
The Effect of Feldspathic Thickness on Fluorescence of a Variety of Resin Cements and Flowable Composites

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
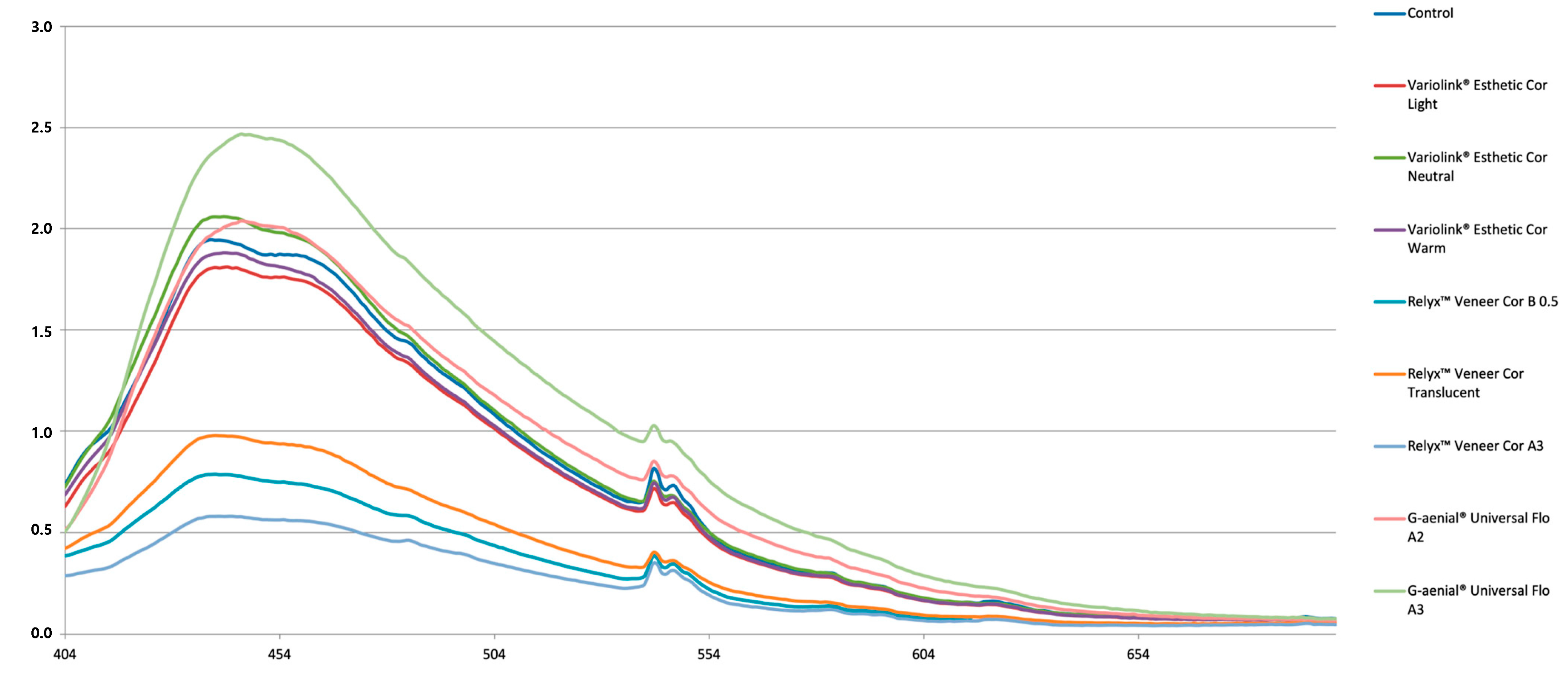
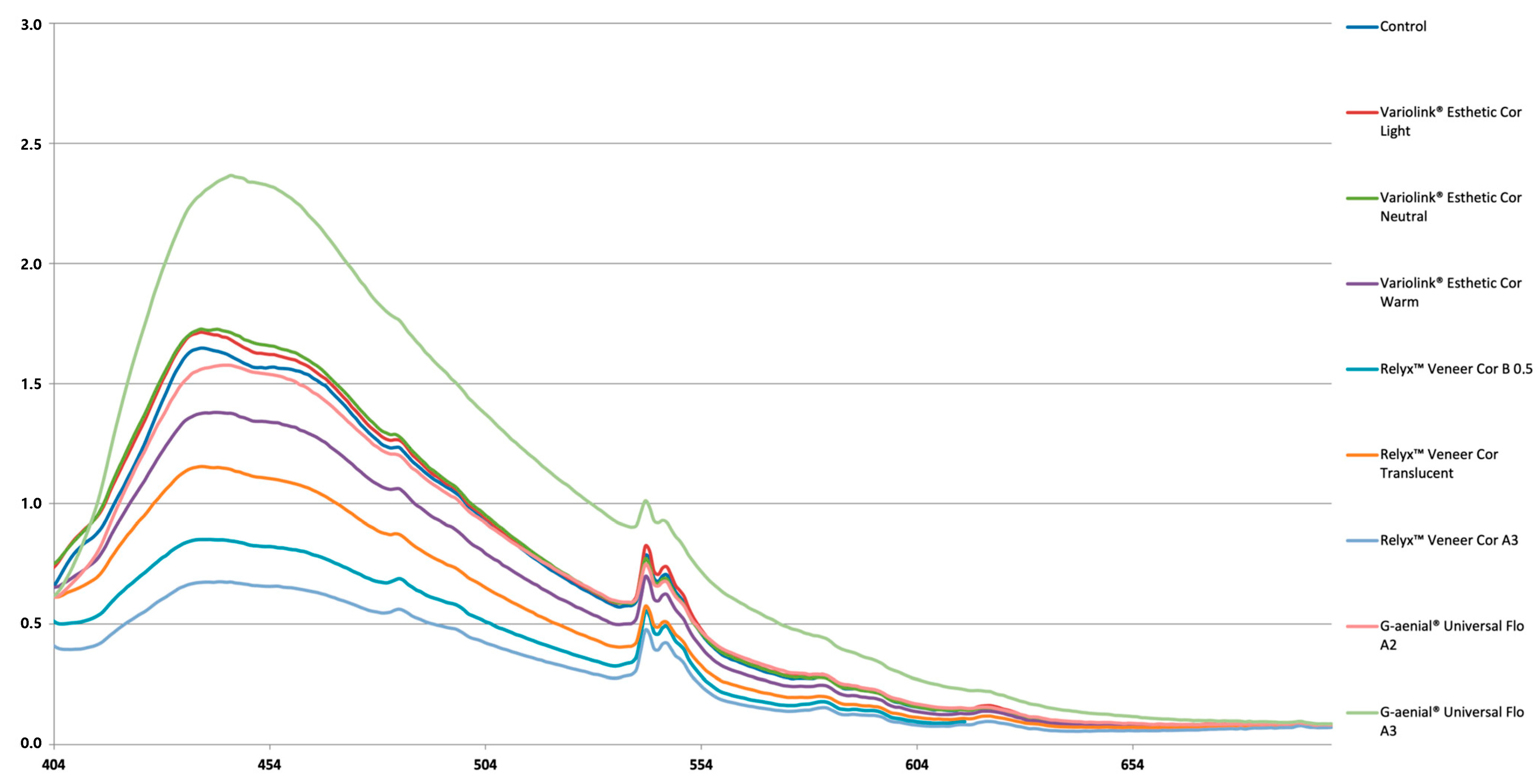
3. Results
4. Discussion
5. Conclusions
- -
- The fluorescence of feldspathic ceramic veneer restorations (CEREC Blocs) can be influenced by the shade and brand of resin-based materials used for luting;
- -
- Thicker feldspathic veneers show less fluorescence emission intensity when they are cemented with resin cements or flowable composite resins in darker shades.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beier, U.S.; Dumfahrt, H. Clinical performance of porcelain laminate veneers for up to 20 years. J. Prosthet. Dent. 2012, 107, 157. [Google Scholar] [CrossRef]
- Mauro, F.; Marco, R.; Marcantonio, C. Porcelain laminate veneers: 6- to 12-year clinical evaluation—A retrospective study. Int. J. Periodontics Restor. Dent. 2005, 25, 9–17. [Google Scholar]
- Faus-Matoses, V.; Ruiz-Bell, E.; Faus-Matoses, I.; Özcan, M.; Salvatore, S.; Faus-Llácer, V.J. An 8-year prospective clinical investigation on the survival rate of feldspathic veneers: Influence of occlusal splint in patients with bruxism. J. Dent. 2020, 99, 103352. [Google Scholar] [CrossRef] [PubMed]
- Hong, N.; Yang, H.; Li, J.; Wu, S.; Li, Y. Effect of preparation designs on the prognosis of porcelain laminate veneers: A systematic review and meta-analysis. Oper. Dent. 2017, 42, E197–E213. [Google Scholar] [CrossRef]
- Morimoto, S.; Albanesi, R.; Sesma, N.; Agra, C.; Braga, M. Main Clinical Outcomes of Feldspathic Porcelain and Glass-Ceramic Laminate Veneers: A Systematic Review and Meta-Analysis of Survival and Complication Rates. Int. J. Prosthodont. 2016, 29, 38–49. [Google Scholar] [CrossRef] [PubMed]
- D’Arcangelo, C.; Vanini, L.; Rondoni, G.D.; De Angelis, F. Wear properties of dental ceramics and porcelains compared with human enamel. J. Prosthet. Dent. 2016, 115, 350–355. [Google Scholar] [CrossRef]
