
Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review




Abstract
:1. Introduction
2. Methods
2.1. Context
2.2. Type of Studies
2.3. Concept
2.4. Search Strategy
2.5. Databases
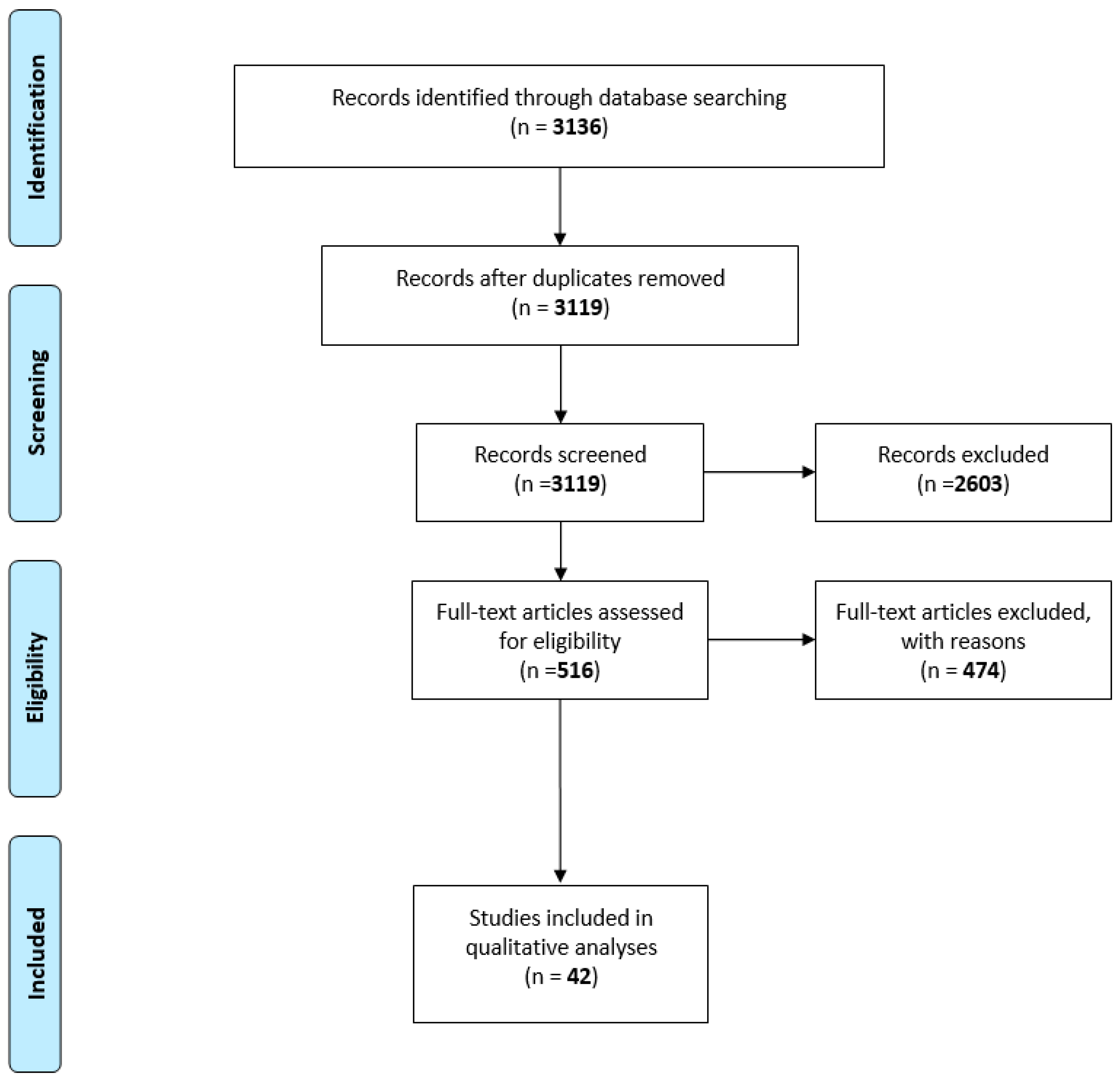
3. Results
3.1. Technology to Support Hand Rehabilitation
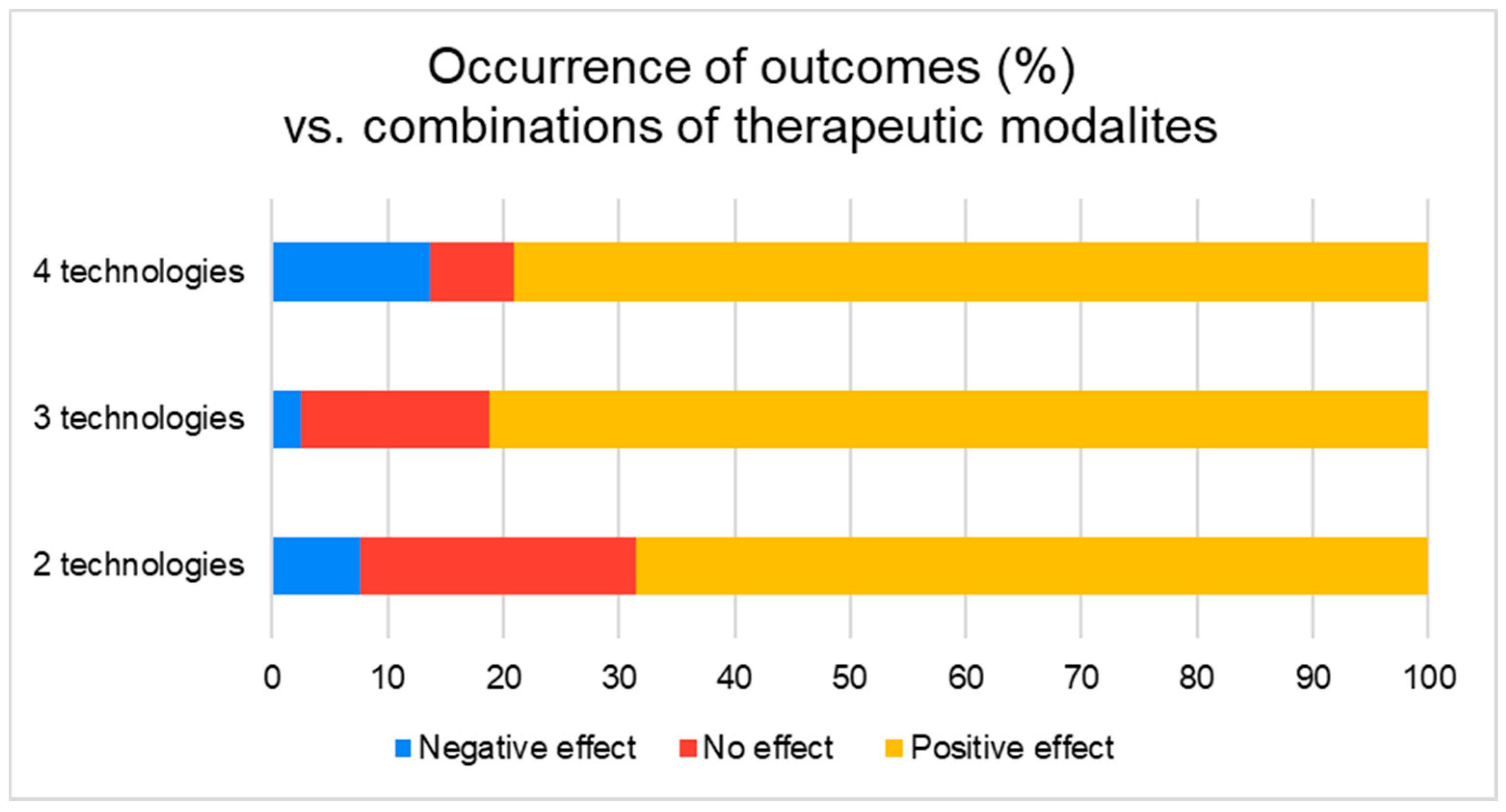
3.2. Outcomes
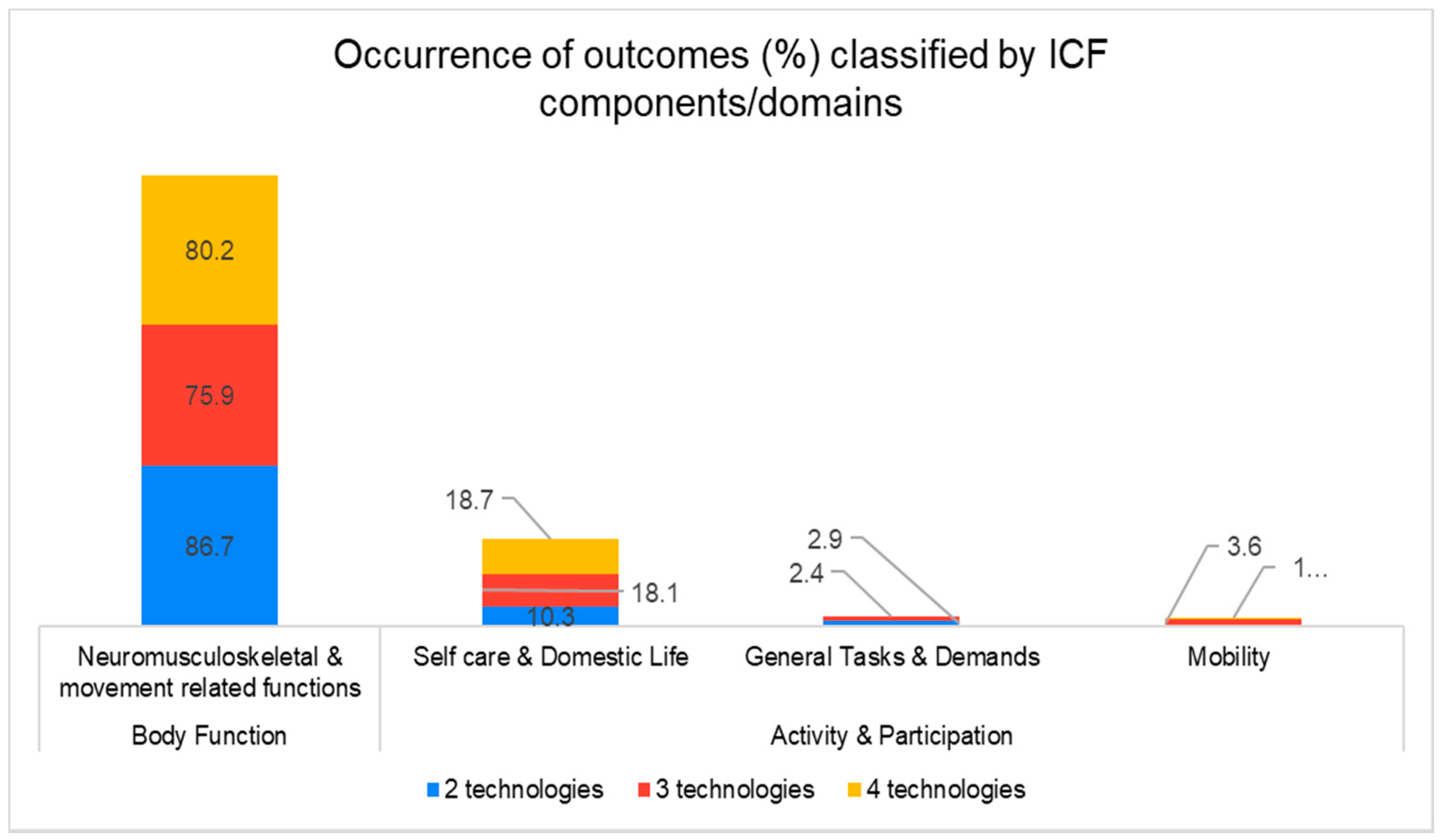
3.3. Outcome Classification
3.4. User’s Perspective
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
- Robotics/
- Exoskeleton device/
- Man-Machine Systems/
- Orthotic Devices/
- Self-Help Devices/
- Automation/
- Therapy, Computer-Assisted/
- (electromechanical or “electro mechanical” or mechanical or mechanised or mechanized or driven or “assistive device*”).tw,kw.
