1. Introduction
Radiation-based imaging has played an important role in the development of medical technology. After Röntgen discovered X-rays in the 19th century, researchers were given insight into the internal structure of the human body. The development of two-dimensional (2D) radiographic imaging has provided clues about the unique structures of the human body, and three-dimensional (3D) computed tomography (CT) has provided tools for non-invasively observing the interior of the human body in 3D form. This development has significantly contributed to the advancement of medical diagnostic skills.
Image-guided surgery uses medical imaging technology to develop diagnostic and interventional technologies [
1]. Radiographic imaging is one of the most commonly used imaging modalities for image-guided surgery, providing physicians with live positional information. As such, it plays an important role in the accuracy and safety of the operation [
2]. Importantly, image data distortion must be minimized to ensure the accuracy of image-guided surgery, which necessitates accurate knowledge of the geometric information corresponding to the imaged volume and the development of an image-guided surgical system. Vascular intervention using angiographic imaging represents one of the clinical applications of the image-guided approach. In this procedure, a catheter is inserted into the patient’s body and fed in the desired direction [
3]. When the catheter reaches its destination, it can be maneuvered to remove sediment from the vessel or insert a mesh-type structure to widen the narrowed vessel, or even inject therapeutic drugs. The medical staff can track the catheter’s location during these procedures using 2D radiographic imaging, and 3D Cone-Beam CT (CBCT) is only used as an auxiliary means of helping determine and guide the catheter location. This necessitates the development of techniques for intuitively determining the 3D location of the catheter using the spatial relationship between 3D CBCT data and 2D radiographs taken repeatedly during the procedures. There are some existing approaches to estimating the 3D position of the catheter by utilizing the image registration techniques of 2D radiographic imaging and 3D CBCT data. Calculating the precise location of the catheter necessitates precise calibration of the projectional geometry of the radiographic imaging device, which is essential for the implementation of 2D and 3D image registration techniques.
Therefore, previous studies have been conducted to accurately calculate the geometric information of the imaging device and improves the accuracy of the registration between the 2D and 3D CT images based on this information. Consequently, the findings of this study contribute to the advancement of this work by improving the accuracy and stability of image-guided surgery. The accuracy of the geometric parameters of the imaging device that acquires the image data influences the accuracy of registration between the 2D radiographic image and the 3D CT data. Image registration with inaccurate geometric parameters cannot guarantee high accuracy, which negatively impacts the accuracy and stability of image-guided surgery. Therefore, several groups are also interested in improving the calibration accuracy of the projectional geometry of the imaging device to improve the accuracy of the registration and ultimately guarantee the safety of the image-guided surgical system. Calibration techniques for radiographic systems have been studied as methods for calculating the geometric information of radiographic images using a calibration phantom [
4,
5,
6,
7]. The phantom-based calibration method requires several radiographic images of a phantom that employs ball bearings to establish accurate locations at multiple angles. The geometric parameters of the system are then calculated using the spatial relationship between the 2D images acquired by the imaging device and the known 3D spatial fiducial markers of the phantom calibration model. Kohei Sato et al. proposed an algorithm for estimating the geometric parameters of the system by attaching calibration markers to the X-ray source housing [
4]. When the X-ray images are acquired, the calibration markers are always presented with the objects. However, such markers can introduce noise and scattering effects and can act as physical obstacles that prevent the accurate diagnosis of a patient. J. Chetley Ford et al. proposed an algorithm to improve and verify the accuracy of CBCT geometric parameter estimation by performing additional calibration with the results of the initial calibration [
5]. Calibration errors caused by phantom tolerance were corrected during the calibration procedures in their study. C. Fragnaud et al. also proposed a calibration method that uses a Computer-Aided Design (CAD) model to estimate the initial projective model of the X-ray device and then compute the real projective parameters by comparing the projective model from X-ray images with the CAD-based projective mode [
8]. There have also been efforts to improve calibration accuracy with a new calibration phantom design. V. Nguyen et al. devised a low-cost method for creating a calibration phantom [
7]. The goal of their research was to devise a method for creating a phantom using lightweight and inexpensive LEGO blocks. Consequently, the calibration phantom could be easily and cheaply designed and built for clinical applications. J. da Silva et al. proposed a paddle-wheel type phantom for cone-beam CT geometric calibration [
9], and V. Nguyen reported geometrical calibration results using a new phantom with a cylindrical shape and then embedding fiducial markers on the body. The calibration using the new phantom improved the accuracy compared to traditional designs. In addition, Hui Miao et al. used Singular Value Decomposition (SVD) to calculate the geometric parameters of the radiographic system [
6]. Although their study proposed an approach similar to that in this study that applies SVD [
10,
11] to the calibration of the radiographic imaging device, their work had a limitation in the degree of freedom of the geometric parameters. Furthermore, the approach proposed herein can be applied to the same device when provided with known geometric parameters.