- Ghazal, M.; Kern, M. Wear of human enamel and nano-filled composite resin denture teeth under different loading forces. J. Oral Rehabil. 2009, 36, 58–64. [Google Scholar] [CrossRef] [PubMed]
- D’Arcangelo, C.; De Angelis, F.; Vadini, M.; D’Amario, M.; Caputi, S. Fracture Resistance and Deflection of Pulpless Anterior Teeth Restored with Composite or Porcelain Veneers. J. Endod. 2010, 36, 153–156. [Google Scholar] [CrossRef]
- Dozić, A.; Kleverlaan, C.J.; Meegdes, M.; Van Der Zel, J.; Feilzer, A.J. The influence of porcelain layer thickness on the final shade of ceramic restorations. J. Prosthet. Dent. 2003, 90, 563–570. [Google Scholar] [CrossRef]
- Pissaia, J.F.; Guanaes, B.K.A.; Kintopp, C.C.A.; Correr, G.M.; da Cunha, L.F.; Gonzaga, C.C. Color stability of ceramic veneers as a function of resin cement curing mode and shade: 3-year follow-up. PLoS ONE 2019, 14, e0219183. [Google Scholar] [CrossRef]
- Silami, F.D.J.; Tonani, R.; Alandia-Román, C.C.; Pires-De-Souza, F.C.P. Influence of different types of resin luting agents on color stability of ceramic laminate veneers subjected to accelerated artificial aging. Braz. Dent. J. 2016, 27, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vichi, A.; Ferrari, M.; Davidson, C.L. Influence of ceramic and cement thickness on the masking of various types of opaque posts. J. Prosthet. Dent. 2000, 83, 412–417. [Google Scholar] [CrossRef]
- Volpato, C.A.M.; Monteiro, S.; de Andrada, M.C.; Fredel, M.C.; Petter, C.O. Optical influence of the type of illuminant, substrates and thickness of ceramic materials. Dent. Mater. J. 2009, 25, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Turgut, S.; Bagis, B. Effect of resin cement and ceramic thickness on final color of laminate veneers: An in vitro study. J. Prosthet. Dent. 2013, 109, 179–186. [Google Scholar] [CrossRef]
- Joiner, A. Tooth colour: A review of the literature. J. Dent. 2004, 32, 3–12. [Google Scholar] [CrossRef]
- Mclaren, E.A. Luminescent Veneers. J. Esthet. Dent. 1997, 9, 3–12. [Google Scholar] [CrossRef]
