
Influence of Paraprobiotics-Containing Moisturizer on Skin Hydration and Microbiome: A Preliminary Study

 ,
,  ,
,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Preparation of Moisturizer
2.2. Study Design and Analysis
2.3. Next-Generation Sequencing
2.4. Microbiome Analyses
2.5. Statistical Analysis
3. Results
3.1. Demographic Parameters
3.2. Skin Moisture
3.3. Microbiome Analysis
3.3.1. Rarefaction Curve Analysis
Microbial Richness
Similarity and Variations in the Microbiome
3.3.2. Taxonomy Assignment
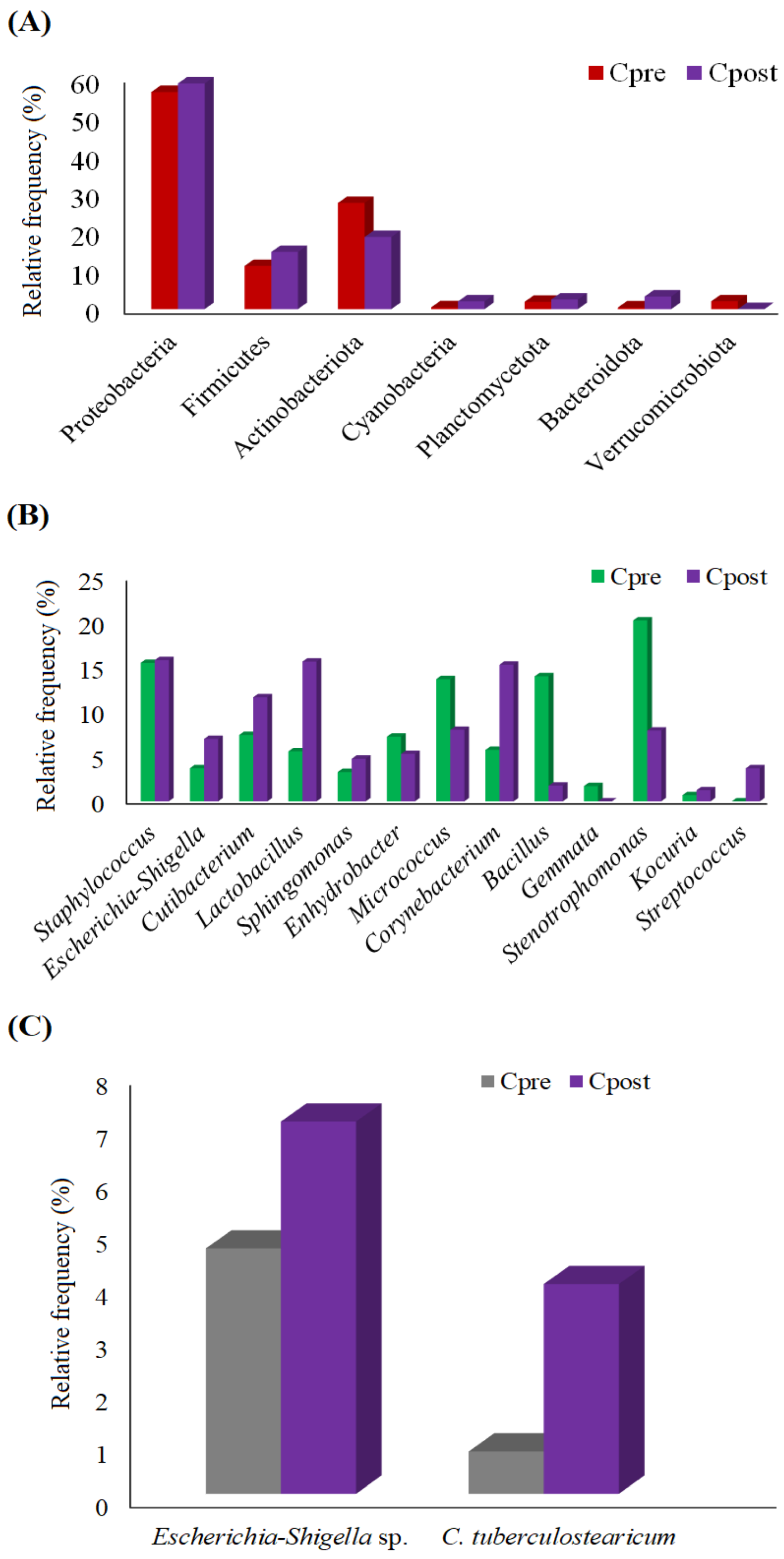
Estimation of the Phylum
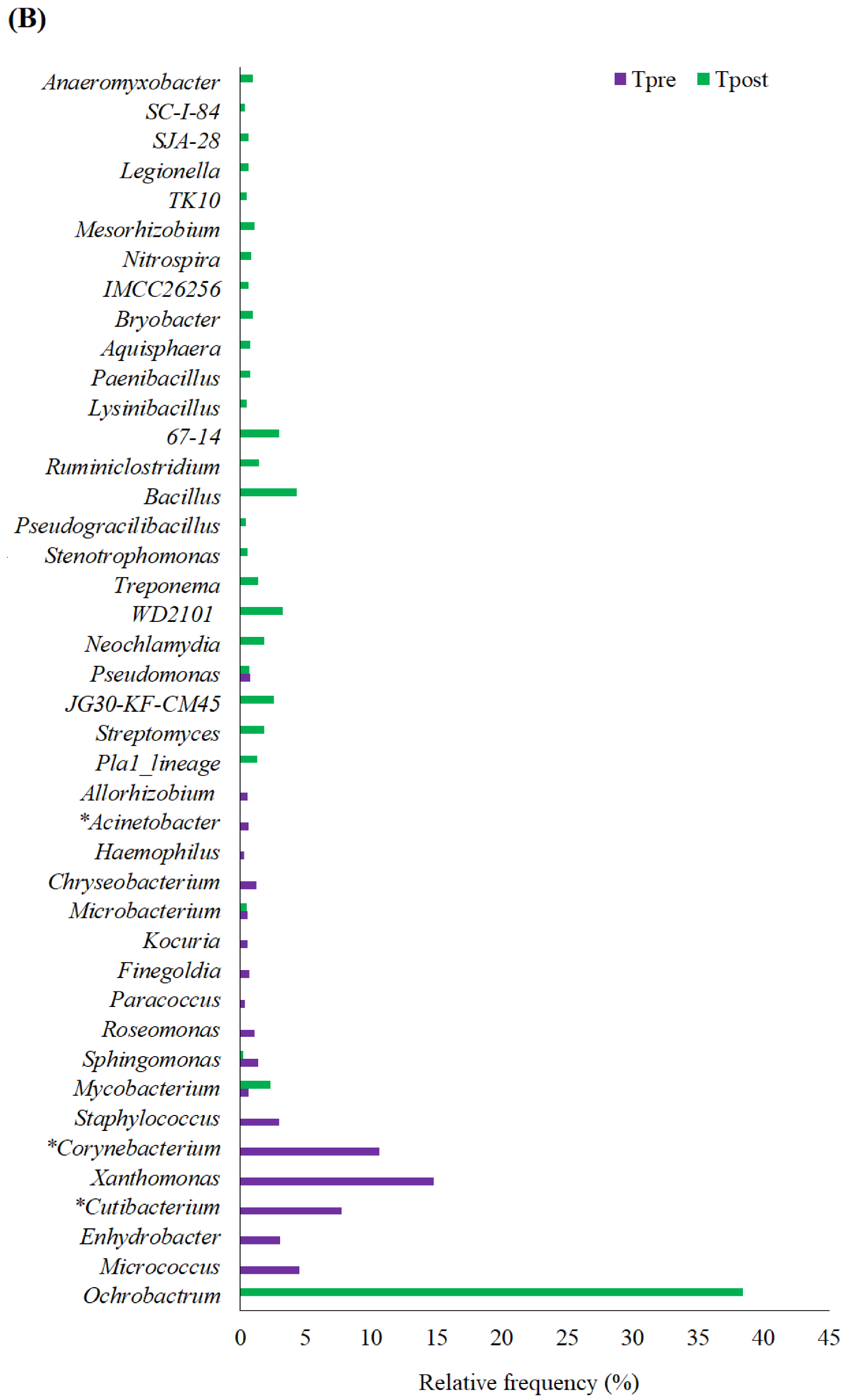
Estimation of the Genus
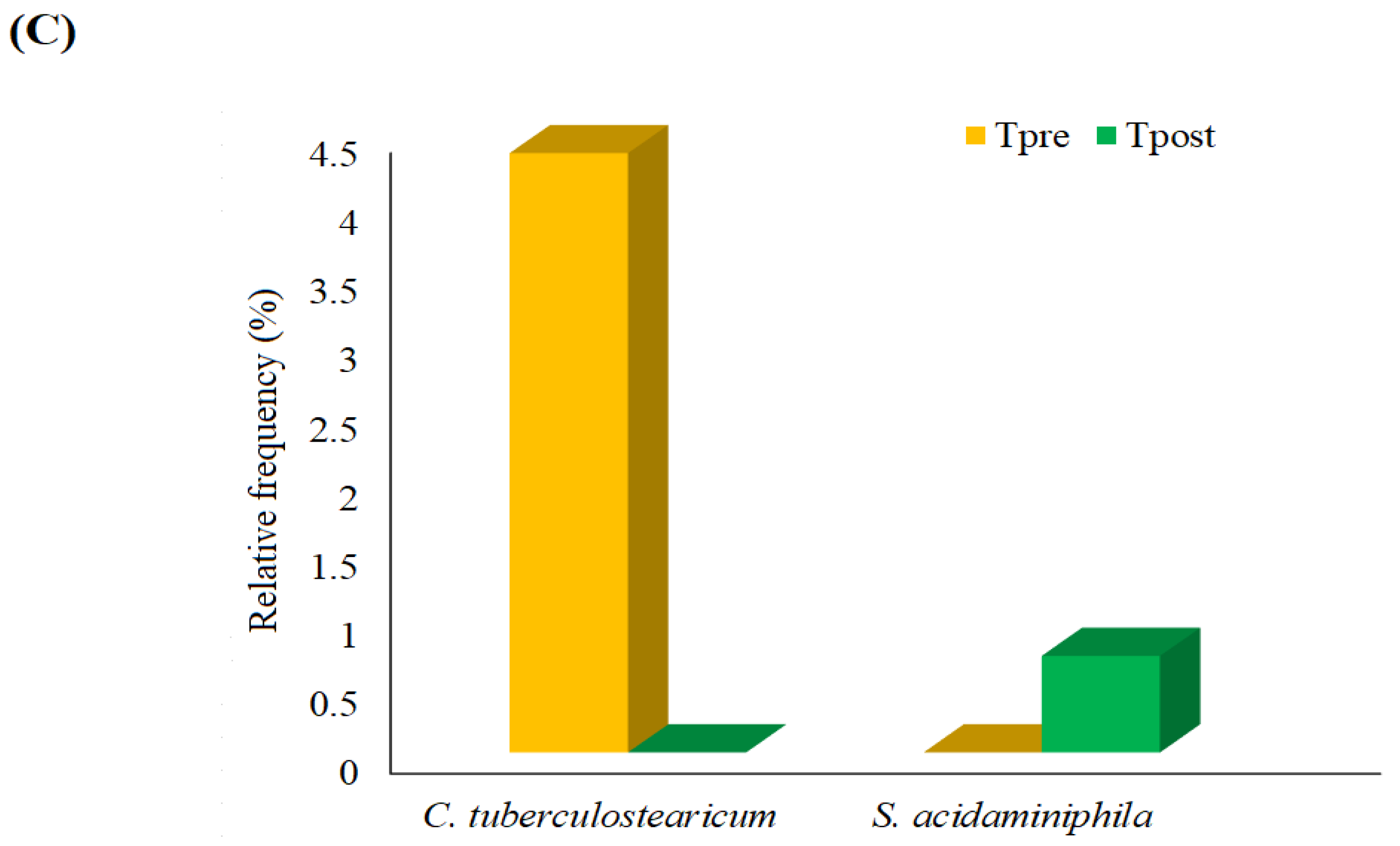
Estimation of the Species
4. Discussion
4.1. Moisturizing Effects of APM
4.2. Changes in Skin Microbiome: Phylum
4.3. Changes in Skin Microbiome: Genus
4.4. Changes in Skin Microbiome: Species
4.5. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Somboonna, N.; Wilantho, A.; Srisuttiyakorn, C.; Assawamakin, A.; Tongsima, S. Bacterial communities on facial skin of teenage and elderly Thai females. Arch. Microbiol. 2017, 199, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Kong, H.H.; Segre, J.A. Skin microbiome: Looking back to move forward. J. Investig. Dermatol. 2012, 132, 933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwarsa, O.; Hazari, M.N.; Dharmadji, H.P.; Dwiyana, R.F.; Effendi, R.M.R.A.; Hidayah, R.M.N.; Avriyanti, E.; Gunawan, H.; Sutedja, E. A Pilot study: Composition and diversity of 16S rRNA based skin bacterial microbiome in Indonesian atopic dermatitis population. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Berg, G.; Rybakova, D.; Fischer, D.; Cernava, T.; Vergès, M.C.; Charles, T.; Chen, X.; Cocolin, L.; Eversole, K.; Corral, G.H.; et al. Microbiome definition re-visited: Old concepts and new challenges. Microbiome 2020, 8, 103. [Google Scholar] [CrossRef] [PubMed]
- Skowron, K.; Bauza-Kaszewska, J.; Kraszewska, Z.; Wiktorczyk-Kapischke, N.; Grudlewska-Buda, K.; Kwiecińska-Piróg, J.; Wałecka-Zacharska, E.; Radtke, L.; Gospodarek-Komkowska, E. Human skin microbiome: Impact of intrinsic and extrinsic factors on skin microbiota. Microorganisms 2021, 9, 543. [Google Scholar] [CrossRef]
- Findley, K.; Grice, E.A. The skin microbiome: A focus on pathogens and their association with skin disease. PLoS Pathog. 2014, 10, e1004436. [Google Scholar] [CrossRef]
