
Regular Physical Activity and Dental Erosion: A Systematic Review

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Extraction
- -
- For PubMed: ((dental erosion) OR (tooth erosion) OR (erosi* lesion)) AND ((sport* professional) OR (physical activity) OR (sport*) OR (athlet*) OR (runner) OR (football*) OR (player) OR (cyclist) OR (swimm*) OR (sport* drink) OR (isotonic*))
- -
- For Scopus: TITLE-ABS-KEY((“dental erosion”) OR (“tooth erosion”) OR (“erosi* lesion”)) AND ((“sport* professional”) OR (“physical activity”) OR (sport*) OR (athlet*) OR (runner) OR (football*) OR (player) OR (cyclist) OR (swimm*) OR (“sport* drink”) OR (“isotonic*”))
- -
- For Web of Science: TS = (dental erosion OR tooth erosion OR erosi* lesion) AND TS = (sport* professional OR physical activity OR sport* OR athlet* OR runner OR football* OR player OR cyclist OR swimm* OR sport* drink OR isotonic*).
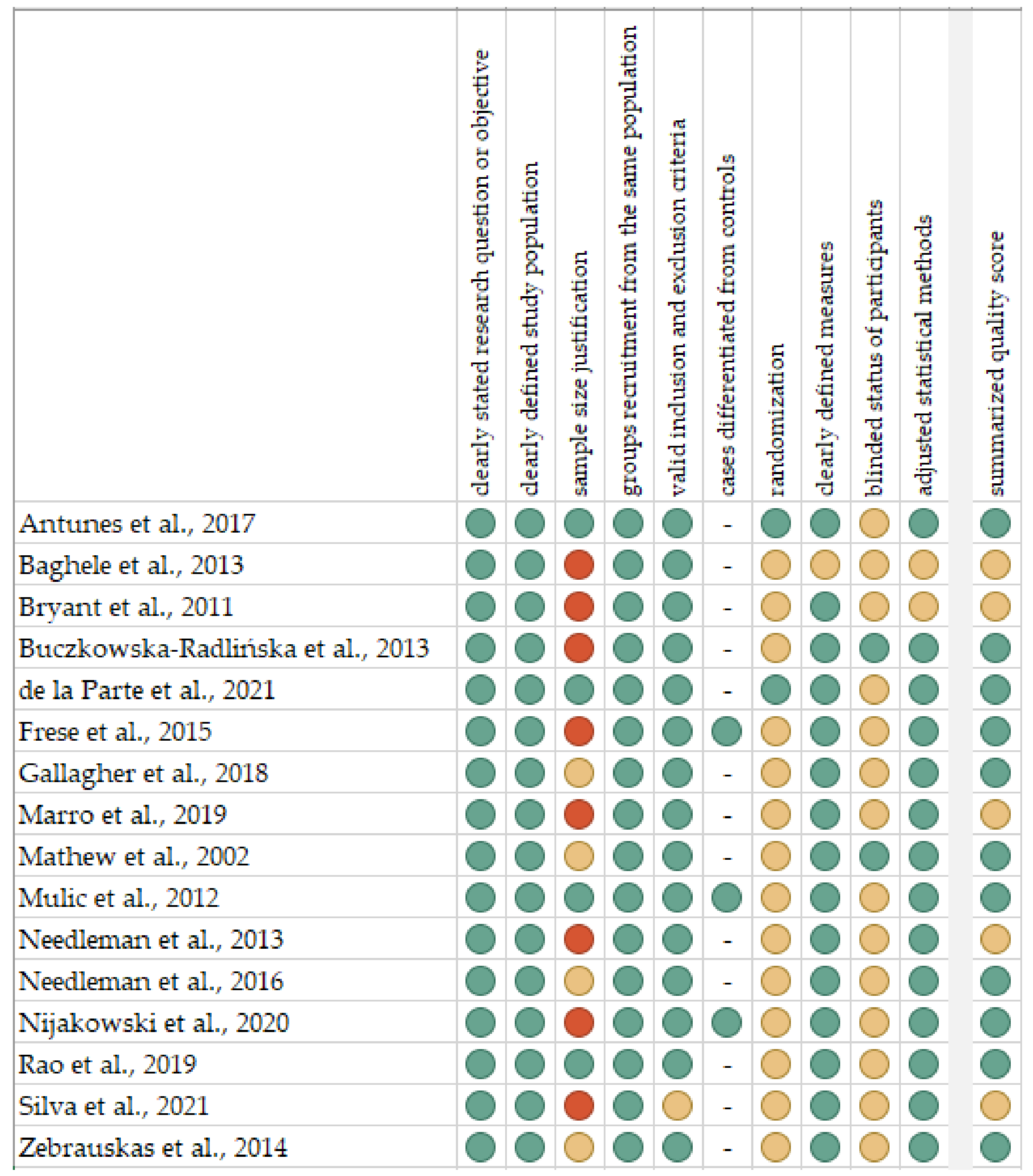
2.2. Quality Assessment and Critical Appraisal for the Systematic Review of Included Studies
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Imfeld, T. Dental Erosion. Definition, Classification and Links. Eur. J. Oral Sci. 1996, 104, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Lussi, A.; Jaeggi, T. Occupation and Sports. Monogr. Oral Sci. 2006, 20, 106–111. [Google Scholar] [CrossRef]
- Lussi, A.; Jaeggi, T. Erosion-Diagnosis and Risk Factors. Clin. Oral Investig. 2008, 12 (Suppl. 1), S5–S13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanzow, P.; Wegehaupt, F.J.; Attin, T.; Wiegand, A. Etiology and Pathogenesis of Dental Erosion. Quintessence Int. 2016, 47, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Zero, D.T.; Lussi, A. Erosion-Chemical and Biological Factors of Importance to the Dental Practitioner. Int. Dent. J. 2005, 55, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Wilson, M.A. Dental Erosion: A Case Study of a Marathon Runner. Dent. Update 2001, 28, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Salem, M.N.; Hafez, S. Aesthetic Management of Erosive Tooth Wear in a Young Egyptian Swimmer: A Case Report. Clin. Cosmet. Investig. Dent. 2021, 13, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Boonviriya, S.; Tannukit, S.; Jitpukdeebodintra, S. Effects of Tannin-Fluoride and Milk-Fluoride Mixture on Human Enamel Erosion from Inappropriately Chlorinated Pool Water. J. Oral Sci. 2017, 59, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Bertoldi, C.; Lucchi, A.; Zaffe, D. Effects of Soft-Drinks and Remineralising Treatment on Teeth Assessed by Morphological and Quantitative X-Ray Investigations. Eur. J. Paediatr. Dent. 2015, 16, 263–271. [Google Scholar] [PubMed]
