
Calculation of Intracoronary Pressure-Based Indexes with JLabChart


 , ,
, ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Material and Methods
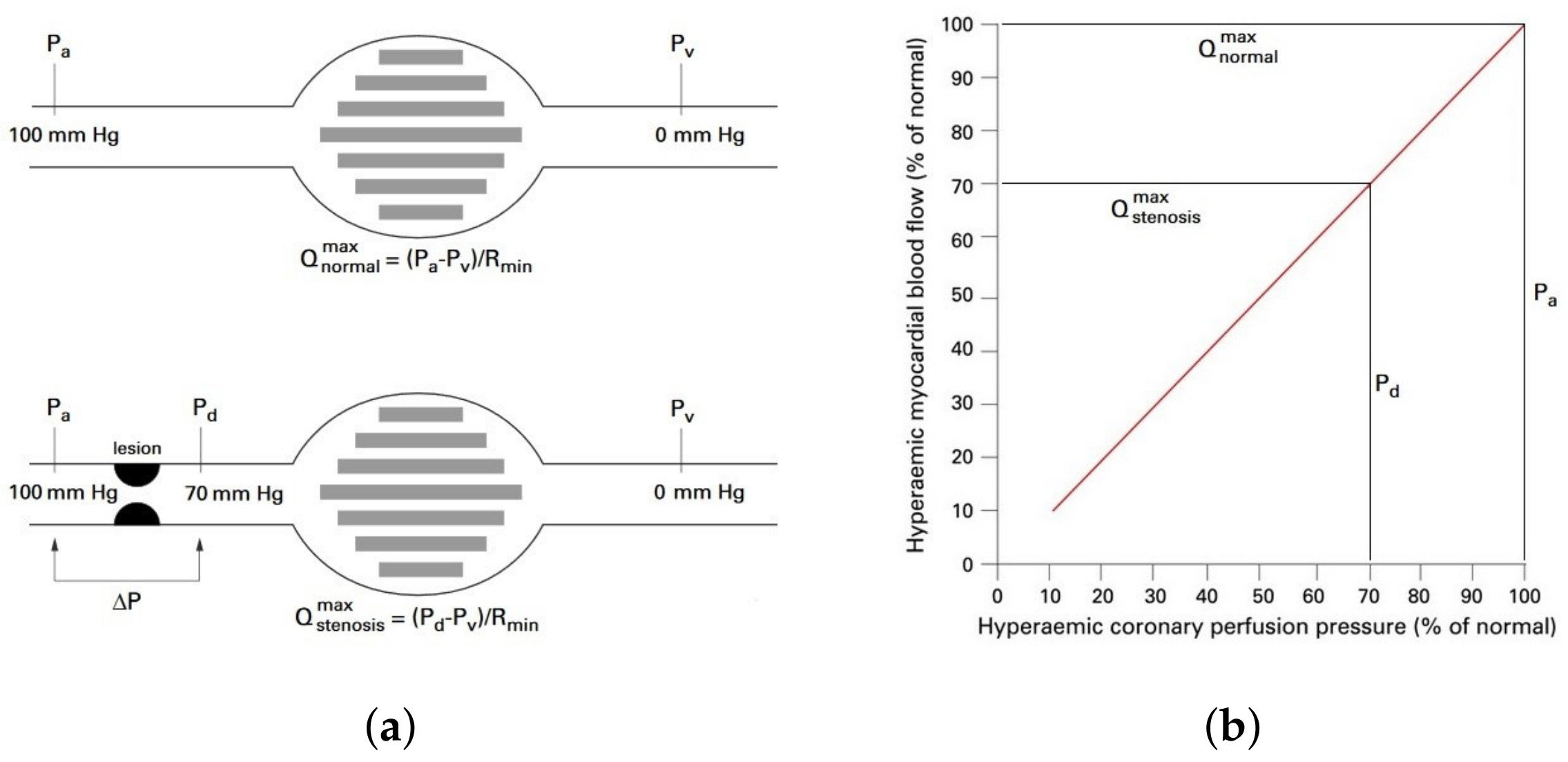
2.1. Fractional Flow Reserve
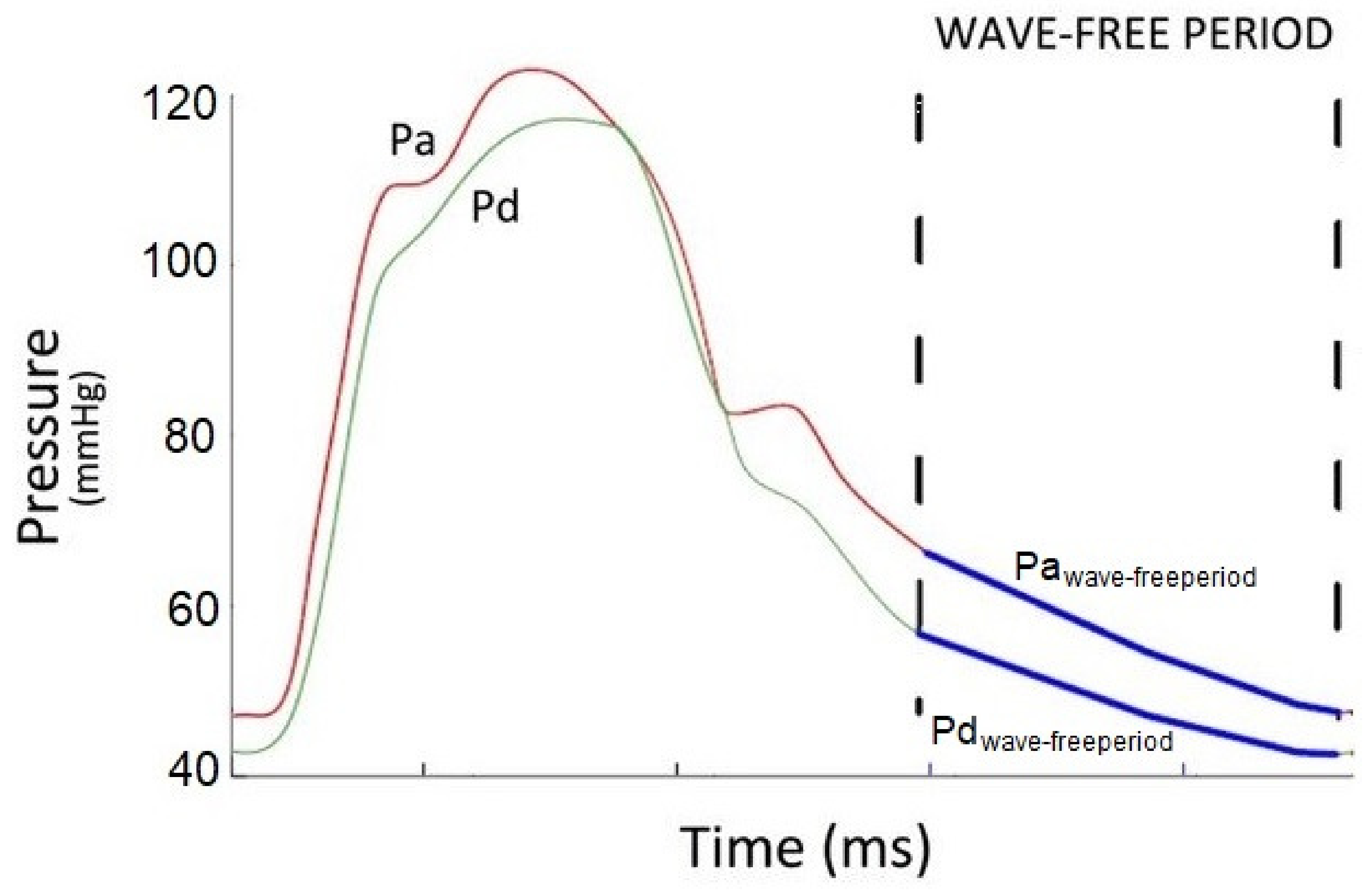
2.2. Instantaneous Wave-Free Ratio (iFR)
