

Assessing Non-Intrusive Wearable Devices for Tracking Core Body Temperature in Hot Working Conditions



Abstract
:1. Introduction
1.1. Heat Stress and Mitigation Techniques in Occupational Settings
1.2. Wearable Sensing Devices for Core Temperature Measurement
- H1a: SS wearable sensor CT data are within the clinically acceptable limits.
- H1b: There is a linear association between SS and ICTS, ρ ≠ 0.
- H1c: Individual differences have a significant effect on the SS CT measurement.
- H2a: ZephyrTM wearable sensor CT data are within the clinically acceptable limits.
- H2b: There is a linear correlation between ZephyrTM and ICTS, ρ ≠ 0.
- H2c: Individual differences have a significant effect on the Zephyr CT measurement.
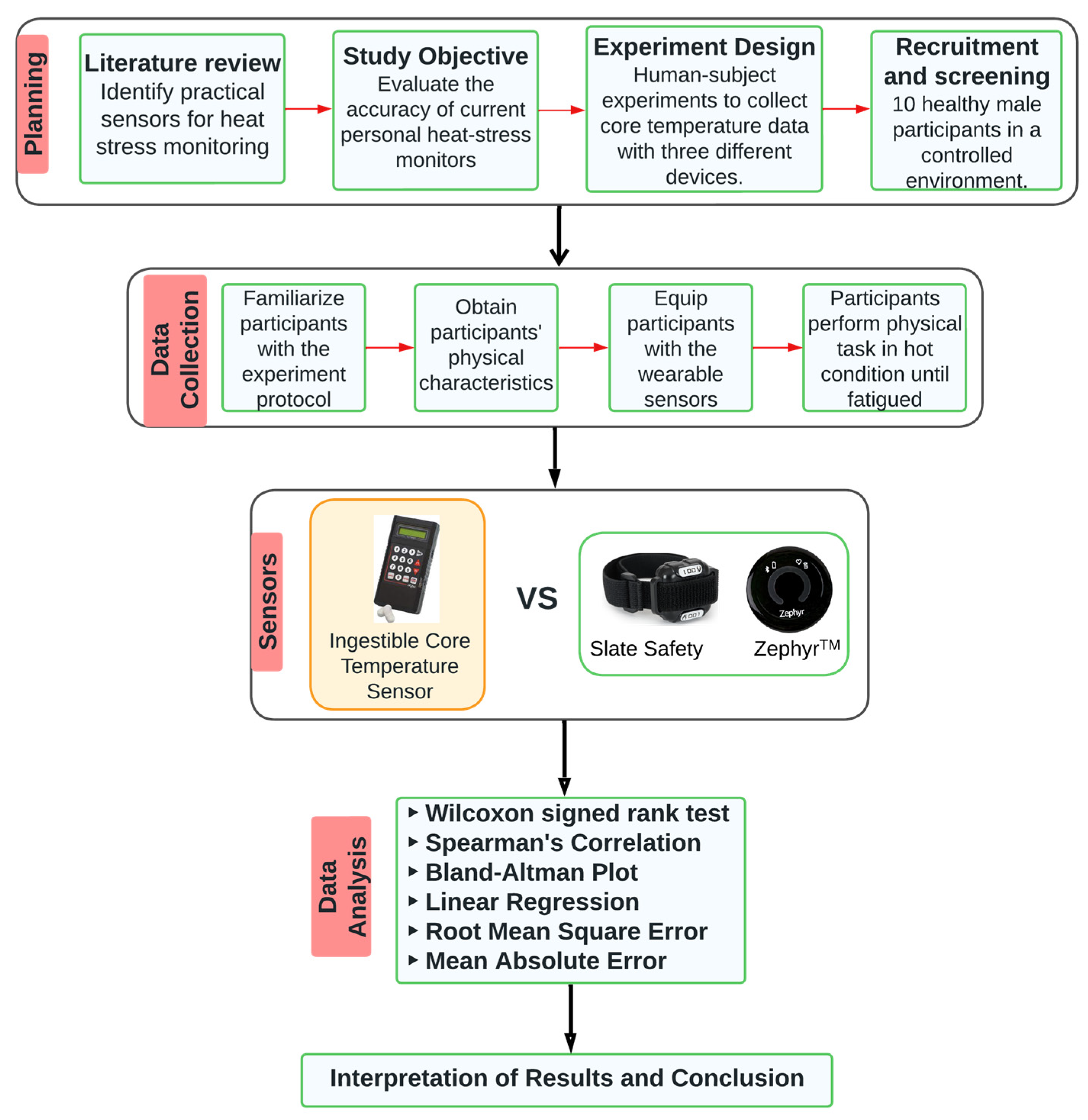
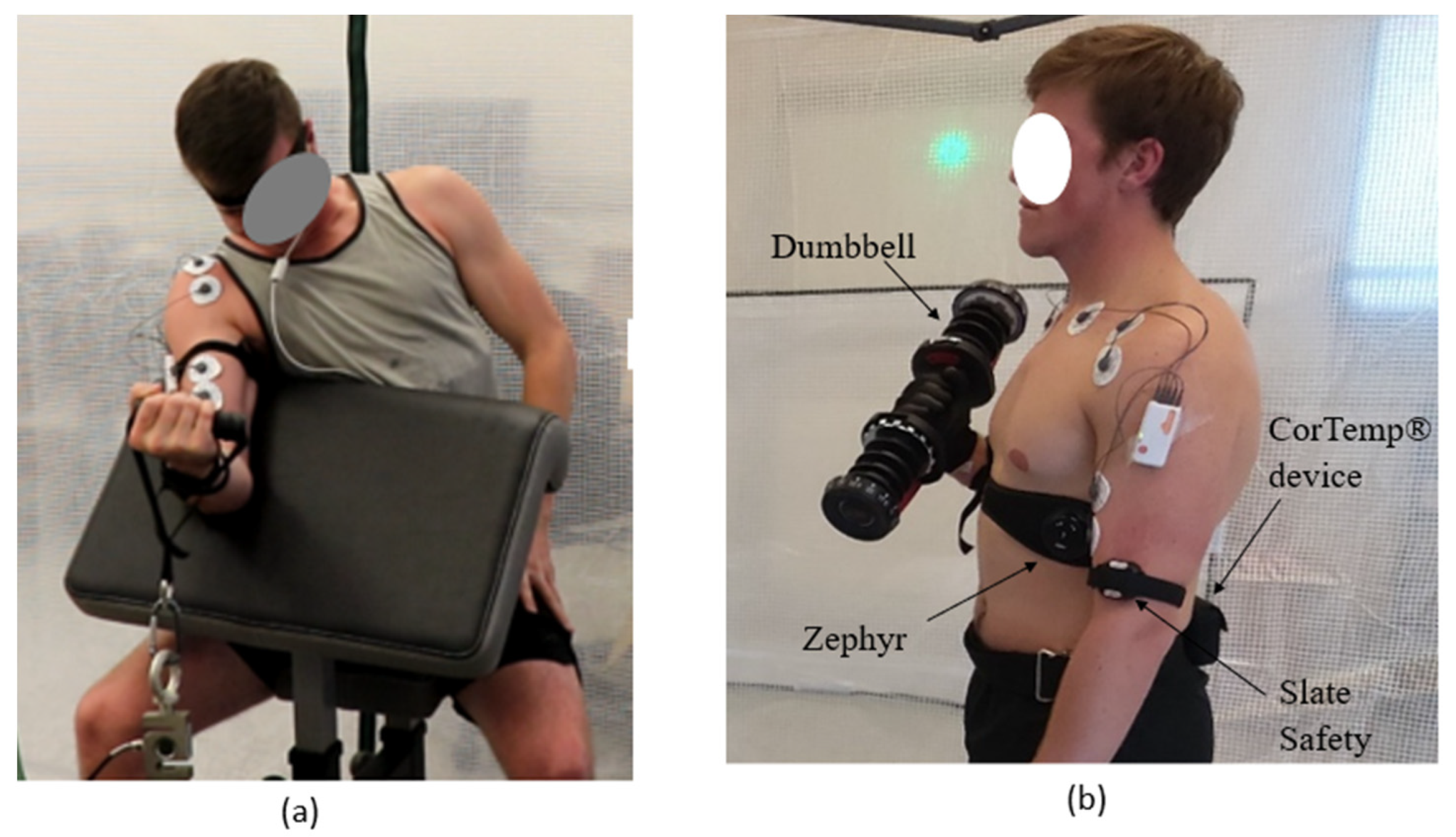
2. Materials and Methods
2.1. Experimental Design
2.2. Data Analysis
3. Results
3.1. Slate Safety Wearable Sensor
