1. Introduction
Despite the important number of patients affected every year (A World Health Organization report estimates the lifetime prevalence of non-specific low back pain (LBP) at 60 to 70% in industrialized countries [
1]), few authors have investigated the mechanisms of the action of lumbar belts. These devices are part of a large series of care strategies for LBP and several clinical trials showed their clinical efficacy [
2,
3]. However, their mechanical effects remain unclear and, consequently, it is almost impossible to propose an optimized belt design.
Many studies found in the literature dealt with braces for scoliosis correction. Beauséjour et al. [
4] proposed a link between brace wearing, interface pressure, and spine correction using the posture changes as a landmark. Munoz et al. measured the local intervertebral disk geometry with a low-dose radiation X-ray [
5] or fluoroscopy [
6] while wearing a belt, which demonstrated and quantified the spine posture changes induced by the medical device.
Calmels et al. [
2] studied the efficacy of lumbar belts by assessing the improvement of functional capacity, pain reduction, and drug consumption of 197 patients over 90 days. Two randomized groups were formed: one group wore the belt (Lombacross
® Activity, Thuasne, France) and the other one was the control group. Both groups were allowed to use medication to help reduce pain. Three check-ups for each patient were done: the first one on the day of inclusion in the study, the second after 30 days, and the last after 90 days. Functional capacity was assessed by the EIFEL score, pain intensity was measured by a visual analogical scale, and medical consumption was counted as the number of days the patients were taking pain killers (analgesics, NSAID, and/or myorelaxants). The cost of care for these patients was also evaluated [
7]. The cost per patient with a lumbar belt for 3 months was lower than that for the other group (Δ = 205.72€). This study shows that the group wearing a lumbar belt had a significant improvement of functional capacity, a significant reduction of pain intensity, and a significant reduction in medication consumption compared to the control group.
Hamonet et al. [
8] also conducted a survey about the efficacy of lumbar belts on 108 patients that used a lumbar belt for more than 30 days. It included people suffering from LBP for more than 6 months. They did not have any criteria regarding age, sex, associated pathology, or context of pain. The lumbar belts used were Lombacross
® (Thuasne, France), Lombax
® (Thuasne, France), and Lombacross
® Activity (Thuasne, France) or others (11%). The belts were worn for 1 month up to more than a year and were used daily (50%), often (32%), or occasionally (18%). The results are that 92% of the patients considered the belt to have good or very good efficiency; though there were some reports of discomforts (heat, bloating, difficulty to seat), 77% of the patients had a good tolerance.
The way lumbar belts reduce pain is not well-known. Studies were conducted to better determine the effect of the belt on patients. Lumbar belts might reduce lumbar motion and, therefore, decrease the load on some vertebras and keep the body out of any harmful position. Moreover, the friction of the belt on the skin can also activate cutaneous mechanoreceptors, improve lumbar proprioception, and restore lumbar stability. Boucher et al. [
9] studied the proprioception issues in patients suffering from LBP. They conducted a study that included 60 patients distributed into two groups: 38 patients in the LBP group and 19 patients in the control group. Patients from the LBP group answered a questionnaire (Roland Morris Disability Questionnaire) in order to evaluate their level of pain. Their lumbar instability was evaluated in 2 ways: a prone instability test (Prone IT) and a questionnaire based on 15 clinical signs of lumbar instability. There were three experimental conditions: no belt, extensible belt, and non-extensible belt. They concluded that there was no statistical difference in the variability of lumbar proprioception between the two groups. The LBP group had a worse proprioception than the control group, but the study showed “no improvement in lumbar proprioception with use of a lumbar belt for patients with LBP or for healthy control”. They also couldn’t identify sub-groups of patients with LBP for whom using a lumbar belt would be better than for the others.
In the field of engineering, the link among the textile characteristics, the belt design, the pressure applied on the trunk, and its effect on the human body and, particularly, on the spine was poorly studied—but it was proposed that the main mechanical effect of the lumbar belt is the pressure applied on the trunk; this pressure is supposed to force the patient to change his or her lumbar spinal posture (lordosis) by acting on the abdomen. Bonnaire et al. [
10] proposed a clinical study using optical methods and pressure map sensors, but the method is tedious and time consuming, and some early-stage information would be of great help for the design of new belts.
