1. Introduction
Automated analysis of surgery videos has been indispensable for collecting information about surgery. Combined with computer vision and machine learning, it can improve performance and contribute to enhancing surgical safety and efficiency. A great deal of attention to surgical video analysis has sparked active research in the medical computer vision community.
Most research on surgery video analysis has been conducted in the area of minimally invasive surgery (MIS) and cataract surgery. MIS has especially gained great attention, and many tasks have been proposed to analyze surgery, such as workflow analysis [
1], phase recognition [
2], type recognition [
3], video segmentation [
4], and video summarization [
5].
Here, we focus on surgical tool detection, which can provide an estimation of the identification and position of each surgical tool that appears in a frame (
Figure 1). This task is fundamental for recognizing the surgical scene. It can be used for a lot of downstream applications, such as tool tracking [
6,
7,
8], tool pose estimation [
9,
10,
11], prediction of the remaining surgery duration [
12], and surgical technical skill assessment [
13]. Surgical tool detection has also been well investigated in MIS [
13,
14,
15,
16] and cataract surgery [
17] as there are various datasets available in public.
However, tool detection in the open surgery field has been limited because of the dataset collection and privacy-preserving costs. In MIS and cataract surgery, the surgeon sees the surgery through an endoscope camera, and videos can be easily recorded. The recordings only include surgical fields and tools and do not contain information that may identify individuals. This enables large and well-annotated datasets in MIS [
18,
19,
20] and cataract surgery [
17]. On the other hand, in open surgery, the surgeon sees the surgery with their own eyes. Thus, head-mounted cameras or cameras in the operating room are needed for recording videos. The recordings may include surgeon and patient faces and information that may identify individuals. Thus, the datasets annotated for open surgery are small and often collected in simulations [
21,
22,
23], which is difficult to be transferred for use in real-world surgery. Moreover, the computer vision task in open surgery has challenging inherent properties: varied number and roles of people (e.g., surgeons, anesthesiologists, perfusionists, nurses), the complex interaction of tools and hands, various operative environments, and lighting conditions. Hence, a diverse and large-scale dataset is indispensable.
In this paper, we introduce a large-scale egocentric open surgery dataset that contains densely annotated bounding boxes and their categories of tools. Compared with the conventional open surgery dataset for tool detection [
22,
23,
24,
25], our dataset contains a tremendous number of annotated frames and is captured at an actual surgery scene. The exampled images in the dataset are shown in
Figure 1. Our data were collected by six surgeons in real-world open surgery at our university’s school of medicine. We recorded 15 videos of seven different types of surgery. Different from MIS and cataract surgery, there are several choices of the recording viewpoint (e.g., view from the head-mounted camera, the camera attached to the light [
26], the surveillance camera). We choose a first-person view as the viewpoint of recording because the data from an egocentric viewpoint are suitable for capturing the details during the surgery. The dataset has 15 h of recording from a camera attached to the surgeon’s head, densely annotated bounding boxes, and the corresponding category of the surgical tool. In total, there are 19,560 frames with the bounding boxes of the 31 categories, which is relatively large-scale compared to conventional open surgery datasets.
We provide an extensive evaluation of the conventional object detection methods that have been trained with our proposed dataset. Because only a few prior works have tackled object detection with large-scale open surgery datasets, we employ two well-known object detection methods—Faster R-CNN [
27] and RetinaNet [
28] —with different backbones.
2. Related Work
2.1. Surgical Tool Detection in Mis and Cataract Surgery
Surgical tool detection has been worked on using various approaches. These include sensor-based methods such as radiofrequency identification (RFID) [
29] or endoscopic image-based methods. The most conventional image-based methods rely on the defined handcrafted features, such as color [
30,
31], gradient [
32], and texture [
33].
With the rapid development of convolutional neural networks (CNN), most surgical tool detection algorithms started to utilize deep learning techniques. Twinanda et al. [
18] introduced a baseline model called EndoNet that performs both tool presence detection and phase recognition tasks in a multi-task manner. Choi et al. [
14] employed the YOLO architecture [
34], which can directly predict the location of tools as a representation of the boundary box in real-time but has no outstanding accuracy. Sarikaya et al. [
15] utilized a region proposal network and a multi-modal two-stream convolutional network for the surgical tool detector. Kurmann et al. [
9] proposed a U-Net architecture-based model performing tool detection and 2D pose estimation jointly. A. Jin et al. [
13] achieved high detection accuracy using a region-based CNNs (R-CNNs) [
27].
Moreover, many approaches that consider the long-term temporal information and model the temporal dependency between the frames have been proposed. Particularly, a method combining CNN with a recurrent neural network (RNN) has been a trend [
6,
35,
36]. Al Hajj et al. [
36] applied a CNN-RNN model to detect a tool used in the surgical videos; they employed a boosting mechanism instead of end-to-end training. Nwoye et al. [
6] developed an end-to-end approach composed of CNN + convolutional LSTM (ConvLSTM) neural networks that can perform tool presence detection and tool tracking using tool binary labels. Wang et al. [
37] proposed taking advantage of both 3D CNNs and graph convolutional networks (GCNs) for tool presence detection, thereby considering the relationship between tools. Y. Jin et al. [
38] presented a multi-task recurrent convolutional network with correlation loss (MTRCNet-CL) for tool presence detection and surgical phase recognition.
2.2. Computer Vision Research in the Open Surgery Domain
A small body of research exists in the open surgery domain. Most works have been related to recording techniques. Shimizu et al. [
26] proposed a novel surgical recording system using multiple cameras mounted on a surgical lump where computer vision-based region segmentation and recognition techniques are applied to automatically select the camera with the best view, hence producing a single video without occlusion. Hachiuma et al. [
39] improved this camera selection algorithm using CNNs. Saito et al. [
40] presented self-supervised learning for camera selection by taking advantage of a first-person view. Yoshida et al. [
41] estimated the incision scenes in long-duration open surgery videos using learning gaze speed, hand movements, number of hands, and background movements in egocentric surgical videos.
Few studies have focused on research related to surgical tool detection in open surgery videos [
22,
23,
24,
25,
42]. Ref. [
42] performs operating hands detection and tracking in open surgery videos. Ref. [
24] proposed detecting two similar surgical tools using hand information in an open surgery video recorded by an egocentric camera. Basiev et al. [
22] performed surgical tool detection using a multi-camera setting that can help prevent the surgical tool from being totally invisible in open surgery videos, where occlusion often occurs. In the same approach as MIS, the multi-task framework has been often utilized in open surgery video analysis. Goodman et al. [
25] proposed a multi-task network for action segmentation, tool detection, hands detection, and hand pose keypoints estimation. Goldbraikh et al. [
23] proposed a multi-task network that solves both tool localization and tool hand interaction detection task.
2.3. Surgical Dataset
Because a large-scale dataset is essential for the improvement of the data-driven deep learning algorithms, a dataset for surgical tool detection in the open surgery domain is not available; however, several datasets in other surgical domains for various tasks have been released in recent years.
