
Biomechanical Rationale for a Novel Implant Design Reducing Stress on Buccal Bone



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nicolielo, L.F.P.; Van Dessel, J.; Jacobs, R.; Quirino Silveira Soares, M.; Collaert, B. Relationship between trabecular bone architecture and early dental implant failure in the posterior region of the mandible. Clin. Oral Implant. Res. 2020, 31, 153–161. [Google Scholar]
- Karl, M.; Irastorza-Landa, A. Does implant design affect primary stability in extraction sites? Quintessence Int. 2017, 48, 219–224. [Google Scholar] [PubMed]
- Elias, C.N.; Rocha, F.; Nascimento, A.L.; Coelho, P.G. Influence of implant shape, surface morphology, surgical technique and bone quality on the primary stability of dental implants. J. Mech. Behav. Biomed. Mater. 2012, 16, 169–180. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Pérez-Díaz, L.; Mazón, P.; De Aza, P.N. Biomechanical Effects of a New Macrogeometry Design of Dental Implants: An In Vitro Experimental Analysis. J. Funct. Biomater. 2019, 10, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Zhu, Y.; Liu, Z.; Tian, Z.; Zhu, S. Association between diabetes and dental implant complications: A systematic review and meta-analysis. Acta. Odontol. Scand. 2021, 79, 9–18. [Google Scholar] [CrossRef]
- Chen, H.; Liu, N.; Xu, X.; Qu, X.; Lu, E. Smoking, radiotherapy, diabetes and osteoporosis as risk factors for dental implant failure: A meta-analysis. PLoS ONE 2013, 8, e71955. [Google Scholar] [CrossRef] [Green Version]
- Toia, M.; Stocchero, M.; Cecchinato, F.; Corrà, E.; Jimbo, R.; Cecchinato, D. Clinical Considerations of Adapted Drilling Protocol by Bone Quality Perception. Int. J. Oral Maxillofac. Implant. 2017, 32, 1288–1295. [Google Scholar] [CrossRef] [Green Version]
- Dard, M.; Kuehne, S.; Obrecht, M.; Grandin, M.; Helfenstein, J.; Pippenger, B.E. Integrative Performance Analysis of a Novel Bone Level Tapered Implant. Adv. Dent. Res. 2016, 28, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Eppell, S.J.; Nguyen, C.; Morris, N. Relative Contribution of Trabecular and Cortical Bone to Primary Implant Stability: An In Vitro Model Study. J. Oral Implant. 2016, 42, 145–152. [Google Scholar] [CrossRef]
- Huang, H.L.; Chang, Y.Y.; Lin, D.J.; Li, Y.F.; Chen, K.; Hsu, J.T. Initial stability and bone strain evaluation of the immediately loaded dental implant: An in vitro model study. Clin. Oral Implant. Res. 2011, 22, 691–698. [Google Scholar]
- Cohen, O.; Ormianer, Z.; Tal, H.; Rothamel, D.; Weinreb, M.; Moses, O. Differences in crestal bone-to-implant contact following an under-drilling compared to an over-drilling protocol. A study in the rabbit tibia. Clin. Oral Investig. 2016, 20, 2475–2480. [Google Scholar] [CrossRef]
