
A Novel Soft Robotic Exoskeleton System for Hand Rehabilitation and Assistance Purposes

 ,
,  ,
,  and
and
Abstract
:1. Introduction
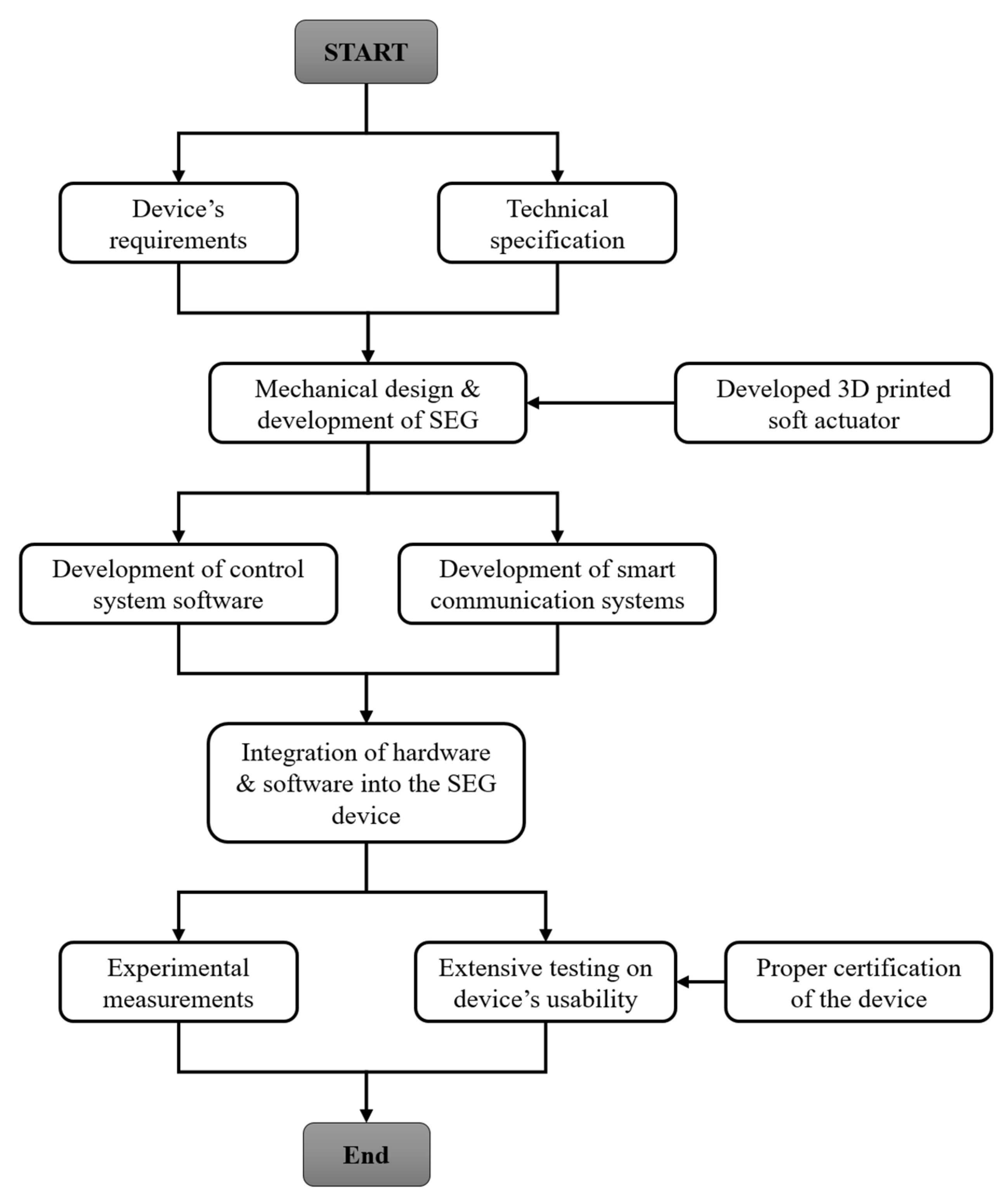
2. Development of the SEG Device
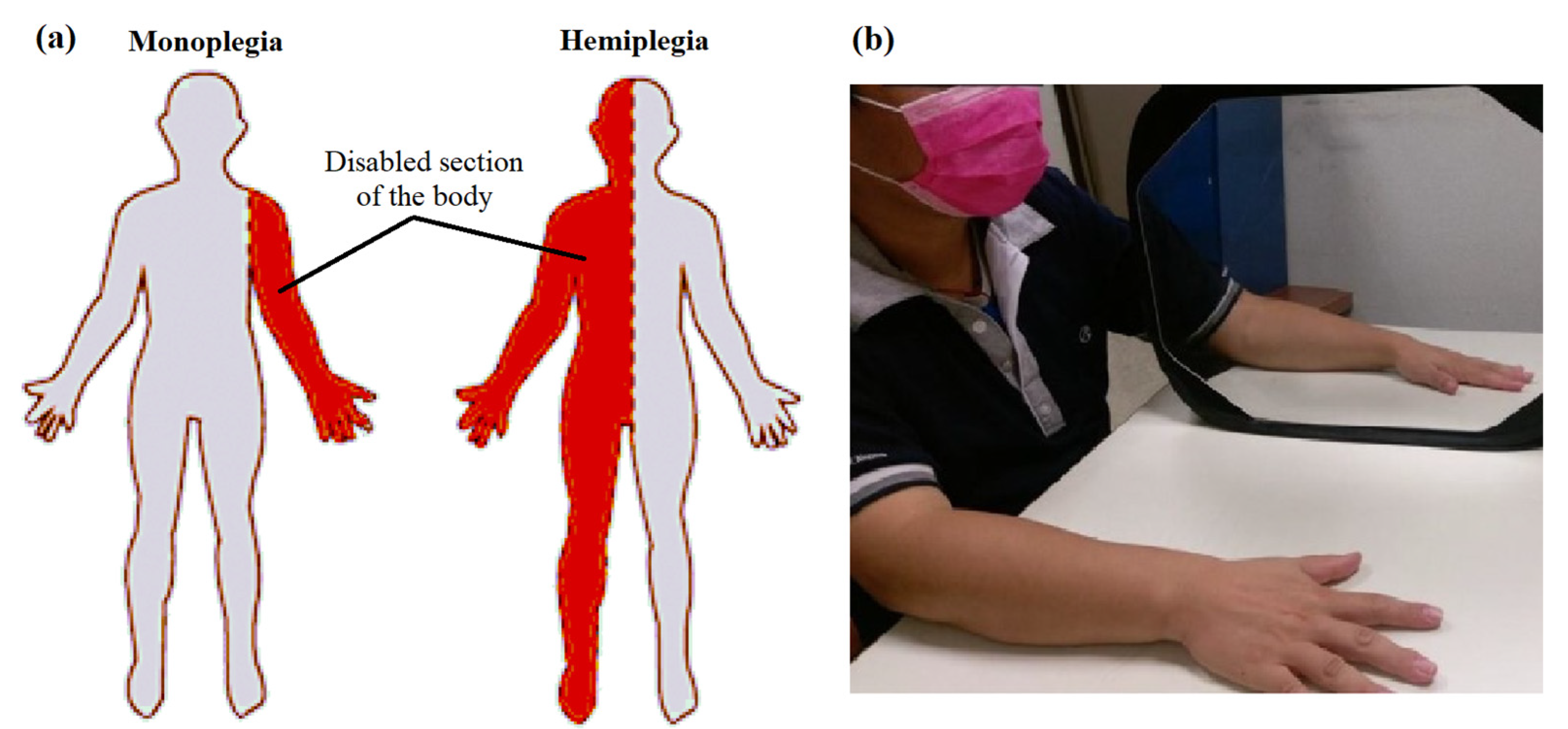
2.1. Requirments and Technical Specifications
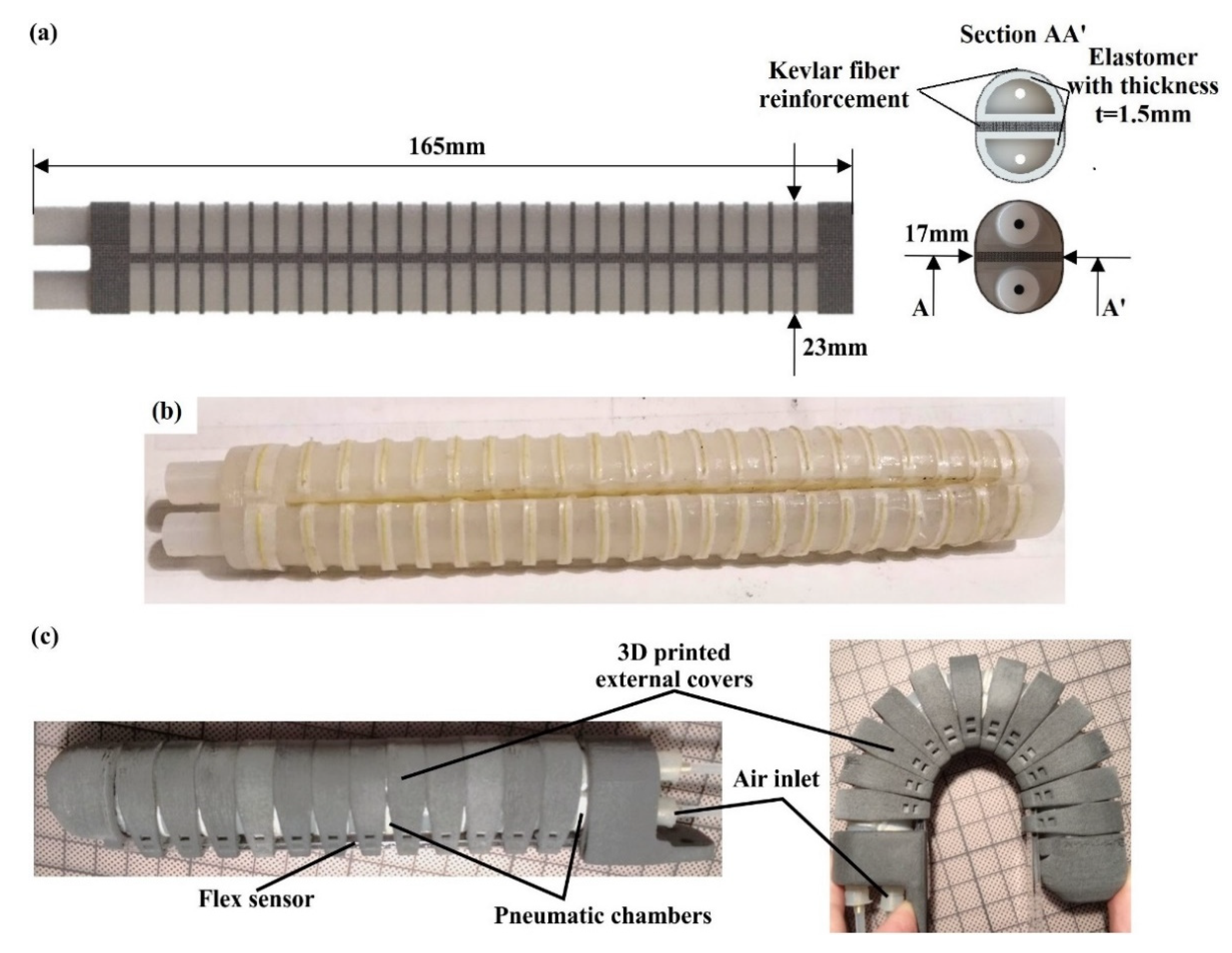
2.2. Description of the Employed Soft Actuator
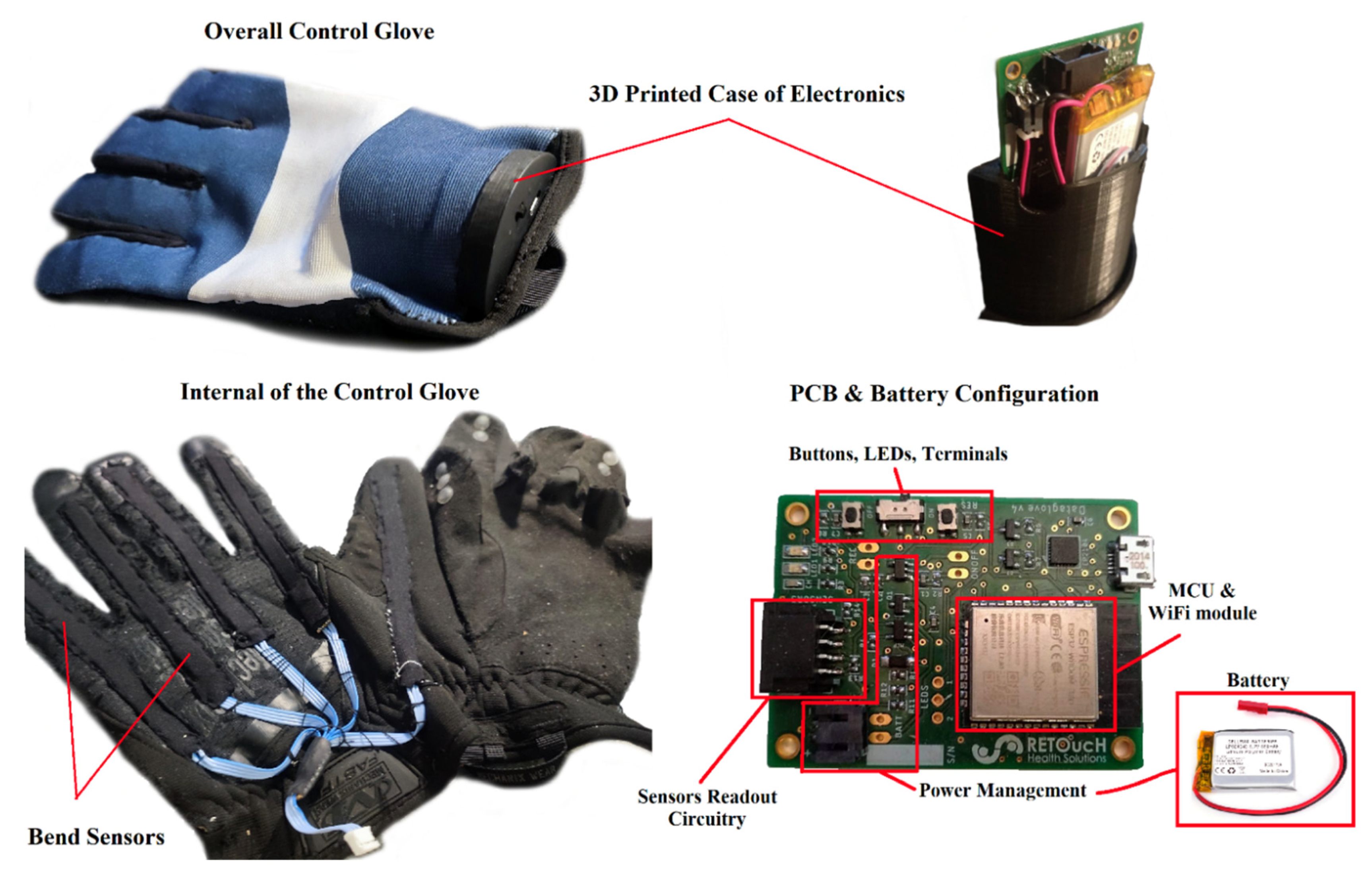
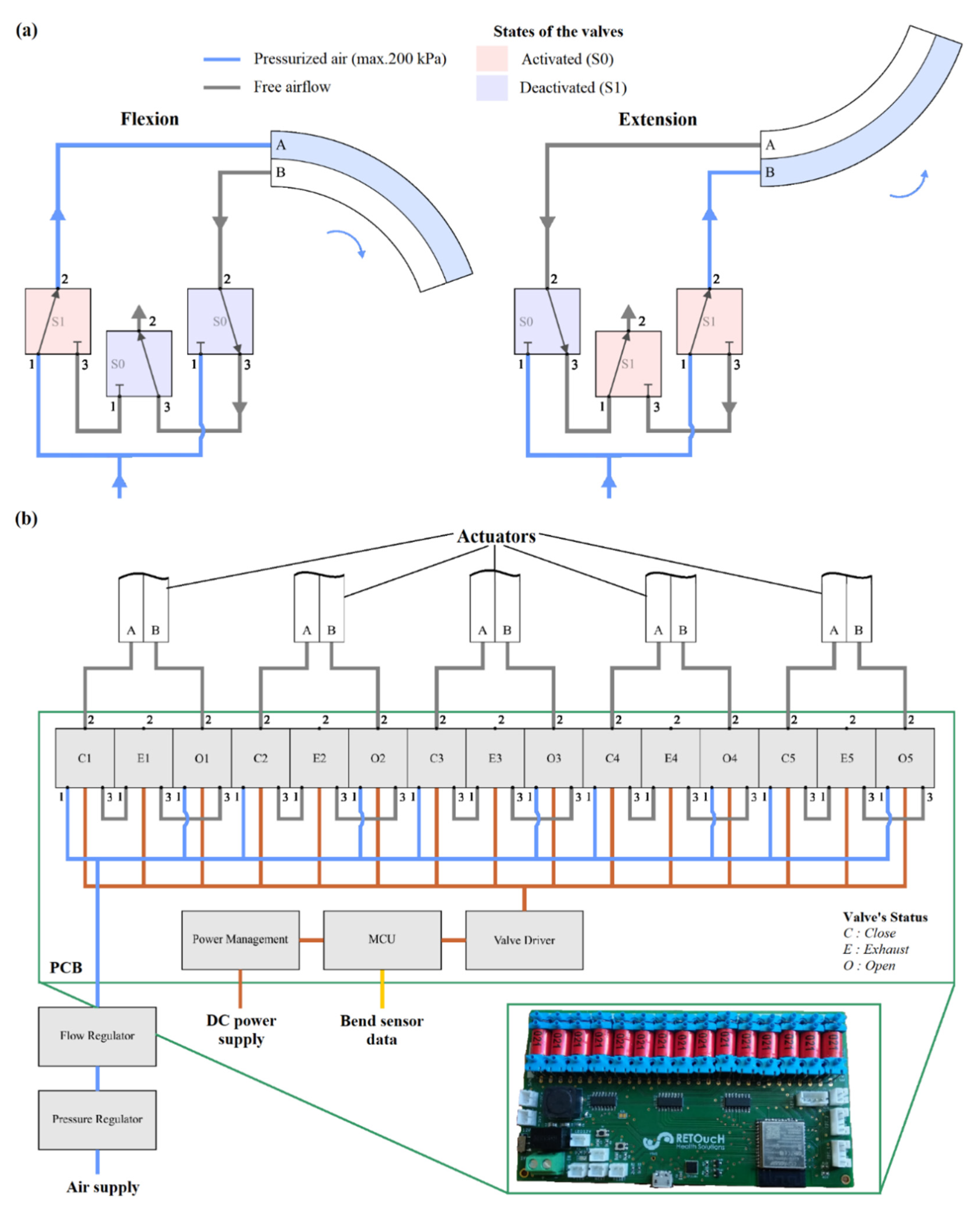
2.3. Development of the SEG Device’s Hardware
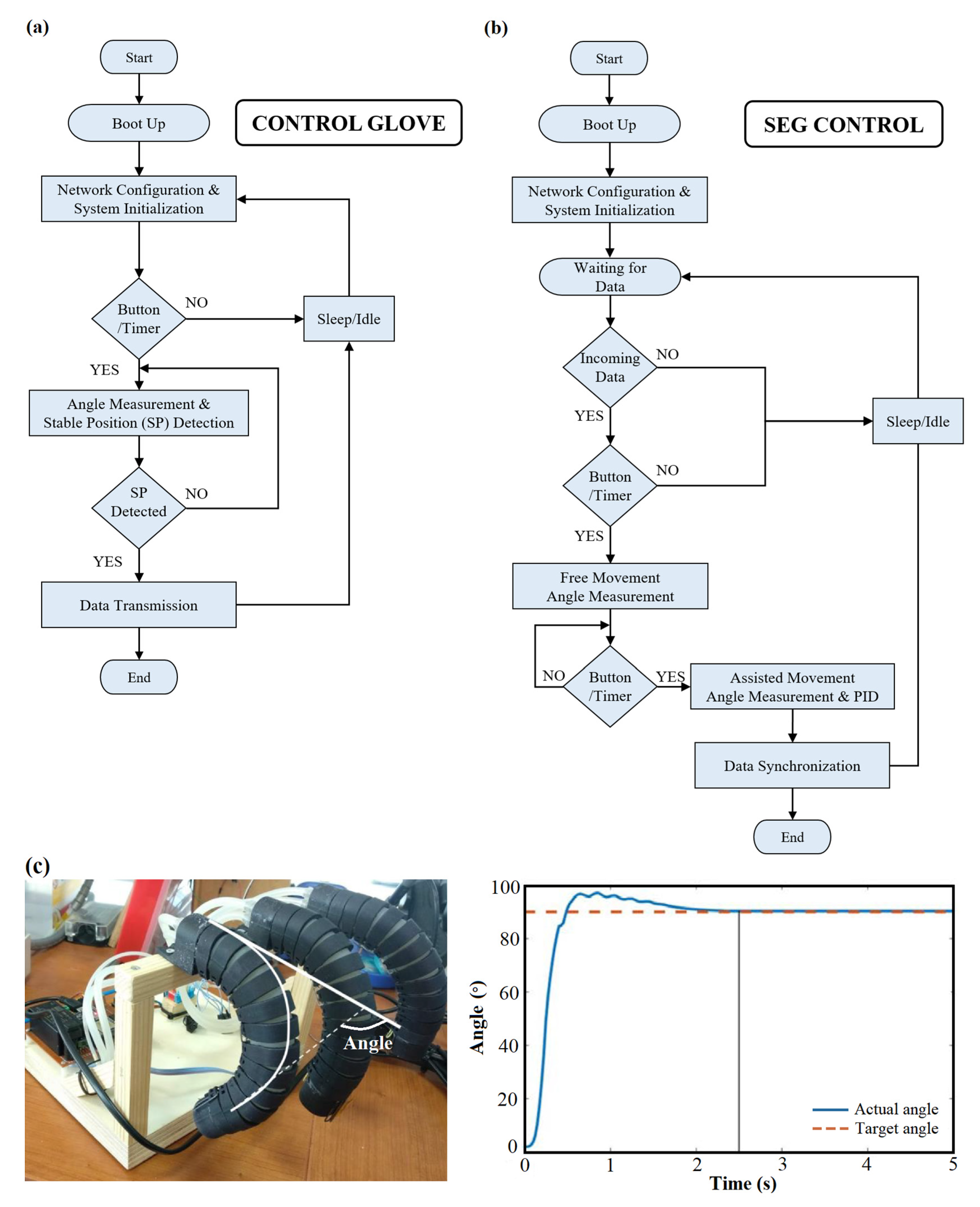
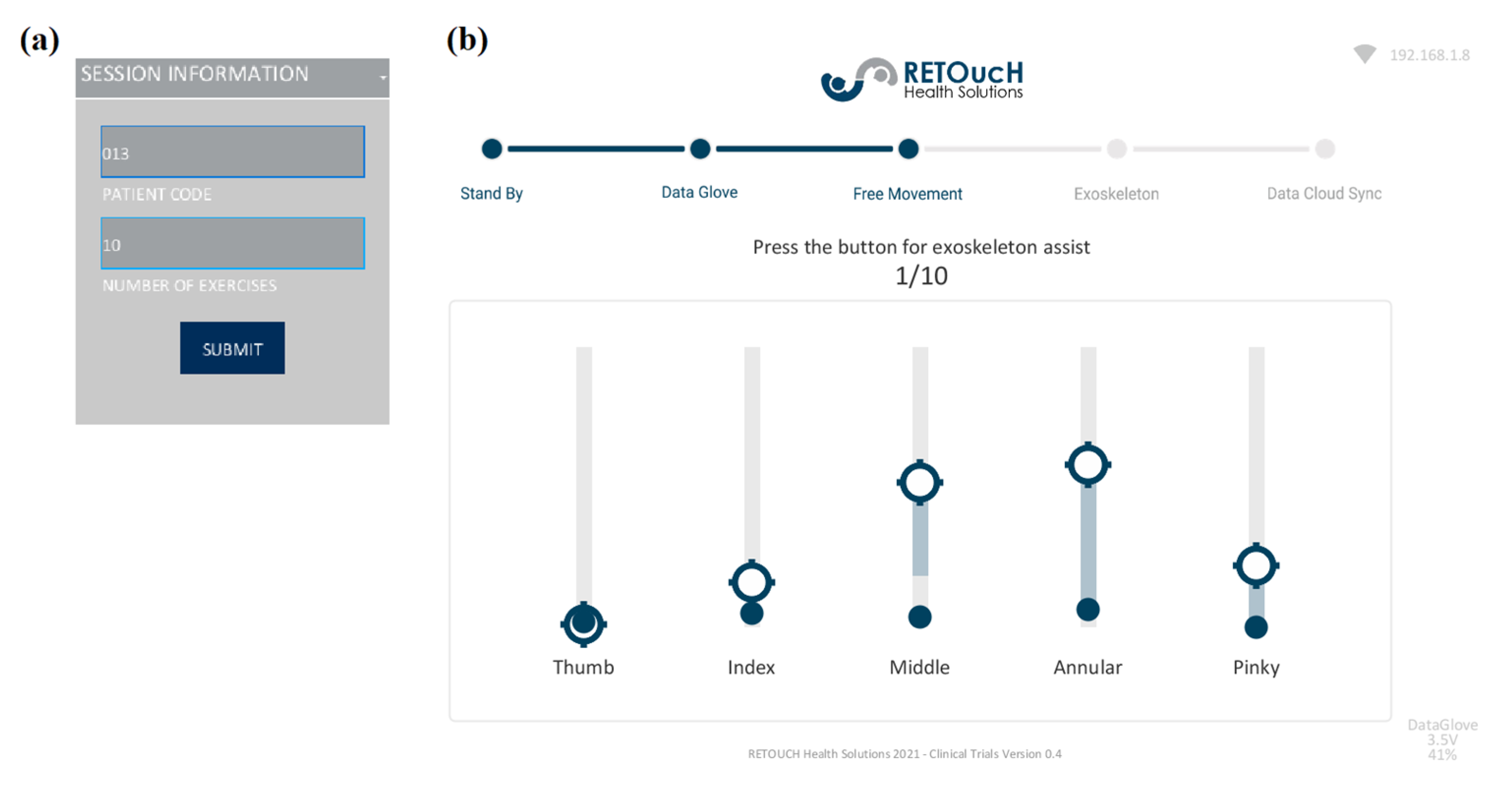
2.4. Development of the SEG Device’s Software
3. Results and Discussion
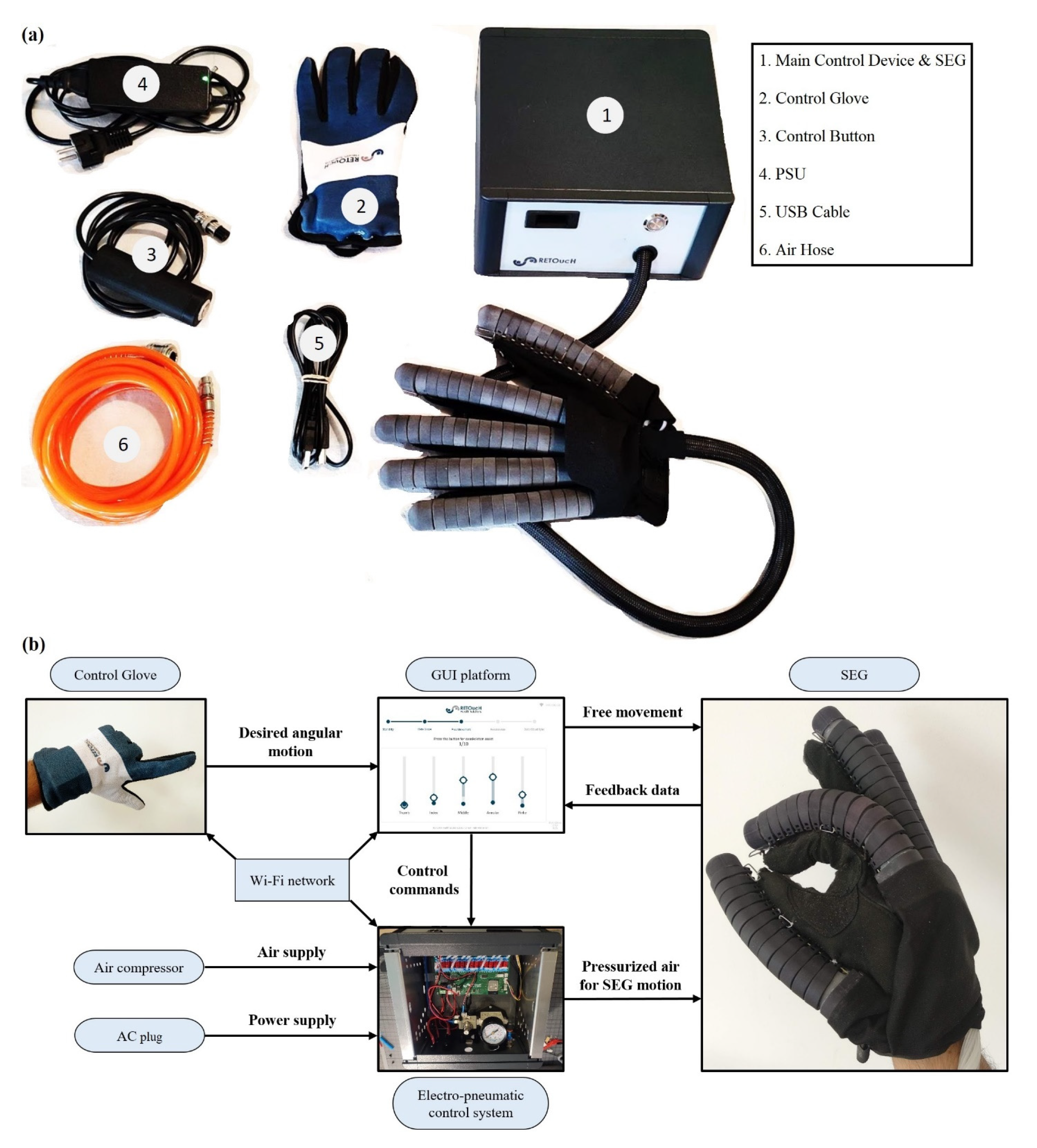
3.1. Final Design of the SEG Device
3.2. Experimental Procedure and Validation
4. Conclusions
5. Patent
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- Zacharaki, A.; Kostavelis, I.; Gasteratos, A.; Dokas, I. Safety bounds in human robot interaction: A survey. Saf. Sci. 2020, 127, 104667. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Singh, R.P.; Suman, R. Substantial capabilities of robotics in enhancing industry 4.0 implementation. Cogn. Robot. 2021, 1, 58–75. [Google Scholar] [CrossRef]
- Tantawi, K.H.; Sokolov, A.; Tantawi, O. Advances in Industrial Robotics: From Industry 3.0 Automation to Industry 4.0 Collaboration. In Proceedings of the 4th Technology Innovation Management and Engineering Science International Conference (TIMES-iCON), Bangkok, Thailand, 11–13 December 2019; pp. 1–4. [Google Scholar] [CrossRef]