Some studies were conducted in order to identify parameters related to the performance of lumbar belts for patients. Another way of reducing pain is related to the change in posture. In the intervertebral disk, most of nerve endings are located in the posterior part, so even if many other reasons for the pain should be invoked [
11], decompressing the back part of the disk could reasonably be associated with pain relief [
12]. Muñoz et al. [
5] proposed a complete methodology to estimate and optimize the pressure distribution of the disks in the lumbar region. A bi-planar X-ray imaging system (EOS) giving the disk shape variations was associated to a Finite Elements Model of the disc and an optimization loop on the lumbar belt design. This methodology was proven to be efficient for restoring the lumbar curvature, but it is still impossible to understand the mode of action of the belt exactly and to separate purely mechanical effects and antalgic effects related to proprioception or to heat. In reality, the belt is acting on the skin, outside the body, and the medical effect is deep inside the body in the spine.
Some recent research works are oriented to compare extensible lumbar belts with non-extensible ones for trunk postural balance in a static state or for sit-to-stand movement [
13,
14]. In particular, Ludvig et al. [
15] and Anders et al. [
16] attempted to reveal the effect of lumbar belts on trunk muscle activity and lumbar stiffness.
The way the load is transmitted was studied by Bonnaire et al. [
17] in a numerical parametric study. They modelled the effect of three lumbar belts on four idealized numerical trunks of different morphologies: tall and thin, tall and large, small and thin, and small and large. Other factors were included in the study, such as the initial lordosis angle, the height of the subject, or the patient’s soft tissues behavior. The results of this parametric study showed that the choice of the belt and the patient’s morphology are governing factors in disk decompression. Surprisingly, the mechanical characteristics of the body structures have very little influence on the therapeutic treatment, except for the mechanical properties of intervertebral discs. Unfortunately, this first model only considered the global disk decompression but not the pressure variation inside a disk or other factors that should be related to the wearability and comfort. Moreover, the quality of the belt geometrical representation was poor, considering that the choice of the belt is influential. Recently, a semi-analytical approach based on real trunk shape and a more detailed belt structure has been proposed [
18]. This approach provided a first in-silico pre-clinical trial that clearly outlines the influence of morphology on belt response; it also shows that the belt structure could change the treatment efficiency. The main drawback is that the belt performance is derived from the pressure distribution—without any access to the disk pressure variation because the work is only based on external data.
The purpose of this paper is to identify some key mechanisms and/or parameters that are useful in the design of new lumbar belts. This work is based on an improved version of the model presented by Bonnaire [
19] and a set of lumbar belts representative of the French market. As a result, it is necessary to qualify the effect of the belt on the trunk using various parameters (lordosis angle, applied pressure, intervertebral disk pressure variation …), both characterizing the functional efficiency of a belt and its wearability.
Thus, the objective of this work is to study the internal effect of a set of belts that are representative of the French market. It will use the Finite Element Model developed in [
19], with specific attention to the belt description, as it has been done in [
20]. The quality assessment of the belt is a specific issue: various possible indicators will be compared and discussed. They could be used to optimize both the mechanical efficacy of the belt and attendance to the treatment of the patient. Last, key design parameters will be outlined.
2. Approaches
2.1. Belts and Morphologies
In order to verify the therapeutic and biomechanical impacts of lumbar belts on the patient, we selected four typical morphologies of patients having hyper-lordosis among the patients studied by Bonnaire [
19], and they were subsequently referred to as tall-large, tall-thin, small-large, and small-thin. The morphologic characteristics of the four chosen subjects are shown in
Table 1. The angle of lordosis of the subjects taken is 53°. These data are used for building numerical models.