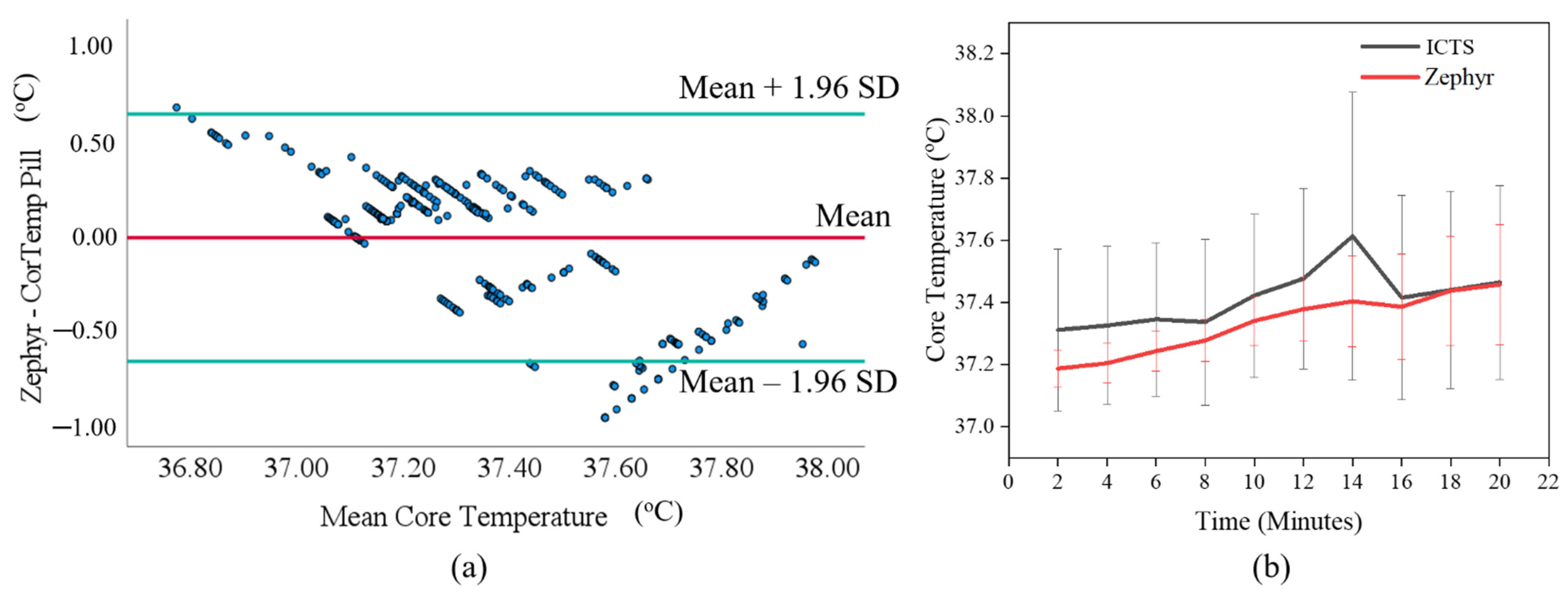
3.2. Zephyr Wearable Sensor
4. Discussion
4.1. Clinically Acceptable Limits
4.2. Relationship between Wearable Sensors and ICTS
4.3. Individual Differences
4.4. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The National Institute for Occupational Safety and Health (NIOSH). Heat Stress. Workplace Safety and Health Topics. 2020. Available online: https://www.cdc.gov/niosh/topics/heatstress/default.html (accessed on 13 February 2023).
