
Blood Pressure Estimation by Photoplethysmogram Decomposition into Hyperbolic Secant Waves

 , ,
, , 
Abstract
:1. Introduction
2. Methods
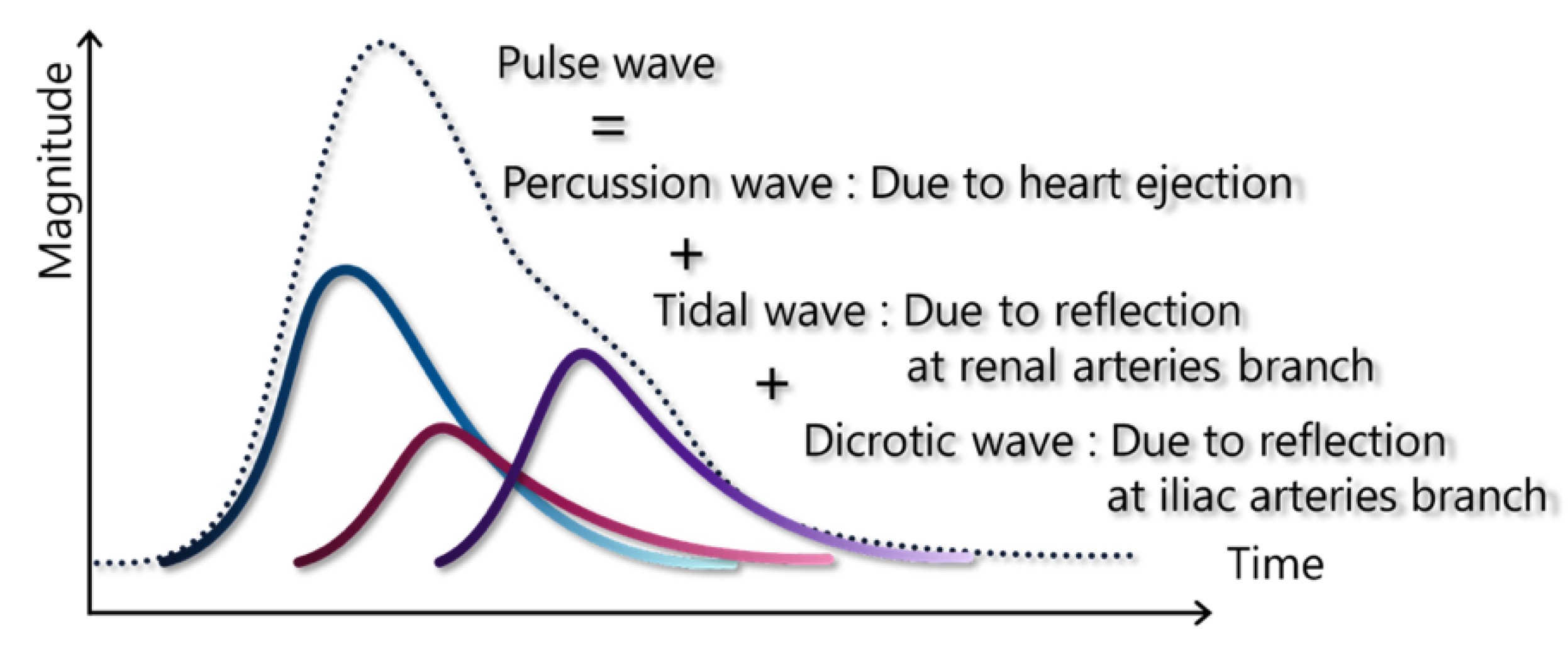
2.1. Pulse Wave Model for Blood Pressure Estimation
2.1.1. Mathematical Models for Pulse Decomposition Analysis
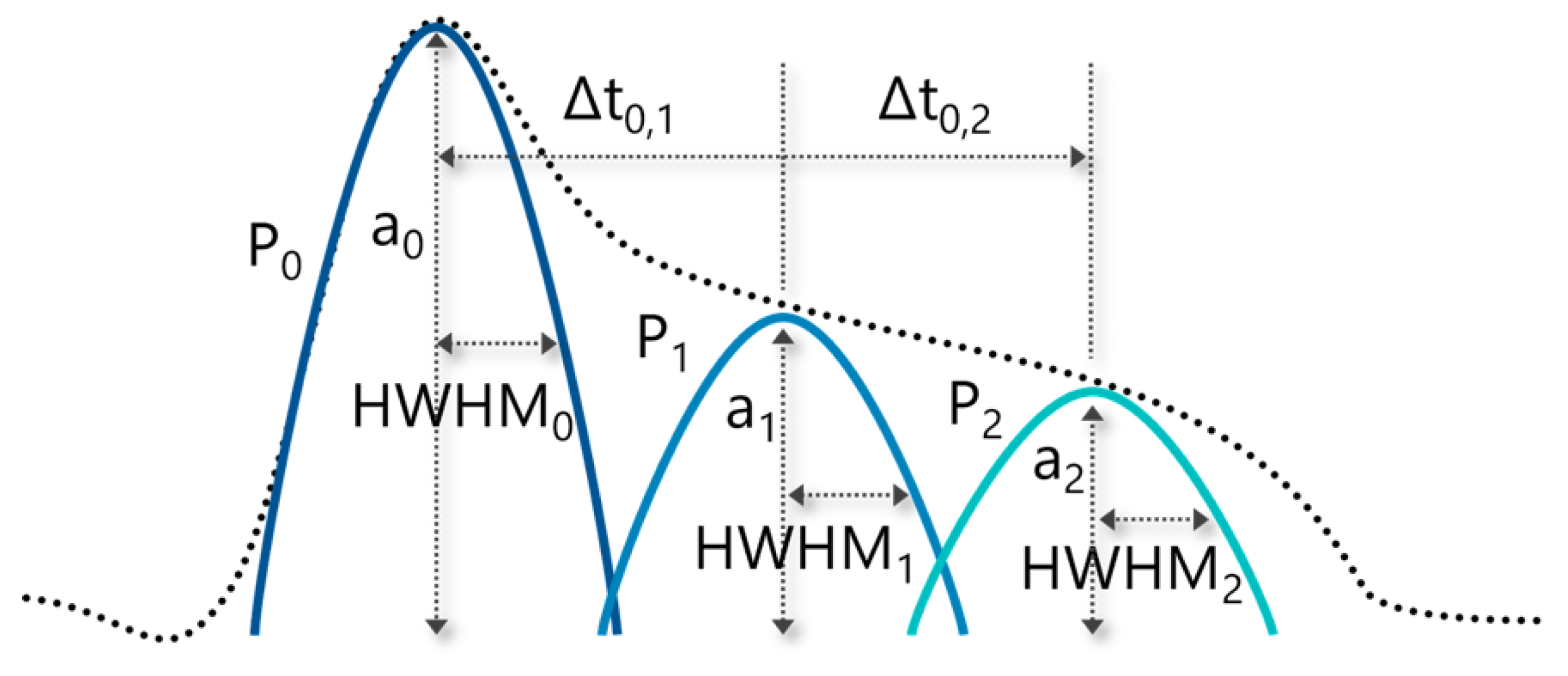
2.1.2. Features Extraction from Decomposed Waves Based on Pulse Wave
2.1.3. Multiple Regression for the Relationship between the Features and Blood Pressure
2.2. Dataset Construction for the Verification of Our Proposed Method
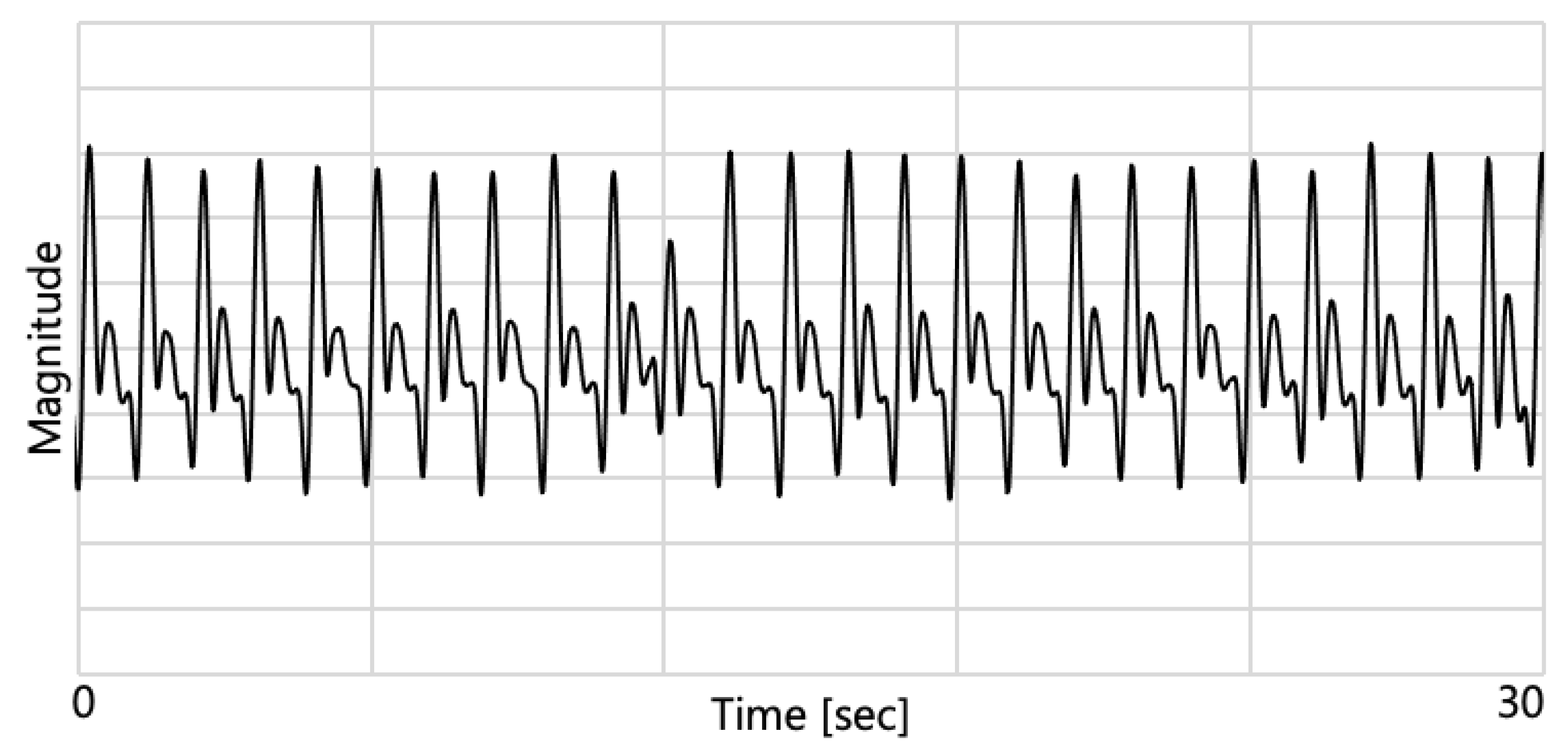
2.2.1. Vital Signs Acquisition
2.2.2. Data Pre-Processing
2.3. The Verification of Our Proposed Method
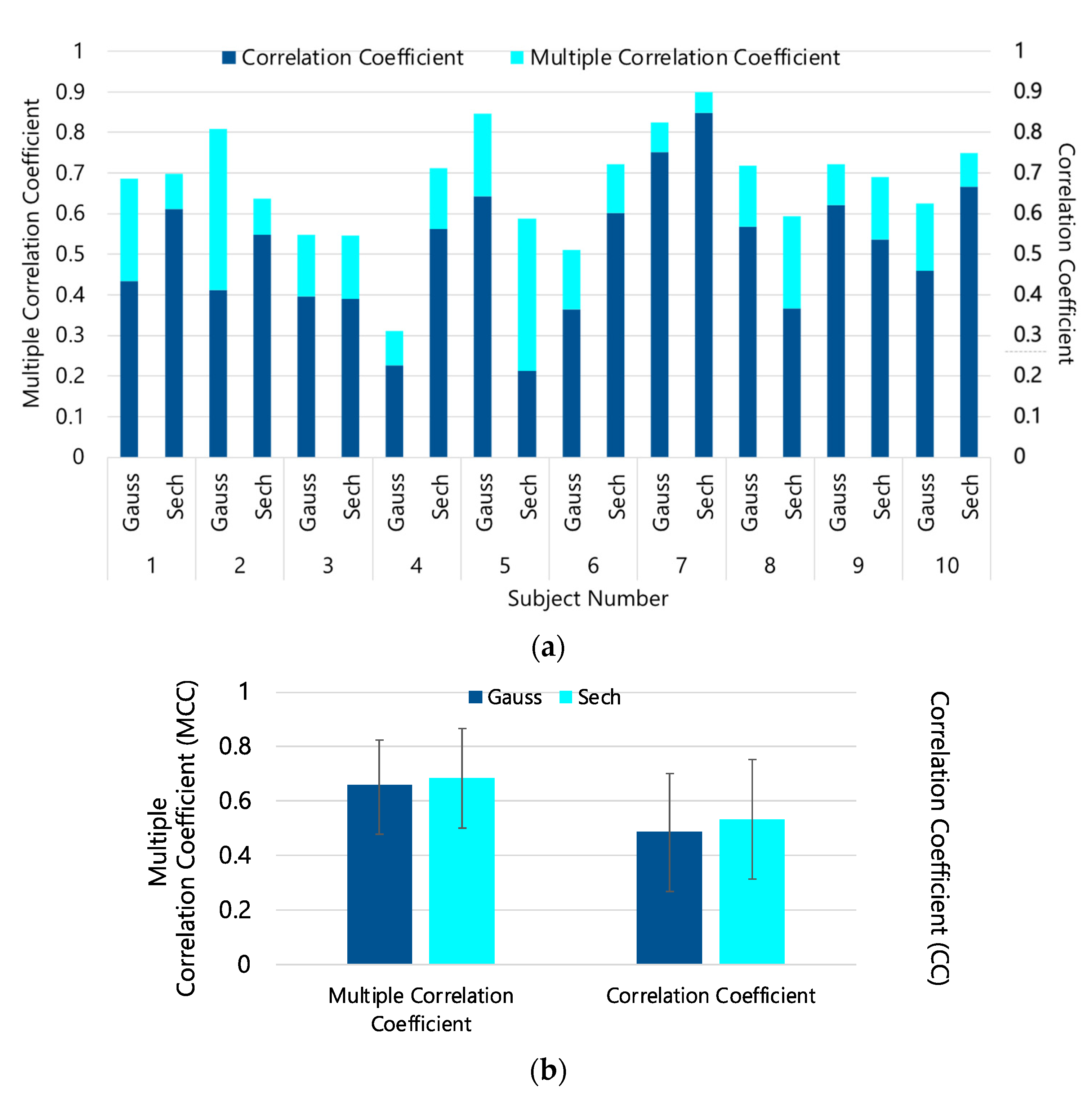
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vrijkotte, T.G.; Van Doornen, L.J.; De Geus, E.J. Effects of work stress on ambulatory blood pressure, heart rate, and heart rate variability. Hypertension 2000, 35, 880–886. [Google Scholar] [CrossRef]
- Zheng, W.; Zhang, S.; Deng, Y.; Wu, S.; Ren, J.; Sun, G.; Yang, J.; Jiang, Y.; Xu, X.; Wang, T.; et al. Trial of intensive blood-pressure control in older patients with hypertension. N. Engl. J. Med. 2021, 385, 1268–1279. [Google Scholar] [CrossRef] [PubMed]
- McGhee, B.H.; Bridges, E.J. Monitoring arterial blood pressure: What you may not know. Crit. Care Nurse 2002, 22, 60–79. [Google Scholar] [CrossRef]
