
The Impact of Technical Error of Measurement on Somatotype Categorization



Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
3. Results
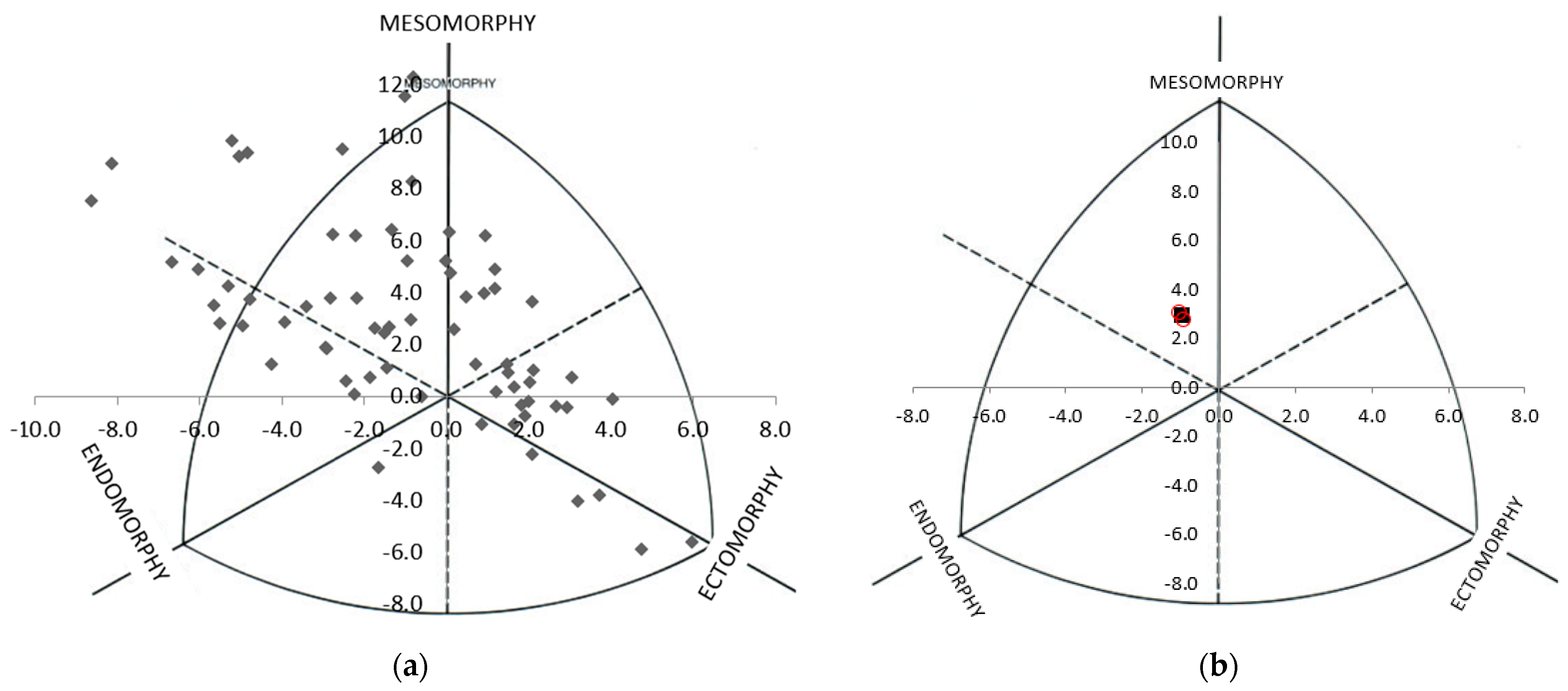
3.1. Somatotype Distribution
3.2. Somatotype Categorization
4. Discussion

{kind=link}
{kind=link}
| Author, Year | Participants | Population Somatotype | Somatotype Grouping | TEMs Reported? | Potential for Mis-Classification |
|---|---|---|---|---|---|
| Busko et al., 2017 [14] | 15 male Judoists (training experience 10.0 ± 2.8 years); 154 untrained students. | Judoists: 3.21 [±0.78], 5.87 [±1.16], 1.83 [±0.96]. Untrained: 3.90 [±1.56], 4.60 [±1.14], 2.88 [±1.27] | Simple | No | Up to 6 judoists and 59 untrained students. |
| Roklicer et al., 2020 [15] | 61 male judokas, 37 female judokas separated into 7 weight categories | Males range: 1.69–2.92, 3.65–6.35, 0.91–3.99 Females range: 2.17–4.44, 2.71–5.68, 0.22–3.48. | In descriptive text—detailed. | No | Up to 44 male and 27 female judokas. |
| Guereno et al., 2018 [16] | 20 elite male rowers | 3.5 [±0.4], 4.7 [±0.6], 2.4 [±3.5] | In descriptive text—detailed | No | Up to 15 participants |
| Gryko et al., 2018 [17] | 70 male basketball players (young [n = 35] and adult [n = 35]) | Young: 2.12 [±0.81], 3.75 [±1.01], 4.17 [±1.08]. Adult: 2.26 [±0.59], 4.57 [±1.07], 3.04 [±0.89]. | In descriptive text—detailed. | No | Up to 50 participants |
| Giannopoulos et al., 2017 [18] | 144 Greek male volleyball players grouped by Division and position | 3.05 [±0.74], 2.32 [±1.09], 2.93 [±1.01] | Detailed | Test-retest reliability but no TEM provided. | Up to 104 participants |
| Cardenas-Fernandez et al., 2019 [20] | 174 youth soccer players (U14 n = 34; U16 n = 40; U19 n = 100) | Range: 2.8–4.5, 3.2–5.2, 2.2–3.9 | Detailed | Yes—<3% for skinfolds, <1% all other measures. | Up to 69 players (U14 = 13; U16 = 16; U19 = 40). |
| Cinarli and Kafkas, 2019 [22] | 150 untrained males | Median: 2.8, 4.3, 2.6. | Detailed | No | Up to 108 participants |
| Chatterjee et al., 2019 [23] | 148 trained athletes (aged 10–20 years) | Not given | Simple | No | Up to 57 participants |
| Sunitha and Joseph, 2018 [30] | 60 male PE students (15–17 years) | Not given | Simple | No | Up to 23 participants |
| Bolunchuk et al., 2000 [35] | 63 male participants | 3.1 [±0.2], 3.7 [±0.2], 2.4 [±0.2] | Simple | Yes, <0.2 somatotype units. | 19 participants |