- Zink, A.; Wurstbauer, D.; Rotter, M.; Wildner, M.; Biedermann, T. Do outdoor workers know their risk of NMSC? Perceptions, beliefs and preventive behaviour among farmers, roofers and gardeners. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1649–1654. [Google Scholar] [CrossRef] [Green Version]
- U.S. Bureau of Labor Statistics. 43 Work-Related Deaths Due to Environmental Heat Exposure in 2019. The Economics Daily, 2021. Available online: https://www.bls.gov/opub/ted/2021/43-work-related-deaths-due-to-environmental-heat-exposure-in-2019.htm (accessed on 13 February 2023).
- CPWR. The Construction Chart Book; The Center for Construction Research and Training: Silver Spring, MD, USA, 2016. [Google Scholar]
- Fitzwater, J.; Johnstone, C.; Schippers, M.; Cordoza, M.; Norman, B. A Comparison of Oral, Axillary, and Temporal Artery Temperature Measuring Devices in Adult Acute Care. MedsurgNursing 2019, 28, 35–41. [Google Scholar]
- Glaser, J.; Lemery, J.; Rajagopalan, B.; Diaz, H.F.; García-Trabanino, R.; Taduri, G.; Madero, M.; Amarasinghe, M.; Abraham, G.; Anutrakulchai, S.; et al. Climate change and the emergent epidemic of CKD from heat stress in rural communities: The case for heat stress nephropathy. Clin. J. Am. Soc. Nephrol. 2016, 11, 1472–1483. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Heat Stress Controls. 2022. Available online: https://www.cdc.gov/niosh/topics/heatstress/controls.html (accessed on 2 April 2023).
- Notley, S.R.; Kenny, G.P.; Flouris, A.D. On the use of wearable physiological monitors to assess heat strain during occupational heat stress. Appl. Physiol. Nutr. Metab. 2018, 43, 869–881. [Google Scholar] [CrossRef]
- Sawka, M.N.; Friedl, K.E. Emerging Wearable Physiological Monitoring Technologies and Decision Aids for Health and Performance. J. Appl. Physiol. 2018, 124, 430–431. [Google Scholar] [CrossRef]
- Haldane, J.S. The Influence of High Air Temperatures No. I. Epidemiol. Infect. 1905, 5, 494–513. [Google Scholar] [CrossRef] [PubMed]
- Institute for Quality and Efficiency in Health Care (IQWiG). How Is Body Temperature Regulated and What Is Fever?—InformedHealth.org—NCBI Bookshelf. 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK279457/ (accessed on 21 March 2023).
- Leon, L.R.; Bouchama, A. Heat Stroke. Compr. Physiol. 2015, 5, 611–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Conference of Governmental Industrial Hygienists (ACGIH). TLVs and BEIs Based on the Documentation of the Threshold Limit Values for Chemical Substances and Physical Agents & Biological Exposure Indices; American Conference of Governmental Industrial Hygienists (ACGIH): Cincinnati, OH, USA, 2017. [Google Scholar]
- Petersen, C.J.; Portus, M.R.; Pyne, D.B.; Dawson, B.T.; Cramer, M.N.; Kellett, A.D. Partial Heat Acclimation in Cricketers Using a 4-Day High Intensity Cycling Protocol. Int. J. Sports Physiol. Perform. 2010, 5, 535–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neff, L.M.; Hoffmann, M.E.; Zeiss, D.M.; Lowry, K.; Edwards, M.; Rodriguez, S.M.; Wachsberg, K.N.; Kushner, R.; Landsberg, L. Core body temperature is lower in postmenopausal women than premenopausal women: Potential implications for energy metabolism and midlife weight gain. Cardiovasc. Endocrinol. 2016, 5, 151. [Google Scholar] [CrossRef] [Green Version]
- Petry, A.; McGilvray, W.; Rakhshandeh, A.R.; Rakhshandeh, A. Technical note: Assessment of an alternative technique for measuring body temperature in pigs. J. Anim. Sci. 2017, 95, 3270–3274. [Google Scholar] [CrossRef]
- Casa, D.J.; Becker, S.M.; Ganio, M.S.; Brown, C.M.; Yeargin, S.W.; Roti, M.W.; Siegler, J.; Blowers, J.A.; Glaviano, N.R.; Huggins, R.A.; et al. Validity of Devices That Assess Body Temperature During Outdoor Exercise in the Heat. J. Athl. Train. 2007, 42, 333. [Google Scholar] [CrossRef] [PubMed]
- HQ, Inc. CorTemp. 2022. Available online: https://www.hqinc.net/cortemp/ (accessed on 14 February 2023).