Most datasets released so far are related to MIS or cataract surgery. The Cholec80 dataset [
18] consists of endoscopic videos of 80 cholecystectomy procedures labeled with phase and tool presence annotations. There are seven categories of surgical tools, including grasper, hook, clipper, bipolar, irrigator, scissors, and specimen bag. Some of the videos in Cholec 80 are included in the M2CAI16-tool dataset [
19], which consists of 15 cholecystectomy videos with ground truth binary annotations of the tools. A. Jin et al. [
13] introduced a new dataset, M2CAI16-tool-locations, which extends the M2CAI16- tool dataset with the coordinates of spatial bounding boxes around surgical tools. In the same way, Shi et al. [
43] extended the Cholec80 dataset [
18] with spatial annotations of surgical tool. ATLAS Dione [
15] consists of 99 action video clips recorded in a simulated surgical scene of 10 surgeons performing six surgical tasks on the da Vinci Surgical System (dVSS) with surgical tool annotations. The JHU-ISI Gesture and Skill Assessment Working Set (JIGSAWS) [
44,
45] was released as the first public dataset containing video and kinematic recordings of robotic surgical demonstrations, as well as gesture and skill annotations. Bawa et al. [
20] introduced the ESAD dataset for surgeon action detection in real-world endoscopic videos. This dataset is annotated with a surgical tool bounding box and its action label. The CATARACTS dataset [
17] contains 50 videos of cataract surgeries, which involves removing a clouded natural lens and replacing it with an artificial lens. Here, the presence of 21 surgical tools was manually annotated by two experts.
Recently, some datasets for open surgery video analysis have been proposed to perform object detection. Surgery hands [
42] was developed for hand detection in open surgery videos composed of publicly available videos of open surgery collected from YouTube and the annotation of spatial bounding boxes of the surgeon’s hands. Shimizu et al. [
24] recorded seven different types of actual open surgery with an egocentric camera for detecting two similar surgical tools: scissors and needle holders. Basiev et al. [
22] collected the videos taken from two different angles simulating injured open bowel repairing surgery for a tool and hand detection task. These videos contain four surgical tools: needle holder, forceps, scissors, and mosquito forceps. Another open surgery dataset is Annotated Videos of Open Surgery (AVOS), which contains 1997 videos scraped from YouTube and annotated with bounding boxes for surgical tools, including electrocautery, needle drivers, forceps, and hands, and 21 joint key points for hands and action. Goldbraikh et al. [
23] introduced a dataset recorded by the open surgery suturing simulation system and provided tool bounding box and tool and hand bounding box annotations including three surgical tools: needle drivers, forceps, and scissors. In these existing open surgery datasets, unlike ours, the videos are often collected from a simulator [
22,
23], and if the videos are collected from actual open surgery, they only provide, at most, four types of surgical tool class annotations [
24,
25].
Behavioral analysis during surgery also has many potential applications for research, quality improvement, and education. The Multi View Operating Room (MVOR) dataset [
46] is the first multi-view pose estimation dataset generated from real surgery recordings obtained in an operating room (OR) using three different views. The dataset has been manually annotated to provide both 2D and 3D upper-body poses.
3. Dataset
In this section, we present the details of the collection, annotation, statistics, and quality of the dataset, respectively.
3.1. Dataset Collection and Annotation
Because there is no dataset available that contains open surgery recordings via an egocentric camera, we record our own dataset. The actual plastic surgeries were recorded using Tobii cameras attached to the surgeon’s head. The surgeries were recorded at Keio University Hospital. Video recording of the patients was approved by the Keio University School of Medicine Ethics Committee, and written informed consent was obtained from all patients or their parents.
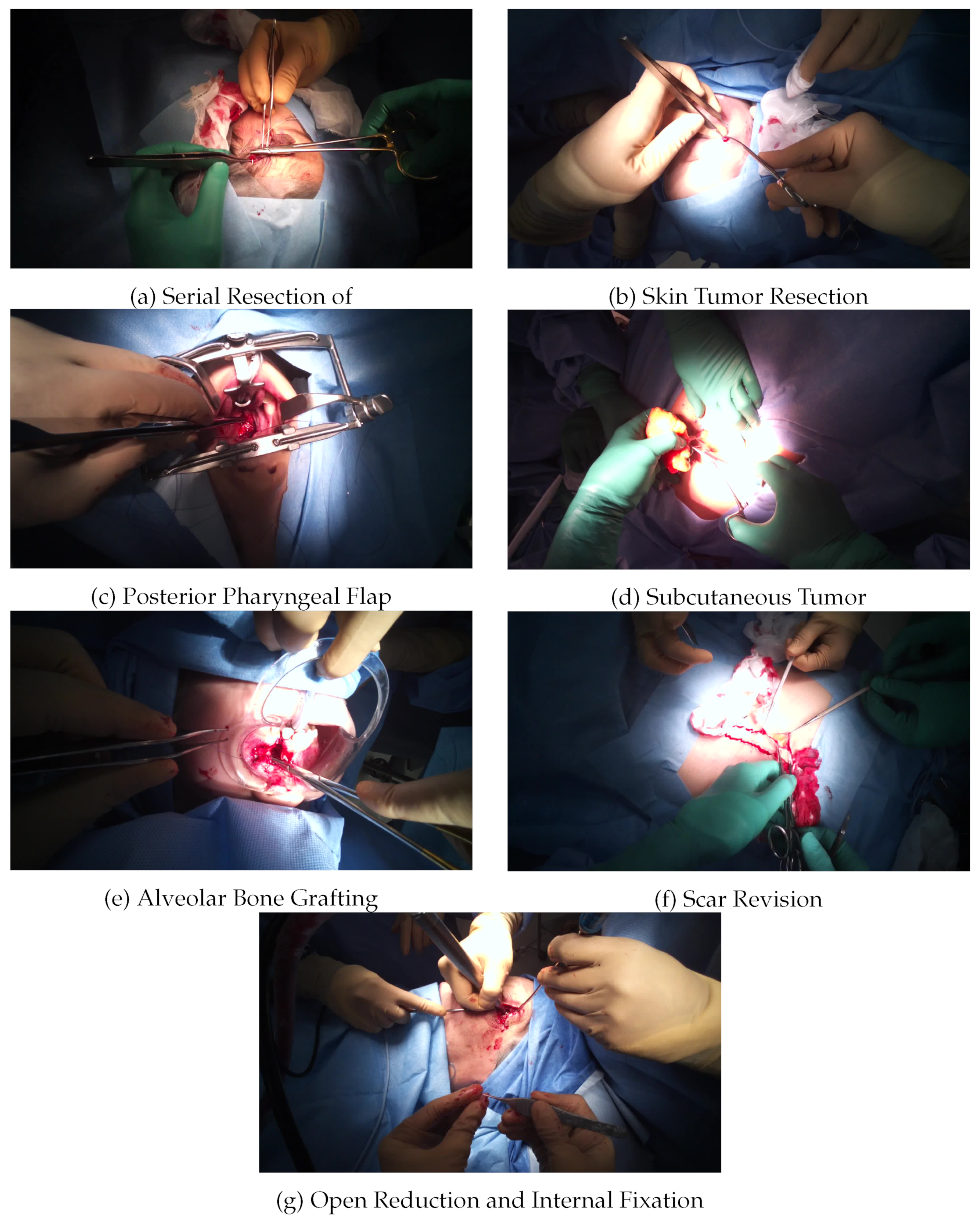
Our dataset contains 15 videos of seven different types of surgery, including serial resection of skin lesions, skin tumor resection, posterior pharyngeal flap, subcutaneous tumor resection, alveolar bone grafting, scar revision, and open reduction and internal fixation, which were performed by six surgeons. Images from each type of open surgery video are shown in
Figure 2. Each surgery video is about 30 to 90 min long and was recorded at 25 frames per second (FPS). The videos are downsampled to 1 fps for processing to avoid frames where the scene changes very little. Each instance is annotated using a bounding box and its surgical tool category label. The frame size of each video is
(pixels).