- Baran, G.R.; O’brien, W.J.; Tien, T.Y. Colored Emission of Rare Earth Ions in a Potassium Feldspar Glass. J. Dent. Res. 1977, 56, 1323–1329. [Google Scholar] [CrossRef]
- Wozniak, W.T.; Moore, B.K. Luminescence Spectra of Dental Porcelains. J. Dent. Res. 1978, 57, 971–974. [Google Scholar] [CrossRef]
- Volpato, C.A.M.; Pereira, M.R.C.; Silva, F.S. Fluorescence of natural teeth and restorative materials, methods for analysis and quantification: A literature review. J. Esthet. Restor. Dent. 2018, 30, 397–407. [Google Scholar] [CrossRef]
- Correia, A.M.O.; Borges, A.B.; Caneppele, T.M.F.; Torres, C.R.G. Influence of interim cements on the optical properties of interim restorations. J. Prosthet. Dent. 2019, 121, 821–827. [Google Scholar] [CrossRef]
- Revilla-León, M.; Sorensen, J.A.; Nelson, L.Y.; Gamborena, I.; Yeh, Y.M.; Özcan, M. Effect of fluorescent and nonfluorescent glaze pastes on lithium disilicate pressed ceramic color at different thicknesses. J. Prosthet. Dent. 2020, 125, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.K.; Vieira, S.; Rached, R.N.; De Almeida, J.B.; Aguiar, M.; De Souza, E.M. Fluorescence intensity of resin composites and dental tissues before and after accelerated aging: A comparative study. Oper. Dent. 2008, 33, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Ecker, G.A.; Moser, J.B.; Wozniak, W.T.; Brinsden, G.I. Effect of repeated firing on fluorescence of porcelain-fused-to-metal porcelains. J. Prosthet. Dent. 1985, 54, 207–214. [Google Scholar] [CrossRef]
- Uo, M.; Okamoto, M.; Watari, F.; Tani, K.; Morita, M.; Shintani, A. Rare earth oxide-containing fluorescent glass filler for composite resin. Dent. Mater. J. 2005, 24, 49–52. [Google Scholar] [CrossRef]
- Rüttermann, S.; Ritter, J.; Raab, W.H.M.; Bayer, R.; Janda, R. Laser-induced fluorescence to discriminate between a dental composite resin and tooth. Dent. Mater. 2007, 23, 1390–1396. [Google Scholar] [CrossRef]
- Foreman, P.C. The excitation and emission spectra of fluorescent components of human dentine. Arch. Oral Biol. 1980, 25, 641–647. [Google Scholar] [CrossRef]
