected event occurrence. | |
| Prediction | Used when HM has some signs of a future event. | |
| Third | Update | Used to update the cluster status. |
| Fourth | New messages | Used to inform the device that new function(s) is required. |
| Fifth | Aggregate | Used to gather information about devices in HM’s cluster. |
| Tool | Mission | Network | Coverage | ||
|---|---|---|---|---|---|
| Medical Sensors | Monitoring | WSN | Internet | HAP | Satellite |
| RFID | Tracking | RFID | |||
| Mobile | Connection | Cellular | |||
| Health Software | Decisions | AI | |||
| Specialist Temporary Cooperation | Discussion | MANET | |||
| Parameter | Value |
|---|---|
| Number of patients | 50,000 |
| Number of organizations | 20 |
| Number of users | 100,000 |
| Number of active devices | 200,000 |
| Number of passive devices | 300,000 |
| Distance between organizations | Random range (200–1000 km) |
| Number of wearable devices | 30,000 |
| Number of body sensors | 15,000 |
| Number of mobiles with medical applications | 10,000 |
| Number of HAPs | 5 |
| Number of satellites | 1 |
| Distance between users | Random in range (10–1000 km) |
| Distance between patients | Random in range (10–100 km) |
| Computing centers | Cloud and fog |
| Data types | Text, image, and multimedia |
| Transmission channels | Full duplex |
| Types of sensors | Heterogeneous |
| Number of medical devices | 1000 (distributed) |
| Number of monitoring devices | 20,000 |
| Number of importance queues | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, O.; Tolba, A. Design and Evaluation of Large-Scale IoT-Enabled Healthcare Architecture. Appl. Sci. 2021, 11, 3623. https://doi.org/10.3390/app11083623
Said O, Tolba A. Design and Evaluation of Large-Scale IoT-Enabled Healthcare Architecture. Applied Sciences. 2021; 11(8):3623. https://doi.org/10.3390/app11083623
Chicago/Turabian StyleSaid, Omar, and Amr Tolba. 2021. "Design and Evaluation of Large-Scale IoT-Enabled Healthcare Architecture" Applied Sciences 11, no. 8: 3623. https://doi.org/10.3390/app11083623
APA StyleSaid, O., & Tolba, A. (2021). Design and Evaluation of Large-Scale IoT-Enabled Healthcare Architecture. Applied Sciences, 11(8), 3623. https://doi.org/10.3390/app11083623