- Gibson, I.; Rosen, D.W.; Stucker, B. Additive Manufacturing Technologies; Springer: New York, NY, USA, 2010. [Google Scholar] [CrossRef]
- Rosen, D.W. Research supporting principles for design for additive manufacturing. J. Virtual Phys. Prototyp. 2014, 9, 225–232. [Google Scholar] [CrossRef]
- Polygerinos, P.; Wang, Z.; Galloway, K.C.; Wood, R.J.; Walsh, C.J. Soft robotic glove for combined assistance and at-home rehabilitation. Robot. Auton. Syst. 2015, 73, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Papadimitriou, P.; Andriotis, E.G.; Fatouros, D.; Tzetzis, D. Design and Prototype Fabrication of a Cost-Effective Microneedle Drug Delivery Apparatus Using Fused Filament Fabrication, Liquid Crystal Display and Semi-Solid Extrusion 3D Printing Technologies. Micromachines 2022, 13, 1319. [Google Scholar] [CrossRef]
- Kazanskiy, N.L.; Butt, M.A.; Khonina, S.N. Recent Advances in Wearable Optical Sensor Automation Powered by Battery versus Skin-like Battery-Free Devices for Personal Healthcare—A Review. Nanomaterials 2022, 12, 334. [Google Scholar] [CrossRef]
- Kladovasilakis, N.; Tsongas, K.; Tzetzis, D. Finite Element Analysis of Orthopedic Hip Implant with Functionally Graded Bioinspired Lattice Structures. Biomimetics 2020, 5, 44. [Google Scholar] [CrossRef]
- González-Henríquez, C.M.; Sarabia-Vallejos, M.A.; Rodriguez-Hernandez, J. Polymers for additive manufacturing and 4D-printing: Materials, methodologies, and biomedical applications. J. Polym. Sci. 2019, 94, 57–116. [Google Scholar] [CrossRef]
- Li, G.; Cheng, L.; Sun, N. Design, manipulability analysis and optimization of an index finger exoskeleton for stroke rehabilitation. Mech. Mach. Theory 2022, 167, 104526. [Google Scholar] [CrossRef]