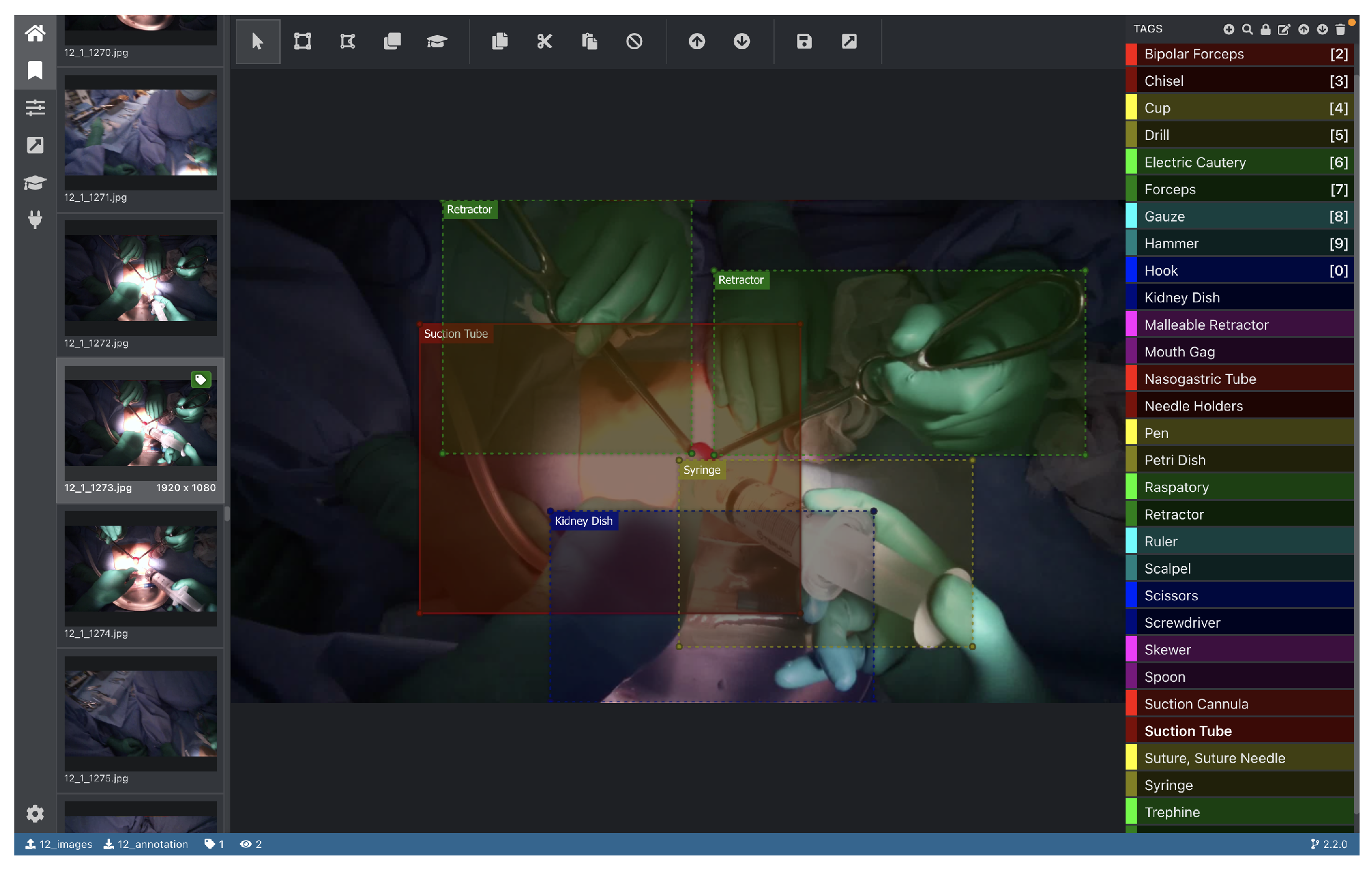
We conducted the annotation using the coordinates of spatial bounding boxes around the tools using eight graduate students in the Department of Information and Computer Science; all annotations have been examined by an expert surgeon. We used the Virtual object Tagging Tool (VoTT) for annotation. VoTT is a Microsoft open-source tool for the annotation and labeling of image and video assets. A screenshot of its graphical user interface is shown in
Figure 3.
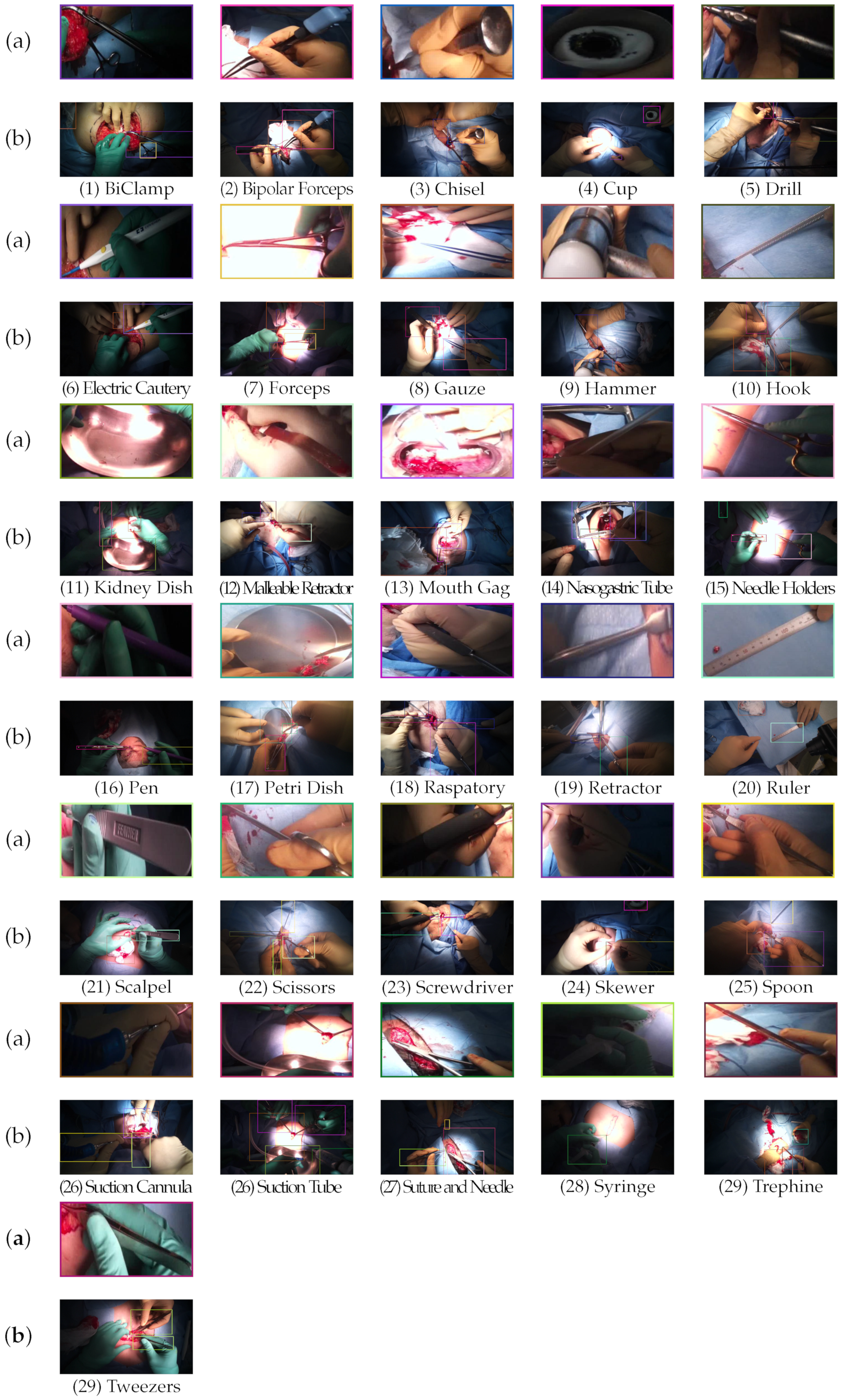
All surgical tool categories that appeared in the recording video are annotated. Then, we eliminated the surgical tool categories that appear less than 10 times. As a result, our dataset contains 31 surgical tool categories for initial annotation. The list of categories is shown in
Table 1, and examples of each surgical tool category are shown in
Figure 4. We have focused on the annotation of the surgical tool in use and excluded the annotation of the surgical tool not in use (e.g., surgical tools placed on the operating table).