- Callihan, M.; Cole, H.; Stokley, H.; Gunter, J.; Clamp, K.; Martin, A.; Doherty, H. Comparison of Slate Safety Wearable Device to Ingestible Pill and Wearable Heart Rate Monitor. Sensors 2023, 23, 877. [Google Scholar] [CrossRef] [PubMed]
- SlateSafety. Connected Worker Safety. 2021. Available online: https://slatesafety.com/ (accessed on 5 January 2022).
- Zephyr Technology. Omnisense Analysis and Help; Zephyr Technology: Annapolis, MD, USA, 2016. [Google Scholar]
- Kalman, R.E. A New Approach to Linear Filtering and Prediction Problems. J. Basic Eng. 1960, 82, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Seo, Y.; DiLeo, T.; Powell, J.B.; Kim, J.H.; Roberge, R.J.; Coca, A. Comparison of estimated core body temperature measured with the BioHarness and rectal temperature under several heat stress conditions. J. Occup. Environ. Hyg. 2016, 13, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Daanen, H.A.M.; Kohlen, V.; Teunissen, L.P.J. Heat flux systems for body core temperature assessment during exercise. J. Therm. Biol. 2023, 112, 103480. [Google Scholar] [CrossRef]
- Iden, T.; Horn, E.P.; Bein, B.; Böhm, R.; Beese, J.; Höcker, J. Intraoperative temperature monitoring with zero heat flux technology (3M SpotOn sensor) in comparison with sublingual and nasopharyngeal temperature. Eur. J. Anaesthesiol. 2015, 32, 387–391. [Google Scholar] [CrossRef]
- Rubia-Rubia, J.; Arias, A.; Sierra, A.; Aguirre-Jaime, A. Measurement of body temperature in adult patients: Comparative study of accuracy, reliability and validity of different devices. Int. J. Nurs. Stud. 2011, 48, 872–880. [Google Scholar] [CrossRef]
- Edwards, B.; Waterhouse, J.; Reilly, T.; Atkinson, G. A comparison of the suitabilities of rectal, gut, and insulated axilla temperatures for measurement of the circadian rhythm of core temperature in field studies. Chronobiol. Int. 2009, 19, 579–597. [Google Scholar] [CrossRef]
- Hwang, H.J.; Chung, W.H.; Song, J.H.; Lim, J.K.; Kim, H.S. Prediction of biceps muscle fatigue and force using electromyography signal analysis for repeated isokinetic dumbbell curl exercise. J. Mech. Sci. Technol. 2016, 30, 5329–5336. [Google Scholar] [CrossRef]
- Antwi-Afari, M.F.; Li, H.; Edwards, D.J.; Pärn, E.A.; Seo, J.; Wong, A.Y.L. Biomechanical analysis of risk factors for work-related musculoskeletal disorders during repetitive lifting task in construction workers. Autom. Constr. 2017, 83, 41–47. [Google Scholar] [CrossRef]
- Al-Ashaik, R.A.; Ramadan, M.Z.; Al-Saleh, K.S.; Khalaf, T.M. Effect of safety shoes type, lifting frequency, and ambient temperature on subject’s MAWL and physiological responses. Int. J. Ind. Ergon. 2015, 50, 43–51. [Google Scholar] [CrossRef]
- Place, N.; Maffiuletti, N.A.; Martin, A.; Lepers, R. Assessment of the reliability of central and peripheral fatigue after sustained maximal voluntary contraction of the quadriceps muscle. Muscle Nerve 2007, 35, 486–495. [Google Scholar] [CrossRef] [PubMed]
- IBM Corporation. IBM SPSS Statistics for Windows; IBM Corporation: Armonk, NY, USA, 2019. [Google Scholar]
- CDC. Assessing Your Weight. Healthy Weight, Nutrition, and Physical Activity. Available online: https://www.cdc.gov/healthyweight/assessing/index.html (accessed on 22 May 2023).