- Sun, N.; Li, G.; Cheng, L. Design and Validation of a Self-Aligning Index Finger Exoskeleton for Post-Stroke Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1513–1523. [Google Scholar] [CrossRef]
- Li, G.; Cheng, L.; Gao, Z.; Xia, X.; Jiang, J. Development of an Untethered Adaptive Thumb Exoskeleton for Delicate Rehabilitation Assistance. IEEE Trans. Robot. 2022, 38, 3514–3529. [Google Scholar] [CrossRef]
- Lin, L.; Zhang, F.; Yang, L.; Fu, Y. Design and modeling of a hybrid soft-rigid hand exoskeleton for poststroke rehabilitation. Int. J. Mech. Sci. 2021, 212, 106831. [Google Scholar] [CrossRef]
- Dávila-Vilchis, J.M.; Ávila-Vilchis, J.C.; Vilchis-González, A.H. Design Criteria of Soft Exogloves for Hand Rehabilitation-Assistance Tasks. Appl. Bionics Biomech. 2020, 2724783, 19. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Nichols-Larsen, D. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: The EXCITE randomized clinical trial. JAMA 2006, 296, 2095–2104. [Google Scholar] [CrossRef] [PubMed]
- Gerez, L.; Gao, G.; Dwivedi, A.; Liarokapis, M. A Hybrid, Wearable Exoskeleton Glove Equipped with Variable Stiffness Joints, Abduction Capabilities, and a Telescopic Thumb. IEEE Access 2020, 8, 173345–173358. [Google Scholar] [CrossRef]
- Chu, C.Y.; Patterson, R.M. Soft robotic devices for hand rehabilitation and assistance: A narrative review. J. NeuroEng. Rehabil. 2018, 15, 9. [Google Scholar] [CrossRef] [Green Version]