- Alpert, B.S.; Quinn, D.; Gallick, D. Oscillometric blood pressure: A review for clinicians. J. Am. Soc. Hypertens. 2014, 8, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Drzewiecki, G.; Hood, R.; Apple, H. Theory of the oscillometric maximum and the systolic and diastolic detection ratios. Ann. Biomed. Eng. 1994, 22, 88–96. [Google Scholar] [CrossRef]
- Couceiro, R.; Carvalho, P.; Paiva, R.P.; Henriques, J.; Quintal, I.; Antunes, M.; Muehlsteff, J.; Eickholt, C.; Brinkmeyer, C.; Kelm, M.; et al. Assessment of cardiovascular function from multi-Gaussian fitting of a finger photoplethysmogram. Physiol. Meas. 2015, 36, 1801. [Google Scholar] [CrossRef] [PubMed]
- Baruch, M.C.; Kalantari, K.; Gerdt, D.W.; Adkins, C.M. Validation of the pulse decomposition analysis algorithm using central arterial blood pressure. Biomed. Eng. Online 2014, 13, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teng, X.F.; Zhang, Y.T. Continuous and noninvasive estimation of arterial blood pressure using a photoplethysmographic approach. In Proceedings of the 25th Annual International Conference IEEE Engineering Medicine and Biology Society, Cancun, Mexico, 17–21 September 2003; pp. 3153–3156. [Google Scholar]
- Suzuki, S.; Oguri, K. Cuffless and and non-invasive systolic blood pressure estimation for aged class by using a photoplethysmography. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 1327–1330. [Google Scholar]