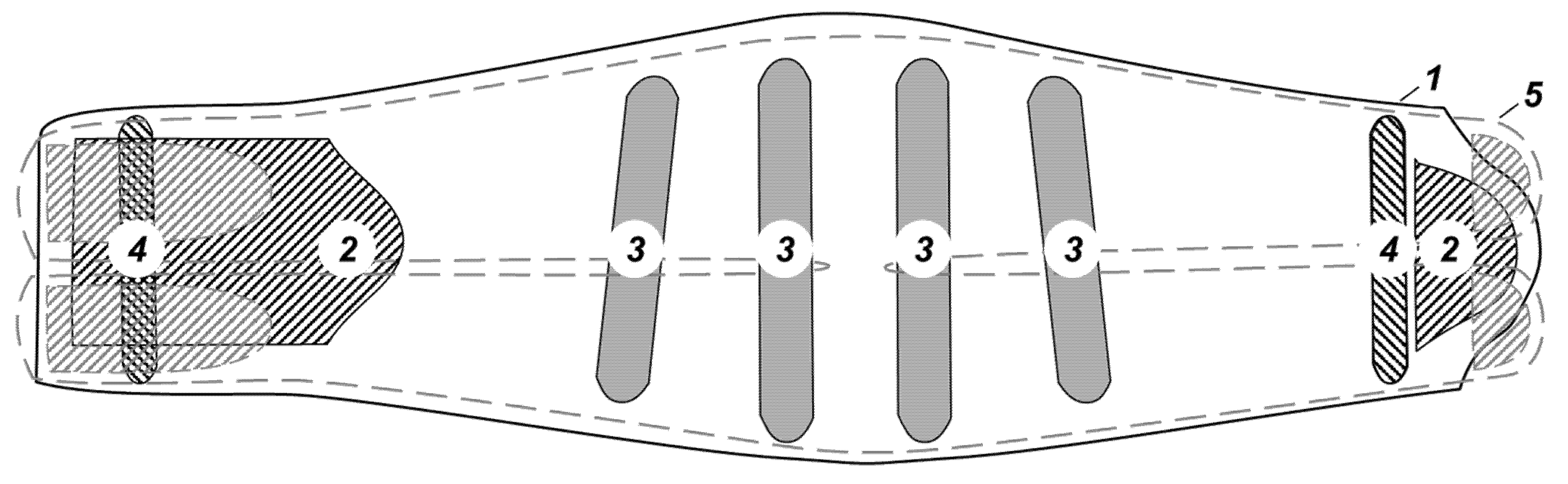
Table 2 shows the typical characteristics of lumbar belts tested in this study. The lumbar belts have the same architecture: four rigid anatomic whalebones in the dorsal element and two soft whalebones in the abdominal—corresponding to the French healthcare system recommendations [
21]—and can be considered as representative products on this market (see
Figure 1).
2.2. Modelling of Lumbar Belt’s Pressure
As a first approximation, the lumbar belt acts on the body by delivering a pressure
p proportional to the belt tension (
T1 or
T2, 1 and 2 referring to the weft or warp direction) and to the local curvature defined by its radius (
R1 or
R2), as expressed by Laplace’s law:
Then, the pressure depends on the body’s curvature, the belt geometry and stiffness, and the level of stretch applied by the user. Last, the belt placement on the body has to be carefully addressed. The body shape is extracted from the FE model, thereby calculating the curvature locally.
Belt stiffness is obtained using a tensile test according to the European standard EN ISO 13934-1:1999 with an Instron 3343 Universal testing machine. Belts are stretched 3 times up to 20% of strain, as recommended by the manufacturer. Since the patient closes the belt in a loosening phase, the stiffness is taken as the tangential slope of the strain/lineic force curve during unloading at 20% strain. This procedure is explained in more detail in Molimard et al. [
18].
The belt is stretched around the body in a way, as the mean stretch is 20%, by overlapping the two ends on the abdomen, mimicking real life. Even if the mean stretch value is 20%, local variations are taken into account by comparing the body diameter to the belt size. Considering the local equilibrium on a belt slice—seen as a beam—the mean stretch of each slice varies with the section. If the belt is made of fabric, the section varies along the belt and so does the mean stretch; if the belt is made of elastic bands, the section is constant, even if the width varies, and so the mean stretch of a section remains constant.
This approach is a simplification of a more complex situation by considering only the unidirectional loading of the belt without any transverse or shear effects. Since the material is highly anisotropic, with the shear stiffness being significantly lower than the tensile stiffness, and since there is no transverse loading, this assumption is reasonable and avoids the high complexity of solving the coupled belt/body interaction.