- Roig-Rosello, E.; Rousselle, P. The human epidermal basement membrane: A shaped and cell instructive platform that aging slowly alters. Biomolecules 2020, 10, 1607. [Google Scholar] [CrossRef]
- Iglesia, S.; Kononov, T.; Zahr, A.S. A multi-functional anti-aging moisturizer maintains a diverse and balanced facial skin microbiome. J. Appl. Microbiol. 2022, 133, 1791–1799. [Google Scholar] [CrossRef]
- Yu, J.; Ma, X.; Wang, X.; Cui, X.; Ding, K.; Wang, S.; Han, C. Application and mechanism of probiotics in skin care: A review. J. Cosmet. Dermatol. 2022, 21, 886–894. [Google Scholar] [CrossRef]
- Sevimli-Gür, C.; Onbaşılar, I.; Atilla, P.; Genç, R.; Cakar, N.; Deliloğlu-Gürhan, I.; Bedir, E. In vitro growth stimulatory and in vivo wound healing studies on cycloartane-type saponins of Astragalus genus. J. Ethnopharmacol. 2011, 134, 844–850. [Google Scholar] [CrossRef]
- Pageon, H.; Azouaoui, A.; Zucchi, H.; Ricois, S.; Tran, C.; Asselineau, D. Potentially beneficial effects of rhamnose on skin ageing: An in vitro and in vivo study. Int. J. Cosmet. Sci. 2019, 41, 213–220. [Google Scholar] [CrossRef]
- Dréno, B.; Alexis, A.; Chuberre, B.; Marinovich, M. Safety of titanium dioxide nanoparticles in cosmetics. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 34–46. [Google Scholar] [CrossRef] [Green Version]
- França, K. Topical probiotics in dermatological therapy and skincare: A concise review. Dermatol. Ther. 2021, 11, 71–77. [Google Scholar] [CrossRef]
- Gueniche, A.; Philippe, D.; Bastien, P.; Reuteler, G.; Blum, S.; Castiel-Higounenc, I.; Breton, L.; Benyacoub, J. Randomised double-blind placebo-controlled study of the effect of Lactobacillus paracasei NCC 2461 on skin reactivity. Benef. Microbes 2014, 5, 137–145. [Google Scholar] [CrossRef]
- Lee, D.E.; Huh, C.S.; Ra, J.; Choi, I.D.; Jeong, J.W.; Kim, S.H.; Ryu, J.H.; Seo, Y.K.; Koh, J.S.; Lee, J.H.; et al. Clinical evidence of effects of Lactobacillus plantarum HY7714 on skin aging: A randomized, double blind, placebo-controlled study. J. Microbiol. Biotechnol. 2015, 25, 2160–2168. [Google Scholar] [CrossRef]
- Liu, C.; Tseng, Y.P.; Chan, L.P.; Liang, C.H. The potential of Streptococcus thermophiles (TCI633) in the anti-aging. J. Cosmet. Dermatol. 2022, 21, 2635–2647. [Google Scholar] [CrossRef]