- Rafael, C.F.; Güth, J.-F.; Kauling, A.E.C.; CesaR, P.F.; Volpato, C.A.M.; Liebermann, A. Impact of background on color, transmittance, and fluorescence of leucite based ceramics. Dent. Mater. J. 2017, 36, 394–401. [Google Scholar] [CrossRef] [Green Version]
- Silami, F.D.J.; Pratavieira, S.; Nogueira, M.S.; Barrett, A.A.; Sinhoreti, M.A.C.; Geraldeli, S.; Pires-DE-Souza, F.C.P. Quantitative image of fluorescence of ceramic and resin-cement veneers. Braz. Oral Res. 2019, 33, 1–10. [Google Scholar] [CrossRef]
- Lise, D.P.; Van Ende, A.; De Munck, J.; Yoshihara, K.; Nagaoka, N.; Cardoso Vieira, L.C.; Van Meerbeek, B. Light irradiance through novel CAD–CAM block materials and degree of conversion of composite cements. Dent. Mater. 2018, 34, 296–305. [Google Scholar] [CrossRef]
- Pegoraro, T.A.; da Silva, N.R.F.A.; Carvalho, R.M. Cements for use in esthetic dentistry. Dent. Clin. N. Am. 2007, 51, 453–471. [Google Scholar] [CrossRef]
- Archegas, L.R.P.; Freire, A.; Vieira, S.; Caldas, D.B.D.M.; Souza, E.M.H. Colour stability and opacity of resin cements and flowable composites for ceramic veneer luting after accelerated ageing. J. Dent. 2011, 39, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Monsénégo, G.; Burdairon, G.; Clerjaud, B. Fluorescence of dental porcelain. J. Prosthet. Dent. 1993, 69, 106–113. [Google Scholar] [CrossRef]
- Peplinski, D.R.; Wozniak, W.T.; Moser, J.B. Spectral Studies of New Luminophors for Dental Porcelain. J. Dent. Res. 1980, 59, 1501–1506. [Google Scholar] [CrossRef] [PubMed]
- Tani, K.; Watari, F.; Uo, M.; Morita, M. Fluorescent Properties of Porcelain-Restored Teeth and Their Discrimination. Mater. Trans. 2004, 45, 1010–1014. [Google Scholar] [CrossRef]
- Gawriolek, M.; Sikorska, E.; Ferreira, L.F.V.; Costa, A.I.; Khmelinskii, I.; Krawczyk, A.; Sikorski, M.; Koczorowski, R. Color and Luminescence Stability of Selected Dental Materials In Vitro. J. Prosthodont. 2012, 21, 112–122. [Google Scholar] [CrossRef] [Green Version]
- Conrad, H.J.; Seong, W.-J.; Pesun, I.J. Current ceramic materials and systems with clinical recommendations: A systematic review. J. Prosthet. Dent. 2007, 98, 389–404. [Google Scholar] [CrossRef]