Surgical tool detection in open surgery exhibits several specific features. First, in open surgery, the surgical tools are severely occluded by the surgeon’s hand or other surgical tools (
Figure 5). Second, even though there is no occlusion of the tools, it is difficult to classify the tools because some have similar shapes and textures (
Figure 6). These features make surgical tool detection in open surgery challenging.
3.2. Statistics
Based on the setting of
Section 3.1, we annotated 19,560 images among the 27,208 total frames. As a result, 13,537 instances are annotated in our dataset. The size of the dataset is comparable, and the number of annotated instances is the largest, even in the existing MIS surgical tool detection dataset, as shown in
Table 2.
3.3. Data Splits
The dataset was divided into a training set (10 videos), a validation set (two videos), and a test set (three videos). There are 12,715 images for a training set (
), 1807 images for a validation set (
), and 5038 images for a test set (
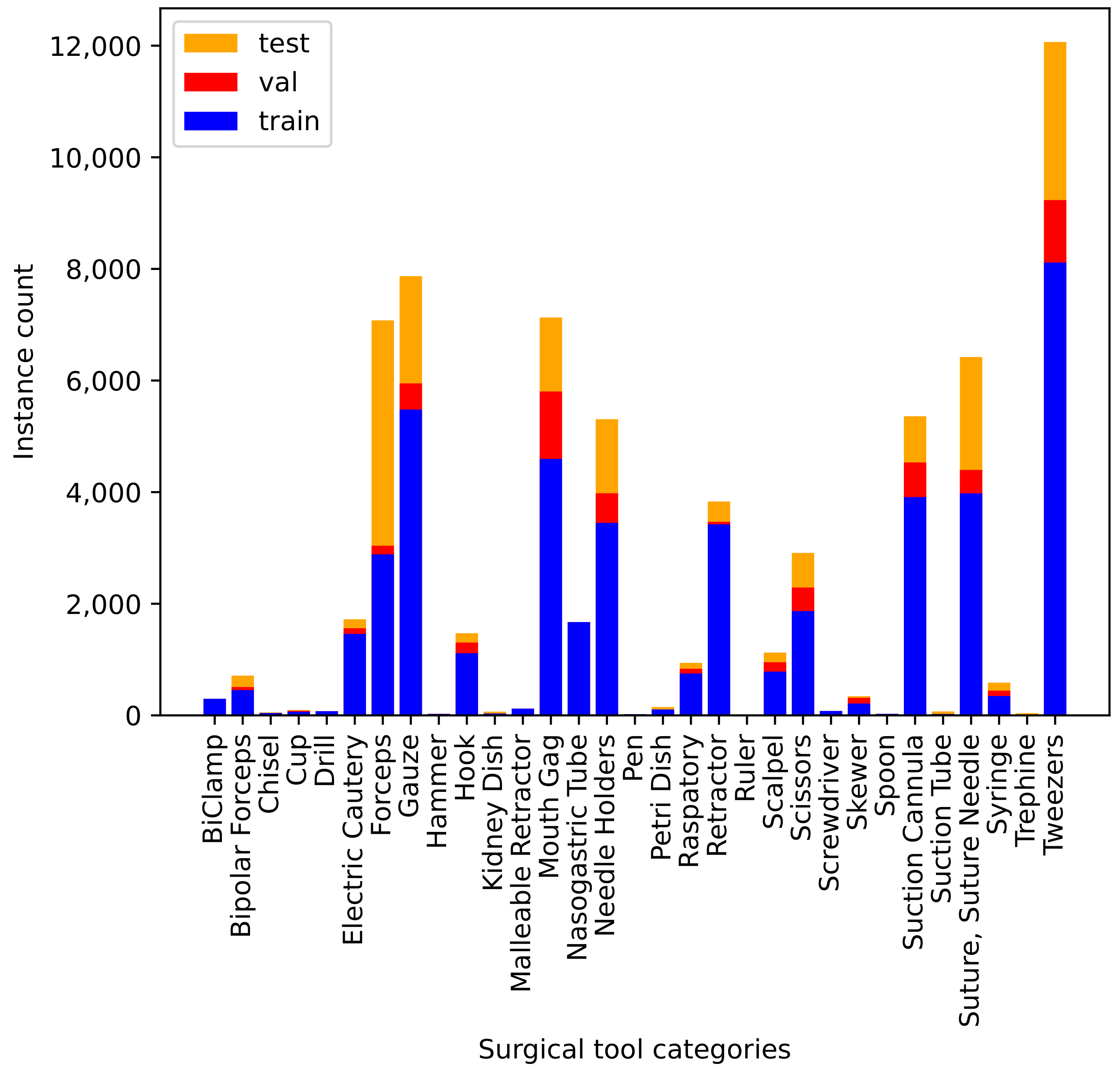
). The distribution of the number of instances per surgical tool category in the three splits is shown in
Figure 7. Because not all categories appear in all videos, we ensured all categories were present in the training set. We split the rest of the videos between the validation and test sets. The distribution of the category in each set is different because data are split by the
video-based split, as shown in
Figure 7. Another way to perform a split, the
frame-based split, can generate a more uniform distribution among the three sets. However, the
frame-based split would have the model be trained and evaluated on almost the same data. In real-world surgery, the data distribution drastically change every surgery, or video due to the various surgery type, operative environments, and lighting conditions. To tackle the tool detection in these challenging settings, we chose
video-based split.