- Sivamaruthi, B.; Kesika, P.; Chaiyasut, C. A review on anti-aging properties of probiotics. Int. J. Appl. Pharm. 2018, 10, 23–27. [Google Scholar] [CrossRef] [Green Version]
- Sharma, D.; Kober, M.M.; Bowe, W.P. Anti-aging effects of probiotics. J. Drugs Dermatol. 2016, 15, 9–12. [Google Scholar]
- Ratanapokasatit, Y.; Laisuan, W.; Rattananukrom, T.; Petchlorlian, A.; Thaipisuttikul, I.; Sompornrattanaphan, M. How microbiomes affect skin aging: The updated evidence and current perspectives. Life 2022, 12, 936. [Google Scholar] [CrossRef]
- Lolou, V.; Panayiotidis, M.I. Functional role of probiotics and prebiotics on skin health and disease. Fermentation 2019, 5, 41. [Google Scholar] [CrossRef] [Green Version]
- Thorakkattu, P.; Khanashyam, A.C.; Shah, K.; Babu, K.S.; Mundanat, A.S.; Deliephan, A.; Deokar, G.S.; Santivarangkna, C.; Nirmal, N.P. Postbiotics: Current trends in food and pharmaceutical industry. Foods 2022, 11, 3094. [Google Scholar] [CrossRef] [PubMed]
- Teame, T.; Wang, A.; Xie, M.; Zhang, Z.; Yang, Y.; Ding, Q.; Gao, C.; Olsen, R.E.; Ran, C.; Zhou, Z. Paraprobiotics and Postbiotics of probiotic lactobacilli, their positive effects on the host and action mechanisms: A review. Front. Nutr. 2020, 7, 570344. [Google Scholar] [CrossRef] [PubMed]
- Cuevas-Gonzalez, P.F.; Liceaga, A.M.; Aguilar-Toala, J.E. Postbiotics and paraprobiotics: From concepts to applications. Food Res. Int. 2020, 136, 109502. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Jeon, B.; Kim, W.J.; Chung, D. Effect of paraprobiotic prepared from Kimchi-derived Lactobacillus plantarum K8 on skin moisturizing activity in human keratinocyte. J. Funct. Foods 2020, 75, 104244. [Google Scholar] [CrossRef]
- Baldwin, H.; Aguh, C.; Andriessen, A.; Benjamin, L.; Ferberg, A.S.; Hooper, D.; Jarizzo, J.L.; Lio, P.A.; Tlougan, B.; Woolery-Lloyd, H.C.; et al. Atopic dermatitis and the role of the skin microbiome in choosing prevention, treatment, and maintenance options. J. Drugs Dermatol. 2020, 19, 935–940. [Google Scholar] [CrossRef]
- Golkar, N.; Ashoori, Y.; Heidari, R.; Omidifar, N.; Abootalebi, S.N.; Mohkam, M.; Gholami, A. A novel effective formulation of bioactive compounds for wound healing: Preparation, in vivo characterization, and comparison of various postbiotics cold creams in a rat model. Evid.-Based Complement. Altern. Med. 2021, 2021, 8577116. [Google Scholar] [CrossRef]