2.3. Positioning of Belts
The belt shape is taken into account to correctly apply the pressure produced by the belt because the belt shape and its structure are different from one belt to another. It was necessary to develop a program using MATLAB™ in order to take into account the belt shape and its stiffness in detail and to compute the pressure generated by the belt.
The belt has to also be adapted to the trunk size. Belt design is based on two fixed-sized components (back panel and front closing) and strap systems or fabrics, whose length is adapted to the trunk size. This simple principle has been numerically reproduced, allowing for a numerical adjustment of the size of a belt portion.
Finally, for each trunk, an adapted belt is placed in such a way that the centre of its back corresponds to the centre of the lumbar curvature (i.e., L3/L4 vertebrae). Sizing is validated if its initial deformation (before tensioning) is between 1% and 4%. This “slightly tight” position, which was already used in the clinical trials from [
19], avoids numerical instabilities when the belt circumference is greater than the patient’s trunk circumference. When this situation is reached, it is easy to reproduce the nominal deformation of 20%.
2.4. Numerical Simulation
Simplified 3D geometrical models of the human trunk were developed for Finite Element Analysis (FEA). These models were built using frontal and sagittal radiographies of the trunk of patients. From these radiographies, the following elements are measured:
the lateral inclination of each intervertebral endplate in the sagittal plane (°),
the height at their centre of the thoracic and lumbar vertebrae (mm),
the diameter of the vertebral anterior segment at thoracic and lumbar level (mm),
the height at their centre of the intervertebral discs in the thoracic and lumbar regions (mm),
the width of the trunk at the chest, below the chest, and at the waist and hips in the frontal plane (mm),