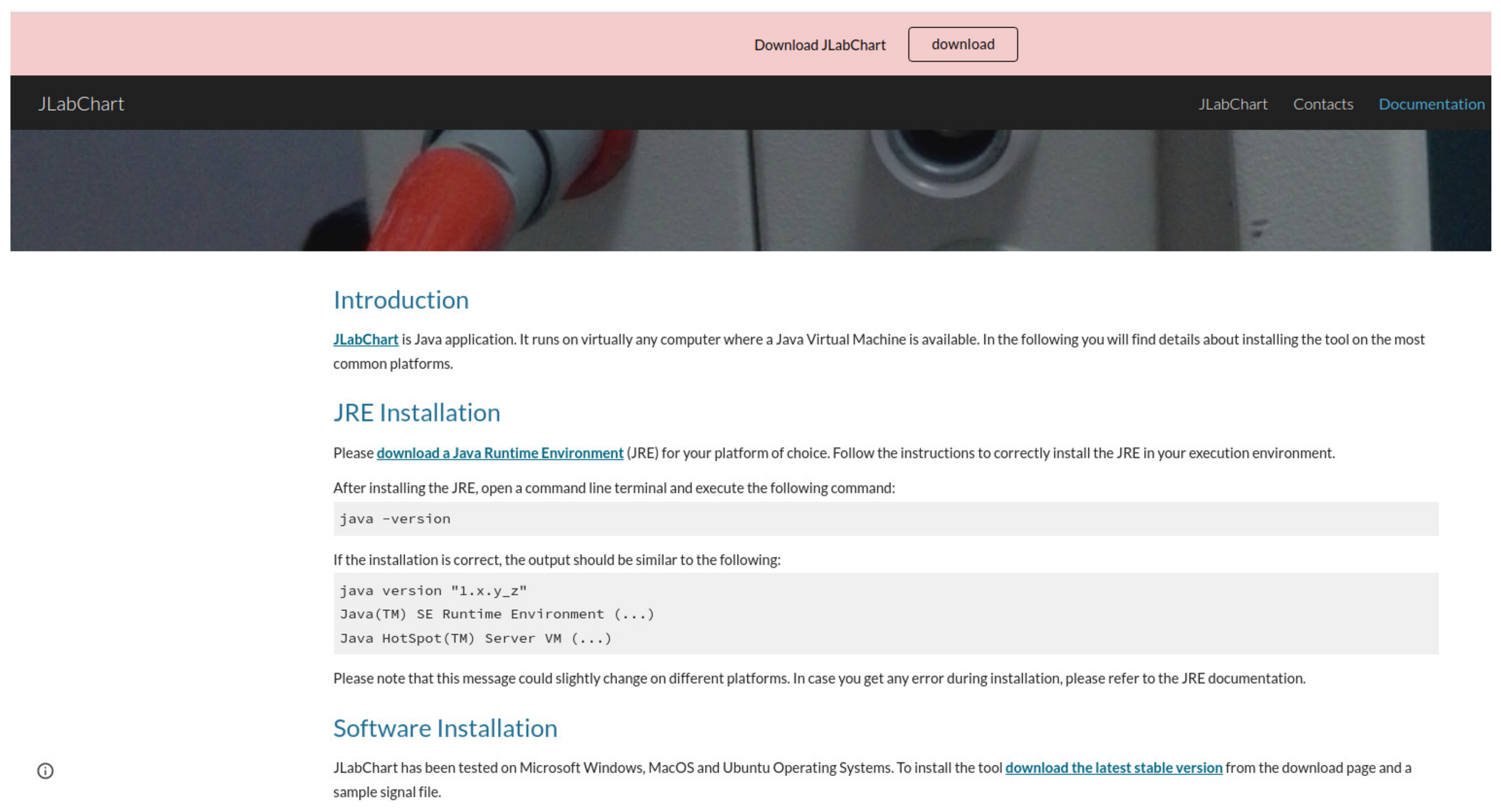
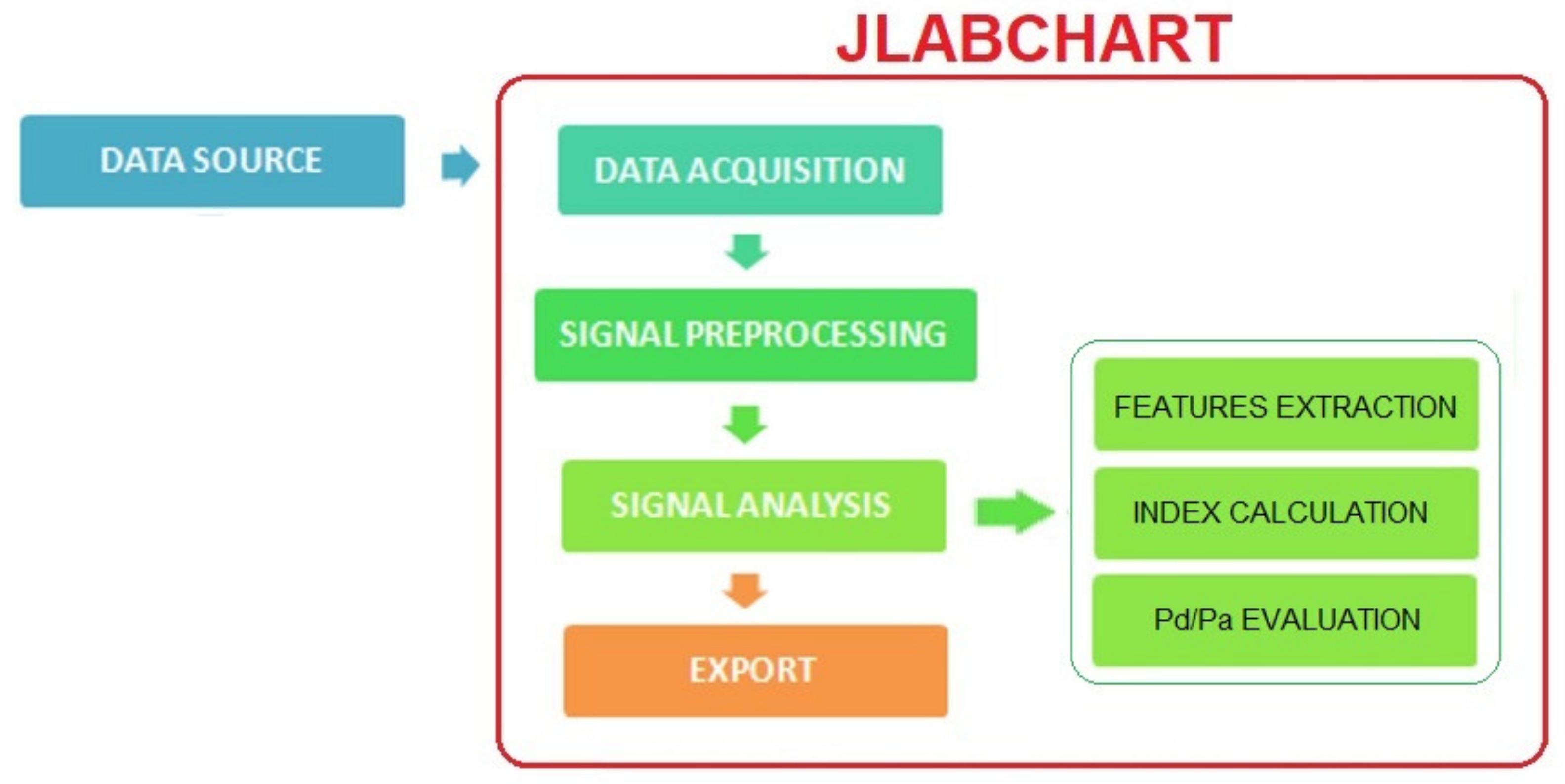
2.3. JLabChart Architecture
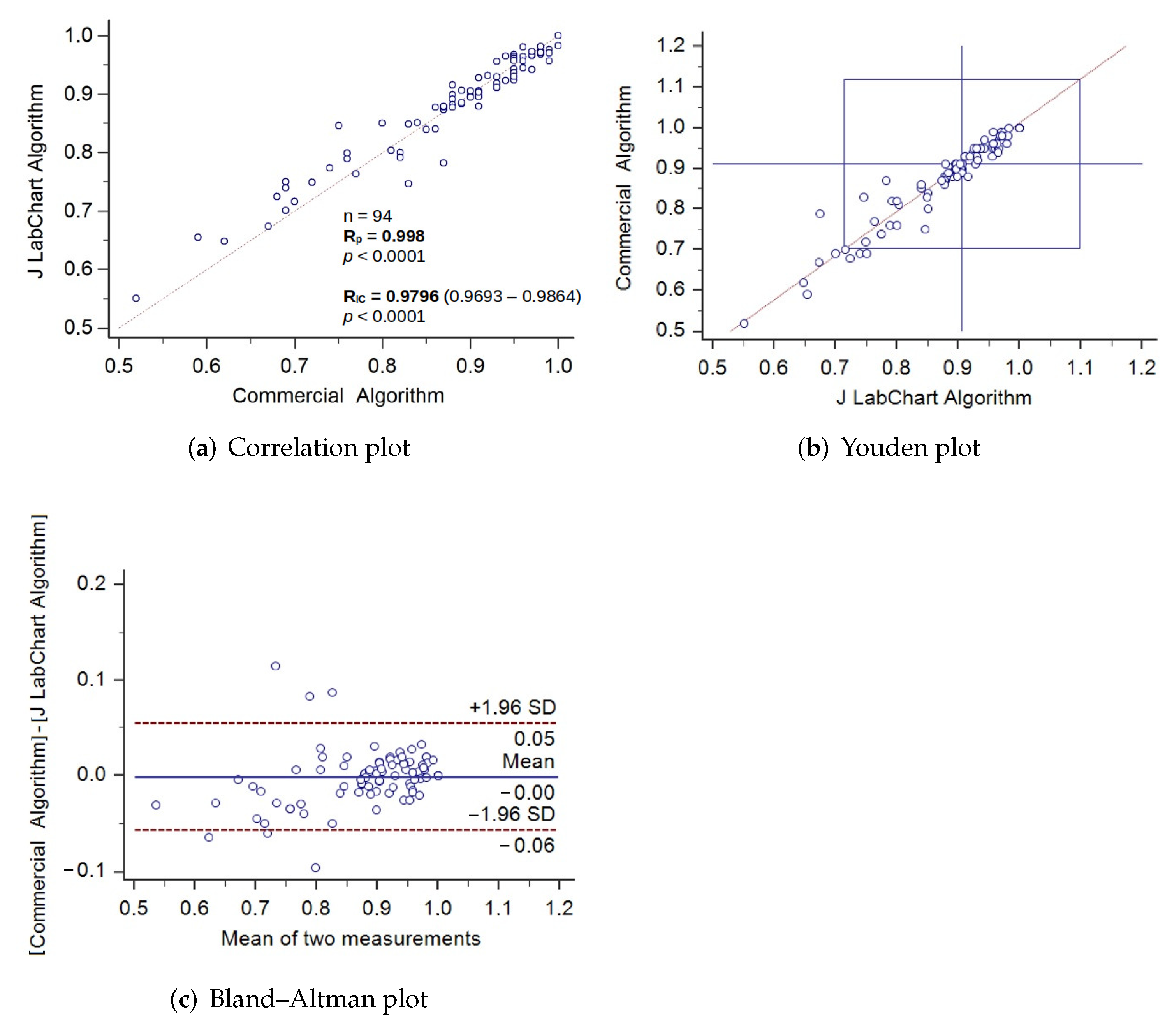
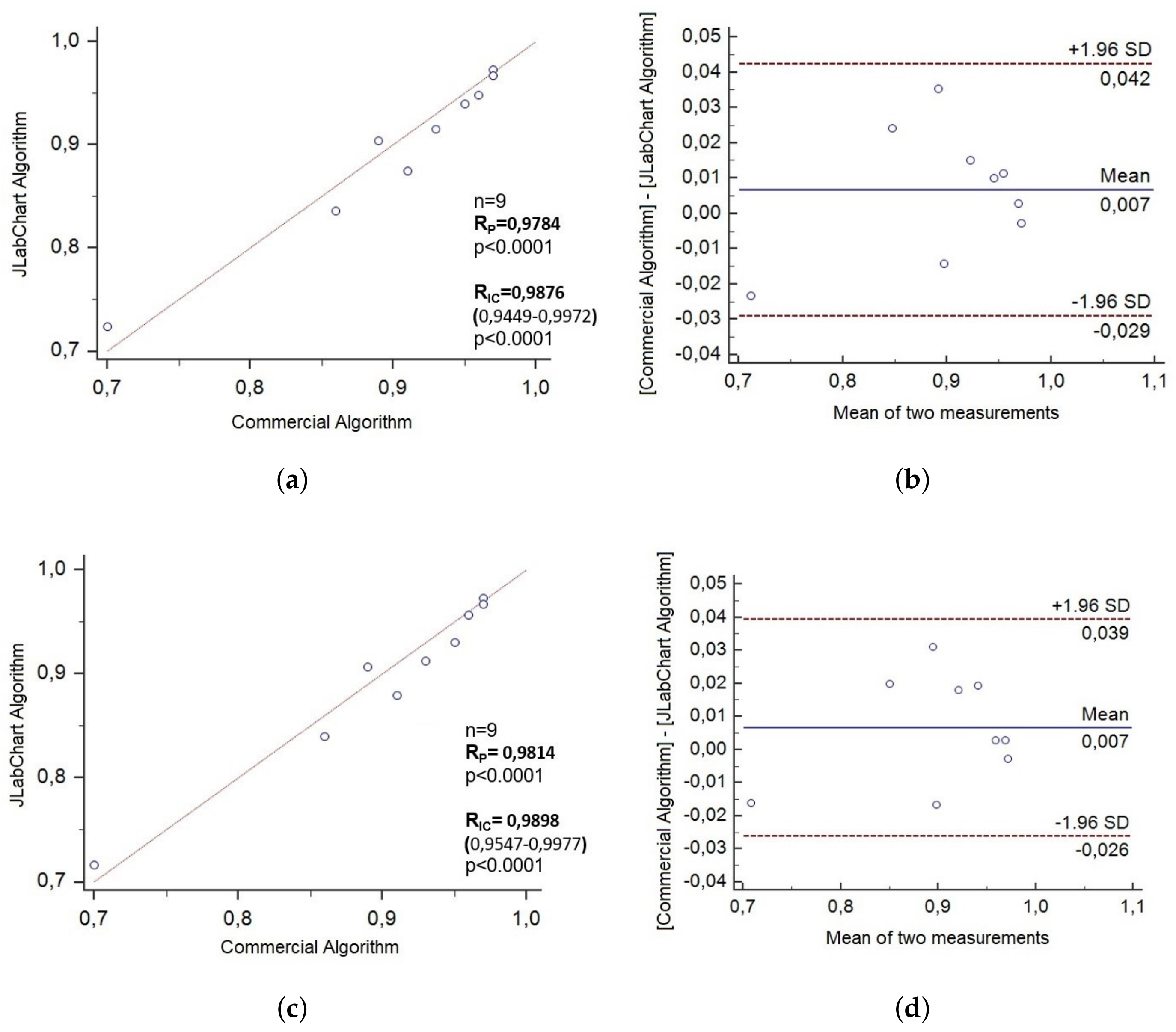
3. Results and Discussion
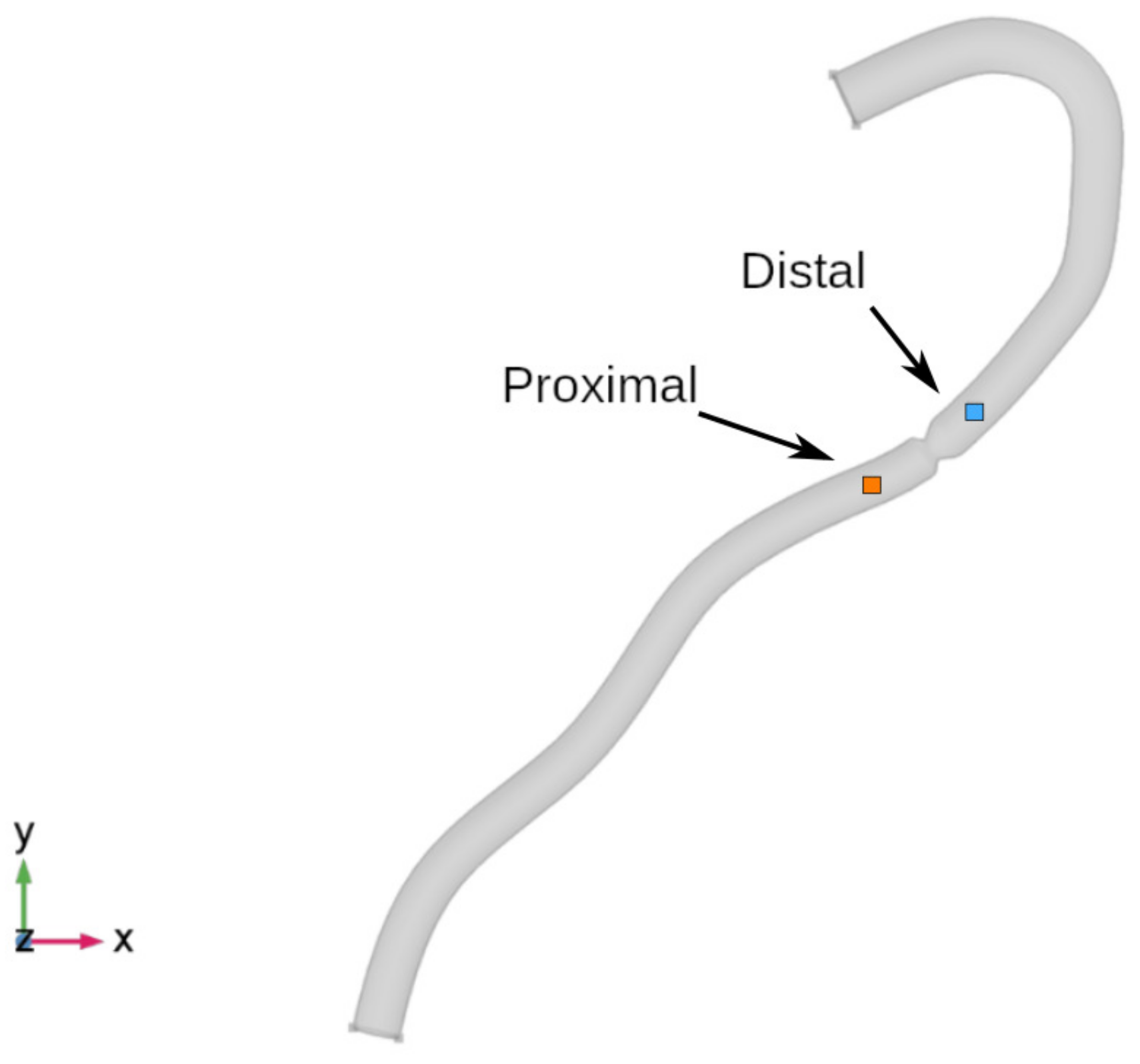
- 595 recognized cycles in the distal pressure signal;
- 600 recognized cycles in the proximal pressure signal.
4. Study Limitations
5. Conclusions
- FFR and iFR are established indexes used to assess severity of coronary stenoses by measuring intra-coronary pressure.
- Despite their widespread use, not all commercial vendors proved calculates both indexes, hence there is still an unmet need for a tool to calculate all pressure-based indexes accurately.
- JLabChart also meets the need to calculate both hyperemic (FFR) and non-hyperemic (iFR) coronary pressure-based indexes from retrospective pressure tracings.
- Measurements performed with JLabChart were first tested by using synthetic images created in a multiphysics modeling environment.
- Measurements performed with JLabChart were then successfully validated on a retrospective clinical dataset.