- Catic, T.; Pehlivanovic, B.; Pljakic, N.; Balicevac, A. The moisturizing efficacy of a proprietary dermo-cosmetic product (cls02021) versus placebo in a 4-week application period. Med. Arch. 2022, 76, 108–114. [Google Scholar] [CrossRef]
- Grice, E.A.; Kong, H.H.; Renaud, G.; Young, A.C. A diversity profile of the human skin microbiota. Genome Res. 2008, 18, 1043–1050. [Google Scholar] [CrossRef] [Green Version]
- Jugé, R.; Rouaud-Tinguely, P.; Breugnot, J.; Servaes, K.; Grimaldi, C.; Roth, M.P.; Coppin, H.; Closs, B. Shift in skin microbiota of western European women across aging. J. Appl. Microbiol. 2018, 125, 907–916. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Tseng, C.H.; Strober, B.E.; Pei, Z.; Blaser, M.J. Substantial alterations of the cutaneous bacterial biota in psoriatic lesions. PLoS ONE 2008, 3, e2719. [Google Scholar] [CrossRef]
- Benhadou, F.; Mintoff, D.; Schnebert, B.; Thio, H.B. Psoriasis and microbiota: A systematic review. Diseases 2018, 6, 47. [Google Scholar] [CrossRef]
- Burns, E.M.; Ahmed, H.; Isedeh, P.N.; Kohli, I.; Van Der Pol, W.; Shaheen, A.; Muzaffar, A.F.; Al-Sadek, C.; Foy, T.M.; Abdelgawwad, M.S.; et al. Ultraviolet radiation, both UVA and UVB, influences the composition of the skin microbiome. Exp. Dermatol. 2019, 28, 136–141. [Google Scholar] [CrossRef]
- Kallscheuer, N.; Jogler, C. The bacterial phylum Planctomycetes as novel source for bioactive small molecules. Biotechnol. Adv. 2021, 53, 107818. [Google Scholar] [CrossRef]
- Ling, Z.; Liu, X.; Luo, Y.; Yuan, L.; Nelson, K.E.; Wang, Y.; Xiang, C.; Li, L. Pyrosequencing analysis of the human microbiota of healthy Chinese undergraduates. BMC Genom. 2013, 14, 390. [Google Scholar] [CrossRef] [Green Version]
- Hsu, D.K.; Fung, M.A.; Chen, H. Role of skin and gut microbiota in the pathogenesis of psoriasis, an inflammatory skin disease. Med. Microecol. 2020, 4, 100016. [Google Scholar] [CrossRef]
- Towner, K. The Genus Acinetobacter. In The Prokaryotes, 3rd ed.; Dworkin, M., Falkow, S., Rosenberg, E., Schleifer, K., Stackebrandt, E., Eds.; Springer: New York, NY, USA, 2006; pp. 746–758. [Google Scholar]
- Blaise, G.; Nikkels, A.F.; Hermanns-Lê, T.; Nikkels-Tassoudji, N.; Piérard, G.E. Corynebacterium-associated skin infections. Int. J. Dermatol. 2008, 47, 884–890. [Google Scholar] [CrossRef]