Previous research presented efforts to improve the geometric calibration of the X-ray imaging device using a calibration pattern fixed to the X-ray source and providing an algorithm to calibrate the geometric parameters. Furthermore, some studies proposed a low-cost, easily manufactured calibration phantom. These studies, however, had several limitations. When a calibration pattern is attached for calibration, the markers on the calibration pattern can sometimes occlude the patient’s lesion. This usually makes diagnosis of the patient’s disorder difficult. In addition, for calibration, the calibration algorithms typically acquired a single or several projectional images of the phantom. Although they showed promising calibration accuracy, it was challenging to maintain calibration accuracy along the various orientations of the C-arm X-ray gantry. This study was designed and conducted to overcome such limitations and improve the calibration accuracy along various orientations of the C-arm X-ray gantry.
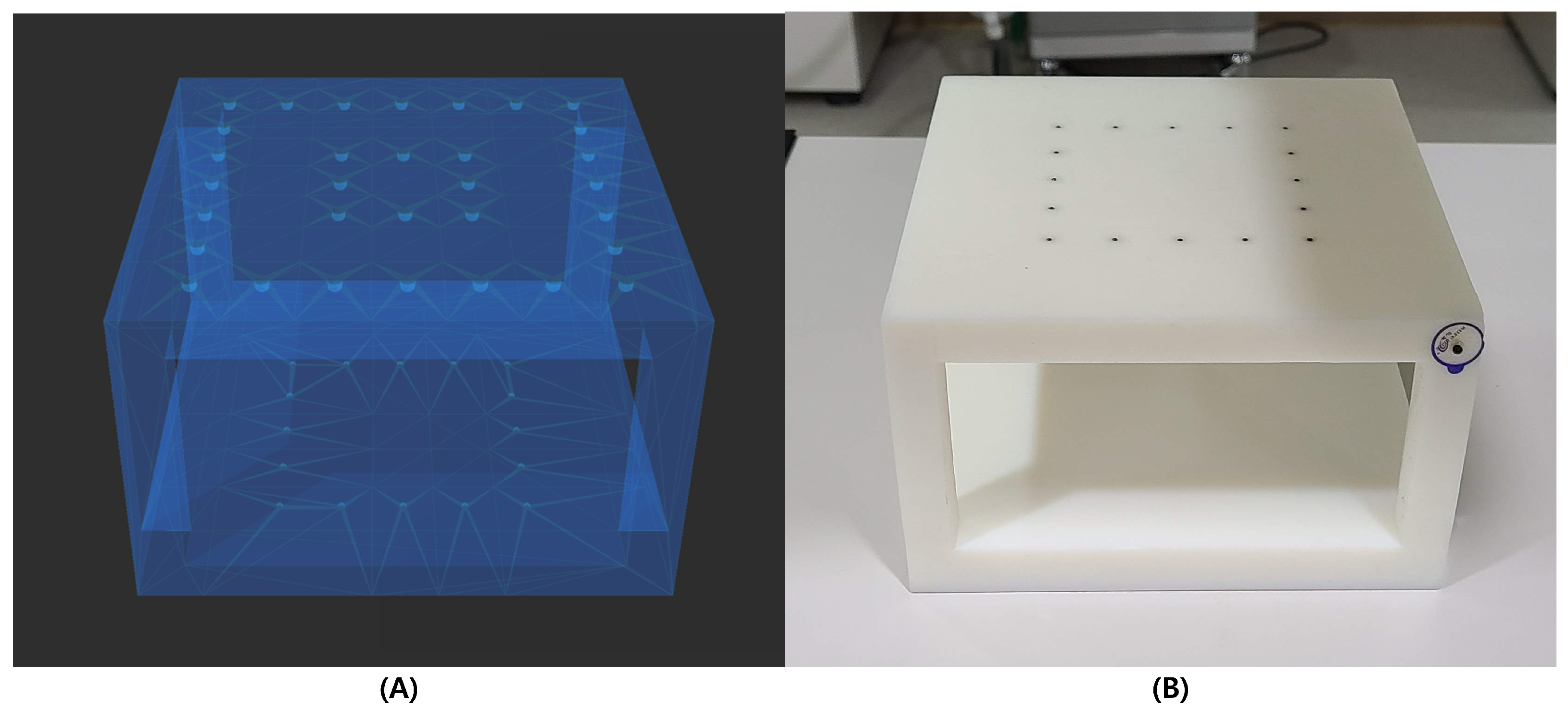
This study aims to develop a projectional geometry calibration method for radiographic use, which is essential for performing registration between 2D radiographic images and CBCT data acquired intraoperatively during an image-guided angiographic intervention. The clinical target of this study is a C-arm angiographic imaging device that has been used in vascular intervention procedures and is equipped with CBCT imaging capabilities. While operating the CBCT, this device can provide sinogram data and radiographic image data with multi-directional projection images at various angles, which are then used to reconstruct 3D CT volume data. The significance of this study is in the calculation and application of the geometric parameters of radiographs required for image-guided vascular intervention procedures using the sinogram data obtained during CBCT acquisition in the intervention room. Herein, we aim to improve the accuracy of the calibration method using sinogram data acquired during the interventional procedures without any additional radiation exposure and any significant increase in the computational time. We attempted to obtain robust calibration accuracy along various orientations of the X-ray gantry using sinogram data and only one calibration procedure. Furthermore, we did not want to permanently fix any calibration pattern to obtain a clear object without using any additional calibration markers. A calibration phantom with ball bearings to establish accurate 3D locations was designed for this purpose, and is used before surgery to calibrate the geometry of the X-ray imaging device. This study also focused on executing the calibration method in under a minute, which is an acceptable calculation time for image-induced vascular intervention, and within a 1 mm accuracy.
4. Results
