
Deep Learning Application in Dental Caries Detection Using Intraoral Photos Taken by Smartphones

 , and
, and
Abstract
:1. Introduction
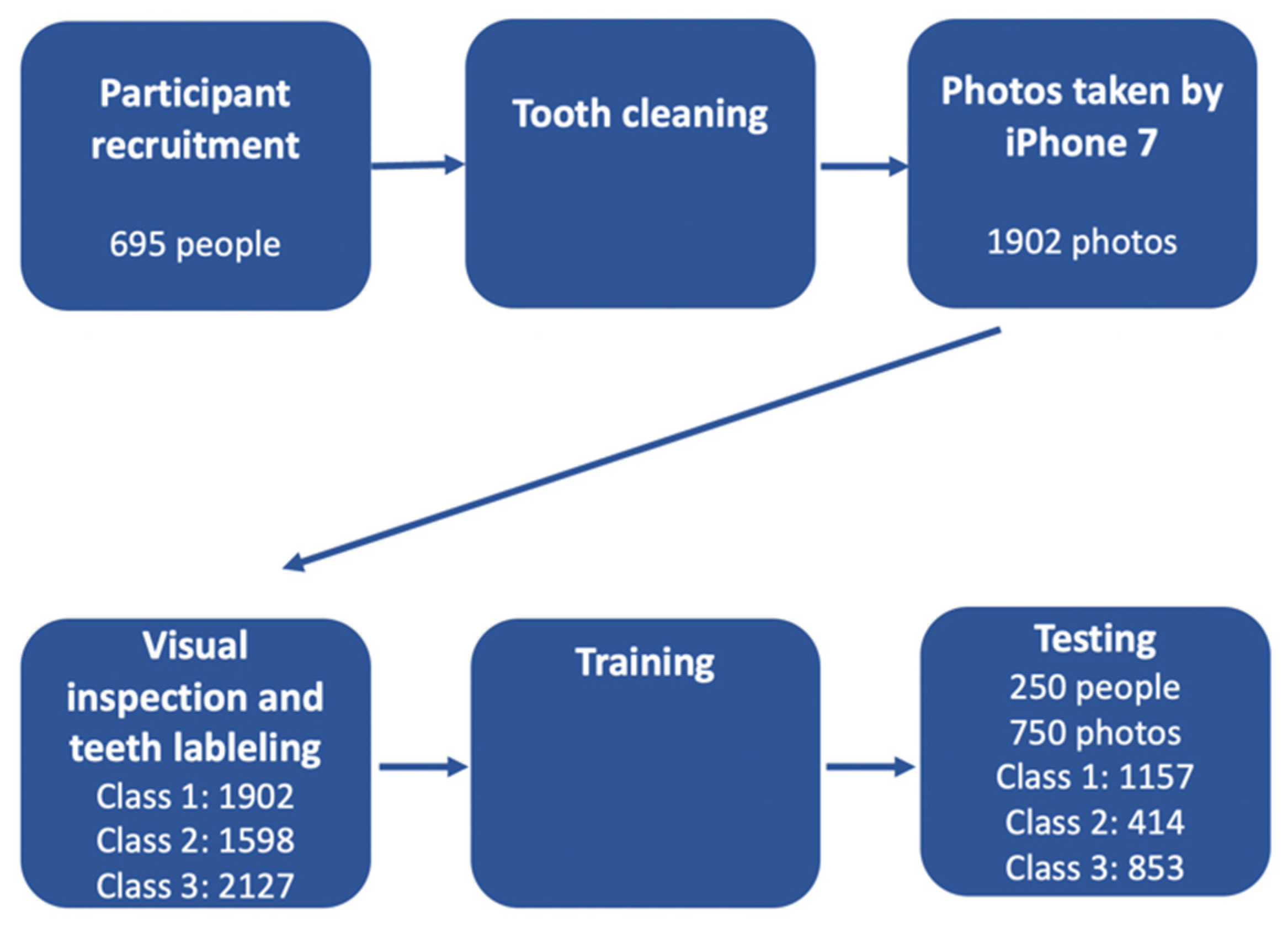
2. Materials and Methods
2.1. Photographic Images
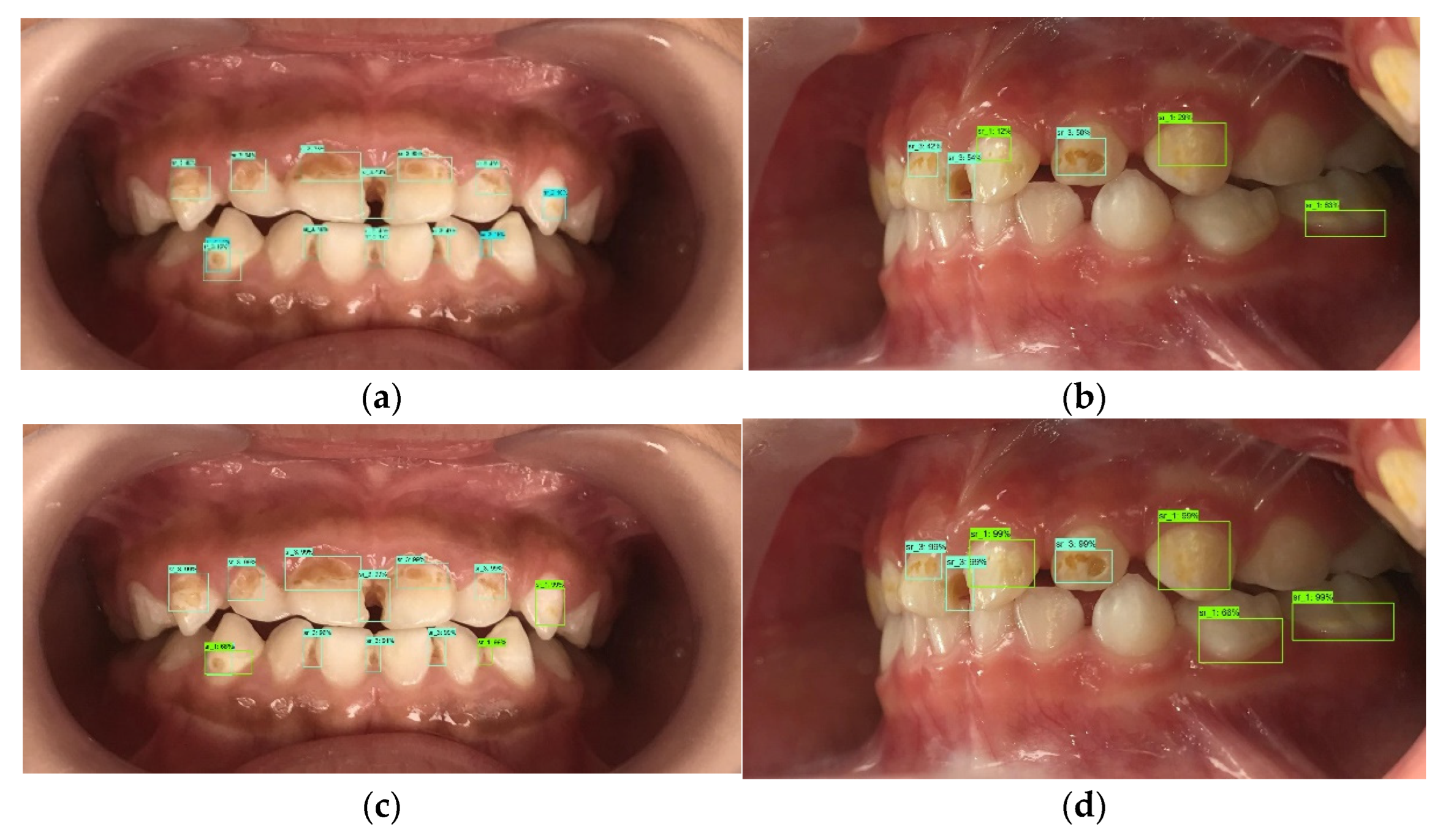
2.2. Reference Standard and Labeling Dataset
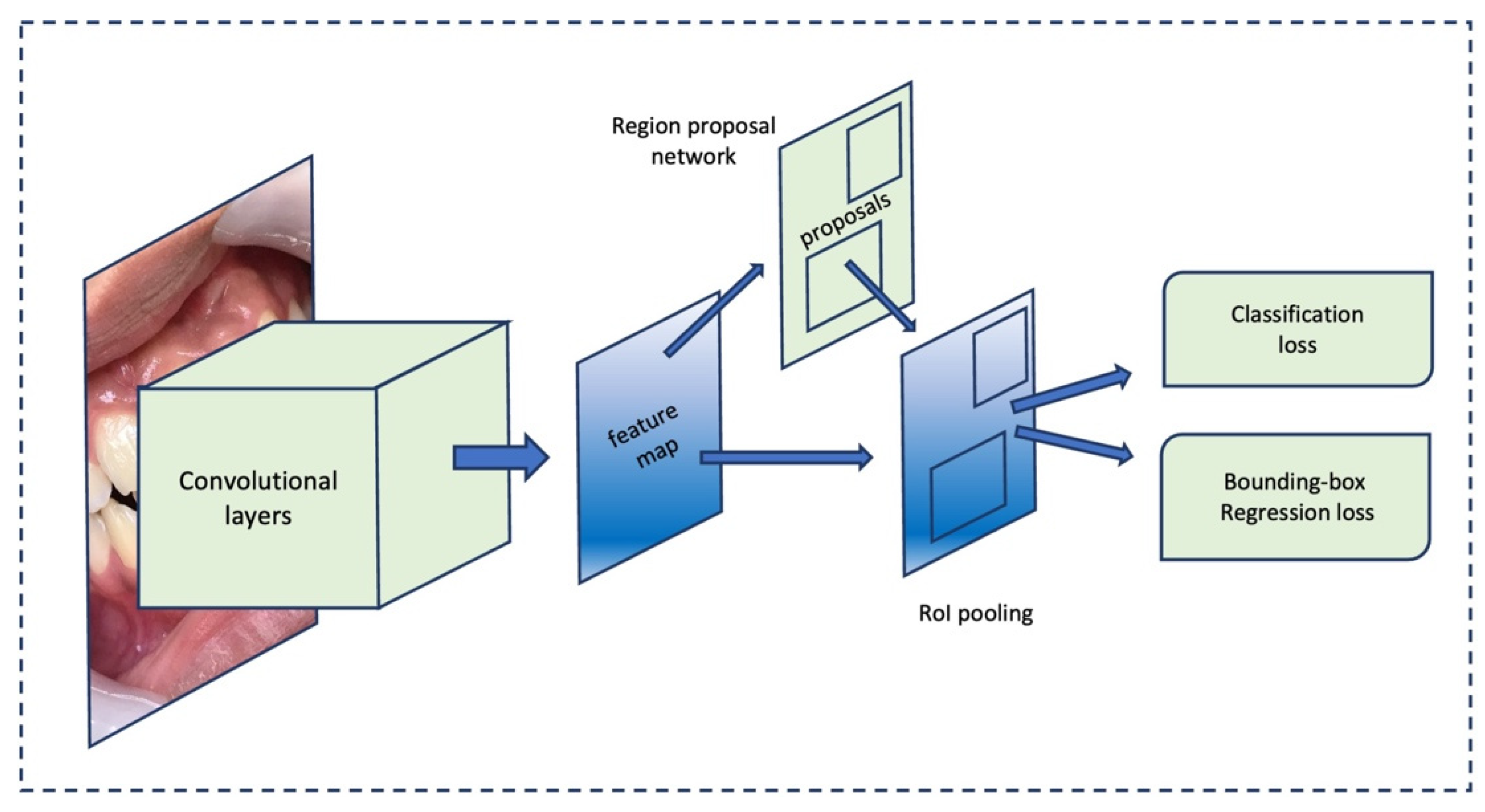
2.3. Deep Learning Architecture
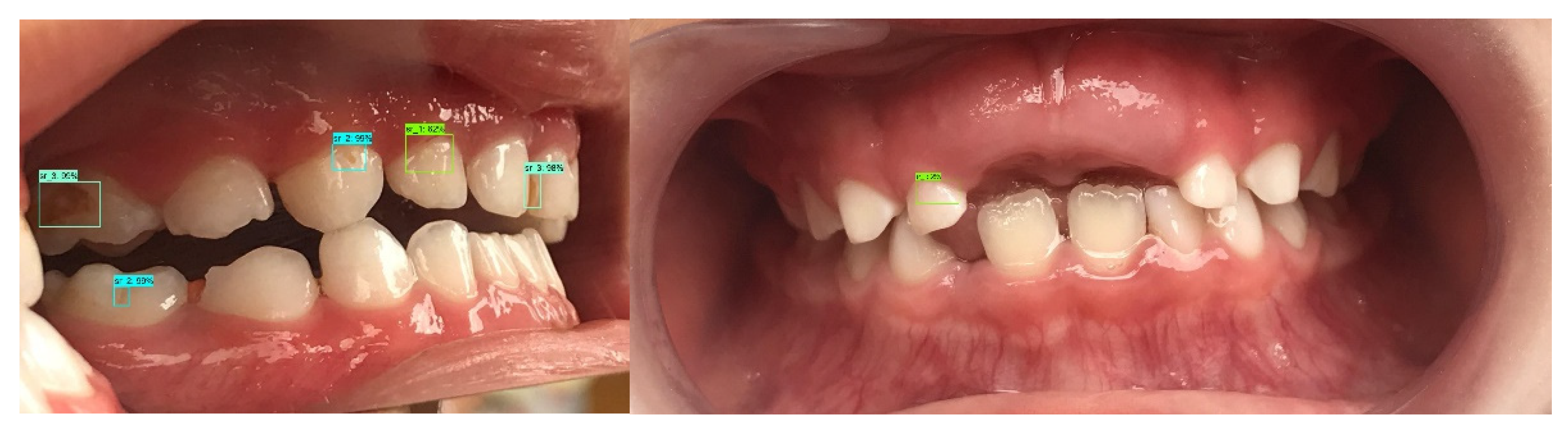
2.4. Evaluation
2.5. Analysis
3. Results
3.1. C vs. NC Classification
3.2. NSC vs. VNC Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.; Jin, B.; Bae, K.; Lee, B.; Han, D. Strategies and Educational Manuals to Improve National Oral Examination Program; Ministry of Health and Welfare: Seoul, Korea, 2009; pp. 25–76. [Google Scholar]
- Kandelman, D.; Arpin, S.; Baez, R.J.; Baehni, P.C.; Petersen, P.E. Oral health care systems in developing and developed countries. Periodontology 2000 2012, 60, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-W. Assessment of panoramic radiography as a national oral examination tool: Review of the literature. Imaging Sci. Dent. 2011, 41, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benzian, H.; Hobdell, M.; Mackay, J. Putting teeth into chronic diseases. Lancet 2011, 377, 464. [Google Scholar] [CrossRef]
- Hwang, J.-J.; Jung, Y.-H.; Cho, B.-H.; Heo, M.-S. An overview of deep learning in the field of dentistry. Imaging Sci. Dent. 2019, 49, 1–7. [Google Scholar] [CrossRef]