- Abbas, K.; Balc, N.; Bremen, S.; Skupin, M. Crystallization and Aging Behavior of Polyetheretherketone PEEK within Rapid Tooling and Rubber Molding. J. Manuf. Mater. Process. 2022, 6, 93. [Google Scholar] [CrossRef]
- Kladovasilakis, N.; Kontodina, T.; Charalampous, P.; Kostavelis, I.; Tzetzis, D.; Tzovaras, D. A case study on 3D scanning, digital reparation and rapid metal additive manufacturing of a centrifugal impeller. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1037, 012018. [Google Scholar] [CrossRef]
- Davis, J. Improving upper-extremity function in adult hemiplegia. OT Pract. 2001, 6, 8–13. [Google Scholar]
- Rothgangel, A.S.; Braun, S.M. Mirror Therapy: Practical Protocol for Stroke Rehabilitation; Pflaum Verlag: Munich, Germany, 2013. [Google Scholar] [CrossRef]
- Ezendam, D.; Bongers, R.M.; Jannink, M.J.A. Systematic review of the effectiveness of mirror therapy in upper extremity function. Disabil. Rehabil. 2009, 31, 2135–2149. [Google Scholar] [CrossRef]
- Pu, S.; Cheng, L.; Chang, J. A Robot-Assisted Hand Exoskeletal System for Mirror Therapy Rehabilitation. In Proceedings of the ASME 2017 Conference on Information Storage and Processing Systems, San Francisco, CA, USA, 29–30 August 2017; p. V001T07A003. [Google Scholar] [CrossRef]
- Díez, J.A.; Blanco, A.; Catalán, J.M.; Badesa, F.J.; Lledó, L.D.; García-Aracil, N. Hand exoskeleton for rehabilitation therapies with integrated optical force sensor. Adv. Mech. Eng. 2018, 10, 1687814017753881. [Google Scholar] [CrossRef]