In the experiments, ten parameters were computed for the geometrical calibration of X-ray projectional imaging, including the SDD, position and orientation of the phantom, and position of the isocenter. The sinogram and 2D projectional X-ray images were obtained, and the evaluation procedures were followed using the software application developed in this study.
Three different methods were used to analyze the results. First, the accuracy of the calibration method was assessed using the angular range of the sinogram data used in the calibration. As shown in
Figure 8, the calibration algorithm was executed under a variety of data size conditions, with the data set ranging from −15 to 15 to −60 to 60, increasing 10 degrees at each step. The results are presented in the orange bar graph of
Figure 8, which shows that the operation with a wide range of data provided improved accuracy. If the data are wider than the angle from −40 to 40, the accuracy of the calibration was stable, and further improvement could not be detected. However, as the range of the data increased, so did the computational time for the calibration algorithm, as shown in the blue plot in
Figure 8.
Second, the accuracy of the calibration method was assessed using the data intervals applied to the calibration algorithm. The calibration method was followed in several conditions with different angle intervals but with the same angular range applied to the algorithm, as shown in
Figure 9. As illustrated with the orange bar graph in
Figure 9, the narrower the angular interval, the smaller the error. The improvement in the error was not dramatic but gradual. Furthermore, as the angular interval widened, the calculation time decreased, which is indicated by the blue plot in
Figure 9.
We also tested the robustness of our method by projecting the 3D positions of the fiducial markers into various angles based on the rotation of the C-arm gantry and calculating the mean error between the projected fiducial positions and the centers of the fiducial markers in the sinogram projection image. Calibrations were performed under five different conditions, as shown in
Figure 10, with angular ranges ranging from −20 to 20 degrees, −30 to 30 degrees, −40 to 40 degrees, −50 to 50 degrees, and −60 to 60 degrees. Based on the results of each trial with different conditions, the 3D fiducial positions were projected into all of the projected images that belong to the sinogram. As illustrated in
Figure 10, the evaluation result of the calibration with sinogram data with a range of −20 to 20 degrees shows the worst accuracy. The accuracy improved by broadening the data range used by the calibration algorithm. Furthermore, as the angle moved away from 0 degrees, the projectional errors in each trial increased, and the gradient became much larger in the rotation angle outside of the range of the data used for calibration. In addition, the wider the angle range, the better the accuracy of the projectional error. Moreover, the gradient is much less for the results with a narrower data range.