- Kim, J.H.; Son, S.M.; Park, H.; Kim, B.K.; Choi, I.S.; Kim, H.; Huh, C.S. Taxonomic profiling of skin microbiome and correlation with clinical skin parameters in healthy Koreans. Sci. Rep. 2021, 11, 16269. [Google Scholar] [CrossRef]
- Higuchi, R.; Goto, T.; Hirotsu, Y.; Otake, S.; Oyama, T.; Amemiya, K.; Ohyama, H.; Mochizuki, H.; Omata, M. Sphingomonas and Phenylobacterium as major microbiota in thymic epithelial tumors. J. Pers. Med. 2021, 11, 1092. [Google Scholar] [CrossRef]
- Krzyściak, W.; Jurczak, A.; Kościelniak, D.; Bystrowska, B.; Skalniak, A. The virulence of Streptococcus mutans and the ability to form biofilms. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 499–515. [Google Scholar] [CrossRef] [Green Version]
- Jalalvand, F.; Su, Y.C.; Manat, G.; Chernobrovkin, A.; Kadari, M.; Jonsson, S.; Janousková, M.; Rutishauser, D.; Semsey, S.; Løbner-Olesen, A.; et al. Protein domain-dependent vesiculation of Lipoprotein A, a protein that is important in cell wall synthesis and fitness of the human respiratory pathogen Haemophilus influenzae. Front. Cell. Infect. Microbiol. 2022, 12, 984955. [Google Scholar] [CrossRef]
- Meunier, M.; Scandolera, A.; Chapuis, E.; Lambert, C.; Jarrin, C.; Robe, P.; Chajra, H.; Auriol, D.; Reynaud, R. From stem cells protection to skin microbiota balance: Orobanche rapum extract, a new natural strategy. J. Cosmet. Dermatol. 2019, 18, 1140–1154. [Google Scholar] [CrossRef] [PubMed]
- Bayal, N.; Nagpal, S.; Haque, M.M.; Patole, M.S.; Shouche, Y.; Mande, S.C.; Mande, S.S. Structural aspects of lesional and non-lesional skin microbiota reveal key community changes in leprosy patients from India. Sci. Rep. 2021, 11, 3294. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, H.S.; Lee, S.H.; Kim, S. Characterization and analysis of the skin microbiota in acne: Impact of systemic antibiotics. J. Clin. Med. 2020, 9, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karst, M.J. Staphylococcus aureus. In Encyclopedia of Toxicology, 2nd ed.; Wexler, P., Ed.; Academic Press: Cambridge, MA, USA, 2005; pp. 86–87. [Google Scholar]