- Wilson, T.G., Jr.; Miller, R.J.; Trushkowsky, R.; Dard, M. Tapered Implants in Dentistry: Revitalizing Concepts with Technology: A Review. Adv. Dent. Res. 2016, 28, 4–9. [Google Scholar] [CrossRef]
- Ikar, M.; Grobecker-Karl, T.; Karl, M.; Steiner, C. Mechanical stress during implant surgery and its effects on marginal bone: A literature review. Quintessence Int. 2020, 51, 142–150. [Google Scholar] [PubMed]
- Barone, A.; Alfonsi, F.; Derchi, G.; Tonelli, P.; Toti, P.; Marchionni, S.; Covani, U. The Effect of Insertion Torque on the Clinical Outcome of Single Implants: A Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2016, 18, 588–600. [Google Scholar] [CrossRef]
- De Santis, D.; Cucchi, A.; Rigoni, G.; Longhi, C.; Nocini, P.F. Relationship Between Primary Stability and Crestal Bone Loss of Implants Placed with High Insertion Torque: A 3-Year Prospective Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Norton, M.R. The Influence of Low Insertion Torque on Primary Stability, Implant Survival, and Maintenance of Marginal Bone Levels: A Closed-Cohort Prospective Study. Int. J. Oral Maxillofac. Implant. 2017, 32, 849–857. [Google Scholar] [CrossRef]
- Kern, J.S.; Kern, T.; Wolfart, S.; Heussen, N. A systematic review and meta-analysis of removable and fixed implant-supported prostheses in edentulous jaws: Post-loading implant loss. Clin. Oral. Implants. Res. 2016, 27, 174–195. [Google Scholar] [PubMed] [Green Version]
- Stavropoulos, A.; Cochran, D.; Obrecht, M.; Pippenger, B.E.; Dard, M. Effect of Osteotomy Preparation on Osseointegration of Immediately Loaded, Tapered Dental Implants. Adv. Dent. Res. 2016, 28, 34–41. [Google Scholar] [CrossRef]
- Eom, T.G.; Kim, H.W.; Jeon, G.R.; Yun, M.J.; Huh, J.B.; Jeong, C.M. Effects of Different Implant Osteotomy Preparation Sizes on Implant Stability and Bone Response in the Minipig Mandible. Int. J. Oral Maxillofac. Implant. 2016, 31, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Sadowsky, S.J.; Brunski, J.B.; Yuan, X.; Helms, J.A. Effects of masticatory loading on bone remodeling around teeth versus implants: Insights from a preclinical model. Clin. Oral. Implants. Res. 2022, 33, 342–352. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Carcuac, O.; Berglundh, T. Influence of implant geometry and osteotomy design on early bone healing: A pre-clinical in vivo study. Clin. Oral. Implants. Res. 2021, 32, 1190–1199. [Google Scholar] [CrossRef]
- Mehl, C.; Becker, S.T.; Acil, Y.; Harder, S.; Wiltfang, J.; Dabbagh-Afrouz, A.A.; de Buhr, W.; Kern, M. Impact of vertical loading on the implant-bone interface. Clin. Oral. Implants. Res. 2013, 24, 949–956. [Google Scholar] [CrossRef]
- Rea, M.; Lang, N.P.; Ricci, S.; Mintrone, F.; González González, G.; Botticelli, D. Healing of implants installed in over- or under-prepared sites—An experimental study in dogs. Clin. Oral Implant. Res. 2015, 26, 442–446. [Google Scholar] [CrossRef]