| Chaouachi et al., 2005 [36] | 41 fit PE students | Range: 1.7–4.1, 2.0–4.8, 2.1–5.0. | Detailed | No | 30 participants |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- Hopkins, W.G. Measures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Harris, E.F.; Smith, R.N. Accounting for measurement error: A critical but often overlooked process. Arch. Oral Biol. 2009, 54, S107–S117. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; de Ridder, H. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Wellington, New Zealand, 2011. [Google Scholar]
- Ulijaszek, S.J.; Kerr, D.A. Anthropometric measurement error and the assessment of nutritional status. Br. J. Nutr. 1999, 82, 165–177. [Google Scholar] [CrossRef] [Green Version]
- Hume, P.; Marfell-Jones, M. The importance of accurate site location for skinfold measurement. J. Sports Sci. 2008, 26, 1333–1340. [Google Scholar] [CrossRef]
- Mueller, W.H.; Martorell, R. Reliability and accuracy of measurement. In Anthropometric Standardisation Reference Manual; Lohman, T.G., Roche, A.F., Martorell, R., Eds.; Human Kinetics Books: Champaign, IL, USA, 1988; pp. 83–86. [Google Scholar]
- Perini, T.A.; de Oliveira, G.L.; Ornellas, J.d.S.; de Oliveira, F.P. Technical error of measurement in anthropometry. Rev. Bras. Med. Esporte 2005, 11, 86–90. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; SAGE: London, UK, 2009. [Google Scholar]
- Eliasziw, M.; Young, S.L.; Woodbury, M.G.; Fryday-Field, K. Statistical Methodology for the Concurrent Assessment of Interrater and Intrarater Reliability: Using Goniometric Measurements as an Example. Phys. Ther. 1994, 74, 777–788. [Google Scholar] [CrossRef]
- Willgoose, C.E.; Rogers, M.L. Relationship of Somatotype to Physical Fitness. J. Educ. Res. 1949, 42, 704–712. [Google Scholar] [CrossRef]
- Carter, J.E.; Heath, B.H. Somatotyping Development and Applications; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Carter, J.E.L. Somatotyping. In Anthropometrica; Norton, K., Olds, T., Eds.; University of New South Wales Press: Sydney, Australia, 2002; pp. 147–170. [Google Scholar]
- Buśko, K.; Pastuszak, A.; Kalka, E. Body composition and somatotype of judo athletes and untrained male students as a reference group for comparison in sport. Biomed. Hum. Kinet. 2017, 9, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Roklicer, R.; Atanasov, D.; Sadri, F.; Jahic, D.; Bojanic, D.; Ljubojevic, M.; Trivic, T.; Drid, P. Somatotype of male and female judokas according to weight categories. Biomed. Hum. Kinet. 2020, 12, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Guereño, P.L.; Otegui, A.U.; Zourdos, M.C.; Ayuso, J.M. Anthropometric profile, body composition and somatotype in elite traditional rowers: A cross-sectional study. Rev. Esp. Nutr. Hum. Diet. 2018, 22, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Gryko, K.; Kopiczko, A.; Mikołajec, K.; Stasny, P.; Musálek, M. Anthropometric Variables and Somatotype of Young and Professional Male Basketball Players. Sports 2018, 6, 9. [Google Scholar] [CrossRef] [Green Version]