- Hung, J.-W.; Yen, C.-L.; Chang, K.-C.; Chiang, W.-C.; Chuang, I.-C.; Pong, Y.-P.; Wu, W.-C.; Wu, C.-Y. A Pilot Randomized Controlled Trial of Botulinum Toxin Treatment Combined with Robot-Assisted Therapy, Mirror Therapy, or Active Control Treatment in Patients with Spasticity Following Stroke. Toxins 2022, 14, 415. [Google Scholar] [CrossRef] [PubMed]
- Pheasant, S.; Haslegrave, C.M. Bodyspace: Anthropometry, Ergonomics and the Design of Work, 3rd ed.; CRC Press: Boca Raton, FL, USA; Taylor and Francis: London, UK, 2003. [Google Scholar] [CrossRef]
- Kladovasilakis, N.; Sideridis, P.; Tzetzis, D.; Piliounis, K.; Kostavelis, I.; Tzovaras, D. Design and Development of a Multi-Functional Bioinspired Soft Robotic Actuator via Additive Manufacturing. Biomimetics 2022, 7, 105. [Google Scholar] [CrossRef]
- Wang, Y.; Pandit, P.; Kandhari, A.; Liu, Z.; Daltorio, K.A. Rapidly Exploring Random Tree Algorithm-Based Path Planning for Worm-Like Robot. Biomimetics 2020, 5, 26. [Google Scholar] [CrossRef]
- Kandhari, A.; Wang, Y.; Daltorio, K.; Chiel, H.J. Turning in Worm-Like Robots: The Geometry of Slip Elimination Suggests Nonperiodic Waves. Soft Robot. 2019, 6, 560–577. [Google Scholar] [CrossRef] [PubMed]
- Ozkan-Aydin, Y.; Liu, B.; Ferrero, A.C.; Seidel, M.; Hammond, F.L.; Goldmand, D.I. Lateral bending and buckling aids biological and robotic earthworm anchoring and locomotion. Bioinspir. Biomim. 2022, 17, 016001. [Google Scholar] [CrossRef]
- Wang, J.; Fei, Y. Design and Modelling of Flex-Rigid Soft Robot for Flipping Locomotion. J. Intell. Robot. Syst. 2019, 95, 379–388. [Google Scholar] [CrossRef]
- Carvajal, J.; Chen, G.; Ogmen, H. Fuzzy PID controller: Design, performance evaluation, and stability analysis. Inf. Sci. 2000, 123, 249–270. [Google Scholar] [CrossRef]