- (robot* or automat* or “computer aided” or “computer assisted” or “power assist*”).tw,kw.
- (orthos* or orthotic*).tw,kw.
- or/1–10 [Robotic Concept]
- Computer Simulation/
- software/
- Mobile Applications/
- Video Games/
- Computers/
- exp Microcomputers/
- exp Cell Phones/
- Games, Experimental/
- (“virtual realit*” or VR).tw,kw.
- simulat*.tw,kw.
- ((interactiv* or virtual) adj2 technolog*).tw,kw.
- “augmented realit*”.tw,kw.
- (smartphone* or “smart-phone*”).tw,kw.
- ((mobile or cell or smart) adj2 phone*).tw,kw.
- (iphone* or android* or ipad*).tw,kw.
- (“personal digital assistant*” or “handheld computer*” or “handheld device*”).tw,kw.
- (“mobile app” or “mobile application”).tw,kw.
- (“serious game*” or “serious gaming”).tw,kw.
- or/12–29 [Virtual Reality Concept]
- Wearable Electronic Devices/
- Touch/
- exp Touch Perception/
- haptic*.tw,kw.
- biofeedback.tw,kw.
- (tactile or tactual).tw,kw.
- ((force or tactile or touch) adj2 (feedback or perception)).tw,kw.
- “sensory substitution”.tw,kw.
- (“electro-tactile” or “electro tactile” or electrotactile).tw,kw.
- (“electro-vibration” or “electro vibration” or electrovibration).tw,kw.
- ((vibrat* or servo or stepper) adj2 (motor or motors)).tw,kw.
- “wire actuator*”.tw,kw.
- piezoelectric*.tw,kw.
- pneumatic*.tw,kw.
- “shape memory alloy*”.tw,kw.
- solenoid*.tw,kw.
- “electro-active polymer*”.tw,kw.
- electrode*.tw,kw.
- (vibrotactile or vibration).tw,kw.
- wearable*.tw,kw.
- or/31–50 [Haptic Concept]
- (technolog* adj2 assist*).tw,kw.
- or/11,30,51–52 [Technological assistance concept]
- Hand/
- wrist/
- (hand* or wrist* or finger* or thumb*).tw,kw.
- or/54–56 [Hand Concept]
- exp cerebrovascular disorders/ or brain injury, chronic/
- (stroke* or cva or poststroke or “post stroke”).tw,kw.
- (cerebrovasc* or cerebral vascular).tw,kw.
- (cerebral or cerebellar or brain* or vertebrobasilar).tw,kw.
- (infarct* or isch?emi* or thrombo$ or emboli* or apoplexy).tw,kw.
- and/61–62
- (cerebral or brain or subarachnoid).tw,kw.
- (haemorrhage or hemorrhage or haematoma or hematoma or bleed*).tw,kw.
- and/64–65
- hemiplegia/ or exp paresis/
- (hempar* or hemipleg* or brain injur*).tw,kw.
- or/58–60,63,66–68 [Stroke Concept]
- and/53,57,69
- (rehabilitat* or rehab or “occupational therap*” or physiotherap* or “physical therap*”).tw,kw.
- exp Physical Therapy Modalities/
- exp Occupational Therapy/
- or/71–73 [Rehabilitation Concept]
- 70 and 74
References
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Krueger, H.; Koot, J.; Hall, R.E.; O’Callaghan, C.; Bayley, M.; Corbett, D. Prevalence of Individuals Experiencing the Effects of Stroke in Canada: Trends and Projections. Stroke 2015, 46, 2226–2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatem, S.M.; Saussez, G.; Della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, S.-M.; Studenski, S.; Duncan, P.W.; Perera, S. Persisting Consequences of Stroke Measured by the Stroke Impact Scale. Stroke 2002, 33, 1840–1844. [Google Scholar] [CrossRef] [Green Version]
- Parker, V.M.; Wade, D.T.; Hewer, R.L. Loss of arm function after stroke: Measurement, frequency, and recovery. Int. Rehabil. Med. 1986, 8, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.T.; Langton-Hewer, R.; Wood, V.A.; Skilbeck, C.E.; Ismail, H.M. The hemiplegic arm after stroke: Measurement and recovery. J. Neurol. Neurosurg. Psychiatry 1983, 46, 521–524. [Google Scholar] [CrossRef] [Green Version]
- LeWinn, E.B. Physiological Factors in Childhood Epilepsy. Epilepsia 1980, 21, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Rugnetta, M. “Neuroplasticity”. Encyclopedia Britannica. 3 September 2020. Available online: https://www.britannica.com/science/neuroplasticity (accessed on 16 April 2021).