Figure 7 indicates that the dataset is highly imbalanced; consequently, accurate instrument classification is more challenging.
Tweezers contains the largest number of instances because surgeons use them commonly for all procedures. On the other hand,
Ruler contains the smallest number of instances, as surgeons use it only for specific purposes (e.g., measuring tumors). Furthermore, there are other visual challenges because of the high inter-category similarity among tools. For instance,
Forceps,
Needle Holders, and
Scissors categories have similar appearances, as shown in
Figure 4.
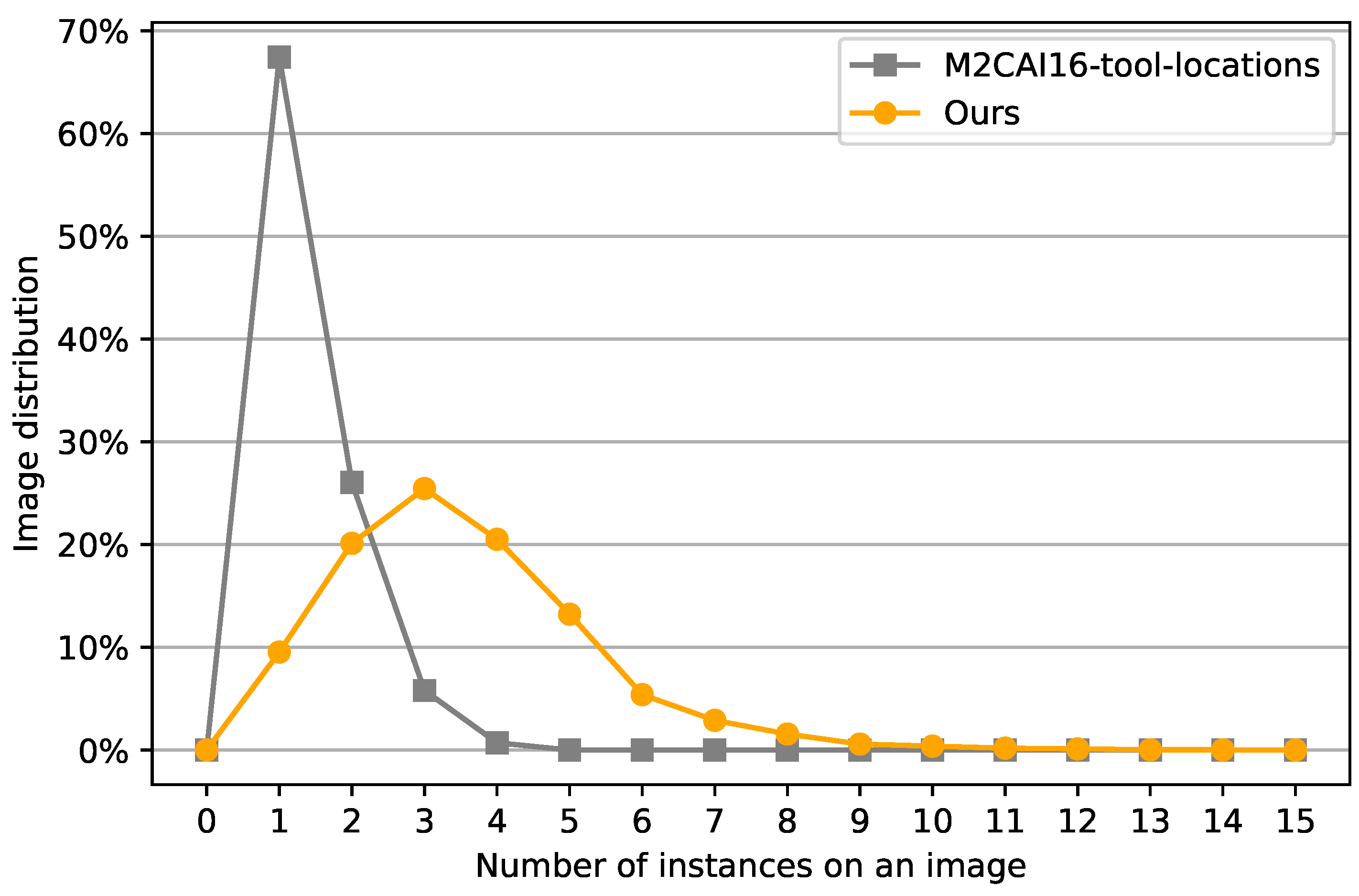
3.4. Number of Instances per Frame
We provide a comparison between our dataset and M2CAI16-tool-locations [
13], which is a common dataset for surgical tool detection for MIS in terms of the number of instances per image. According to
Figure 8, our dataset is more dense than m2cai16-tool-locations [
13]. In general, MIS contains three surgeons performing operations. Two surgeons operate the laparoscopic tools, and one surgeon controls the laparoscopic camera. Thus, the number of surgical tools that appear in a frame is at most four. On the other hand, in open surgery, in addition to the surgeons, other people (e.g., anesthesiologists, perfusionists, and nurses) controlling surgical tools can appear in a frame at the same time. The maximum number of surgical tools that appear in our dataset is 15. Moreover, the number of surgical tools appear in a frame drastically varies based on the surgery type. This makes the variance of the number of instances per image from our open surgery dataset significantly larger than the existing MIS dataset.
3.5. Co-Occurrences of the Surgical Tools
We also study the co-occurrences in our dataset. In
Figure 9a, the co-occurrence matrix of surgical tools and surgical types, we can see some tools are only used in particular surgery types. As is obvious, we can see
Mouth Gag is only used in the types of surgery performed around the mouth (
Posterior Pharyngeal Flap and
Alveolar Bone Grafting), and
Skewer is only used for
Scar Revision. On the other hand, we can confirm
Tweezers are used in all surgeries. Therefore, since the surgical tool type can be the main indicator of the type of surgery performed, it is important to distinguish between the types of surgical tools. In
Figure 9b, the c0-occurrence matrix of the surgical tools and surgical tools, we can see some sets of tools appear at the same time. For example,
Cup and
Skewer,
Chisel and
Hammer and
Needle Holders and
Suture, Suture Needle are often used together. On the other hand,
Gauze,
Suction Cannula and
Tweezers appear with any type of tool. Therefore, it indicates that the information of one tool can help the detection of other tools.
4. Experiments
4.1. Object Detection Models
We provide the baseline results on two widely used detectors, Faster R-CNN [
27] and RetinaNet [
28], as our benchmark testing algorithms.Faster R-CNN [
27] is a two-stage-based object detection method. A feature extraction network takes an RGB image as input and extracts features. Then, a region proposal network (RPN) is used to generate regions of interest (ROIs) and features are pooled over these ROIs before being passed to a final classification and bounding box refinement network. We employ the FPN feature extraction backbone to extract the features from multiple-resolution feature maps. RetinaNet [
28] is a single-stage-based object detection method. A RetinaNet detector is made up of a backbone network and two subnets, one for object classification and the other for object localization. FPN is used at the end of a RetinaNet backbone network. RetinanNet adopts Focal Loss which is designed to handle the problem of class imbalance. For the experiment, we exploit three kinds of backbones, i.e., ResNet-50, ResNet-101 [
47], and ResNe-X101 [
48].