- Buzalaf, M.A.R.; Magalhães, A.C.; Wiegand, A. Alternatives to Fluoride in the Prevention and Treatment of Dental Erosion. Monogr. Oral Sci. 2014, 25, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.; Loyn, T.; Chadwick, B. Pronamel and Tooth Mousse: An Initial Assessment of Erosion Prevention in Vitro. J. Dent. 2007, 35, 355–357. [Google Scholar] [CrossRef]
- Vongsawan, K.; Surarit, R.; Rirattanapong, P. The Effect of High Calcium Milk and Casein Phosphopeptide-Amorphous Calcium Phosphate on Enamel Erosion Caused by Cholinated Water. Southeast Asian J. Trop. Med. Public Health 2010, 41, 1494–1499. [Google Scholar] [PubMed]
- West, N.X.; Hooper, S.M.; O’Sullivan, D.; Hughes, N.; North, M.; Macdonald, E.L.; Davies, M.; Claydon, N.C.A. In Situ Randomised Trial Investigating Abrasive Effects of Two Desensitising Toothpastes on Dentine with Acidic Challenge Prior to Brushing. J. Dent. 2012, 40, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Absi, E.G.; Addy, M.; Adams, D. Dentine Hypersensitivity--the Effect of Toothbrushing and Dietary Compounds on Dentine in Vitro: An SEM Study. J. Oral Rehabil. 1992, 19, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Damo, D.M.; Arossi, G.A.; da Silva, H.A.; dos Santos, L.H.; Kappaun, D.R. Erosive Potential of Sports Beverages on Human Enamel “In Vitro”. Rev. Bras. Med. Esporte 2018, 24, 386–390. [Google Scholar] [CrossRef]
- Shellis, R.P.; Featherstone, J.D.B.; Lussi, A. Understanding the Chemistry of Dental Erosion. Monogr. Oral Sci. 2014, 25, 163–179. [Google Scholar] [CrossRef] [Green Version]
- Rees, J.; Loyn, T.; McAndrew, R. The Acidic and Erosive Potential of Five Sports Drinks. Eur. J. Prosthodont. Restor. Dent. 2005, 13, 186–190. [Google Scholar]
- Dawes, C. What Is the Critical PH and Why Does a Tooth Dissolve in Acid? J. Can. Dent. Assoc. 2003, 69, 722–724. [Google Scholar] [PubMed]
- Arnauteanu, C.; Stoleriu, S.; Iovan, G.; Sandu, A.V.; Iliescu, A.; Andrian, S. Comparative Study Regarding the Impact of Saliva on Chemical Disolution of Enamel Induced by Various Acidic Beverages. Rev. De Chim. Buchar. Orig. Ed. 2013, 64, 1335. [Google Scholar]
- Johansson, A.-K.; Lingström, P.; Imfeld, T.; Birkhed, D. Influence of Drinking Method on Tooth-Surface PH in Relation to Dental Erosion. Eur. J. Oral Sci. 2004, 112, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, A.L.; Xavier, A.F.C.; Souto, R.Q.; Oliveira, M.C.; dos Santos, J.A.; Vieira, F.F. In Vitro Evaluation of the Erosive Potential of Sports Drinks. Rev. Bras. Med. Esporte 2010, 16, 455–458. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 22 August 2020).