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. Atlas Writing Group European Society of Cardiology: Cardiovascular Disease Statistics 2019 (Executive Summary). Eur. Heart J. Qual. Care Clin. Outcomes 2020, 6, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Al-Lamee, R.K.; Nowbar, A.N.; Francis, D.P. Percutaneous coronary intervention for stable coronary artery disease. Heart 2019, 105, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Iaizzo, P.A. Handbook of Cardiac Anatomy, Physiology, and Devices; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Safi, M.; Khaheshi, I.; Eslami, V.; Beheshtian, M.M.; Naderian, M. Impact of Lesion Length on Functional Significance in Intermediate Coronary Lesions. Int. J. Cardiovasc. Pract. 2017, 2, 57–60. [Google Scholar] [CrossRef] [Green Version]
- Marcus, M.L.; Skorton, D.J.; Johnson, M.R.; Collins, S.M.; Harrison, D.G.; Kerber, R.E. Visual estimation of precent diameter coronary stenosis: “A battered gold standard”. J. Am. Coll. Cardiol. 1988, 11, 1143. [Google Scholar] [CrossRef] [Green Version]
- Pijls, N.H.; Van Gelder, B.; Van der Voort, P.; Peels, K.; Bracke, F.A.; Bonnier, H.J.; El Gamal, M.I. Fractional flow reserve. A useful index to evaluate the influence of an epicardial coronary stenosis on myocardial blood flow. Circulation 1995, 92, 3183–3193. [Google Scholar] [CrossRef] [PubMed]
- Pijls, N.H.; De Bruyne, B.; Peels, K.; Van Der Voort, P.H.; Bonnier, H.J.; Bartunek, J.; Koolen, J.J.; Koolen, J.J. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N. Engl. J. Med. 1996, 334, 1703–1708. [Google Scholar] [CrossRef]
- De Bruyne, B.; Pijls, N.H.; Kalesan, B.; Barbato, E.; Tonino, P.A.L.; Piroth, Z.; Jagic, N.; Möbius-Winkler, S.; Rioufol, G.; Witt, N.; et al. Fractional Flow Reserve-Guided PCI Versus Medical Therapy in Stable Coronary Disease. N. Engl. J. Med. 2012, 36, 991–1001. [Google Scholar] [CrossRef] [Green Version]
- Scalise, M.; Torella, M.; Marino, F.; Ravo, M.; Giurato, G.; Vicinanza, C.; Cianflone, E.; Mancuso, T.; Aquila, I.; Salerno, L.; et al. Atrial myxomas arise from multipotent cardiac stem cells. Eur. Heart J. 2020, 41, 4332–4345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salatino, A.; Aversa, I.; Battaglia, A.M.; Sacco, A.; Di Vito, A.; Santamaria, G.; Chirillo, R.; Veltri, P.; Tradigo, G.; Di Cello, A.; et al. H-Ferritin Affects Cisplatin-Induced Cytotoxicity in Ovarian Cancer Cells through the Modulation of ROS. Oxidative Med. Cell. Longev. 2019, 2019, 3461251. [Google Scholar] [CrossRef]
- Stouffer, G.A. Cardiovascular Hemodynamics for the Clinician; John Wiley and Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Murtagh, B.; Higano, S.; Lennon, R.; Mathew, V.; Holmes, D.R., Jr.; Lerman, A. Role of incremental doses of intracoronary adenosine for fractional flow reserve assessment. Am. Heart J. 2003, 146, 99–105. [Google Scholar] [CrossRef]
- Samady, H.; Gogas, B.D. Does Flow During Rest and Relaxation Suffice? J. Am. Coll. Cardiol. 2013, 61, 1436–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumann, S.; Bojara, W.; Post, H.; Rudolph, T.; Schäufele, T.; Ong, P.; Lehmann, R.; Von Zur Mühlen, C.; Universitäts-Herzzentrum Freiburg-Bad Krozingen; Medizinische Fakultät Albert-Ludwigs-Universität Freiburg; et al. Coronary physiology in the catheter laboratory. Herz 2020, 46, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, H.; Kawase, Y. FFR and iFR guided percutaneous coronary intervention. Cardiovasc. Interv. Ther. 2016, 31, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Escaned, J.; Malik, I.S.; Mikhail, G.W.; Foale, R.A.; Mila, R.; Tarkin, J.; Petraco, R.; Broyd, C.; Jabbour, R.; et al. Development and Validation of a New Adenosine-Independent Index of Stenosis Severity From Coronary Wave—Intensity Analysis. J. Am. Coll. Cardiol. 2012, 59, 1392–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijjer, S.; Davies, J. Application of iFR in Clinical Scenarios. In Physiological Assessment of Coronary Stenoses and the Microcirculation; Springer: London, UK, 2017; pp. 233–248. [Google Scholar]
- De Rosa, S.; Polimeni, A.; Petraco, R.; Davies, J.E.; Indolfi, C. Diagnostic Performance of the Instantaneous Wave-Free Ratio: Comparison With Fractional Flow Reserve. Circ Cardiovasc. Interv. 2018, 11, e004613. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, Y.; Cook, C.M.; Sharp, A.S.P.; Salinas, P.; Kawase, Y.; Shiono, Y.; Giavarini, A.; Nakayama, M.; De Rosa, S.; Sen, S.; et al. Pre-Angioplasty Instantaneous Wave-Free Ratio Pullback Predicts Hemodynamic Outcome In Humans With Coronary Artery Disease: Primary Results of the International Multicenter iFR GRADIENT Registry. JACC Cardiovasc. Interv. 2018, 11, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Petraco, R.; van de Hoef, T.P.; Nijjer, S.; Sen, S.; van Lavieren, M.A.; Foale, R.A.; Meuwissen, M.; Broyd, C.; Echavarria-Pinto, M.; Foin, N.; et al. Baseline instantaneous wave-free ratio as a pressure-only estimation of underlying coronary flow reserve results of the JUSTIFY-CFR Study (Joined Coronary Pressure and Flow Analysis to Determine Diagnostic Characteristics of Basal and Hyperemic Indices of Functional Lesion Severity-Coronary Flow Reserve). Circ. Cardiovasc. Interv. 2014, 7, 492–502. [Google Scholar] [PubMed] [Green Version]
- Jeremias, A.; Maehara, A.; Généreux, P.; Asrress, K.N.; Berry, C.; Bruyne, B.; Davies, J.E.; Escaned, J.; Fearon, W.F.; Gould, K.L.; et al. Multicenter core laboratory comparison of the instantaneous wave-free ratio and resting Pd/Pa with fractional flow reserve: The RESOLVE study. J. Am. Coll. Cardiol. 2014, 63, 1253–1261. [Google Scholar] [CrossRef] [Green Version]