- Falkinham, J.O.; Wall, T.E.; Tanner, J.R.; Tawaha, K.; Alali, F.Q.; Li, C.; Oberlies, N.H. Proliferation of antibiotic-producing bacteria and concomitant antibiotic production as the basis for the antibiotic activity of Jordan’s red soils. Appl. Environ. Microbiol. 2009, 75, 2735–2741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, I.; Yokota, A.; Yamazoe, A.; Fujiwara, T. Proposal of Lysinibacillus boronitolerans gen. nov. sp. nov., and transfer of Bacillus fusiformis to Lysinibacillus fusiformis comb. nov. and Bacillus sphaericus to Lysinibacillus sphaericus comb. nov. Int. J. Syst. Evol. Microbiol. 2007, 57, 1117–1125. [Google Scholar] [CrossRef] [Green Version]
- Grady, E.N.; MacDonald, J.; Liu, L.; Richman, A.; Yuan, Z.C. Current knowledge and perspectives of Paenibacillus: A review. Microb. Cell Fact. 2016, 15, 203. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Ma, Z.; Zhang, J.; Yang, L. Antifungal compounds against candida infections from traditional chinese medicine. BioMed Res. Int. 2017, 2017, 4614183. [Google Scholar] [CrossRef] [Green Version]
- Ryan, M.P.; Pembroke, J.T. The Genus Ochrobactrum as major opportunistic pathogens. Microorganisms 2020, 8, 1797. [Google Scholar] [CrossRef]
- Gardini, G.; Gregori, N.; Matteelli, A.; Castelli, F. Mycobacterial skin infection. Curr. Opin. Infect. Dis. 2022, 35, 79–87. [Google Scholar] [CrossRef]
- Norris, S.J.; Paster, B.J.; Moter, A.; Göbel, U.B. The Genus Treponema. In The Prokaryotes; Dworkin, M., Falkow, S., Rosenberg, E., Schleifer, K.H., Stackebrandt, E., Eds.; Springer: New York, NY, USA, 2006; Volume 7, pp. 211–234. [Google Scholar]
- Oya, A.L. Stenotrophomonas, Burkholderia and other related microorganisms. In Encyclopedia of Infection and Immunity, 1st ed.; Rezaei, N., Ed.; Elsevier: Amsterdam, The Netherlands, 2022; pp. 656–661. [Google Scholar]
- Altonsy, M.O.; Kurwa, H.A.; Lauzon, G.J.; Amrein, M.; Gerber, A.N.; Almishri, W.; Mydlarski, P.R. Corynebacterium tuberculostearicum, a human skin colonizer, induces the canonical nuclear factor-κB inflammatory signaling pathway in human skin cells. Immun. Inflamm. Dis. 2020, 8, 62–79. [Google Scholar] [CrossRef] [Green Version]
- Nagase, S.; Ogai, K.; Urai, T.; Shibata, K.; Matsubara, E.; Mukai, K.; Matsue, M.; Mori, Y.; Aoki, M.; Arisandi, D.; et al. Distinct skin microbiome and skin physiological functions between bedridden older patients and healthy people: A Single-center study in Japan. Front. Med. 2020, 7, 101. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Placebo | Treatment | p-Value (Statistical Method) | |
|---|---|---|---|---|
| Gender (%) | Male | 12 ± 48 | 10 ± 40 | 0.776 (Exact Fisher) |