- Silva, L.H.; Lima, E.; Miranda, R.B.P.; Favero, S.S.; Lohbauer, U.; Cesar, P.F. Dental ceramics: A review of new materials and processing methods. Braz. Oral Res. 2017, 31, 133–146. [Google Scholar] [CrossRef]
- Spitznagel, F.A.; Boldt, J.; Gierthmuehlen, P.C. CAD/CAM Ceramic Restorative Materials for Natural Teeth. J. Dent. Res. 2018, 97, 1082–1091. [Google Scholar] [CrossRef]
- Mack, P.J. The recent history of radioactive fluorescers in dental porcelain. Aust. Dent. J. 1988, 33, 404–406. [Google Scholar] [CrossRef]
- Lu, H.; Lee, Y.K.; Villalta, P.; Powers, J.M.; Garcia-Godoy, F. Influence of the amount of UV component in daylight simulator on the color of dental composite resins. J. Prosthet. Dent. 2006, 96, 322–327. [Google Scholar] [CrossRef]
- Kiran, R.; Chapman, J.; Tennant, M.; Forrest, A.; Walsh, L. Direct tooth-colored restorative materials: A comparative analysis of the fluorescence properties among different shades. Int. J. Esthet. Dent. 2020, 15, 318–332. [Google Scholar] [PubMed]
- Duro, F.R.; Andrade, J.S. Fluorescence: Clinical Evaluation of New Composite Resins. Quintessence Dent. Technol. 2012, 35, 145–157. [Google Scholar]
- Ameer, Z.M.A.; Sc, M. In Vitro Evaluation of Fluorescence Stability of Different Composites and Dental Tissues before and after Accelerated Aging. J. Med. Dent. Sci. Res. 2015, 3, 1–6. [Google Scholar]
- de Lima, L.M.; Abreu, J.D.; Cohen-Carneiro, F.; Regalado, D.F.; Pontes, D.G. A new methodology for fluorescence analysis of composite resins used in anterior direct restorations. Gen. Dent. 2015, 63, 66–69. [Google Scholar] [PubMed]
- Magne, P.; Belser, U. Bonded Porcelain Restorations in the Anterior Dentition: A Biomimetic Approach; Quintessence Publishing Co, Inc.: Berlin, Germany, 2002; ISBN 0-86715-422-5. [Google Scholar]
- Matsumoto, H.; Kitamura, S.; Araki, T. Applications of fluorescence microscopy to studies of dental hard tissue. Front. Med. Biol. Eng. 2001, 10, 269–284. [Google Scholar] [CrossRef]