- Giannopoulos, N.; Vagenas, G.; Noutsos, K.; Barzouka, K.; Bergeles, N. Somatotype, Level of Competition, and Performance in Attack in Elite Male Volleyball. J. Hum. Kinet. 2017, 58, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Kandel, M.; Baeyens, J.P.; Clarys, P. Somatotype, training and performance in Ironman athletes. Eur. J. Sport Sci. 2013, 14, 301–308. [Google Scholar] [CrossRef]
- Cárdenas-Fernández, V.; Chinchilla-Minguet, J.L.; Castillo-Rodríguez, A. Somatotype and Body Composition in Young Soccer Players According to the Playing Position and Sport Success. J. Strength Cond. Res. 2019, 33, 1904–1911. [Google Scholar] [CrossRef]
- Ryan-Stewart, H.; Faulkner, J.; Jobson, S. The influence of somatotype on anaerobic performance. PLoS ONE 2018, 13, e0197761. [Google Scholar] [CrossRef]
- Çinarli, F.; Kafkas, M. The effect of somatotype characters on selected physical performance parameters. Phys. Educ. Stud. 2019, 23, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, P.; Bandyopadhyay, A.; Chatterjee, P.; Nandy, P. Assessment and Comparative Analysis of Different Lung Capacities in Trained Athletes According to Somatotype. Am. J. Sports Sci. 2019, 7, 72–77. [Google Scholar] [CrossRef]
- Arroyo, M.; Freire, M.; Ansotegui, L.; Rocandio, A.M. Intraobserver error associated with anthropometric measurements made by dietitians. Nutr. Hosp. 2010, 25, 1053–1056. [Google Scholar] [PubMed]
- Buśko, K.; Lewandowska, J.; Lipińska, M.; Michalski, R.; Pastuszak, A. Somatotype-variables related to muscle torque and power output in female volleyball players. Acta Bioeng. Biomech. 2013, 15, 119–126. [Google Scholar]
- Ferrari, E.P.; Silva, D.A.S.; Martins, C.R.; Fidelix, Y.L.; Petroski, E.L. Morphological characteristics of professional ballet dancers of the Bolshoi theater company. Coll. Antropol. 2013, 37, 37–43. [Google Scholar] [PubMed]
- Marta, C.C.; Marinho, D.A.; Barbosa, T.M.; Carneiro, A.L.; Izquierdo, M.; Marques, M.C. Effects of Body Fat and Dominant Somatotype on Explosive Strength and Aerobic Capacity Trainability in Prepubescent Children. J. Strength Cond. Res. 2013, 27, 3233–3244. [Google Scholar] [CrossRef] [PubMed]
- Grgantov, Z.; Padulo, J.; Milić, M.; Ardigò, L.P.; Erceg, M.; Cular, D. Intra-Positional and Inter-Positional Differences in Somatotype Components and Proportions of Particular Somatotype Categories in Youth Volleyball Players. Ann. Appl. Sport Sci. 2017, 5, 37–49. [Google Scholar] [CrossRef]