- Cha, J.Y.; Pereira, M.D.; Smith, A.A.; Houschyar, K.S.; Yin, X.; Mouraret, S.; Brunski, J.B.; Helms, J.A. Multiscale analyses of the bone-implant interface. J. Dent. Res. 2015, 94, 482–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Wu, Y.; Perez, K.C.; Hyman, S.; Brunski, J.B.; Tulu, U.; Bao, C.; Salmon, B.; Helms, J.A. Effects of Condensation on Peri-implant Bone Density and Remodeling. J. Dent. Res. 2017, 96, 413–420. [Google Scholar] [CrossRef]
- Bandela, V.; Shetty, N.; Munagapati, B.; Basany, R.B.; Kanaparthi, S. Comparative Evaluation of Osseodensification Versus Conventional Osteotomy Technique on Dental Implant Primary Stability: An Ex Vivo Study. Cureus 2022, 14, e30843. [Google Scholar] [CrossRef] [PubMed]
- Winter, W.; Möhrle, S.; Holst, S.; Karl, M. Parameters of implant stability measurements based on resonance frequency and damping capacity: A comparative finite element analysis. Int. J. Oral. Maxillofac. Implants. 2010, 25, 532–539. [Google Scholar]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontology 2000 2017, 73, 41–50. [Google Scholar] [CrossRef]
- Friberg, B.; Ahmadzai, M. A prospective study on single tooth reconstructions using parallel walled implants with internal connection (Nobel Parallel CC) and abutments with angulated screw channels (ASC). Clin. Implant. Dent. Relat. Res. 2019, 21, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Klär, V.; Karl, M.; Grobecker-Karl, T. Bone damage during dental implant insertion: A pilot study combining strain gauge and histologic analysis. Appl. Sci. 2022, 12, 291. [Google Scholar] [CrossRef]
- Steiner, C.; Karl, M.; Grobecker-Karl, T. Insertion and loading characteristics of three different bone-level implants. Int. J. Oral Maxillofac. Implant. 2020, 35, 560–565. [Google Scholar] [CrossRef]
- Steiner, C.; Karl, M.; Grobecker-Karl, T. Wedge shaped vs. round implants: Bone strain during the insertion process. J. Oral Implantol. 2022; accepted. [Google Scholar]
- Sierra-Rebolledo, A.; Allais-Leon, M.; Maurette-O’Brien, P.; Gay-Escoda, C. Primary Apical Stability of Tapered Implants Through Reduction of Final Drilling Dimensions in Different Bone Density Models: A Biomechanical Study. Implant. Dent. 2016, 25, 775–782. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Arosio, P.; Gastaldi, G.; Gherlone, E. The insertion torque-depth curve integral as a measure of implant primary stability: An in vitro study on polyurethane foam blocks. J. Prosthet. Dent. 2018, 120, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.M.; Lee, M.S.; Wang, J.S.; Lin, L.D. The effect of implant design and bone quality on insertion torque, resonance frequency analysis, and insertion energy during implant placement in low or low- to medium-density bone. Int. J. Prosthodont. 2015, 28, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Ueno, D.; Nakamura, K.; Kojima, K.; Toyoshima, T.; Tanaka, H.; Ueda, K.; Koyano, K.; Kodama, T. A stepwise under-prepared osteotomy technique improves primary stability in shallow-placed implants: A preliminary study for simultaneous vertical ridge augmentation. Odontology 2018, 106, 187–193. [Google Scholar] [CrossRef]