the thickness of the trunk at the chest, below the chest, and at the waist and hips in the sagittal plane (mm).
2.5. Extraction of Output Data
The retained indicators to interpret the results are the following.
Local indicators:
Pressure map on intervertebral discs (MPa),
Reaction forces and moments on vertebrae (N, N.mm).
Global indicators:
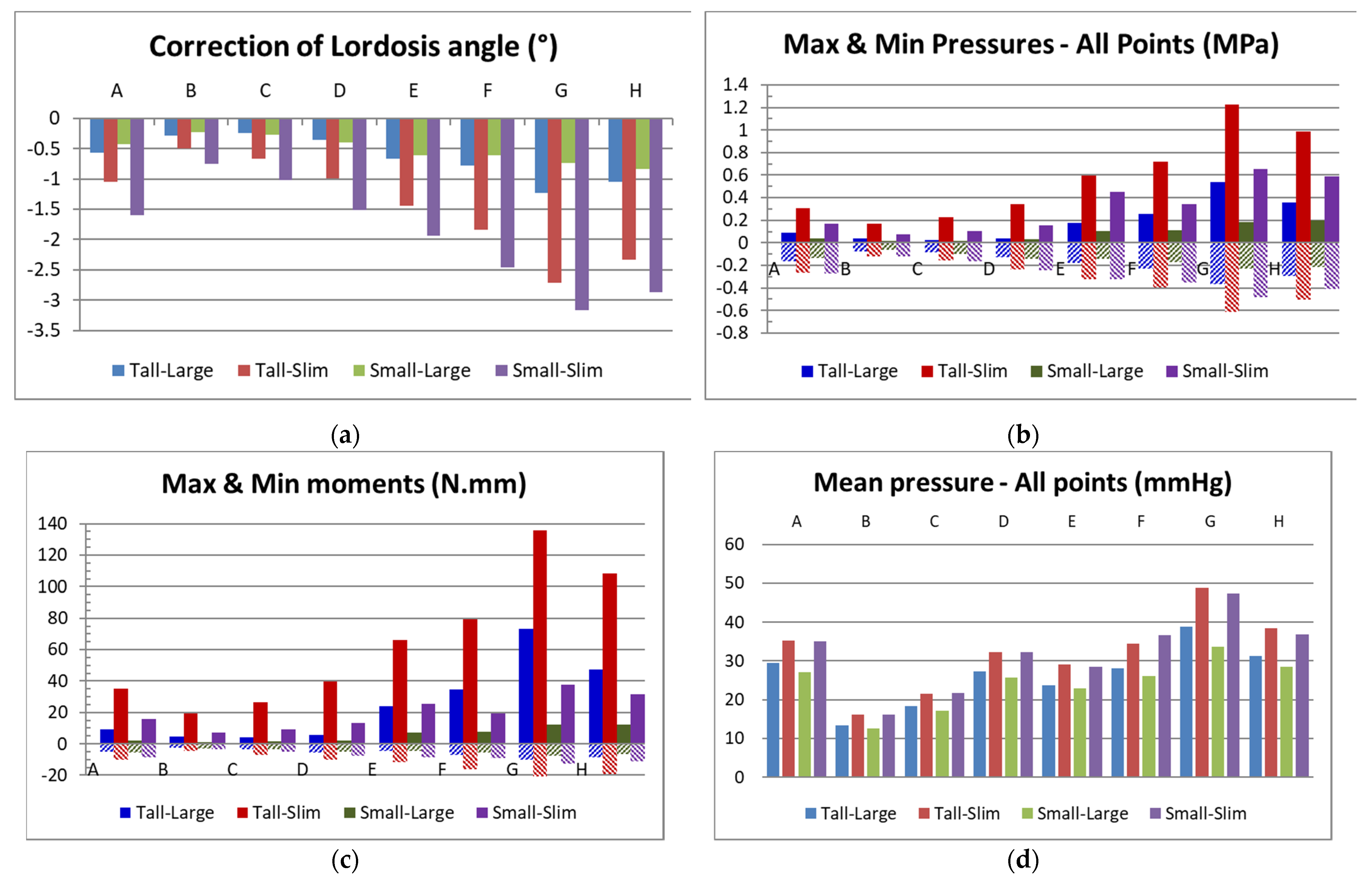
Variation of lordosis angle, defined as the angle between the upper plateau of L1 and the lower of L5 (°),
Max and min pressures on the spine (MPa),
Mean pressure on the spine (MPa),
Max and min of mean pressures on each disc (MPa),
Max and min forces and moments obtained on the vertebrae (N, N.mm).
It is important to note that the aforementioned pressure means the difference in pressure between the state without belt wearing and the state after belt wearing, while excluding all other physiological loadings, such as loadings due to gravity or movement.
Each vertebra is modelled as a cylinder based on radiographies. Lumbar lordosis and thoracic kyphosis are constructed using two circle arcs obtained by the lateral inclinations of each vertebral endplate. It is assumed that the vertebra has parallel lower and upper endplates. The posterior segment of vertebra is not represented in this model since their action is assumed to be negligible for this study. The intervertebral discs are also modelled as a cylinder with two distinct parts: a central circular part corresponding to 30% of the volume and representing the nucleus, and a peripheral part representing the annulus [
20].
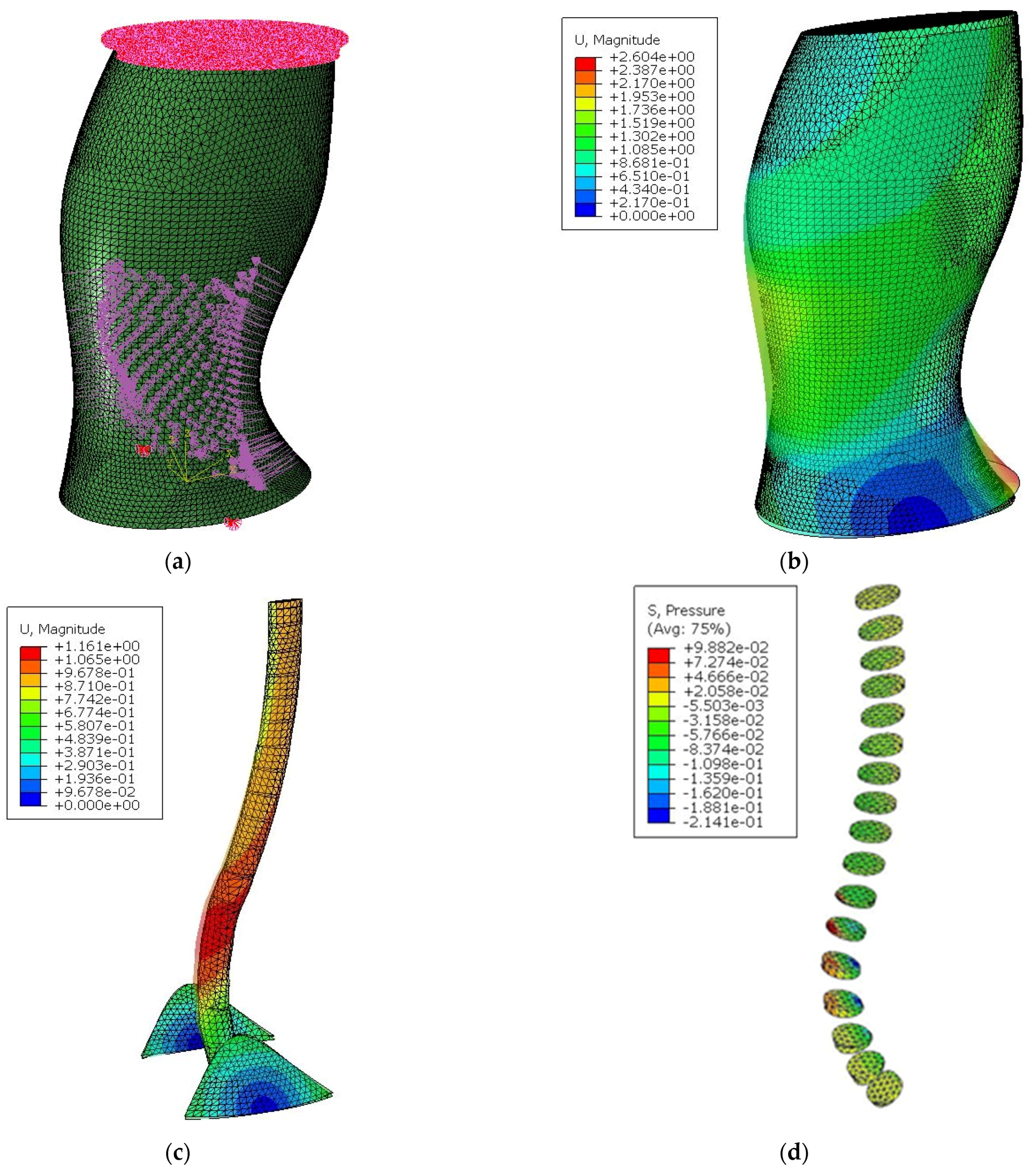
The tissues composing the trunk, except the spinal column, are divided into three zones in order to represent the abdomen, the iliac crests, and another part that includes the thorax and the soft tissues in the back zone (see
Figure 2).