- Astrom, K.J.; Hagglund, H. PID Controllers: Theory, Design and Tuning, 2nd ed.; Instrument Society of America: Research Triangle Park, NC, USA, 1995. [Google Scholar]
- Matheus, K.; Dollar, A.M. Benchmarking grasping and manipulation: Properties of the objects of daily living. In Proceedings of the International Conference on Intelligent Robots and Systems IROS, Taipei, Taiwan, 18–22 October 2010; pp. 5020–5027. [Google Scholar] [CrossRef]
- Dutta, D.; Aruchamy, S.; Mandal, S.; Sen, S. Poststroke Grasp Ability Assessment Using an Intelligent Data Glove Based on Action Research Arm Test: Development, Algorithms, and Experiments. IEEE Trans. Biomed. Eng. 2021, 69, 945–954. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Technical Characteristics |
|---|---|
| Power Supply | 110–220 V (50–60 Hz) |
| Connectivity | WiFi, USB type B |
| Air Supply | 300–1000 kPa |
| Operating Air Pressure | 200–250 kPa |
| Circuit Voltage | 3.3 V DC |
| Control Glove Power Supply | 5 V DC |
| Control Glove Battery | Li-Po 3.7 V—550 mAh |
| Operating Actuators | 5 |
| Description | Patient Characteristics |
|---|---|
| Age | >25 |
| Gender | Male and female |
| Disabled limb | Left or right hand |
| Rehabilitation stage | Partial hypoxia |
| Disability medical condition | Monoplegia and hemiplegia |
| Pathological condition | Cerebrovascular accident |
| Level of disability | 1–3 (Ashworth scale) |
| 1st Questionnaire (Control Group and Patients) | Likert Scale (1–Strongly Disagree to 5–Strongly Agree) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control Group | Patients | ||||||||||