- OCEBM Levels of Evidence. Available online: https://www.cebm.net/2016/05/ocebm-levels-of-evidence/ (accessed on 22 August 2020).
- Antunes, L.S.; Veiga, L.; Nery, V.S.; Nery, C.C.; Antunes, L.A. Sports Drink Consumption and Dental Erosion among Amateur Runners. J. Oral Sci. 2017, 59, 639–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baghele, O.N.; Majumdar, I.A.; Thorat, M.S.; Nawar, R.; Baghele, M.O.; Makkad, S. Prevalence of Dental Erosion among Young Competitive Swimmers: A Pilot Study. Compend. Contin. Educ. Dent. 2013, 34, e20–e24. [Google Scholar]
- Bryant, S.; McLaughlin, K.; Morgaine, K.; Drummond, B. Elite Athletes and Oral Health. Int. J. Sports Med. 2011, 32, 720–724. [Google Scholar] [CrossRef] [PubMed]
- Buczkowska-Radlińska, J.; Łagocka, R.; Kaczmarek, W.; Górski, M.; Nowicka, A. Prevalence of Dental Erosion in Adolescent Competitive Swimmers Exposed to Gas-Chlorinated Swimming Pool Water. Clin. Oral Investig. 2013, 17, 579–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Parte, A.; Monticelli, F.; Toro-Roman, V.; Pradas, F. Differences in Oral Health Status in Elite Athletes According to Sport Modalities. Sustainability 2021, 13, 7282. [Google Scholar] [CrossRef]
- Frese, C.; Frese, F.; Kuhlmann, S.; Saure, D.; Reljic, D.; Staehle, H.J.; Wolff, D. Effect of Endurance Training on Dental Erosion, Caries, and Saliva. Scand. J. Med. Sci. Sports 2015, 25, e319–e326. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.; Ashley, P.; Petrie, A.; Needleman, I. Oral Health and Performance Impacts in Elite and Professional Athletes. Community Dent. Oral Epidemiol. 2018, 46, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Marro, F.; Fernandez, C.; Martens, L.; Jacquet, W.; Marks, L. Erosive Tooth Wear in Special Olympic Athletes with Intellectual Disabilities. BMC Oral Health 2019, 19, 37. [Google Scholar] [CrossRef]
- Mathew, T.; Casamassimo, P.S.; Hayes, J.R. Relationship between Sports Drinks and Dental Erosion in 304 University Athletes in Columbus, Ohio, USA. Caries Res. 2002, 36, 281–287. [Google Scholar] [CrossRef]
- Mulic, A.; Tveit, A.B.; Songe, D.; Sivertsen, H.; Skaare, A.B. Dental Erosive Wear and Salivary Flow Rate in Physically Active Young Adults. BMC Oral Health 2012, 12, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Needleman, I.; Ashley, P.; Petrie, A.; Fortune, F.; Turner, W.; Jones, J.; Niggli, J.; Engebretsen, L.; Budgett, R.; Donos, N.; et al. Oral Health and Impact on Performance of Athletes Participating in the London 2012 Olympic Games: A Cross-Sectional Study. Br. J. Sports Med. 2013, 47, 1054–1058. [Google Scholar] [CrossRef] [Green Version]
- Needleman, I.; Ashley, P.; Meehan, L.; Petrie, A.; Weiler, R.; McNally, S.; Ayer, C.; Hanna, R.; Hunt, I.; Kell, S.; et al. Poor Oral Health Including Active Caries in 187 UK Professional Male Football Players: Clinical Dental Examination Performed by Dentists. Br. J. Sports Med. 2016, 50, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Nijakowski, K.; Walerczyk-Sas, A.; Surdacka, A. Regular Physical Activity as a Potential Risk Factor for Erosive Lesions in Adolescents. Int. J. Environ. Res. Public. Health 2020, 17, 3002. [Google Scholar] [CrossRef] [PubMed]
- Rao, K.A.; Thomas, S.; Kumar, J.K.; Narayan, V. Prevalence of Dentinal Hypersensitivity and Dental Erosion among Competitive Swimmers, Kerala, India. Indian J. Community Med. Off. Publ. Indian Assoc. Prev. Soc. Med. 2019, 44, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.-R.G.; Chetti, M.-A.; Neves, H.; Manso, M.-C. Is the Consumption of Beverages and Food Associated to Dental Erosion? A Cross-Sectional Study in Portuguese Athletes. Sci. Sports 2021, 36, 477.e1–477.e11. [Google Scholar] [CrossRef]