- Kurylyak, Y.; Lamonaca, F.; Grimaldi, D. A neural network-based method for continuous blood pressure estimation from a PPG signal. In Proceedings of the 2013 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Minneapolis, MN, USA, 6–9 May 2013; pp. 280–283. [Google Scholar]
- Yoon, Y.Z.; Kang, J.M.; Kwon, Y.; Park, S.; Noh, S.; Kim, Y.; Park, J.; Hwang, S.W. Cuff-Less Blood Pressure Estimation Using Pulse Waveform Analysis and Pulse Arrival Time. IEEE J. Biomed. Health Inform. 2017, 22, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Jeong, I.C.; Finkelstein, J. Introducing contactless blood pressure assessment using a high speed video camera. J. Med. Syst. 2016, 40, 77. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.L.; Yan, B.P.; Zhang, Y.T.; Poon, C.C. An armband wearable device for overnight and cuff-less blood pressure measurement. IEEE Trans. Biomed.-Med. Eng. 2014, 61, 2179–2186. [Google Scholar] [CrossRef] [PubMed]
- Sawada, Y.; Tanaka, G.; Yamakoshi, K.I. Normalized pulse volume (NPV) derived photo-plethysmographically as a more valid measure of the finger vascular tone. Int. J. Psychophysiol. 2001, 41, 1–10. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Ranta-Aho, P.O.; Karjalainen, P.A. An advanced detrending method with application to HRV analysis. IEEE Trans. Biomed. Eng. 2002, 49, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Rodríguez, J.C.; Ruiz-Sanmartín, A.; Ribas, V.; Caballero, J.; García-Roche, A.; Riera, J.; Nuvials, X.; de Nadal, M.; de Sola-Morales, O.; Serra, J.; et al. Innovative continuous non-invasive cuffless blood pressure monitoring based on photoplethysmography technology. Intensive Care Med. 2013, 39, 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- De Souza, R.P.; Janke, B.; Cardoso, G.C. Decomposição de pulsos fotopletismográfico para redução da incerteza do Tempo de Trânsito. Rev. Bras. Física Médica 2020, 14, 546–554. [Google Scholar]
- Tang, Q.; Chen, Z.; Ward, R.; Elgendi, M. Synthetic photoplethysmogram generation using two Gaussian functions. Sci. Rep. 2020, 10, 13883. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Combination of Features | ||
|---|---|---|
| Subject Number | Sech-PDA | Gaussian-PDA |
| 1 | Δt0,1, FWHM2 | Δt0,2, a1, a2, FWHM1, FWHM2, FWHM3 |
| 2 | a3, FWHM1, FWHM2, FWHM3 | Δt0,2, FWHM1 |
| 3 | Δt0,1, a1, a2, FWHM2 | Δt0,1, a2 |
| 4 | Δt0,1, a1, a2, FWHM1 | Δt0,1, FWHM1 |
| 5 | FWHM2, FWHM3 | Δt0,1, FWHM1, FWHM2, FWHM3 |
| 6 | Δt0,1, a2, a3, FWHM3 | Δt0,1, Δt0,2, a1, a2, FWHM1 |
| 7 | a1, a3, FWHM2, FWHM3 | Δt0,1, FWHM3 |
| 8 | Δt0,1, a3 | Δt0,1, a1, a2, a3, FWHM1, FWHM2, FWHM3 |
| 9 | Δt0,1, a2, FWHM1, FWHM2 | Δt0,1, a2, FWHM1, FWHM2 |