- Tamaki, Y.; Nomura, Y.; Katsumura, S.; Okada, A.; Yamada, H.; Tsuge, S.; Kadoma, Y.; Hanada, N. Construction of a dental caries prediction model by data mining. J. Oral Sci. 2009, 51, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Patil, S.; Kulkarni, V.; Bhise, A. Algorithmic analysis for dental caries detection using an adaptive neural network architecture. Heliyon 2019, 5, e01579. [Google Scholar] [CrossRef] [Green Version]
- Prados-Privado, M.; García Villalón, J.; Martínez-Martínez, C.H.; Ivorra, C.; Prados-Frutos, J.C. Dental caries diagnosis and detection using neural networks: A systematic review. J. Clin. Med. 2020, 9, 3579. [Google Scholar] [CrossRef]
- Moutselos, K.; Berdouses, E.; Oulis, C.; Maglogiannis, I. Recognizing occlusal caries in dental intraoral images using deep learning. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1617–1620. [Google Scholar]
- Askar, H.; Krois, J.; Rohrer, C.; Mertens, S.; Elhennawy, K.; Ottolenghi, L.; Mazur, M.; Paris, S.; Schwendicke, F. Detecting white spot lesions on dental photography using deep learning: A pilot study. J. Dent. 2021, 107, 103615. [Google Scholar] [CrossRef]
- Ding, B.; Zhang, Z.; Liang, Y.; Wang, W.; Hao, S.; Meng, Z.; Guan, L.; Hu, Y.; Guo, B.; Zhao, R.; et al. Detection of dental caries in oral photographs taken by mobile phones based on the YOLOv3 algorithm. Ann. Transl. Med. 2021, 9, 1622. [Google Scholar] [CrossRef]