The geometric model is meshed using ten-node tetrahedral second-order elements (C3D10H) in Abaqus. A static linear analysis is performed using the standard solver. To determine the appropriate number of elements, a convergence study was done with Abaqus. This study consists of determining the mean abdominal and intradiscal pressure in the lumbar region as a function of the mean size of elements [
17].
As it is shown that mechanical behaviour has a second-order influence [
17], in order to ensure FEA simplicity and for the comparative purpose, all the structures have elastic linear mechanical properties and the same value for each part.
Table 3 shows the mechanical properties of different tissues of the human body through mean values from the data taken by Bonnaire [
19].
Boundary conditions were determined in order to obtain realistic movements of the trunk when under belt application (
Figure 2h). When the patient wears a belt, the pelvis can rotate slightly relative to the transverse axis. In addition, the patient tends to straighten up. This is why the upper plate of the trunk in translation is blocked in the transverse plane. The top of the trunk can translate in the frontal plane. The lower plate of the trunk is restricted in order to enable rotation of this plate only in the transverse axis. This restriction is obtained by embedding the two points at the intersection of the ellipse, thereby representing the extremity of the lower plate of the trunk and the frontal plane of the trunk. A meshed model of the trunk and its boundary conditions are represented in
Figure 2g,h. Finally, the pressure field computed as described in the previous section was applied to the belt area.
4. Discussion
4.1. Limitation of the Model
The geometric model of the trunk is built up in a simplified way on the four idealized subjects. Therefore, the position of the spine is not precise because no medical image is available, and we cannot associate precise morphological information from the subjects (height, weight, BMI).