| Female | 13 ± 52 | 15 ± 60 | ||
| Age (years) (Mean ± SE) | 26.92 ± 8.06 | 31.36 ± 12.26 | 0.0793 (Wilcoxon rank-sum) | |
| BMI (kg/m2) (Mean ± SE) | 21.53 ± 1.75 | 22.19 ± 3.46 | 0.3989 (t-test) | |
| Group | Measurement Time | TEWL (mg (Water)/m2/h) | p-Value | SCM (Au) | p-Value |
|---|---|---|---|---|---|
| Placebo (n = 25) | Baseline | 7.30 ± 0.43 | 34.07 ± 1.97 | ||
| 1st h | 6.53 ± 0.49 * | 0.1181 | 32.10 ± 2.37 a | 0.4512 | |
| 2nd h | 6.86 ± 0.33 a | 0.7672 | 36.32 ± 2.54 a | 0.3745 | |
| 3rd h | 7.10 ± 0.32 a | 0.9463 | 35.59 ± 2.43 b | 0.2864 | |
| 4th h | 6.79 ± 0.39 a | 0.6664 | 34.99 ± 2.23 b | 0.5289 | |
| 4th week | 6.93 ± 0.36 * | 0.4084 | 32.80 ± 1.60 b | 0.5724 | |
| Treatment (n = 25) | Baseline | 7.81± 0.36 | 30.18 ± 2.28 | ||
| 1st h | 3.41± 0.50 * | <0.0001 | 54.83 ± 3.46 b | <0.0001 * | |
| 2nd h | 3.46 ± 0.53 * | <0.0001 | 51.99 ± 3.57 b | <0.0001 * | |
| 3rd h | 4.21± 0.57 * | <0.0001 | 48.42 ± 3.40 b | <0.0001 * | |
| 4th h | 4.62 ± 0.47 * | <0.0001 | 44.24 ± 3.02 b | <0.0001 * | |
| 4th week | 5.91± 0.35 * | <0.0001 | 35.96 ± 1.93 b | 0.0007 * |
| Parameters | Comparison Time | Placebo (n = 25) | Treatment (n = 25) | p-Value |
|---|---|---|---|---|
| TEWL (mg(water)/m2/hour) | Baseline to 1st h | 0.77 ± 0.47 | 4.40 ± 0.38 | |
| Baseline to 2nd h | 0.44 ± 0.34 | 4.34 ± 0.46 | <0.0001 * | |
| Baseline to 3rd h | 0.20 ± 0.31 | 3.60 ± 0.46 | <0.0001 * | |
| Baseline to 4th h | 0.51 ± 0.42 | 3.18 ± 0.38 | <0.0001 * | |
| Baseline to 4th week | 0.37 ± 0.44 | 1.90 ± 0.28 | 0.0054 * | |
| SCM (Au) | 1st h to Baseline | −1.96 ± 1.46 | 24.64 ± 2.53 | |
| 2nd h to Baseline | 2.25 ± 1.81 | 21.80 ± 2.07 | <0.0001 * | |
| 3rd h to Baseline | 1.52 ± 1.40 | 18.24 ± 2.53 | <0.0001 * | |
| 4th h to Baseline | 0.92 ± 1.45 | 14.05 ± 1.91 | <0.0001 * | |
| 4th week to Baseline | −1.27 ± 2.22 | 5.77 ± 1.49 | 0.0114 * |
| Parameters | Coefficients | Confidence Interval (95%) | p-Value |
|---|---|---|---|
| Treatment compared to placebo | −2.494 | −3.605 to −1.383 | <0.0001 |
| Gender (Female compared to male) | 0.498 | −0.675 to 1.671 | 0.397 |
| Age | 0.013 | −0.043 to 0.069 | 0.643 |
| BMI | −0.088 | −0.285 to 0.109 | 0.373 |
| TEWL in placebo | 0.571 | 0.293 to 0.849 | <0.0001 |
| Constant | 3.905 | −1.035 to 8.846 | 0.118 |
| Parameters | Coefficients | Confidence Interval (95%) | p-Value |
|---|---|---|---|