- Kwakkel, G. Impact of intensity of practice after stroke: Issues for consideration. Disabil. Rehabil. 2006, 28, 823–830. [Google Scholar] [CrossRef]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Nichols-Larsen, D. EXCITE Investigators. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: The EXCITE randomized clinical trial. JAMA 2006, 296, 2095–2104. [Google Scholar] [CrossRef]
- Bear-Lehman, J.; Bassile, C.C.; Gillen, G. A Comparison of Time Use on an Acute Rehabilitation Unit: Subjects with and without a Stroke. Phys. Occup. Ther. Geriatr. 2001, 20, 17–27. [Google Scholar] [CrossRef]
- Bernhardt, J.; Dewey, H.; Thrift, A.; Donnan, G. Inactive and alone: Physical activity within the first 14 days of acute stroke unit care. Stroke 2004, 35, 1005–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, E.M.; Nelson, D.L.; Bush, M.A. Comparison of Performance in Materials-Based Occupation, Imagery-Based Occupation, and Rote Exercise in Nursing Home Residents. Am. J. Occup. Ther. 1992, 46, 607–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thielman, G.; Kaminski, T.; Gentile, A.M. Rehabilitation of Reaching After Stroke: Comparing 2 Training Protocols Utilizing Trunk Restraint. Neurorehabilit. Neural Repair 2008, 22, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Thielman, G.T.; Dean, C.M.; Gentile, A. Rehabilitation of reaching after stroke: Task-related training versus progressive resistive exercise. Arch. Phys. Med. Rehabil. 2004, 85, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Ada, L.; Canning, C.G.; Carr, J.H.; Kilbreath, S.L.; Shepherd, R.B. Task-Specific Training of Reaching and Manipulation. In Advances in Psychology; Bennett, K.M.B., Castiello, U., Eds.; Elsevier: North-Holland, The Netherlands, 1994; Volume 105, pp. 239–265. [Google Scholar]
- Michaelsen, S.M.; Dannenbaum, R.; Levin, M.F. Task-specific training with trunk restraint on arm recovery in stroke: Randomized control trial. Stroke 2006, 37, 186–192. [Google Scholar] [CrossRef] [Green Version]
- Bütefisch, C.; Hummelsheim, H.; Denzler, P.; Mauritz, K.-H. Repetitive training of isolated movements improves the outcome of motor rehabilitation of the centrally paretic hand. J. Neurol. Sci. 1995, 130, 59–68. [Google Scholar] [CrossRef]
- Logigian, M.K.; Samuels, M.A.; Falconer, J.; Zagar, R. Clinical exercise trial for stroke patients. Arch. Phys. Med. Rehabil. 1983, 64, 364–367. [Google Scholar]
- Wagenaar, R.C.; Meijer, O.G.; Van Wieringen, P.C.; Kuik, D.J.; Hazenberg, G.J.; Lindeboom, J.; Wichers, F.; Rijswijk, H. The functional recovery of stroke: A comparison between neuro-developmental treatment and the Brunnstrom method. Scand. J. Rehabil. Med. 1990, 22, 1–8. [Google Scholar] [PubMed]
- Wolf, S.L.; Lecraw, D.E.; Barton, L.A. Comparison of Motor Copy and Targeted Biofeedback Training Techniques for Restitution of Upper Extremity Function among Patients with Neurologic Disorders. Phys. Ther. 1989, 69, 719–735. [Google Scholar] [CrossRef]
- Guillot, A.; Collet, C. Construction of the Motor Imagery Integrative Model in Sport: A review and theoretical investigation of motor imagery use. Int. Rev. Sport. Exerc. Psychol. 2008, 1, 31–44. [Google Scholar] [CrossRef]
- Watt, A.P.; Morris, T.; Andersen, M.B. Development and validation of the sport imagery ability measure. Vic. Univ. Technol. 2003, 28, 149–180. [Google Scholar]
- Nilsen, D.M.; Gillen, G.; Gordon, A.M. Use of mental practice to improve upper-limb recovery after stroke: A systematic review. Am. J. Occup. Ther. 2010, 64, 695–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brokaw, E.B.; Murray, T.M.; Nef, T.; Lum, P.S.; Nichols, D.; Holley, R.J. Time Independent Functional Task Training: A case study on the effect of inter-joint coordination driven haptic guidance in stroke therapy. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011. [Google Scholar] [CrossRef]
- Squeri, V.; Masia, L.; Giannoni, P.; Sandini, G.; Morasso, P. Wrist rehabilitation in chronic stroke patients by means of adaptive, progressive robot-aided therapy. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, A.A.; Lemmens, R.J.; Monfrance, M.; Geers, R.P.; Bakx, W.; Smeets, R.J.; Seelen, H.A. Effects of task-oriented robot training on arm function, activity, and quality of life in chronic stroke patients: A randomized controlled trial. J. Neuroeng. Rehabil. 2014, 11, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, H.A.; Tarry, C.; Lambert, C.; Barreca, S.; Allen, B.O. Results of Clinicians Using a Therapeutic Robotic System in an Inpatient Stroke Rehabilitation Unit. J. Neuroeng. Rehabil. 2011, 8, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.-C.; Liao, Y.-C.; Cheng, Y.-H.; Shih, P.-C.; Tsai, C.-M.; Lin, C.-Y. The potential effect of a vibrotactile glove rehabilitation system on motor recovery in chronic post-stroke hemiparesis. Technol. Health Care 2017, 25, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Mukherjee, M.; Tsaur, Y.; Kim, S.; Liu, H.; Natarajan, P.; Agah, A. Development and feasibility study of a sensory-enhanced robot-aided motor training in stroke rehabilitation. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 5965–5968. [Google Scholar] [CrossRef]
- Mokienko, O.A.; Lyukmanov, R.K.; Chernikova, L.A.; Suponeva, N.A.; Piradov, M.A.; Frolov, A.A. Brain–computer interface: The first experience of clinical use in Russia. Hum. Physiol. 2016, 42, 24–31. [Google Scholar] [CrossRef]
- Connelly, L.; Stoykov, M.E.; Jia, Y.; Toro, M.L.; Kenyon, R.V.; Kamper, D.G. Use of a pneumatic glove for hand rehabilitation following stroke. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 2434–2437. [Google Scholar] [CrossRef]
- Deutsch, J.E.; Merians, A.S.; Burdea, G.C.; Boian, R.; Adamovich, S.V.; Poizner, H. Haptics and Virtual Reality Used to Increase Strength and Improve Function in Chronic Individuals Post-stroke: Two Case Reports. J. Neurol. Phys. Ther. 2002, 26, 79–86. [Google Scholar] [CrossRef]
- Tsoupikova, D.; Stoykov, N.S.; Corrigan, M.; Thielbar, K.; Vick, R.; Li, Y.; Triandafilou, K.; Preuss, F.; Kamper, D. Virtual immersion for post-stroke hand rehabilitation therapy. Ann. Biomed. Eng. 2015, 43, 467–477. [Google Scholar] [CrossRef]