- Matsumoto, H.; Kitamura, S.; Araki, T. Autofluorescence in human dentine in relation to age, tooth type and temperature measured by nanosecond time-resolved fluorescence microscopy. Arch. Oral Biol. 1999, 44, 309–318. [Google Scholar] [CrossRef]
- Tani, K.; Watari, F.; Uo, M.; Morita, M. Discrimination between composite resin and teeth using fluorescence properties. Dent. Mater. J. 2003, 22, 569–580. [Google Scholar] [CrossRef] [Green Version]
- Caneppele, T.M.F.; Torres, C.R.G.; Bresciani, E. Analysis of the color and fluorescence alterations of enamel and dentin treated with hydrogen peroxide. Braz. Dent. J. 2015, 26, 514–518. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-K. Fluorescence properties of human teeth and dental calculus for clinical applications. J. Biomed. Opt. 2015, 20, 040901. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Material and Manufacturer | Composition | Batch Number |
|---|---|---|
| Cerec® Blocs C/PC VITA Shade: A2 CAD-CAM feldspathic ceramic | SiO2 (56–64%), Al2O3 (20–23%), Na2O (6–9%), K2 (6–8%), CaO (0.3–0.8%), TiO2 (0.0–0.1%), pigments <0.1%. | 66301 |
| RelyX Veneer 3M Oral Care Shade: B0.5, A3 and Translucent Resin cement | Bis-GMA, TEGDMA, Zirconia/silica, modified silica. Particle loading approximately 66% by weight, particle size approximately 0.6 mm, photoinitiator. | N862421 N816236 N843828 |
| Variolink Esthetic LCIvoclar Vivadent Shade: Light, Neutral and Warm Resin cement | Dimethacrylate, methacrylate monomers, inorganic particles Ytterbium trifluoride and spheroid oxide mixed. primers, stabilizers and pigments. Particle size is from 0.04 to 0.2 μm. Inorganic charge is approximately 38%. | v48653 w05218 w06171 |
| G-aenial Universal GC Corporation Shade: Flo A2 and A3Flowable composite resin | Urethanedimetrylate, Bis-MEPP, TEGDMA (31%). Silicon dioxide (16 nm), Strontium glass (200 nm), pigments (69%), photoinitiator. | 161202 |
| Filtek Supreme XTE3M Oral Care Shade: A3 Body Nanofilled composite resin | UDMA, Bis-GMA, Bis-EMA, Silica (20 nm) Zirconia (4–10 nm). Size of the particles together 0.6 to 10 μm. Inorganic particles represent 72.5% of the total charge. | N859611 |