- Kim, D.; Choi, J.; Ahn, S.; Park, E. A smart home dental care system: Integration of deep learning, image sensors, and mobile controller. J. Ambient Intell. Humaniz. Comput. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Estai, M.; Tennant, M.; Gebauer, D.; Brostek, A.; Vignarajan, J.; Mehdizadeh, M.; Saha, S. Evaluation of a deep learning system for automatic detection of proximal surface dental caries on bitewing radiographs. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- DentalMonitoring Home Page. Available online: https://dental-monitoring.com/ (accessed on 21 May 2022).
- Duong, D.L.; Kabir, M.H.; Kuo, R.F. Automated caries detection with smartphone color photography using machine learning. Health Inform. J. 2021, 27, 14604582211007530. [Google Scholar] [CrossRef] [PubMed]
- Casalegno, F.; Newton, T.; Daher, R.; Abdelaziz, M.; Lodi-Rizzini, A.; Schürmann, F.; Krejci, I.; Markram, H. Caries Detection with Near-Infrared Transillumination Using Deep Learning. J. Dent. Res. 2019, 98, 1227–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kühnisch, J.; Meyer, O.; Hesenius, M.; Hickel, R.; Gruhn, V. Caries Detection on Intraoral Images Using Artificial Intelligence. J. Dent. Res. 2022, 101, 158–165. [Google Scholar] [CrossRef]
- Pitts, N.B.; Ekstrand, K.R. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef]
- Lohia, A.; Kadam, K.D.; Joshi, R.R.; Bongale, A.M. Bibliometric Analysis of One-stage and Two-stage Object Detection. Libr. Philos. Pract. 2021, 4910. Available online: https://digitalcommons.unl.edu/libphilprac/4910 (accessed on 28 March 2022).