4.2. Experiment Setup
We used the latest PyTorch implementations of Faster R-CNN and RetinaNet, released by Facebook research [
49]. For training, we fine-tune models pretrained on MS-COCO [
50] with our training data. We trained our detector on an NVIDIA RTX A5000 GPU, with a batch size of 8. The input image size is
. For training, we use the same setting defined in detectron2 [
49] for COCO except for the learning rate schedule. We set the learning rate to
. The networks were trained for 50K iterations with a learning rate drop of a factor of 10 after 33K and 44K iterations.
5. Results
The performance of the baseline models for the validation and test sets is represented in
Table 3. Overall, Faster-RCNN, which is a two-stage detector, clearly outperforms RetinaNet, which is a single-stage detector. In general, two-stage models are considered to be able to provide better detection accuracy. We can find this tendency in our results. The average precision (AP) of the test set was found to be much lower than that of the validation set for all models. This is caused by the way of performing a split. Because we split training, validation, and test sets with
video-based split considering the practical scenario, the distribution of categories in the three-set is different. Therefore, a gap in AP between validation and test sets occurs.
We conducted experiments with different backbones to explore the dependency of performance from the backbone. Faster-RCNN with a ResNet-X101 backbone presents the highest AP, and RetinaNet with a ResNet-50 backbone presents the lowest for both validation and test sets. The increase in depth and parameters slightly improves the AP in Faster-RCNN. On the other hand, for RetinaNet, the increase in depth and parameters have little effect on the AP.
The AP per category given in
Table 4 and
Table 5 shows that each surgical tool was detected with varying degrees of accuracy. This is mainly because of heavily imbalanced data, which naturally incur bias in the model. As a whole, the greater the number of annotated instances we can get, the better AP. For example, the baseline models successfully detected
Mouth Gag,
Needle Holders,
Suction Cannula, and
Tweezers categories, which have a relatively large number of instances. On the other hand, they fail to detect
Chisel,
Hammer,
Pen, and
Suction Tube categories, which have a small number of instances. The class imbalance is the main reason why there is a large gap between the AP of validation data and test data. As shown in
Table 1, compared to the validation data, the test data includes the category in which the number of instances is relatively small. This may result in better AP of validation sets rather than that of the test set.
There are cases where the models fail to detect the categories that have profound instances because of their challenging characteristics. First, the deformable surgical tool category is difficult to be detected. Gauze has the second largest number of instances in the dataset, but the AP of the best baseline model, Faster-RCNN ResNet-X101, is . This is much worse than the Mouth Gag category, which has almost the same number of instances in the dataset. The reason for this may be that the Gauze category is deformable and its appearance drastically changes every scene. Suture, Suture Needle also has this characteristic. Second, the surgical tool category that has a variety of appearances through instances is difficult to detect. Retractor, which is used to separate the edges of a surgical incision, has a different shape and size depending on the situation. The Retractor category also has a relatively large number of instances, but the AP of the best baseline model is only . Finally, the surgical tool category, which has different usages is difficult to detect. For instance, the Forceps category, which is used to grasp and hold objects, is mainly utilized to grasp the tissues or organs but sometimes surgical drape. In the former usage, Forceps is handled by the surgeon’s hand, and in the latter usage, Forceps is laid down around the surgical fields. Thus, depending on the usage, the visual feature drastically changes. This affects the surgical tool detection results.
6. Conclusions
Surgical tool detection is an indispensable task to be tackled for the surgical scene. However, mainly because of the lack of a large-scale and diverse dataset, there is only a small body of research work on open surgery videos. We presented our large-scale egocentric dataset for open surgery and the extensive evaluation of conventional object detection methods. We collected 15 open surgery videos of 7 different types of surgery using a camera attached to the surgeon’s head. The dataset consists of 67,687 annotated images with a bounding box around the surgical tool and its category label. Our dataset is superior in size and number of tool types compared with the existing open surgery dataset, which is often collected using a simulator. The statistics presented for the dataset illustrate that the dataset is imbalanced because many surgical tools are used for various purposes.
Despite the baseline experiments showing promising results for the detection of surgery tools in open surgery, the AP is not still acceptable for critical medical applications. One promising direction in future work is finding strategies to overcome the difficulty in the detection of heavily imbalanced data. Planned future work will collect surgery videos of which surgery type is less frequent in our dataset considering the revealed fact that the occurrence of some surgery tools depends on the surgery type.
Author Contributions
Conceptualization, R.F.; data curation, R.F. and H.K.; formal analysis, R.F.; funding acquisition, H.K. and H.S.; investigation, R.F.; methodology, R.F.; project administration, H.K. and H.S.; resources, H.S.; supervision, H.S.; validation, R.F.; visualization, R.F.; writing—original draft, R.F.; writing—review and editing, R.H. and H.S. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by MHLW Health, Labour, and Welfare Sciences Research Grants Research on Medical ICT and Artificial Intelligence Program Grant Number 20AC1004, the MIC/SCOPE #201603003, and JSPS KAKENHI Grant Number 22H03617.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Keio University School of Medicine.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Primus, M.J.; Putzgruber-Adamitsch, D.; Taschwer, M.; Münzer, B.; El-Shabrawi, Y.; Böszörmenyi, L.; Schoeffmann, K. Frame-Based Classification of Operation Phases in Cataract Surgery Videos. In MultiMedia Modeling; Schoeffmann, K., Chalidabhongse, T.H., Ngo, C.W., Aramvith, S., O’Connor, N.E., Ho, Y.S., Gabbouj, M., Elgammal, A., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 241–253. [Google Scholar]