- Hagen, J.; Himmler, A.; Clark, J.; Ramadan, J.; Stone, J.; Divine, J.; Mangine, R. Test and Evaluation of Heart Rate Derived Core Temperature Algorithms for Use in NCAA Division I Football Athletes. J. Funct. Morphol. Kinesiol. 2020, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Fortney, S.M.; Vroman, N.B. Exercise, performance and temperature control: Temperature regulation during exercise and implications for sports performance and training. Sports Med. 1985, 2, 8–20. [Google Scholar] [CrossRef]
- Lim, C.L.; Byrne, C.; Lee, J.K. Human Thermoregulation and Measurement of Body Temperature in Exercise and Clinical Settings. Ann. Acad. Med. Singap. 2008, 37, 347–353. [Google Scholar] [CrossRef]
- Dolson, C.M.; Harlow, E.R.; Phelan, D.M.; Gabbett, T.J.; Gaal, B.; McMellen, C.; Geletka, B.J.; Calcei, J.G.; Voos, J.E.; Seshadri, D.R. Wearable Sensor Technology to Predict Core Body Temperature: A Systematic Review. Sensors 2022, 22, 7639. [Google Scholar] [CrossRef] [PubMed]
- Hintz, C.; Presley, D.M.; Butler, C.R. Heat Stroke Burden and Validity of Wearable-Derived Core Temperature Estimation during Elite Military Training. Physician Sportsmed. 2023, 1–6. [Google Scholar] [CrossRef]
- Tyler, C.J.; Reeve, T.; Hodges, G.J.; Cheung, S.S. The Effects of Heat Adaptation on Physiology, Perception and Exercise Performance in the Heat: A Meta-Analysis. Sports Med. 2016, 46, 1699–1724. [Google Scholar] [CrossRef]
- McGowan, C.J.; Pyne, D.B.; Thompson, K.G.; Rattray, B. Warm-Up Strategies for Sport and Exercise: Mechanisms and Applications. Sports Med. 2015, 45, 1523–1546. [Google Scholar] [CrossRef]
- Coris, E.E.; Ramirez, A.M.; Van Durme, D.J. Heat Illness in Athletes: The Dangerous Combination of Heat, Humidity and Exercise. Sports Med. 2004, 34, 9–16. [Google Scholar] [CrossRef]
- Epstein, Y.; Roberts, W.O. The pathopysiology of heat stroke: An integrative view of the final common pathway. Scand. J. Med. Sci. Sports 2011, 21, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Savastano, D.M.; Gorbach, A.M.; Eden, H.S.; Brady, S.M.; Reynolds, J.C.; Yanovski, J.A. Adiposity and human regional body temperature. Am. J. Clin. Nutr. 2009, 90, 1124–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannon, B.; Nedergaard, J. Brown Adipose Tissue: Function and Physiological Significance. Physiol. Rev. 2004, 84, 277–359. [Google Scholar] [CrossRef] [PubMed]
- Dulloo, A.G.; Jacquet, J. An adipose-specific control of thermogenesis in body weight regulation. Int. J. Obes. 2001, 25, S22–S29. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Mean | Median | Standard Deviation | Minimum | Maximum |
|---|---|---|---|---|---|
| Age (years) | 21.7 | 20 | 3.9 | 18.0 | 29.0 |