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. In Proceedings of the 25th International Conference on Neural Information Processing Systems, Lake Tahoe, NV, USA, 3–6 December 2012. [Google Scholar]
- Inês Meurer, M.; Caffery, L.J.; Bradford, N.K.; Smith, A.C. Accuracy of dental images for the diagnosis of dental caries and enamel defects in children and adolescents: A systematic review. J. Telemed. Telecare 2015, 21, 449–458. [Google Scholar] [CrossRef]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You only look once: Unified, real-time object detection. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 779–788. [Google Scholar]
- Redmon, J.; Farhadi, A. Yolov3: An incremental improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar]
- Mao, Q.-C.; Sun, H.-M.; Liu, Y.-B.; Jia, R.-S. Mini-YOLOv3: Real-time object detector for embedded applications. IEEE Access 2019, 7, 133529–133538. [Google Scholar] [CrossRef]
- Liu, W.; Anguelov, D.; Erhan, D.; Szegedy, C.; Reed, S.; Fu, C.-Y.; Berg, A.C. Ssd: Single shot multibox detector. In Computer Vision—ECCV 2016. ECCV 2016; Leibe, B., Matas, J., Sebe, N., Welling, M., Eds.; Lecture Notes in Computer Science Series; Springer: Cham, Switzerland, 2016; Volume 9905, pp. 21–37. [Google Scholar]
- Lin, T.-Y.; Goyal, P.; Girshick, R.; He, K.; Dollár, P. Focal loss for dense object detection. In Proceedings of the 2017 IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017; pp. 2980–2988. [Google Scholar]