| Resin-Based Material | Ceramic Thickness | 0.5 mm vs. 0.8 mm (p-Value) | |
|---|---|---|---|
| 0.5 mm | 0.8 mm | ||
| Mean ± SD | Mean ± SD | ||
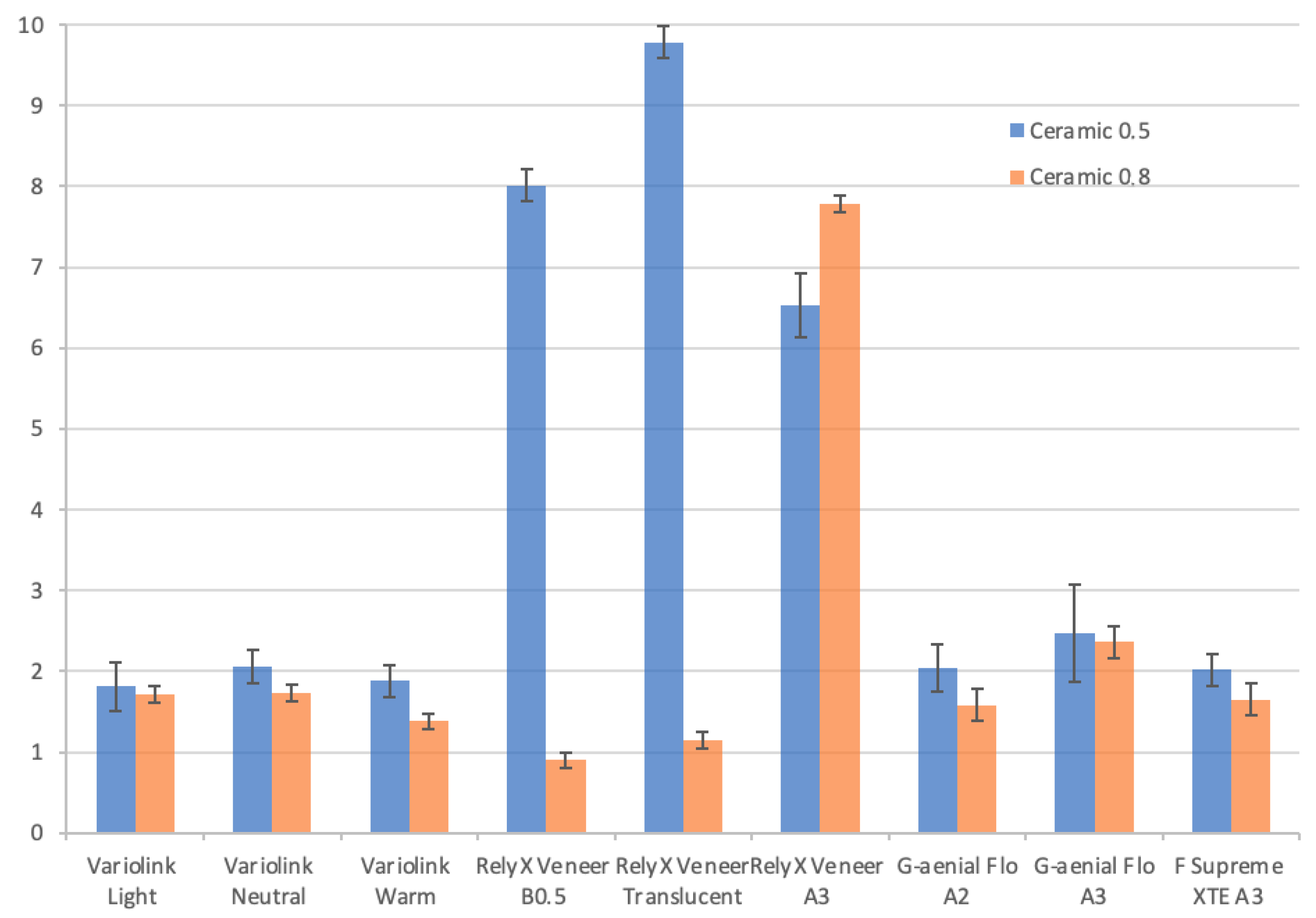
| Variolink Light | 1.81 × 106 ± (3 × 105) B | 1.71 × 106 ± (1 × 105) E | 0.361 |
| Variolink Neutral | 2.06 × 106 ± (2 × 105) BC | 1.73 × 106 ± (1 × 105) E | 0.005 |
| Variolink Warm | 1.88 × 106 ± (2 × 105) B | 1.38 × 106 ± (1 × 105) CD | <0.001 |
| RelyX Veneer B0.5 | 8.01 × 105 ± (2 × 105) A | 8.99 × 105 ± (1 × 105) AB | 0.296 |
| RelyX Veneer Translucent | 9.78 × 105 ± (2 × 105) A | 1.15 × 106 ± (1 × 105) BC | 0.072 |
| RelyX Veneer A3 | 6.53 × 105 ± (4 × 105) A | 7.78 × 105 ± (1 × 105) A | 0.442 |
| G-aenial Flo A2 | 2.04 × 106 ± (3 × 105) AC | 1.58 × 106 ± (2 × 105) DE | 0.003 |
| G-aenial Flo A3 | 2.47 × 106 ± (6 × 105) C | 2.36 × 106 ± (2 × 105) F | 0.630 |
| F Supreme XTE A3 (preheated) | 2.02 × 106 ± (2 × 105) BC | 1.65 × 106 ± (2 × 105) DE | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, J.S.d.C.; Reis, J.A.; Martins, F.; Maurício, P.; Fuentes, M.V. The Effect of Feldspathic Thickness on Fluorescence of a Variety of Resin Cements and Flowable Composites. Appl. Sci. 2022, 12, 6535. https://doi.org/10.3390/app12136535
Pereira JSdC, Reis JA, Martins F, Maurício P, Fuentes MV. The Effect of Feldspathic Thickness on Fluorescence of a Variety of Resin Cements and Flowable Composites. Applied Sciences. 2022; 12(13):6535. https://doi.org/10.3390/app12136535
Chicago/Turabian StylePereira, Joana Santos de Cunha, José Alexandre Reis, Francisco Martins, Paulo Maurício, and M. Victoria Fuentes. 2022. "The Effect of Feldspathic Thickness on Fluorescence of a Variety of Resin Cements and Flowable Composites" Applied Sciences 12, no. 13: 6535. https://doi.org/10.3390/app12136535
APA StylePereira, J. S. d. C., Reis, J. A., Martins, F., Maurício, P., & Fuentes, M. V. (2022). The Effect of Feldspathic Thickness on Fluorescence of a Variety of Resin Cements and Flowable Composites. Applied Sciences, 12(13), 6535. https://doi.org/10.3390/app12136535