5. Discussion
We conducted phantom experiments and analyzed the experimental results using three different methods to evaluate our calibration method. First, we assessed the accuracy of the calibration method using a variety of data range conditions applied to the calibration algorithm. Calibrations were performed using different ranges of sinogram data, and the results are shown in
Figure 8. The results show that a wider range of sinogram angles could guarantee improved accuracy compared to a narrower range of data or a single image from one angle. Although a broader range of data yields higher accuracy, it also necessitates more computational time. As shown in the blue plot of
Figure 8, by increasing the range of the data, the computational time also increases significantly. However, the accuracy with different data ranges shows that there are no significant differences in accuracy if the data range is wider than −40 to 40 degrees. Therefore, when considering the required computational time, the range between −40 and 40 degrees is an optimized range of data for calibration.
Second, we assessed how much the data interval affected the accuracy. The calibration algorithm’s accuracy was tested with intervals ranging from 0.4 degrees to 3.2 degrees over the same angular range.
Figure 9 depicts the evaluation results, which show that the interval of the sinogram data applied to the algorithm affects the accuracy less than the range of the sinogram data. As shown in
Figure 9, the results show no trend of decreasing accuracy as the data interval is increased. The computational time, on the other hand, can be reduced by reducing the amount of data and increasing the interval of the data using the same angular range. Although the data size is reduced linearly by increasing the interval of the data linearly, the computational time is not reduced linearly. This is because the data loading time is involved in the computational time. By reducing the data size (by increasing the interval), the percentage of the loading time relative to the entire computational time is increased. Consequently, the computational time can be reduced by selecting a larger interval, as shown in
Figure 9. Given the accuracy and computational time constraints, an interval of 1.6 degrees can be considered an optimized interval for the data used by the calibration algorithm.
Finally, the robustness of the algorithm was evaluated based on the results with various data ranges by projecting 3D fiducial markers of the phantom to each projectional image of the sinogram and comparing the error between the projected coordinates and the center of the fiducial marker region in each image slice of the sinogram. As shown in
Figure 10, the condition that applies a wider range of sinogram data to the algorithm outperforms that with a narrower range. Furthermore, the shape of the plot is similar to the parabolic shape of the quadratic polynomial with a minimum value near 0, and errors increase as the rotation angle of the C-arm gantry increases in both directions within the range. The accuracy of the calibration presented errors below 1 mm within the method’s range, whereas the errors are much larger outside of the range, particularly for the ranges of −20 to 20 degrees and −30 to 30 degrees. For the wider range of −40 to 40 degrees, the overall accuracy is below 1 mm. The plots in
Figure 10 are asymmetric due to the rotational error of the C-arm gantry. If the rotational motion of the C-arm gantry is pure, the error would demonstrate a symmetric pattern. However, since the rotational motion has some errors during the rotational operation of the C-arm gantry in a real situation, due to the vibration or bias of the rotational center of the C-arm, the error pattern is not perfectly symmetric.
6. Conclusions Furthermore, Future Work
This study aims to create a calibration method that can be used in the intervention theater immediately prior to a vascular intervention procedure. Furthermore, it aims to improve the accuracy of the calibration method using sinogram data acquired during the CBCT imaging process. In other words, the goal of this study is to create a calibration method that ensures the safety of the vascular intervention procedure and executes within the acceptable computational time for the image-guided vascular intervention room without exposing the patient to any additional radiation.
The proposed method is a phantom-based calibration technique that uses sinogram data to compute ten geometric parameters of the imaging device. By comparing and evaluating the calibration accuracy across various angular ranges and interval conditions, the optimal angle range and interval are proposed. Consequently, the optimal calibration conditions considering the calculation time and accuracy were found to be an angular range from −40 to 40 degrees, with an optimal angular interval of 1.6 degrees. Therefore, a calibration method with an operation time of 2.92 s and a mean error of 0.36 mm could be achieved, thus satisfying our goal of below 1 mm accuracy within a minute computational time. We plan to conduct additional research in the near future to apply this calibration method to a robotic system for vascular intervention.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