- Akkoyun, E.F.; Demirbaş, A.E.; Gümüş, H.Ö.; Alkan, B.A.; Alkan, A. Custom-Made Root Analog Immediate Dental Implants: A Prospective Clinical Study with 1-Year Follow-up. Int. J. Oral. Maxillofac. Implants. 2022, 37, 1223–1231. [Google Scholar] [CrossRef]
- Li Manni, L.; Lecloux, G.; Rompen, E.; Aouini, W.; Shapira, L.; Lambert, F. Clinical and radiographic assessment of circular versus triangular cross-section neck Implants in the posterior maxilla: A 1-year randomized controlled trial. Clin. Oral Implant. Res. 2020, 31, 814–824. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group Name | Straumann | AlfaGate |
|---|---|---|
| Implant | Straumann Bone Level Tapered 4.1 × 10 mm (Institut Straumann AG, Basel, Switzerland) | AlfaGate Novel Design 4.3 × 10 mm (Alfa Gate, Kfar Qara, Israel) |
| Drill sequence | Needle drill 2.2 mm pilot drill 2.8 mm BLT drill 3.5 mm BLT drill Cortical drill @ conical part | Start drill @ 3 mm 2.0 2.8 3.2 3.65 @ 6 mm |
| Parameter | BLT | AG | t-Test (p-Value) | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
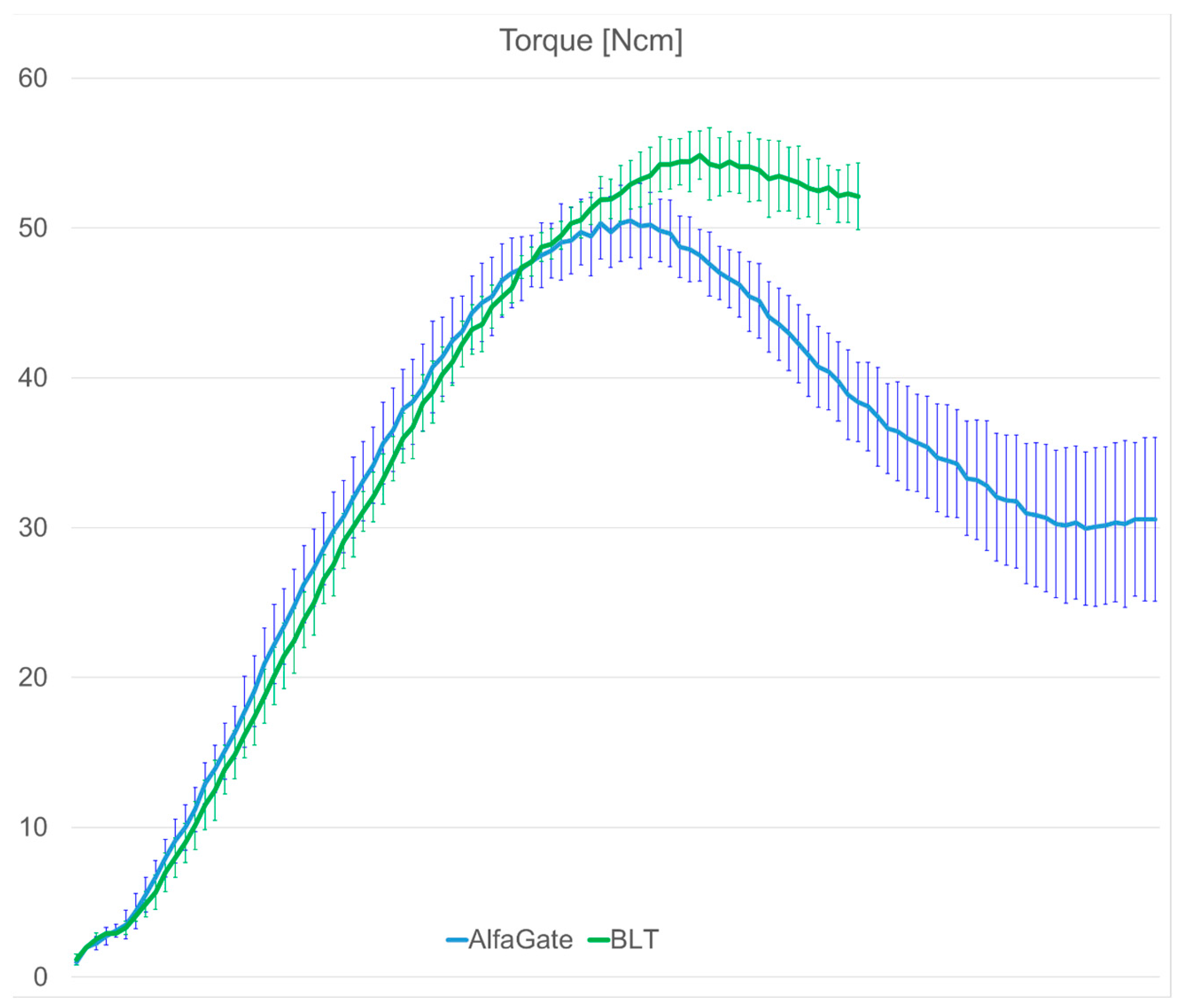
| Maximum insertion torque [Ncm] | 55.16 | 1.95 | 50.9 | 2.6 | 0.0016 |
| Position of maximum insertion torque | 63.14 | 2.97 | 54.5 | 3.95 | 0.0001 |
| Final insertion torque [Ncm] | 52.11 | 2.22 | 30.55 | 5.47 | <0.00001 |
| Maximum strain [µm/m] | 11,370.18 | 4206.6 | 8236.39 | 2176.31 | 0.1069 |
| Position of maximum strain | 912.29 | 57.48 | 716.9 | 50.59 | <0.0001 |
| Final strain [µm/m] | 10,834.31 | 3923.14 | 5798.27 | 1868.82 | 0.0137 |
| Periotest [PTV] | 8.415 | 3.003 | 6.685 | 3.072 | 0.219 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz, A.; Klär, V.; Grobecker-Karl, T.; Karl, M. Biomechanical Rationale for a Novel Implant Design Reducing Stress on Buccal Bone. Appl. Sci. 2023, 13, 666. https://doi.org/10.3390/app13010666
Schulz A, Klär V, Grobecker-Karl T, Karl M. Biomechanical Rationale for a Novel Implant Design Reducing Stress on Buccal Bone. Applied Sciences. 2023; 13(1):666. https://doi.org/10.3390/app13010666
Chicago/Turabian StyleSchulz, Annika, Virgilia Klär, Tanja Grobecker-Karl, and Matthias Karl. 2023. "Biomechanical Rationale for a Novel Implant Design Reducing Stress on Buccal Bone" Applied Sciences 13, no. 1: 666. https://doi.org/10.3390/app13010666
APA StyleSchulz, A., Klär, V., Grobecker-Karl, T., & Karl, M. (2023). Biomechanical Rationale for a Novel Implant Design Reducing Stress on Buccal Bone. Applied Sciences, 13(1), 666. https://doi.org/10.3390/app13010666