- Indolfi, C.; Mongiardo, A.; Spaccarotella, C.; Torella, D.; Caiazzo, G.; Polimeni, A.; Sorrentino, S.; Micieli, M.; Sabatino, J.; Curcio, A.; et al. The instantaneous wave-free ratio (iFR) for evaluation of non-culprit lesions in patients with acute coronary syndrome and multivessel disease. Int. J. Cardiol. 2015, 178, 46–54. [Google Scholar] [CrossRef]
- Darenskiy, D.; Gramovich, V.; Mitroshkin, M.; Sergienko, V.; Zharova, E.; Matchin, Y. Instantaneous wave-free ratio is not inferior to fractional flow reserve for assessment of intermediate coronary artery stenoses. J. Am. Coll. Cardiol. 2016, 67, 397. [Google Scholar] [CrossRef]
- Petraco, R.; Javier, E.; Justin, D. Validation of iFR: Clinical registries. In Physiological Assessment of Coronary Stenoses and the Microcirculation; Springer: London, UK, 2017; pp. 225–231. [Google Scholar]
- Man, W.; Hu, J.; Zhao, Z.; Zhang, M.; Wang, T.; Lin, J.; Duan, Y.; Wang, L.; Wang, H.; Sun, D.; et al. Diagnostic performance of instantaneous wave-free ratio for the evaluation of coronary stenosis severity confirmed by fractional flow reserve: A PRISMA-compliant meta-analysis of randomized studies. Medicine 2016, 95, e4774. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E.; Sen, S.; Dehbi, H.M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotberg, M.; Christiansen, E.H.; Gudmundsdottir, I.J.; Sandhall, L.; Danielewicz, M.; Jakobsen, L.; Olsson, S.E.; Öhagen, P.; Olsson, H.; Omerovic, E.; et al. iFR-SWEDEHEART Investigators. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. N. Engl. J. Med. 2017, 376, 1813–1823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoole, S.P.; Seddon, M.D.; Poulter, R.S.; Starovoytov, A.; Wood, D.A.; Jacqueline, S. Development and validation of the fractional flow reserve (FFR) angiographic scoring tool (FAST) to improve the angiographic grading and selection of intermediate lesions that require FFR assessment. Coron. Artery Dis. 2012, 23, 45–50. [Google Scholar] [CrossRef]
- Nijjer, S.S.; Sen, S.; Petraco, R.; Sachdeva, R.; Cuculi, F.; Escaned, J.; Broyd, C.; Foin, N.; Hadjiloizou, N.; Foale, R.A.; et al. Improvement in coronary haemodynamics after percutaneous coronary intervention: Assessment using instantaneous wave-free ratio. Heart 2013, 99, 1740–1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, C.M.; Ahmad, Y.; Shun-Shin, M.J.; Nijjer, S.; Petraco, R.; Al-Lamee, R.; Mayet, J.; Francis, D.P.; Sen, S.; Davies, J.E. Quantification of the Effect of Pressure Wire Drift on the Diagnostic Performance of Fractional Flow Reserve, Instantaneous Wave-Free Ratio, and Whole-Cycle Pd/Pa. Circ. Cardiovasc. Interv. 2016, 9, e002988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Va not Veer, M.; Pijls, N.H.J.; Hennigan, B.; Watkins, S.; Ali, Z.A.; De Bruyne, B.; Zimmermann, F.M.; van Nunen, L.X.; Barbato, E.; Berry, C.; et al. Comparison of Different Diastolic Resting Indexes to iFR: Are They All Equal? J. Am. Coll. Cardiol. 2017, 70, 3088–3096. [Google Scholar] [CrossRef] [PubMed]
- Morioka, Y.; Arashi, H.; Otsuki, H.; Yamaguchi, J.; Hagiwara, N. Relationship between instantaneous wave-free ratio and fractional flow reserve in patients receiving hemodialysis. Cardiovasc. Interv. Ther. 2018, 33, 256–263. [Google Scholar] [CrossRef]
- Rivero, F.; Cuesta, J.; Bastante, T.; Benedicto, A.; Fernández-Pérez, C.; Antuña, P.; García-Guimaraes, M.; Alfonso, F. Reliability of physiological assessment of coronary stenosis severity using intracoronary pressure techniques: A comprehensive analysis from a large cohort of consecutive intermediate coronary lesions. EuroIntervention 2017, 13, 193–200. [Google Scholar] [CrossRef]
- Harle, T.; Meyer, S.; Vahldiek, F.; Elsasser, A. Differences between automatically detected and steady-state fractional flow reserve. Clin. Res. Cardiol. 2016, 105, 127–134. [Google Scholar] [CrossRef]
- Tradigo, G.; Vizza, P.; Fragomeni, G.; Veltri, P. On the reliability of measurements for a stent positioning simulation system. Int. J. Med. Inform. 2019, 123, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Moser, D.K.; Riegel, B. Cardiac Nursing: A Companion to Braunwald’s Heart Disease; Elsevier Health Sciences: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Miller, G. Fundamentals of Biomedical Transport Processes; Morgan and Claypool Publishers: Williston, VT, USA, 2010. [Google Scholar]
- Caroprese, L.; Veltri, P.; Vocaturo, E.; Zumpano, E. Deep learning techniques for electronic health record analysis (2019). In Proceedings of the 2018 9th International Conference on Information, Intelligence, Systems and Applications, IISA, Zakynthos, Greece, 23–25 July 2018. [Google Scholar]
- Escaned, J.; Echavarría-Pinto, M.; Garcia-Garcia, H.M.; Van de Hoef, T.P.; De Vries, T.; Kaul, P.; Raveendran, G.; Altman, J.D.; Kurz, H.I.; Brechtken, J.; et al. Prospective Assessment of the Diagnostic Accuray of Instantaneous Wave-Free Ratio to Assess Coronary Stenosis Relevance: Results of ADVISE II International, Multicenter Study (ADenosine Vasodilator Independent Stenosis Evaluation II. JACC Cardiovasc. Interv. 2015, 8, 824–833. [Google Scholar] [CrossRef] [Green Version]
- Adiputra, Y.; Chen, S.L. Clinical Relevance of Coronary Fractional Flow Reserve: Art-of-state. Chin. Med. J. 2015, 128, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Asrress, K.N.; Nijjer, S.; Petraco, R.; Malik, I.; Foale, R.A.; Mikhail, G.W.; Foin, N.; Broyd, C.; Hadjiloizou, N.; et al. Diagnostic Classification of the Instantaneous Wave-Free Ratio is Equivalent to Fractional Flow Reserve and Is Not Improved with Adenosine Administration. J. Am. Coll. Cardiol. 2013, 61, 1409–1420. [Google Scholar] [CrossRef] [Green Version]
- Vizza, P.; Curcio, A.; Tradigo, G.; Indolfi, C.; Veltri, P. A framework for the atrial fibrillation prediction in electrophysiological studies. Comput. Methods Programs Biomed. 2015, 120, 65–76. [Google Scholar] [CrossRef]
- Comsol Multiphysics. Available online: https://www.comsol.it/ (accessed on 6 March 2022).