- Zebrauskas, A.; Birskute, R.; Maciulskiene, V. Prevalence of Dental Erosion among the Young Regular Swimmers in Kaunas, Lithuania. J. Oral Maxillofac. Res. 2014, 5, e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | people practising sport professionally or with regular physical activity—aged from 0 to 99 years, both sexes | people with irregular physical activity; people only drinking sports beverages without declared physical activity |
| Intervention | not applicable | |
| Comparison | not applicable | |
| Outcomes | determined clinically erosive lesions (prevalence and/or severity) | determined only other dental indices |
| Study design | case-control, cohort and cross-sectional studies | literature reviews, case reports, expert opinion, letters to the editor, conference reports |
| published after 2000 | not published in English |
| Author, Year, Setting | Participants (F/M) | Age [Years] | Controls (F/M; Age) | Kind of Physical Activity | Kind of Beverages | Clinical Indices for Erosion |
|---|---|---|---|---|---|---|
| Antunes et al., 2017, Brazil [25] | 108 (41/67) | 18–60; mean 34.1 | - | amateur running | sports drinks | dental wear and type according to Eccles |
| Baghele et al., 2013, India [26] | 100 (25/75) | mean 17.8 | - | swimming | NR | presence according to Eccles and Jenkins |
| Bryant et al., 2011, New Zealand [27] | 31 (16/15) | 18–36; mean 24.2 | - | triathlon (swimming, cycling, running) | sports drinks | presence according to Eccles and Jenkins |
| Buczkowska-Radlińska et al., 2013, Poland [28] | 62 competitive swimmers (25/37), 69 recreational swimmers (34/35) | 14–16 | - | swimming | acidic drinks | Lussi Index |
| de la Parte et al., 2021, Spain [29] | 74 individual sports (21/53), 112 team sports (15/97) | 18–35; mean 24.7 | - | individual (fencing, tennis, table tennis, athletics, rowing, canoeing, cycling, cross-country skiing, alpine skiing, judo, triathlon, karate, trail running, paddle, badminton, orienteering, bicycle motocross, swimming, rhythmic gymnastics, climbing, and taekwondo) or team (volleyball, basketball, ice hockey, handball, soccer, and water polo) | energy/sugary drinks | presence according to the WHO criteria |
| Frese et al., 2015, Germany [30] | 35 (11/24) | 21–48; mean 36.8 | 35 (sex-and age-matched) | triathlon (swimming, cycling, running) | sports drinks | BEWE |
| Gallagher et al., 2018, UK [31] | 344 (114/230) | 18–39; mean 25.0 | - | athletics, gymnastics, sprint cycling and sprint swimming; swimming, cycling, rowing; football, rugby, hockey, sailing | NR | BEWE |
| Marro et al., 2019, Belgium [32] | 232 (97 with DS.) | 9–62; mean 23.9 | - | Special Olympics | NR | BEWE |
| Mathew et al., 2002, USA [33] | 304 (119/185) | 18–28; mean 19.0 | - | football, lacrosse | sports drinks | Lussi Index |
| Mulic et al., 2012, Norway [34] | 104 (68/36) | 18–32; mean 25.0 | 116 (75/41; 18-year-old) | fitness | acidic drinks (including sports drinks) | VEDE |
| Needleman et al., 2013, UK [35] | 278 (119/159) | 16–47; mean 25.7 | - | the London 2012 Olympic Games: track and field, boxing, hockey, swimming, water polo, judo, volleyball, shooting, football, weightlifting, fencing, archery, handball, beach volleyball, taekwondo, wrestling, cycling, basketball, canoeing, gymnastics, equestrian, sailing, table tennis, rowing, badminton | sports drinks | BEWE |
| Needleman et al., 2016, UK [36] | 187 (0/187) | 18–39; median 24.0 | - | football | sports drinks | BEWE |