| Treatment compared to placebo | 13.190 | 7.931 to 18.449 | <0.0001 |
| Gender (Female compared to male) | 1.597 | −3.861 to 7.055 | 0.558 |
| Age | −0.051 | −0.317 to 0.215 | 0.701 |
| BMI | −0.234 | −1.172 to 0.705 | 0.619 |
| SCM in placebo | 0.951 | 0.709 to 1.193 | <0.0001 |
| Constant | 8.158 | −16.890 to 33.207 | 0.515 |
| Parameters | Coefficients | Confidence Interval (95%) | p-Value |
|---|---|---|---|
| Treatment compared to placebo | −1.251 | −2.189 to −0.313 | 0.010 |
| Gender (Female compared to male) | −0.429 | −1.420 to 0.562 | 0.388 |
| Age | −0.003 | −0.050 to 0.045 | 0.909 |
| BMI | 0.053 | −0.114 to 0.219 | 0.528 |
| TEWL in placebo | 0.477 | 0.243 to 0.711 | <0.0001 |
| Constant | 2.612 | −1.560 to 6.784 | 0.214 |
| Parameters | Coefficients | Confidence Interval (95%) | p-Value |
|---|---|---|---|
| Treatment compared to placebo | 4.615 | −0.198 to 9.032 | 0.041 |
| Gender (Female compared to male) | 4.434 | −0.150 to 9.019 | 0.058 |
| Age | −0.037 | −0.261 to 0.186 | 0.737 |
| BMI | 0.258 | −0.530 to 1.047 | 0.513 |
| SCM in placebo | 0.467 | 0.263 to 0.671 | <0.0001 |
| Constant | 10.030 | −11.010 to 31.070 | 0.342 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaiyasut, C.; Sivamaruthi, B.S.; Tansrisook, C.; Peerajan, S.; Chaiyasut, K.; Bharathi, M. Influence of Paraprobiotics-Containing Moisturizer on Skin Hydration and Microbiome: A Preliminary Study. Appl. Sci. 2022, 12, 12483. https://doi.org/10.3390/app122312483
Chaiyasut C, Sivamaruthi BS, Tansrisook C, Peerajan S, Chaiyasut K, Bharathi M. Influence of Paraprobiotics-Containing Moisturizer on Skin Hydration and Microbiome: A Preliminary Study. Applied Sciences. 2022; 12(23):12483. https://doi.org/10.3390/app122312483
Chicago/Turabian StyleChaiyasut, Chaiyavat, Bhagavathi Sundaram Sivamaruthi, Chawin Tansrisook, Sartjin Peerajan, Khontaros Chaiyasut, and Muruganantham Bharathi. 2022. "Influence of Paraprobiotics-Containing Moisturizer on Skin Hydration and Microbiome: A Preliminary Study" Applied Sciences 12, no. 23: 12483. https://doi.org/10.3390/app122312483
APA StyleChaiyasut, C., Sivamaruthi, B. S., Tansrisook, C., Peerajan, S., Chaiyasut, K., & Bharathi, M. (2022). Influence of Paraprobiotics-Containing Moisturizer on Skin Hydration and Microbiome: A Preliminary Study. Applied Sciences, 12(23), 12483. https://doi.org/10.3390/app122312483