- Caruso, M.V.; De Rosa, S.; Indolfi, C.; Fragomeni, G. Computational analysis of stenosis geometry effects on right coronary hemodynamics. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2015, 2015, 981–984. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, L.T.; Caruso, M.V.; De Rosa, S.; Indolfi, C.; Fragomeni, G. Different Blood Flow Models in Coronary Artery Diseases: Effects on hemodynamic parameters. Proc. IEEE Annu. Int. Conf. Eng. Med. Biol. Soc. 2018, 1, 3185–3188. [Google Scholar] [CrossRef]
- Gaudio, L.T.; Veltri, P.; De Rosa, S.; Indolfi, C.; Fragomeni, G. Model and Application to Support the Coronary Artery Diseases (CAD): Development and Testing. Interdiscip. Sci. 2020, 12, 50–58. [Google Scholar] [CrossRef]
- Kukic, P.; Mirabello, C.; Tradigo, G.; Walsh, I.; Veltri, P.; Pollastri, G. Toward an accurate prediction of inter-residue distances in proteins using 2D recursive neural networks. BMC Bioinform. 2014, 5, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID_Patient | ||||
|---|---|---|---|---|
| 1 | 0.77 | 0.79 | 0.90 | 0.91 |
| 2 | 0.85 | 0.87 | 0.87 | 0.88 |
| 3 | 0.87 | 0.88 | 0.90 | 0.89 |
| 4 | 0.82 | 0.84 | 0.74 | 0.77 |
| 5 | 0.84 | 0.85 | 0.97 | 0.97 |
| 6 | 0.70 | 0.72 | 0.77 | 0.76 |
| 7 | 0.96 | 0.96 | 0.97 | 0.94 |
| 8 | 0.75 | 0.87 | 0.85 | 0.84 |
| 9 | 0.66 | 0.67 | 0.52 | 0.55 |
| 10 | 0.73 | 0.77 | 0.84 | 0.85 |
| 11 | 0.91 | 0.93 | 0.99 | 0.96 |
| 12 | 0.82 | 0.84 | 0.74 | 0.77 |
| 13 | 0.73 | 0.79 | 0.95 | 0.94 |
| 14 | 0.79 | 0.83 | 0.95 | 0.94 |
| 15 | 0.80 | 0.95 | 0.95 | 0.96 |
| 16 | 0.71 | 0.73 | 0.91 | 0.93 |
| 17 | 0.91 | 0.94 | 0.91 | 0.90 |
| 18 | 0.97 | 0.98 | 0.99 | 0.98 |
| 19 | 0.76 | 0.77 | 0.88 | 0.90 |
| 20 | 0.97 | 0.98 | 0.98 | 0.97 |
| 21 | 0.81 | 0.89 | 0.69 | 0.70 |
| 22 | 0.71 | 0.73 | 0.87 | 0.78 |
| 23 | 0.90 | 0.90 | 0.96 | 0.95 |
| 24 | 0.85 | 0.86 | 0.98 | 0.97 |
| 25 | 0.80 | 0.82 | 0.90 | 0.90 |
| 26 | 0.80 | 0.82 | 0.96 | 0.98 |
| 27 | ⋯ | ⋯ | ⋯ | ⋯ |
| ⋯ | ⋯ | ⋯ | ⋯ | ⋯ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tradigo, G.; De Rosa, S.; Vizza, P.; Fragomeni, G.; Guzzi, P.H.; Indolfi, C.; Veltri, P. Calculation of Intracoronary Pressure-Based Indexes with JLabChart. Appl. Sci. 2022, 12, 3448. https://doi.org/10.3390/app12073448
Tradigo G, De Rosa S, Vizza P, Fragomeni G, Guzzi PH, Indolfi C, Veltri P. Calculation of Intracoronary Pressure-Based Indexes with JLabChart. Applied Sciences. 2022; 12(7):3448. https://doi.org/10.3390/app12073448
Chicago/Turabian StyleTradigo, Giuseppe, Salvatore De Rosa, Patrizia Vizza, Gionata Fragomeni, Pietro Hiram Guzzi, Ciro Indolfi, and Pierangelo Veltri. 2022. "Calculation of Intracoronary Pressure-Based Indexes with JLabChart" Applied Sciences 12, no. 7: 3448. https://doi.org/10.3390/app12073448
APA StyleTradigo, G., De Rosa, S., Vizza, P., Fragomeni, G., Guzzi, P. H., Indolfi, C., & Veltri, P. (2022). Calculation of Intracoronary Pressure-Based Indexes with JLabChart. Applied Sciences, 12(7), 3448. https://doi.org/10.3390/app12073448