The application of belts to the trunk has been modelled by Laplace’s law under hypotheses: no friction between the belt and the soft tissue, and a unidirectional tensile force. On the other hand, the position and shape of the belt, its orientation, and its closure are taken into account. In addition, the presence of the straps was modelled by the additional rigidity, which could result in some error in the results.
The mechanical properties of the materials are assumed to be identical for all subjects in order to identify these variables from the analysis. Even if it was demonstrated that these parameters have a very limited influence on spinal mechanics [
17], the linear elasticity remains a strong assumption.
4.2. Correlation between Therapeutic Parameters and Mechanical Variables
According to the literature, the variation in the lordosis angle could be considered a therapeutic indicator. Nevertheless, the pressure generated by the belt at the intervertebral discs should be a direct effect for reducing back pain.
A cross-correlation analysis shows that there is a strong correlation between the variation of the lordosis angle resulting from the application of the belt and the mechanical quantities obtained at the intervertebral discs (see
Table 4). For example, the lower the absolute pressure in the vertebral discs, the greater the variation in the lordosis angle.
4.3. Morphological Influence
The pressure on the disc is generally located between L4 and T11, which are in the covered area of the belt, and its maximum value in absolute area is between L3 and T12.
The position of the maximum or minimum moment generated in each vertebra varies according to the morphology. However, we can see the moment that the direction of the vertebrae changes radically from one vertebra to another. For example, in the tall-large case, this moment change is localized between L1 and T11, but in the tall-thin case, it is between T12 and T10, which is shifted slightly upwards. The application of the minimum moment—the most delordosing—is almost not dependent on the belt, but varies according to the trunk. The overall geometry of the patient seems to be the key factor here, but it is necessary to test more different cases (patient-types, belts, position of the belt) to draw a clearer conclusion.
4.4. Influence of Lumbar Belts
A lumbar belt can act on the body in three different ways: its global stiffness, its shape, or the component arrangement.
The pressure being proportional to the tension, and given that the belt stretch is fixed, it should be directly proportional to the stiffness. Here, the results show a high correlation between mean pressure and stiffness (R2 = 0.999). On the other hand, the correlation with the maximum pressure was low—quantified using the last quintile (R2 = 0.328). The fabric-based belts have a pressure variation—and consequently a maximum pressure—twice that of the textile-band-based belts. This result remains valid for all the morphologies, except for the small-large morphology, where the belt design has almost no influence on the pressure peak. This last situation can be explained by a change in the localization of the highest pressures: for thin subjects, the pressure peak is located on the two sides; for the fat ones, this maximum moves to the abdomen, with a shape ratio giving more pressure variations for the small/fat subject. Even if no clinical proof can support this assumption already, we can imagine that the maximum pressure has an incidence on the belt’s comfort and possible trouble, thus the patient compliance should be better with textile-band-based belts. It is much more difficult to conclude on the design parameters’ influence on the lordosis angle.
The design parameters and the global stiffness are correlated, but a multivariate analysis is not powerful enough to give a result. Indeed, this outlines the importance of body shape on the pressure generation first, and, secondly, on the lordosis angle variation.
As a partial conclusion, the design parameter (fabric-based or band-based) has a significant influence on the comfort (using maximum pressure index), but not on the postural efficiency (using the lordosis angle index).
As explained earlier, it is possible to assume that the pressure peak ratio is related to the wearability and that the lordosis angle variation is related to the efficiency.
Figure 7 presents a way to classify the belts according to these two main directions. In order to achieve a presentation as independent of body shape as possible, a relative efficiency is obtained by dividing the angle variation by the mean value of each case.
Therefore, efficient belts should have the following characteristics:
A max/mean pressure index as small as possible
A relative angular variation as big as possible
An area as small as possible, meaning that the belt has a behavior as independent as possible of the patient’s morphology.
Using these criteria, belts A, B, C, and D (all band-based design) have a rather limited efficiency, but with a very good wearability and a high adaptability to the patient’s morphology. E, F, and G have a more unstable behavior, all having a higher-pressure peak ratio. Finally, belt E should be considered as a good choice, its efficacy being significantly higher than the others while keeping a good wearability index.



 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}