- Zisimopoulos, O.; Flouty, E.; Luengo, I.; Giataganas, P.; Nehme, J.; Chow, A.; Stoyanov, D. DeepPhase: Surgical Phase Recognition in CATARACTS Videos. In Medical Image Computing and Computer Assisted Intervention; Frangi, A.F., Schnabel, J.A., Davatzikos, C., Alberola-López, C., Fichtinger, G., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 265–272. [Google Scholar]
- Kannan, S.; Yengera, G.; Mutter, D.; Marescaux, J.; Padoy, N. Future-State Predicting LSTM for Early Surgery Type Recognition. IEEE Trans. Med. Imaging 2020, 39, 556–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkov, M.; Hashimoto, D.A.; Rosman, G.; Meireles, O.R.; Rus, D. Machine learning and coresets for automated real-time video segmentation of laparoscopic and robot-assisted surgery. In Proceedings of the International Conference on Robotics and Automation (ICRA), Singapore, 29 May–3 June 2017; pp. 754–759. [Google Scholar] [CrossRef]
- Liu, T.; Meng, Q.; Vlontzos, A.; Tan, J.; Rueckert, D.; Kainz, B. Ultrasound Video Summarization Using Deep Reinforcement Learning. In Medical Image Computing and Computer Assisted Intervention; Martel, A.L., Abolmaesumi, P., Stoyanov, D., Mateus, D., Zuluaga, M.A., Zhou, S.K., Racoceanu, D., Joskowicz, L., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 483–492. [Google Scholar]
- Nwoye, C.I.; Mutter, D.; Marescaux, J.; Padoy, N. Weakly supervised convolutional LSTM approach for tool tracking in laparoscopic videos. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1059–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, X.; Allan, M.; Dore, A.; Ourselin, S.; Hawkes, D.; Kelly, J.D.; Stoyanov, D. Combined 2D and 3D tracking of surgical instruments for minimally invasive and robotic-assisted surgery. Int. J. Comput. Assist. Radiol. Surg. (IJCARS) 2016, 11, 1109–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Zhao, Z.; Cheng, X. Surgical instruments tracking based on deep learning with lines detection and spatio-temporal context. In Proceedings of the Chinese Automation Congress (CAC), Jinan, China, 20–22 October 2017; pp. 2711–2714. [Google Scholar] [CrossRef]
- Kurmann, T.; Marquez Neila, P.; Du, X.; Fua, P.; Stoyanov, D.; Wolf, S.; Sznitman, R. Simultaneous Recognition and Pose Estimation of Instruments in Minimally Invasive Surgery. In Medical Image Computing and Computer-Assisted Intervention; Descoteaux, M., Maier-Hein, L., Franz, A., Jannin, P., Collins, D.L., Duchesne, S., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 505–513. [Google Scholar]
- Colleoni, E.; Moccia, S.; Du, X.; De Momi, E.; Stoyanov, D. Deep Learning Based Robotic Tool Detection and Articulation Estimation With Spatio-Temporal Layers. IEEE Robot. Autom. Lett. 2019, 4, 2714–2721. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; Kurmann, T.; Chang, P.L.; Allan, M.; Ourselin, S.; Sznitman, R.; Kelly, J.D.; Stoyanov, D. Articulated Multi-Instrument 2-D Pose Estimation Using Fully Convolutional Networks. IEEE Trans. Med. Imaging 2018, 37, 1276–1287. [Google Scholar] [CrossRef] [Green Version]
- Rivoir, D.; Bodenstedt, S.; von Bechtolsheim, F.; Distler, M.; Weitz, J.; Speidel, S. Unsupervised Temporal Video Segmentation as an Auxiliary Task for Predicting the Remaining Surgery Duration. In OR 2.0 Context-Aware Operating Theaters and Machine Learning in Clinical Neuroimaging; Zhou, L., Sarikaya, D., Kia, S.M., Speidel, S., Malpani, A., Hashimoto, D., Habes, M., Löfstedt, T., Ritter, K., Wang, H., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 29–37. [Google Scholar]
- Jin, A.; Yeung, S.; Jopling, J.; Krause, J.; Azagury, D.; Milstein, A.; Fei-Fei, L. Tool Detection and Operative Skill Assessment in Surgical Videos Using Region-Based Convolutional Neural Networks. In Proceedings of the IEEE Winter Conference on Applications of Computer Vision (WACV), Waikoloa, HI, USA, 4–8 January 2018; pp. 691–699. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.; Jo, K.; Choi, S.; Choi, J. Surgical-tools detection based on Convolutional Neural Network in laparoscopic robot-assisted surgery. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 1756–1759. [Google Scholar] [CrossRef]
- Sarikaya, D.; Corso, J.J.; Guru, K.A. Detection and Localization of Robotic Tools in Robot-Assisted Surgery Videos Using Deep Neural Networks for Region Proposal and Detection. IEEE Trans. Med. Imaging 2017, 36, 1542–1549. [Google Scholar] [CrossRef]
- Vardazaryan, A.; Mutter, D.; Marescaux, J.; Padoy, N. Weakly-supervised learning for tool localization in laparoscopic videos. In MICCAI LABELS; Springer: Berlin/Heidelberg, Germany, 2018; pp. 169–179. [Google Scholar]
- Al Hajj, H.; Lamard, M.; Conze, P.H.; Roychowdhury, S.; Hu, X.; Maršalkaitė, G.; Zisimopoulos, O.; Dedmari, M.A.; Zhao, F.; Prellberg, J.; et al. CATARACTS: Challenge on automatic tool annotation for cataRACT surgery. Med. Image Anal. 2019, 52, 24–41. [Google Scholar] [CrossRef]
- Twinanda, A.P.; Shehata, S.; Mutter, D.; Marescaux, J.; de Mathelin, M.; Padoy, N. EndoNet: A Deep Architecture for Recognition Tasks on Laparoscopic Videos. IEEE Trans. Med. Imaging 2017, 36, 86–97. [Google Scholar] [CrossRef] [Green Version]
- Twinanda, A.P.; Mutter, D.; Marescaux, J.; de Mathelin, M.; Padoy, N. Single-and multi-task architectures for tool presence detection challenge at M2CAI 2016. arXiv 2016, arXiv:1610.08851. [Google Scholar]
- Bawa, V.S.; Singh, G.; KapingA, F.; Skarga-Bandurova, I.; Oleari, E.; Leporini, A.; Landolfo, C.; Zhao, P.; Xiang, X.; Luo, G.; et al. The saras endoscopic surgeon action detection (esad) dataset: Challenges and methods. arXiv 2021, arXiv:2104.03178. [Google Scholar]
- Zia, A.; Sharma, Y.; Bettadapura, V.; Sarin, E.L.; Clements, M.A.; Essa, I. Automated Assessment of Surgical Skills Using Frequency Analysis. In Medical Image Computing and Computer-Assisted Intervention; Navab, N., Hornegger, J., Wells, W.M., Frangi, A., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 430–438. [Google Scholar]
- Basiev, K.; Goldbraikh, A.; Pugh, C.M.; Laufer, S. Open surgery tool classification and hand utilization using a multi-camera system. arXiv 2021, arXiv:2111.06098. [Google Scholar] [CrossRef]
- Goldbraikh, A.; D’Angelo, A.L.; Pugh, C.M.; Laufer, S. Video-based fully automatic assessment of open surgery suturing skills. Int. J. Comput. Assist. Radiol. Surg. (IJCARS) 2022, 17, 437–448. [Google Scholar] [CrossRef]
- Shimizu, T.; Hachiuma, R.; Kajita, H.; Takatsume, Y.; Saito, H. Hand Motion-Aware Surgical Tool Localization and Classification from an Egocentric Camera. J. Imaging 2021, 7, 15. [Google Scholar] [CrossRef]
- Goodman, E.D.; Patel, K.K.; Zhang, Y.; Locke, W.; Kennedy, C.J.; Mehrotra, R.; Ren, S.; Guan, M.; Downing, M.; Chen, H.W.; et al. A real-time spatiotemporal AI model analyzes skill in open surgical videos. arXiv 2021, arXiv:2112.07219. [Google Scholar]