| Height (inches) | 70.5 | 70 | 3.2 | 65.1 | 76.4 |
| Weight (pounds) | 160.4 | 166.4 | 25.5 | 112.8 | 201.6 |
| BMI | 22.7 | 23.2 | 3.3 | 17.2 | 29.0 |
| MVC (pounds) | 43.2 | 42.5 | 12.5 | 26.5 | 72.2 |
| ID | Intensity | BMI | Avoid Heat | Duration (mins) | Mean_ICTS | Max_ICTS | Mean_SS | Max_SS | Mean_Zephyr | Max_Zephyr |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Vigorous | Healthy | sometimes | 37 | 37.13 | 37.39 | 37.43 | 37.74 | 37.34 | 37.50 |
| 2 | moderate | Healthy | No | 47 | 37.19 | 37.53 | 37.55 | 38.03 | 37.35 | 37.80 |
| 3 | moderate | Healthy | no | 14 | 37.28 | 37.33 | 37.74 | 38.22 | 37.39 | 37.50 |
| 4 | Low | overweight | sometimes | 16 | 38.06 | 39.63 | 38.16 | 38.59 | 37.31 | 37.70 |
| 5 | moderate | underweight | no | 28 | 38.02 | 38.07 | 37.58 | 38.14 | 37.43 | 37.90 |
| 6 | Vigorous | overweight | sometimes | 9 | 36.60 | 36.78 | 37.41 | 37.68 | 37.12 | 37.20 |
| 7 | Low | Healthy | sometimes | 23 | 37.57 | 37.70 | 37.42 | 37.78 | 37.29 | 37.50 |
| 8 | Vigorous | Healthy | sometimes | 8 | 37.51 | 37.58 | 37.68 | 37.88 | 37.22 | 37.22 |
| 9 | Low | underweight | sometimes | 43 | 37.14 | 37.26 | 37.37 | 37.58 | 37.24 | 37.40 |
| 10 | Low | overweight | sometimes | 10 | 37.12 | 37.19 | 37.68 | 38.07 | 37.26 | 37.40 |
| Average | 37.36 | 37.39 | 37.60 | 37.74 | 37.30 | 37.50 |
| Temperature Difference | Mean | Maximum | ||
|---|---|---|---|---|
| Slate Safety | Zephyr | Slate Safety | Zephyr | |
| ≤±0.5 °C | 8 | 7 | 5 | 9 |
| >±0.5 °C to ±1.0 °C | 2 | 3 | 5 | 1 |
| CT Devices | Bias | Precision (SD) | 95% Limits of Agreement | |
|---|---|---|---|---|
| Lower | Upper | |||
| Slate Safety | 0.201 | 0.345 | −0.474 | 0.877 |
| Zephyr | −0.025 | 0.328 | −0.668 | 0.618 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, A.A.; Khan, M.; Nnaji, C.; Koh, A.S. Assessing Non-Intrusive Wearable Devices for Tracking Core Body Temperature in Hot Working Conditions. Appl. Sci. 2023, 13, 6803. https://doi.org/10.3390/app13116803
Ibrahim AA, Khan M, Nnaji C, Koh AS. Assessing Non-Intrusive Wearable Devices for Tracking Core Body Temperature in Hot Working Conditions. Applied Sciences. 2023; 13(11):6803. https://doi.org/10.3390/app13116803
Chicago/Turabian StyleIbrahim, Abdullahi A., Muhammad Khan, Chukwuma Nnaji, and Amanda S. Koh. 2023. "Assessing Non-Intrusive Wearable Devices for Tracking Core Body Temperature in Hot Working Conditions" Applied Sciences 13, no. 11: 6803. https://doi.org/10.3390/app13116803
APA StyleIbrahim, A. A., Khan, M., Nnaji, C., & Koh, A. S. (2023). Assessing Non-Intrusive Wearable Devices for Tracking Core Body Temperature in Hot Working Conditions. Applied Sciences, 13(11), 6803. https://doi.org/10.3390/app13116803