- Deutsch, J.E.; Merians, A.S.; Adamovich, S.; Poizner, H.; Burdea, G.C. Development and application of virtual reality technology to improve hand use and gait of individuals post-stroke. Restor. Neurol. Neurosci. 2004, 22, 371–386. [Google Scholar]
- Reinkensmeyer, D.; Pang, C.; Nessler, J.; Painter, C. Web-based telerehabilitation for the upper extremity after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Acosta, A.M.; Dewald, H.A.; Dewald, J.P.A. Pilot study to test effectiveness of video game on reaching performance in stroke. J. Rehabil. Res. Dev. 2011, 48, 431–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merians, A.S.; Poizner, H.; Boian, R.; Burdea, G.; Adamovich, S. Sensorimotor training in a virtual reality environment: Does it improve functional recovery poststroke? Neurorehabil. Neural. Repair. 2006, 20, 252–267. [Google Scholar] [CrossRef]
- Jiang, L.; Cutkosky, M.; Ruutiainen, J.; Raisamo, R. Using Haptic Feedback to Improve Grasp Force Control in Multiple Sclerosis Patients. IEEE Trans. Robot. 2009, 25, 593–601. [Google Scholar] [CrossRef]
- Wan, A.H.; Wong, D.W.; Ma, C.Z.; Zhang, M.; Lee, W.C. Wearable Vibrotactile Biofeedback Device Allowing Identification of Different Floor Conditions for Lower-Limb Amputees. Arch. Phys. Med. Rehabil. 2016, 97, 1210–1213. [Google Scholar] [CrossRef] [Green Version]
- Stone, K.D.; Gonzalez, C.L.R. The contributions of vision and haptics to reaching and grasping. Front. Psychol. 2015, 6, 1403. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ Res. Method Rep. 2009, 339, 2700. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Amirabdollahian, F.; Livatino, S.; Vahedi, B.; Gudipati, R.; Sheen, P.; Gawrie-Mohan, S.; Vasdev, N. Prevalence of haptic feedback in robot-mediated surgery: A systematic review of literature. J. Robot. Surg. 2017, 12, 11–25. [Google Scholar] [CrossRef] [Green Version]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, CD006185. [Google Scholar] [CrossRef]
- Saxena, N.; Kyaw, B.M.; Vseteckova, J.; Dev, P.; Paul, P.; Lim, K.T.K.; Kononowicz, A.A.; Masiello, I.; Car, L.T.; Nikolaou, C.K.; et al. Virtual reality environments for health professional education. Cochrane Database Syst. Rev. 2018, 2018, CD012090. [Google Scholar] [CrossRef]
- Williams, M.A.; Srikesavan, C.; Heine, P.J.; Bruce, J.; Brosseau, L.; Hoxey-Thomas, N.; Lamb, S.E. Exercise for rheumatoid arthritis of the hand. Cochrane Database Syst. Rev. 2018, CD003832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampson, M.; McGowan, J.; Cogo, E.; Grimshaw, J.; Moher, D.; Lefebvre, C. An evidence-based practice guideline for the peer review of electronic search strategies. J. Clin. Epidemiol. 2009, 62, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Boian, R.; Sharma, A.; Han, C.; Merians, A.; Burdea, G.; Adamovich, S.; Recce, M.; Tremaine, M.; Poizner, H. Virtual reality-based post-stroke hand rehabilitation. Stud. Health Technol. Inform. 2002, 85, 64–70. [Google Scholar]
- Broeren, J.; Claesson, L.; Goude, D.; Rydmark, M.; Sunnerhagen, K.S. Virtual Rehabilitation in an Activity Centre for Community-Dwelling Persons with Stroke. Cerebrovasc. Dis. 2008, 26, 289–296. [Google Scholar] [CrossRef]
- Yeh, S.-C.; Lee, S.-H.; Chan, R.-C.; Chen, S.; Rizzo, A. A virtual reality system integrated with robot-assisted haptics to simulate pinch-grip task: Motor ingredients for the assessment in chronic stroke. Neurorehabilitation 2014, 35, 435–449. [Google Scholar] [CrossRef]
- Turolla, A.; Albasini, O.A.D.; Oboe, R.; Agostini, M.; Tonin, P.; Paolucci, S.; Sandrini, G.; Venneri, A.; Piron, L. Haptic-Based Neurorehabilitation in Poststroke Patients: A Feasibility Prospective Multicentre Trial for Robotics Hand Rehabilitation. Comput. Math. Methods Med. 2013, 2013, 895492. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.-C.; Lee, S.-H.; Chan, R.-C.; Wu, Y.; Zheng, L.-R.; Flynn, S. The Efficacy of a Haptic-Enhanced Virtual Reality System for Precision Grasp Acquisition in Stroke Rehabilitation. J. Health Eng. 2017, 2017, 9840273. [Google Scholar] [CrossRef] [Green Version]
- Adamovich, S.; Fluet, G.G.; Merians, A.S.; Mathai, A.; Qiu, Q. Recovery of hand function in virtual reality: Training hemiparetic hand and arm together or separately. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 3475–3478. [Google Scholar] [CrossRef]
- Abdollahi, F.; Case Lazarro, E.D.; Listenberger, M.; Kenyon, R.V.; Kovic, M.; Bogey, R.A.; Hedeker, D.; Jovanovic, B.D.; Patton, J.L. Error augmentation enhancing arm recovery in individuals with chronic stroke: A randomized crossover design. Neurorehabil. Neural. Repair. 2014, 28, 120–128. [Google Scholar] [CrossRef]
- Adamovich, S.V.; Fluet, G.G.; Mathai, A.; Qiu, Q.; Lewis, J.; Merians, A.S. Design of a complex virtual reality simulation to train finger motion for persons with hemiparesis: A proof of concept study. J. Neuroeng. Rehabil. 2009, 6, 28. [Google Scholar] [CrossRef] [Green Version]
- Adamovich, S.V.; Fluet, G.G.; Merians, A.S.; Mathai, A.; Qiu, Q. Incorporating Haptic Effects Into Three-Dimensional Virtual Environments to Train the Hemiparetic Upper Extremity. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 512–520. [Google Scholar] [CrossRef] [Green Version]
- Fluet, G.G.; Merians, A.S.; Qiu, Q.; Davidow, A.; Adamovich, S.V. Comparing integrated training of the hand and arm with isolated training of the same effectors in persons with stroke using haptically rendered virtual environments, a randomized clinical trial. J. Neuroeng. Rehabil. 2014, 11, 126. [Google Scholar] [CrossRef] [Green Version]
- Fluet, G.G.; Merians, A.S.; Qiu, Q.; Lafond, I.; Saleh, S.; Ruano, V.; Delmonico, A.R.; Adamovich, S.V. Robots integrated with virtual reality simulations for customized motor training in a person with upper extremity hemiparesis: A case study. J. Neurol. Phys. Ther. 2012, 36, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fluet, G.; Merians, A.; Patel, J.; Wingerden, A.V.; Qiu, Q.; Yarossi, M.; Tunik, E.; Adamovich, S.; Massood, S. Virtual reality-augmented rehabilitation for patients in subacute phase post stroke: A feasibility study. J. Pain. Manag. 2016, 9, 227–234. [Google Scholar]