- Shimizu, T.; Oishi, K.; Hachiuma, R.; Kajita, H.; Takatsume, Y.; Saito, H. Surgery recording without occlusions by multi-view surgical videos. In VISAPP, Proceedings of the International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP), Valetta, Malta, 27–29 February 2020; Farinella, G., Radeva, P., Braz, J., Eds.; SciTePress: Setubal, Portugal, 2020; pp. 837–844. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards Real-Time Object Detection with Region Proposal Networks. In Advances in Neural Information Processing Systems (NIPS); Cortes, C., Lawrence, N., Lee, D., Sugiyama, M., Garnett, R., Eds.; Curran Associates Inc.: Red Hook, NY, USA, 2015; Volume 28. [Google Scholar]
- Lin, T.Y.; Goyal, P.; Girshick, R.; He, K.; Dollár, P. Focal Loss for Dense Object Detection. IEEE Trans. Pattern Anal. Mach. Intell. 2020, 42, 318–327. [Google Scholar] [CrossRef] [Green Version]
- Kranzfelder, M.; Schneider, A.; Fiolka, A.; Schwan, E.; Gillen, S.; Wilhelm, D.; Schirren, R.; Reiser, S.; Jensen, B.; Feussner, H. Real-time instrument detection in minimally invasive surgery using radiofrequency identification technology. J. Surg. Res. 2013, 185, 704–710. [Google Scholar] [CrossRef]
- Haase, S.; Wasza, J.; Kilgus, T.; Hornegger, J. Laparoscopic instrument localization using a 3-D Time-of-Flight/RGB endoscope. In Proceedings of the IEEE Workshop on Applications of Computer Vision (WACV), Clearwater Beach, FL, USA, 15–17 January 2013; pp. 449–454. [Google Scholar] [CrossRef]
- Reiter, A.; Allen, P.K. An online learning approach to in-vivo tracking using synergistic features. In Proceedings of the 2010 IEEE/RSJ International Conference on Intelligent Robots and Systems, Taipei, Taiwan, 18–22 October 2010; pp. 3441–3446. [Google Scholar] [CrossRef] [Green Version]
- Bouget, D.; Benenson, R.; Omran, M.; Riffaud, L.; Schiele, B.; Jannin, P. Detecting Surgical Tools by Modelling Local Appearance and Global Shape. IEEE Trans. Med. Imaging 2015, 34, 2603–2617. [Google Scholar] [CrossRef]
- Reiter, A.; Allen, P.K.; Zhao, T. Feature Classification for Tracking Articulated Surgical Tools. In Medical Image Computing and Computer-Assisted Intervention; Ayache, N., Delingette, H., Golland, P., Mori, K., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 592–600. [Google Scholar]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You Only Look Once: Unified, Real-Time Object Detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 26 June–1 July 2016; pp. 779–788. [Google Scholar] [CrossRef] [Green Version]
- Mishra, K.; Sathish, R.; Sheet, D. Learning Latent Temporal Connectionism of Deep Residual Visual Abstractions for Identifying Surgical Tools in Laparoscopy Procedures. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition Workshops (CVPRW), Honolulu, HI, USA, 21–26 July 2017; pp. 2233–2240. [Google Scholar] [CrossRef]
- Al Hajj, H.; Lamard, M.; Conze, P.H.; Cochener, B.; Quellec, G. Monitoring tool usage in surgery videos using boosted convolutional and recurrent neural networks. Med. Image Anal. 2018, 47, 203–218. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Xu, Z.; Yan, C.; Huang, J. Graph Convolutional Nets for Tool Presence Detection in Surgical Videos. In Information Processing in Medical Imaging; Chung, A.C.S., Gee, J.C., Yushkevich, P.A., Bao, S., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 467–478. [Google Scholar]
- Jin, Y.; Li, H.; Dou, Q.; Chen, H.; Qin, J.; Fu, C.W.; Heng, P.A. Multi-task recurrent convolutional network with correlation loss for surgical video analysis. Med. Image Anal. 2020, 59, 101572. [Google Scholar] [CrossRef]
- Hachiuma, R.; Shimizu, T.; Saito, H.; Kajita, H.; Takatsume, Y. Deep Selection: A Fully Supervised Camera Selection Network for Surgery Recordings. In Medical Image Computing and Computer Assisted Intervention; Martel, A.L., Abolmaesumi, P., Stoyanov, D., Mateus, D., Zuluaga, M.A., Zhou, S.K., Racoceanu, D., Joskowicz, L., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 419–428. [Google Scholar]
- Saito, Y.; Hachiuma, R.; Saito, H.; Kajita, H.; Takatsume, Y.; Hayashida, T. Camera Selection for Occlusion-Less Surgery Recording via Training With an Egocentric Camera. IEEE Access 2021, 9, 138307–138322. [Google Scholar] [CrossRef]
- Yoshida, K.; Hachiuma, R.; Tomita, H.; Pan, J.; Kitani, K.; Kajita, H.; Hayashida, T.; Sugimoto, M. Spatiotemporal Video Highlight by Neural Network Considering Gaze and Hands of Surgeon in Egocentric Surgical Videos. J. Med Robot. Res. 2021, 7, 2141001. [Google Scholar] [CrossRef]
- Zhang, M.; Cheng, X.; Copeland, D.; Desai, A.; Guan, M.; Brat, G.; Yeung, S. Using Computer Vision to Automate Hand Detection and Tracking of Surgeon Movements in Videos of Open Surgery. AMIA Annu. Symp. Proc. 2021, 2020, 1373–1382. [Google Scholar]
- Shi, P.; Zhao, Z.; Hu, S.; Chang, F. Real-Time Surgical Tool Detection in Minimally Invasive Surgery Based on Attention-Guided Convolutional Neural Network. IEEE Access 2020, 8, 228853–228862. [Google Scholar] [CrossRef]
- Ahmidi, N.; Tao, L.; Sefati, S.; Gao, Y.; Lea, C.; Haro, B.B.; Zappella, L.; Khudanpur, S.; Vidal, R.; Hager, G.D. A Dataset and Benchmarks for Segmentation and Recognition of Gestures in Robotic Surgery. IEEE Trans. Biomed. Eng. 2017, 64, 2025–2041. [Google Scholar] [CrossRef]
- Gao, Y.; Vedula, S.S.; Reiley, C.E.; Ahmidi, N.; Varadarajan, B.; Lin, H.C.; Tao, L.; Zappella, L.; Béjar, B.; Yuh, D.D.; et al. Jhu-Isi Gesture and Skill Assessment Working Set (Jigsaws): A Surgical Activity Dataset for Human Motion Modeling. MICCAI Workshop: M2cai. 2014, Volume 3, p. 3. Available online: https://cirl.lcsr.jhu.edu/research/hmm/datasets/jigsaws_release/ (accessed on 31 August 2022).
- Kadkhodamohammadi, A.; Gangi, A.; de Mathelin, M.; Padoy, N. A Multi-view RGB-D Approach for Human Pose Estimation in Operating Rooms. In Proceedings of the IEEE Winter Conference on Applications of Computer Vision (WACV), Santa Rosa, CA, USA, 24–31 March 2017; pp. 363–372. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Xie, S.; Girshick, R.; Dollár, P.; Tu, Z.; He, K. Aggregated Residual Transformations for Deep Neural Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 22–25 July 2017; pp. 5987–5995. [Google Scholar] [CrossRef]
- Wu, Y.; Kirillov, A.; Massa, F.; Lo, W.Y.; Girshick, R. Detectron2. 2019. Available online: https://github.com/facebookresearch/detectron2 (accessed on 31 August 2022).
- Lin, T.Y.; Maire, M.; Belongie, S.; Hays, J.; Perona, P.; Ramanan, D.; Dollár, P.; Zitnick, C.L. Microsoft COCO: Common Objects in Context. In Computer Vision—ECCV 2014; Fleet, D., Pajdla, T., Schiele, B., Tuytelaars, T., Eds.; Springer International Publishing: Cham, Switzerland, 2014; pp. 740–755. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}