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | ||
| Q101 | The use of the device is simple | - | - | 4 | 13 | 8 | - | 1 | - | 2 | 2 |
| Q102 | The use of the device is comfortable | - | - | 2 | 16 | 7 | - | - | 1 | 2 | 2 |
| Q103 | It was easy to learn how to operate the device | - | - | 4 | 15 | 3 | - | - | 1 | 3 | 1 |
| Q104 | I am familiar with the rehabilitation technologies | 2 | 4 | 4 | 12 | 3 | - | - | 2 | 2 | 1 |
| Q105 | The device can be integrated into the rehabilitation schedule | - | - | - | 13 | 12 | - | - | 1 | 3 | 1 |
| Q106 | The device’s user interface is user-friendly | - | 2 | 4 | 10 | 9 | - | 1 | 1 | 3 | - |
| Q107 | The device can offer appropriate movement capability | - | 2 | 3 | 13 | 7 | - | - | 2 | 2 | 1 |
| Q108 | I feel safe while using the device | - | - | - | 6 | 19 | - | - | 1 | 1 | 3 |
| Q109 | I feel that the SEG produces sufficient force | - | - | 4 | 5 | 16 | - | - | - | 4 | 1 |
| Q110 | The device is lightweight | - | - | - | 4 | 21 | - | - | - | 4 | 1 |
| Q111 | The visualized data help and guide the procedure | 5 | 5 | 7 | 8 | - | 1 | 1 | 1 | 2 | - |
| Q112 | The presentation of data on the GUI is clear | - | 4 | 13 | 4 | 4 | - | 2 | 1 | 2 | - |
| Q113 | The device has all the expected functionalities | - | 4 | 4 | 15 | 2 | - | - | 2 | 2 | 1 |
| Q114 | The use of the device is easily learned | - | 3 | 4 | 15 | 3 | - | - | 1 | 3 | 1 |
| 2nd Questionnaire (Healthcare Professionals) | Likert Scale (1—Strongly Disagree to 5—Strongly Agree) | |||||
|---|---|---|---|---|---|---|