- Jack, D.; Boian, R.; Merians, A.; Tremaine, M.; Burdea, G.; Adamovich, S.; Recce, M.; Poizner, H. Virtual reality-enhanced stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, R.C.V.; Harwin, W.S.; Lamperd, R.; Collin, C. Evaluation of Reach and Grasp Robot-Assisted Therapy Suggests Similar Functional Recovery Patterns on Proximal and Distal Arm Segments in Sub-Acute Hemiplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Maris, A.; Coninx, K.; Seelen, H.; Truyens, V.; De Weyer, T.; Geers, R.; Lemmens, M.; Coolen, J.; Stupar, S.; Lamers, I.; et al. The impact of robot-mediated adaptive I-TRAVLE training on impaired upper limb function in chronic stroke and multiple sclerosis. Disabil. Rehabil. Assist. Technol. 2018, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Q.; Fluet, G.G.; Lafond, I.; Merians, A.S.; Adamovich, S.V. Coordination changes demonstrated by subjects with hemiparesis performing hand-arm training using the NJIT-RAVR robotically assisted virtual rehabilitation system. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 1143–1146. [Google Scholar] [CrossRef] [Green Version]
- Rozario, S.V.; Housman, S.; Kovic, M.; Kenyon, R.V.; Patton, J.L. Therapist-mediated post-stroke rehabilitation using haptic/graphic error augmentation. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 1151–1156. [Google Scholar] [CrossRef]
- Rowe, J.B.; Chan, V.; Ingemanson, M.L.; Cramer, S.C.; Wolbrecht, E.T.; Reinkensmeyer, D.J. Robotic Assistance for Training Finger Movement Using a Hebbian Model: A Randomized Controlled Trial. Neurorehabilit. Neural Repair 2017, 31, 769–780. [Google Scholar] [CrossRef]
- Adamovich, S.; Merians, A.; Boian, R.; Tremaine, M.; Burdea, G.; Recce, M.; Poizner, H. A virtual reality based exercise system for hand rehabilitation post-stroke: Transfer to function. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; pp. 4936–4939. [Google Scholar] [CrossRef]
- Broeren, J.; Rydmark, M.; Sunnerhagen, K.S. Virtual reality and haptics as a training device for movement rehabilitation after stroke: A single-case study. Arch. Phys. Med. Rehabil. 2004, 85, 1247–1250. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.C.; Yeh, S.-C.; Jung, Y.; Yoon, H.; Whitford, M.; Chen, S.-Y.; Li, L.; McLaughlin, M.; Rizzo, A.; Winstein, C.J. Intervention to enhance skilled arm and hand movements after stroke: A feasibility study using a new virtual reality system. J. Neuroeng. Rehabil. 2007, 4, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broeren, J.; Rydmark, M.; Björkdahl, A.; Sunnerhagen, K.S. Assessment and Training in a 3-Dimensional Virtual Environment with Haptics: A Report on 5 Cases of Motor Rehabilitation in the Chronic Stage after Stroke. Neurorehabilit. Neural Repair 2007, 21, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Naghdy, F.; Naghdy, G.; Du, H. Clinical effectiveness of combined virtual reality and robot assisted fine hand motion rehabilitation in subacute stroke patients. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 511–515. [Google Scholar] [CrossRef]
- Huang, X.; Naghdy, F.; Du, H.; Naghdy, G.; Murray, G. Design of adaptive control and virtual reality-based fine hand motion rehabilitation system and its effects in subacute stroke patients. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2017, 6, 678–686. [Google Scholar] [CrossRef]
- Merians, A.S.; Jack, D.; Boian, R.; Tremaine, M.; Burdea, G.C.; Adamovich, S.V.; Recce, M.; Poizner, H. Virtual Reality–Augmented Rehabilitation for Patients Following Stroke. Phys. Ther. 2002, 82, 898–915. [Google Scholar] [CrossRef] [Green Version]
- Merians, A.S.; Tunik, E.; Fluet, G.G.; Qiu, Q.; Adamovich, S.V. Innovative approaches to the rehabilitation of upper extremity hemiparesis using virtual environments. Eur. J. Phys. Rehabil. Med. 2009, 45, 123–133. [Google Scholar] [PubMed]
- Brewer, B.R.; McDowell, S.K.; Worthen-Chaudhari, L.C. Poststroke Upper Extremity Rehabilitation: A Review of Robotic Systems and Clinical Results. Top. Stroke Rehabil. 2007, 14, 22–44. [Google Scholar] [CrossRef]
- Zariffa, J.; Kapadia, N.; Kramer, J.L.K.; Taylor, P.; Alizadeh-Meghrazi, M.; Zivanovic, V.; Willms, R.; Townson, A.; Curt, A.; Popovic, M.R.; et al. Effect of a robotic rehabilitation device on upper limb function in a sub-acute cervical spinal cord injury population. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–5. [Google Scholar] [CrossRef]
- Eftekharsadat, B.; Babaei-Ghazani, A.; Mohammadzadeh, M.; Talebi, M.; Eslamian, F.; Azari, E. Effect of virtual reality-based balance training in multiple sclerosis. Neurol. Res. 2014, 37, 539–544. [Google Scholar] [CrossRef]
- Massetti, T.; Trevizan, I.L.; Arab, C.; Favero, F.M.; Ribeiro-Papa, D.C.; Monteiro, C.B.D.M. Virtual reality in multiple sclerosis—A systematic review. Mult. Scler. Relat. Disord. 2016, 8, 107–112. [Google Scholar] [CrossRef]
- Lozano-Quilis, J.-A.; Gil-Gómez, H.; Gil-Gómez, J.-A.; Albiol-Pérez, S.; Palacios-Navarro, G.; Fardoun, H.M.; Mashat, A.S. Virtual Rehabilitation for Multiple Sclerosis Using a Kinect-Based System: Randomized Controlled Trial. JMIR Serious Games 2014, 2, e12. [Google Scholar] [CrossRef]
- Bonnechère, B.; Jansen, B.; Omelina, L.L.; Jan, S.V.S. The use of commercial video games in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2016, 39, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Piggott, L.; Wagner, S.; Ziat, M. Haptic Neurorehabilitation and Virtual Reality for Upper Limb Paralysis: A Review. Crit. Rev. Biomed. Eng. 2016, 44, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.A.; Risi, N.; Ballardini, G.; Mrotek, L.A.; Casadio, M.; Scheidt, R.A. Effect of Dual Tasking on Vibrotactile Feedback Guided Reaching—A Pilot Study. In International Conference on Human Haptic Sensing and Touch Enabled Computer Applications; Springer: Cham, Switzerland, 2018; pp. 3–14. [Google Scholar]