- Gimenez, T.; Piovesan, C.; Braga, M.M.; Raggio, D.P.; Deery, C.; Ricketts, D.N.; Ekstrand, K.R.; Mendes, F.M. Visual Inspection for Caries Detection: A Systematic Review and Meta-analysis. J. Dent. Res. 2015, 94, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Kohara, E.K.; Abdala, C.G.; Novaes, T.F.; Braga, M.M.; Haddad, A.E.; Mendes, F.M. Is it feasible to use smartphone images to perform telediagnosis of different stages of occlusal caries lesions? PLoS ONE 2018, 13, e0202116. [Google Scholar] [CrossRef] [PubMed]
- Koziarski, M.; Cyganek, B. Impact of Low Resolution on Image Recognition with Deep Neural Networks: An Experimental Study. Int. J. Appl. Math. Comput. Sci. 2018, 28, 735–744. [Google Scholar] [CrossRef] [Green Version]
- Thanh, M.T.G.; Van Toan, N.; Toan, D.T.T.; Thang, N.P.; Dong, N.Q.; Dung, N.T.; Hang, P.T.T.; Anh, L.Q.; Tra, N.T.; Ngoc, V.T.N. Diagnostic Value of Fluorescence Methods, Visual Inspection and Photographic Visual Examination in Initial Caries Lesion: A Systematic Review and Meta-Analysis. Dent. J. 2021, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Wang, B.; Zhang, W.; Zeng, X.; Yan, X.; Feng, Z.; Liu, Y.; Wu, Z. An improved faster R-CNN for small object detection. IEEE Access 2019, 7, 106838–106846. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model Deep Learning | Sensitivity % | Specificity % | Accuracy % | Precision % |
|---|---|---|---|---|
| YOLOv3 | 74 | 86.6 | 83.4 | 65.3 |