| Q201 | The user can have full control of the device’s operation | - | - | 1 | - | 4 |
| Q202 | The motion data from the session are clearly visualized | - | - | - | 1 | 4 |
| Q203 | The desired data are easy to export in editable format | - | - | 2 | 2 | 1 |
| Q204 | The device offers a reliable library of each patient’s session data | - | - | - | 4 | 1 |
| Q205 | The device can contribute to the rehabilitation process | - | - | - | 2 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kladovasilakis, N.; Kostavelis, I.; Sideridis, P.; Koltzi, E.; Piliounis, K.; Tzetzis, D.; Tzovaras, D. A Novel Soft Robotic Exoskeleton System for Hand Rehabilitation and Assistance Purposes. Appl. Sci. 2023, 13, 553. https://doi.org/10.3390/app13010553
Kladovasilakis N, Kostavelis I, Sideridis P, Koltzi E, Piliounis K, Tzetzis D, Tzovaras D. A Novel Soft Robotic Exoskeleton System for Hand Rehabilitation and Assistance Purposes. Applied Sciences. 2023; 13(1):553. https://doi.org/10.3390/app13010553
Chicago/Turabian StyleKladovasilakis, Nikolaos, Ioannis Kostavelis, Paschalis Sideridis, Eleni Koltzi, Konstantinos Piliounis, Dimitrios Tzetzis, and Dimitrios Tzovaras. 2023. "A Novel Soft Robotic Exoskeleton System for Hand Rehabilitation and Assistance Purposes" Applied Sciences 13, no. 1: 553. https://doi.org/10.3390/app13010553
APA StyleKladovasilakis, N., Kostavelis, I., Sideridis, P., Koltzi, E., Piliounis, K., Tzetzis, D., & Tzovaras, D. (2023). A Novel Soft Robotic Exoskeleton System for Hand Rehabilitation and Assistance Purposes. Applied Sciences, 13(1), 553. https://doi.org/10.3390/app13010553