- Bark, K.; Wheeler, J.; Shull, P.; Savall, J.; Cutkosky, M. Rotational Skin Stretch Feedback: A Wearable Haptic Display for Motion. IEEE Trans. Haptics 2010, 3, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Huisman, G.; Frederiks, A.D.; van Erp, J.B.; Heylen, D.K. Simulating affective touch: Using a vibrotactile array to generate pleasant stroking sensations. In International Conference on Human Haptic Sensing and Touch Enabled Computer Applications; Springer: Cham, Switzerland, 2016; pp. 240–250. [Google Scholar]
- Risi, N.; Shah, V.; Mrotek, L.A.A.; Casadio, M.; Scheidt, R.A. Supplemental vibrotactile feedback of real-time limb position enhances precision of goal-directed reaching. J. Neurophysiol. 2019, 122, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Krueger, A.R.; Giannoni, P.; Shah, V.; Casadio, M.; Scheidt, R.A. Erratum to: Supplemental vibrotactile feedback control of stabilization and reaching actions of the arm using limb state and position error encodings. J. Neuroeng. Rehabil. 2017, 14, 69. [Google Scholar] [CrossRef] [Green Version]
- Handelzalts, S.; Ballardini, G.; Avraham, C.; Pagano, M.; Casadio, M.; Nisky, I. Integrating Tactile Feedback Technologies into Home-Based Telerehabilitation: Opportunities and Challenges in Light of COVID-19 Pandemic. Front. Neurorobot. 2021, 15, 617636. [Google Scholar] [CrossRef]
- Howard, I.M.; Kaufman, M.S. Telehealth applications for outpatients with neuromuscular or musculoskeletal disorders. Muscle Nerve 2018, 58, 475–485. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Technology | Combinations | Description | Ref ID |
|---|---|---|---|
| Two Technologies | Haptic and gaming | A system that can physically assist or resist the user in playing the therapy games. For example, in Breakout Therapy, the force feedback joystick physically assists in hand movement by predicting the trajectory of the ball after each rebound | [37] |
| Haptics and robotics | Special robot handle generating cutaneous sensory inputs for the middle and index fingers, the thumb, or the palm of the subject + InMotion2 robot | [31] | |
| Haptic system enabling classification of the signals for the real-time identification of a command; exoskeleton of a hand (robotic orthosis) + BCI system consisted of an EEG, encephalograph, and a personal computer | [32] | ||
| Haptic 3 DoF robot: a singly actuated 3 DoF device for assisting in reaching movements in three dimensions across the user’s workspace | [27] | ||
| Haptic Master to correct trajectory performance guided by extra proprioceptive feedback | [28] | ||
| A magnetic plate that is equipped with a force sensor that gauges how hard the fingers press + Vibrotactile glove system designed with light fabric for greater wearability, which is a finger training system in which users interact with the computer | [30] | ||
| An industrial robot (5 DoF desktop robot with position-based control) converted into a novel sensory system incorporating force feedback combined with a graphical interface | [29] | ||
| The ARMin III exoskeleton, which can apply torques directly to each of the 6 DOF of the arm (3 shoulder torques, elbow, flexion–extension, supination–pronation, wrist flexion–extension). The robot applies haptic walls that are exponentially related to each individual joint’s error from its ideal position | [26] | ||
| Haptics and VR | A CyberGlove and a Rutgers Master II (RMII) haptic glove. The two sensing gloves are integrated with VR exercises running on the PC host. RMII glove applies forces to help the patient open the hand before switching to the target of the exercise | [51] | |
| A semi-immersive workbench that uses stereographic shuttered glasses, a 3D image displayed above the tabletop was observed by the user. The system has also a haptic game selection menu | [52] | ||
| 2 PHANToM devices placed perpendicular to each other for the pinch movement and reconfigured to provide hepatic feedback for the pinch task. Haptic feedback was provided for the thumb and index finger, so that the participants felt they were lifting a real cube with mass | [53] | ||
| The PneuGlove used in conjunction with a VR environment (the virtual hand is controlled by the user, who attempts to open the hand sufficiently to grasp the objects displayed), to provide haptic feedback in addition to the assistance of finger extension | [33] | ||
| Four VR hand exercises developed using the WorldToolKit graphics library. Rutgers Master II glove, a compact haptic interface, was used to apply force to the user’s fingertips. It uses non-contact position sensors to measure the fingertip position in relation to the palm | [34] | ||
| VR environments designed for impairment and task-specific training using discrete tasks. Augmented feedback was provided in the form of sensory feedback using haptic cues | [36] | ||
| An immersive VR environment based on the classic story of Alice in Wonderland + The PneuGlove system provides pneumatic assistance to digit extension to help with hand opening or resistance to finger flexion to provide haptic feedback | [35] | ||
| Visual and haptic feedbacks were implemented using the Handshake proSENSE Toolbox. The haptic device is focused on a single finger haptic display, in which the force is exerted at the fingertip. | [54] | ||
| VR tasks were formulated to ensure that pinch movements were required to complete each task and that the patients experienced finger strengthening. Here, 2 Novint Falcon devices operated in coordination to simulate the haptic perceptions of 2 fingertips (perceived the reaction force of the surface and/or the weight of the box). | [55] | ||
| Three Technologies | Haptics, Robotics and VR | CyberGlove Haptic MASTER, a 3 DoF, admittance controlled (force-controlled) robot + Simulations for the hand alone, the arm alone, and the hand and arm together using Virtools software package with the VRPack plug-in + haptic guidance of arm movement in 3D space that is adaptive in real-time as well as on a trial-by-trial basis | [56] |
| PHANTOM robot and the WREX swiveling wrist support + Virtual Reality Robotic and Optical Operations Machine (VRROOM) + Forces only applied by the robot during the Error Augmentation treatment phase | [57] | ||
| CyberGrasp, an exoskeleton device placed on the dorsum of the hand which allows for multiplane arm motion while exerting an extensor force on each individual finger + the virtual piano trainer + CyberGrasp, a force-reflecting exoskeleton that fits over a CyberGlove data glove | [58] | ||