| 10 | Δt0,1, Δt0,2, a2, FWHM1, FWHM2 | Δt0,1, a1, a2, FWHM2, FWHM3 |
| all | a2, FWHM1, FWHM2 | Δt0,1, Δt0,2, a2, FWHM2, FWHM3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagasawa, T.; Iuchi, K.; Takahashi, R.; Tsunomura, M.; de Souza, R.P.; Ogawa-Ochiai, K.; Tsumura, N.; Cardoso, G.C. Blood Pressure Estimation by Photoplethysmogram Decomposition into Hyperbolic Secant Waves. Appl. Sci. 2022, 12, 1798. https://doi.org/10.3390/app12041798
Nagasawa T, Iuchi K, Takahashi R, Tsunomura M, de Souza RP, Ogawa-Ochiai K, Tsumura N, Cardoso GC. Blood Pressure Estimation by Photoplethysmogram Decomposition into Hyperbolic Secant Waves. Applied Sciences. 2022; 12(4):1798. https://doi.org/10.3390/app12041798
Chicago/Turabian StyleNagasawa, Takumi, Kaito Iuchi, Ryo Takahashi, Mari Tsunomura, Raquel Pantojo de Souza, Keiko Ogawa-Ochiai, Norimichi Tsumura, and George C. Cardoso. 2022. "Blood Pressure Estimation by Photoplethysmogram Decomposition into Hyperbolic Secant Waves" Applied Sciences 12, no. 4: 1798. https://doi.org/10.3390/app12041798
APA StyleNagasawa, T., Iuchi, K., Takahashi, R., Tsunomura, M., de Souza, R. P., Ogawa-Ochiai, K., Tsumura, N., & Cardoso, G. C. (2022). Blood Pressure Estimation by Photoplethysmogram Decomposition into Hyperbolic Secant Waves. Applied Sciences, 12(4), 1798. https://doi.org/10.3390/app12041798