| Faster R-CNN | 71.2 | 92.9 | 87.4 | 77.3 |
| RetinaNet | 63.2 | 89.8 | 83 | 67.7 |
| SSD | 26 | 99.7 | 81 | 97.1 |
| Model Deep Learning | Sensitivity % | Specificity % | Accuracy % | Precision % |
|---|---|---|---|---|
| YOLOv3 | 36.9 | 71.4 | 60.7 | 49.7 |
| Faster R-CNN | 23.4 | 87.7 | 67.8 | 61.5 |
| RetinaNet | 26.5 | 83.3 | 65.7 | 61.3 |
| SSD | 0 | 99.7 | 68.8 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thanh, M.T.G.; Van Toan, N.; Ngoc, V.T.N.; Tra, N.T.; Giap, C.N.; Nguyen, D.M. Deep Learning Application in Dental Caries Detection Using Intraoral Photos Taken by Smartphones. Appl. Sci. 2022, 12, 5504. https://doi.org/10.3390/app12115504
Thanh MTG, Van Toan N, Ngoc VTN, Tra NT, Giap CN, Nguyen DM. Deep Learning Application in Dental Caries Detection Using Intraoral Photos Taken by Smartphones. Applied Sciences. 2022; 12(11):5504. https://doi.org/10.3390/app12115504
Chicago/Turabian StyleThanh, Mai Thi Giang, Ngo Van Toan, Vo Truong Nhu Ngoc, Nguyen Thu Tra, Cu Nguyen Giap, and Duc Minh Nguyen. 2022. "Deep Learning Application in Dental Caries Detection Using Intraoral Photos Taken by Smartphones" Applied Sciences 12, no. 11: 5504. https://doi.org/10.3390/app12115504
APA StyleThanh, M. T. G., Van Toan, N., Ngoc, V. T. N., Tra, N. T., Giap, C. N., & Nguyen, D. M. (2022). Deep Learning Application in Dental Caries Detection Using Intraoral Photos Taken by Smartphones. Applied Sciences, 12(11), 5504. https://doi.org/10.3390/app12115504