| Haptic Master, a 3 DoF admittance controlled (force-controlled) robot + A haptic system with force feedback available only for pronation/supination + VR environments enabling multiplane movements against gravity in a 3D workspace | [59] | ||
| Haptic MASTER + using Virtools software package with the VRPack plug-in + CyberGrasp to facilitate individual finger movement by resisting flexion of the adjacent fingers in patients with more pronounced deficits allowing for individual movement of each finger. | [56] | ||
| NJIT RAVR system consists of CyberGlove combined with the Haptic Master + Virtual piano trainer + the robotic arm provides tracking of multiplane movements against gravity in a 3D workspace | [60] | ||
| NJIT-RAVR system using a CyberGlove and a Haptic Master + NJIT Track0Glove system + VR simulations for customized motor training | [61] | ||
| NJIT RAVR System including Haptic Master to produce haptic effects, such as spring, damper and constant force and to create haptic objects like blocks, cylinders and spheres as well as walls, floors, ramps and complex surfaces + A suite of simulations for training shoulder, elbow, wrist and finger movements using the Virtools software package | [62] | ||
| RMII glove is an exoskeleton device that applies force to the user’s fingertips and uses noncontact position sensors to measure the fingertip position in relation to the palm + the CyberGlove, a sensorized structure worn on the hand + VR simulations consist of four exercises: range, speed, fractionation, and strength | [63] | ||
| Haptic Master robot coupled to the Grasp Assistance robot—via a 3 passive DoF gimbal + interactive virtual worlds (e.g., cleaning the table) + haptic feedback when touching the object | [64] | ||
| Haptic Master that can move in the virtual learning environment by means of an avatar that is shown on the screen + haptic feedback can be provided to either support or challenge the participants | [65] | ||
| Haptic Master’s to program the robot to produce haptic objects + VR gaming simulations that translates movement of both the upper arm and the hand | [66] | ||
| A 6 DoF PHANTOM Premium 3.0 robot + a haptics/graphics display combining a projected stereo, head-tracked rendering on a semi-silvered mirror overlay display with a robotic system that can record wrist position, track movements and generate force feedback + A cinema-quality digital projector combined with LCD shutter glasses | [67] | ||
| Haptics, Robotics and Gaming | Arm Coordination Training 3D system providing a haptic interface to simulate various loading conditions while subjects performed arm reaching movements with avatar and game feedback + haptic feedback consisting of a simulated viscous environment that prevented subjects from moving on the haptic table + Air Hockey 3D game | [38] | |
| FINGER robotic exoskeleton providing 2 levels of assistance + Musical computer game in the style of Guitar Hero | [68] | ||
| Haptics, VR and Gaming | Four hand exercises simulations developed with WorldToolKit (Sense 8) + Rutgers Master II-ND (RMII) force feedback glove prototype + Simple games that provided frequent feedback about the success of the action as well as the quality of the performance to encourage participation and concentration | [69] | |
| Four hand exercises simulations developed with WorldToolKit (Sense 8) + RMII glove has a dedicated electropneumatic control interface to provide force feedback to the patient’s fingers + simple video games developed with WorldToolKit (Sense8) graphics library | [69] | ||
| PHANToM haptic device + Reachin 3.0. Reachin API, a 3D model programming (haptic interface) + grasping and reaching game. | [70] | ||
| 4 hand exercise simulations developed with the WorldTool Kit graphics library + Rutgers Master II-ND (RMII), a force feedback prototype glove + games designed to exercise one parameter of finger movement at a time | [39] | ||
| PHANToM devices + tasks displayed using a desktop personal computer and shutter glasses (StereoGraphics) to provide a three-dimensional view of stimuli + Reaching, Ball Shooting, Rotation and Pinch games | [71] | ||
| Four Technologies | Haptics, Robotics, VR and Gaming | A desk-mounted robot + a haptic stylus. + a semi-immersive workbench + 3D Bricks game | [72] |
| Amadeo, A 5 DoF hand rehabilitation robotic device named + incorporated Real-time force and position signals + highly repetitive functional VR tasks + Flying bird and Spaceship games | [73] | ||
| Amadeo, A 5 DoF hand rehabilitation robotic device named + 2D, one 3D VR-based RGS and a 2D transferring virtual environment + Flying bird | [74] | ||
| CyberGlove + haptic (force), visual and auditory feedback + 3D graphics were displayed on a flat personal computer screen using only shadows and perspective cues to give the illusion of depth. + computer games using graphics feedback to encourage participation and concentration | [75] | ||
| Haptic Master + 3 more DoF can be added to the arm by using a gimbal, with force feedback available only pronation/supination + Stimulated unimanual “virtual mirror” + Piano Trainer, Space Pong, Plasma pong, bird hunt and Hammer games | [76] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choukou, M.-A.; Mbabaali, S.; Bani Hani, J.; Cooke, C. Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review. Appl. Sci. 2021, 11, 3712. https://doi.org/10.3390/app11083712
Choukou M-A, Mbabaali S, Bani Hani J, Cooke C. Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review. Applied Sciences. 2021; 11(8):3712. https://doi.org/10.3390/app11083712
Chicago/Turabian StyleChoukou, Mohamed-Amine, Sophia Mbabaali, Jasem Bani Hani, and Carol Cooke. 2021. "Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review" Applied Sciences 11, no. 8: 3712. https://doi.org/10.3390/app11083712
APA StyleChoukou, M. -A., Mbabaali, S., Bani Hani, J., & Cooke, C. (2021). Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review. Applied Sciences, 11(8), 3712. https://doi.org/10.3390/app11083712