| Nijakowski et al., 2020, Poland [37] | 102 (48/54) | 15–18 | 53 (35/18; 15–18) | team sports, fighting sports, water sports, individual sports | sports drinks | BEWE |
| Rao et al., 2019, India [38] | 56 (21/35) | mean 15.0 | - | swimming | fizzy drinks | presence according to the WHO criteria |
| Silva et al., 2021, Portugal [39] | 110 (54/56): 55 swimmers and 55 non-swimmers | 13–62; mean 27.9 | - | swimming, bodybuilding, football, boxing, volleyball, and running | energy/sports drinks | BEWE |
| Zebrauskas et al., 2014, Lithuania [40] | 132 (48/84) | 12–25 | - | swimming | sports and soft drinks | Lussi Index |
| Study | Physical Activity Frequency | Sports Drink Consumption | Sports Drink Consumption Frequency | Erosion Frequency | Erosion Severity |
|---|---|---|---|---|---|
| Antunes et al., 2017 [25] | 33.3% more than 3 times a week | 38.9% | regularly | 19.4% | Classes 1 and 2 according to Eccles |
| Baghele et al., 2013 [26] | 95% more than 2 h a day | - | - | 90% | NR |
| Bryant et al., 2011 [27] | average training time per week 20.6 h | 84% | 53.8% more than 2 times a week | 0% | - |
| Buczkowska-Radlińska et al., 2013 [28] | competitive over 19 h per week; recreational less than 2 h per week | - | - | more than 26% in competitive and 10% in recreational | 100% with grade 1 according to the Lussi Index |
| de la Parte et al., 2021 [29] | at least 5 h per week | NR | NR | 68.9% in individual sports, 55.4% in team sports | NR |
| Frese et al., 2015 [30] | average 9.5 h per week | 45.7% | average 592.9 mL per hour | NR | average cumulative BEWE 9.6 |
| Gallagher et al., 2018 [31] | NR | - | - | 41.4% | 28.9% with total BEWE > 8 |
| Marro et al., 2019 [32] | NR | - | - | 62.1% | 27.1% with BEWE = 2, 26.4% with BEWE = 3 |
| Mathew et al., 2002 [33] | NR | 91.8% | 64.3% at least 1 L daily | 36.5% | 75.2% with grade 1 according to the Lussi Index |
| Mulic et al., 2012 [34] | 55% more than 3 times a week | NR | 3% once per day or more | 64% (vs. 20% in controls) | 37.3% with erosion involved dentine |
| Needleman et al., 2013 [35] | NR | NR | - | 44.6% | 38% anterior teeth and 48% posterior teeth with BEWE > 1 |
| Needleman et al., 2016 [36] | NR | 92.9% | 68.6% at least 3 times a week | 53.1% | 21% with BEWE > 1 |
| Nijakowski et al., 2020 [37] | NR | 17.6% | NR | 59.8% (vs. 22.6%) | 100% with total BEWE < 9 |
| Rao et al., 2019 [38] | average training time per session 2 h | - | - | 48.2 | NR |
| Silva et al., 2021 [39] | average 4.2 times a week; 79.1% with training >60 min | 35.5% | 43.6% at least during each training | 83.6% | 8.7% with total BEWE > 8 |
| Zebrauskas et al., 2014 [40] | 21.2% more than 6 h a day | 27.2% | daily | 35.6% | 100% with grade 1 according to the Lussi Index |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nijakowski, K.; Zdrojewski, J.; Nowak, M.; Podgórski, F.; Surdacka, A. Regular Physical Activity and Dental Erosion: A Systematic Review. Appl. Sci. 2022, 12, 1099. https://doi.org/10.3390/app12031099
Nijakowski K, Zdrojewski J, Nowak M, Podgórski F, Surdacka A. Regular Physical Activity and Dental Erosion: A Systematic Review. Applied Sciences. 2022; 12(3):1099. https://doi.org/10.3390/app12031099
Chicago/Turabian StyleNijakowski, Kacper, Jakub Zdrojewski, Monika Nowak, Filip Podgórski, and Anna Surdacka. 2022. "Regular Physical Activity and Dental Erosion: A Systematic Review" Applied Sciences 12, no. 3: 1099. https://doi.org/10.3390/app12031099
APA StyleNijakowski, K., Zdrojewski, J., Nowak, M., Podgórski, F., & Surdacka, A. (2022). Regular Physical Activity and Dental Erosion: A Systematic Review. Applied Sciences, 12(3), 1099. https://doi.org/10.3390/app12031099