- Gjonbalaj, M.; Georgiev, G.; Bjelica, D. Differences in Anthropometric Characteristics, Somatotype Components, and Functional Abilities among Young Elite Kosovo Soccer Players Based on Team Position. Int. J. Morphol. 2018, 36, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Sunitha, K.B.; Joseph, M.M. Effect of dominant somatotype on motor quality trainability. Yoga 2018, 3, 880–883. [Google Scholar]
- Goto, R.; Mascie-Taylor, C.N. Precision of Measurement as a Component of Human Variation. J. Physiol. Anthr. 2007, 26, 253–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvero-Cruz, J.R.; Mathias, V.P.; García-Romero, J.C. Somatotype Components as Useful Predictors of Disordered Eating Attitudes in Young Female Ballet Dance Students. J. Clin. Med. 2020, 9, 2024. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Munoz, C.; Muros, J.J.; Lopez Belmonte, O.; Zabala, M. Anthropometric characteristics, body composition and somatotype of elite male young runners. Int. J. Environ. Res. Public Health 2020, 17, 674. [Google Scholar] [CrossRef] [Green Version]
- Bolonchuk, W.W.; Siders, W.A.; Lykken, G.I.; Lukaski, H.C. Association of dominant somatotype of men with body structure, function during exercise, and nutritional assessment. Am. J. Hum. Biol. 2000, 12, 167–180. [Google Scholar] [CrossRef]
- Chaouachi, M.; Chaouachi, A.; Chamari, K.; Chtara, M.; Feki, Y.; Amri, M.; Trudeau, F. Effects of dominant somatotype on aerobic capacity trainability. Br. J. Sports Med. 2005, 39, 954–959. [Google Scholar] [CrossRef] [Green Version]
- Carter, J.E.L.; Mirwald, R.L.; Heath-Roll, B.H.; Bailey, D.A. Somatotypes of 7- to 16-year-old boys in Saskatchewan, Canada. Am. J. Hum. Biol. 1997, 9, 257–272. [Google Scholar] [CrossRef]


| Somatotype Category | RTEM | L23TEM | L1TEM |
|---|---|---|---|
| Detailed | 39.7% | 61.8% | 72.1% |
| Simplified | 29.4% | 35.3% | 38.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryan-Stewart, H.; Faulkner, J.; Jobson, S. The Impact of Technical Error of Measurement on Somatotype Categorization. Appl. Sci. 2022, 12, 3056. https://doi.org/10.3390/app12063056
Ryan-Stewart H, Faulkner J, Jobson S. The Impact of Technical Error of Measurement on Somatotype Categorization. Applied Sciences. 2022; 12(6):3056. https://doi.org/10.3390/app12063056
Chicago/Turabian StyleRyan-Stewart, Helen, James Faulkner, and Simon Jobson. 2022. "The Impact of Technical Error of Measurement on Somatotype Categorization" Applied Sciences 12, no. 6: 3056. https://doi.org/10.3390/app12063056
APA StyleRyan-Stewart, H., Faulkner, J., & Jobson, S. (2022). The Impact of Technical Error of Measurement on Somatotype Categorization. Applied Sciences, 12(6), 3056. https://doi.org/10.3390/app12063056