
An Experimental Evaluation of Respiration by Monitoring Ribcage Motion



Abstract
:1. Introduction
2. Materials and Methods
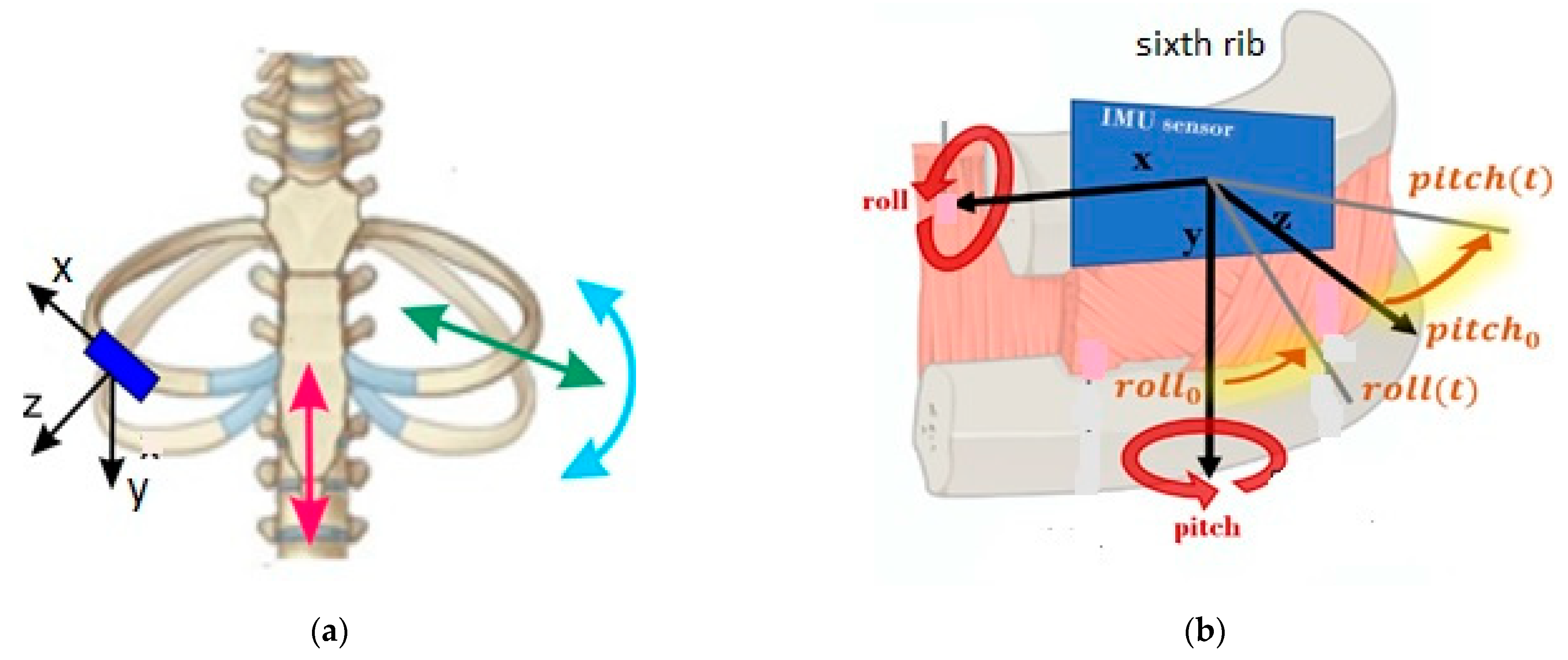
2.1. Respiration Characteristics
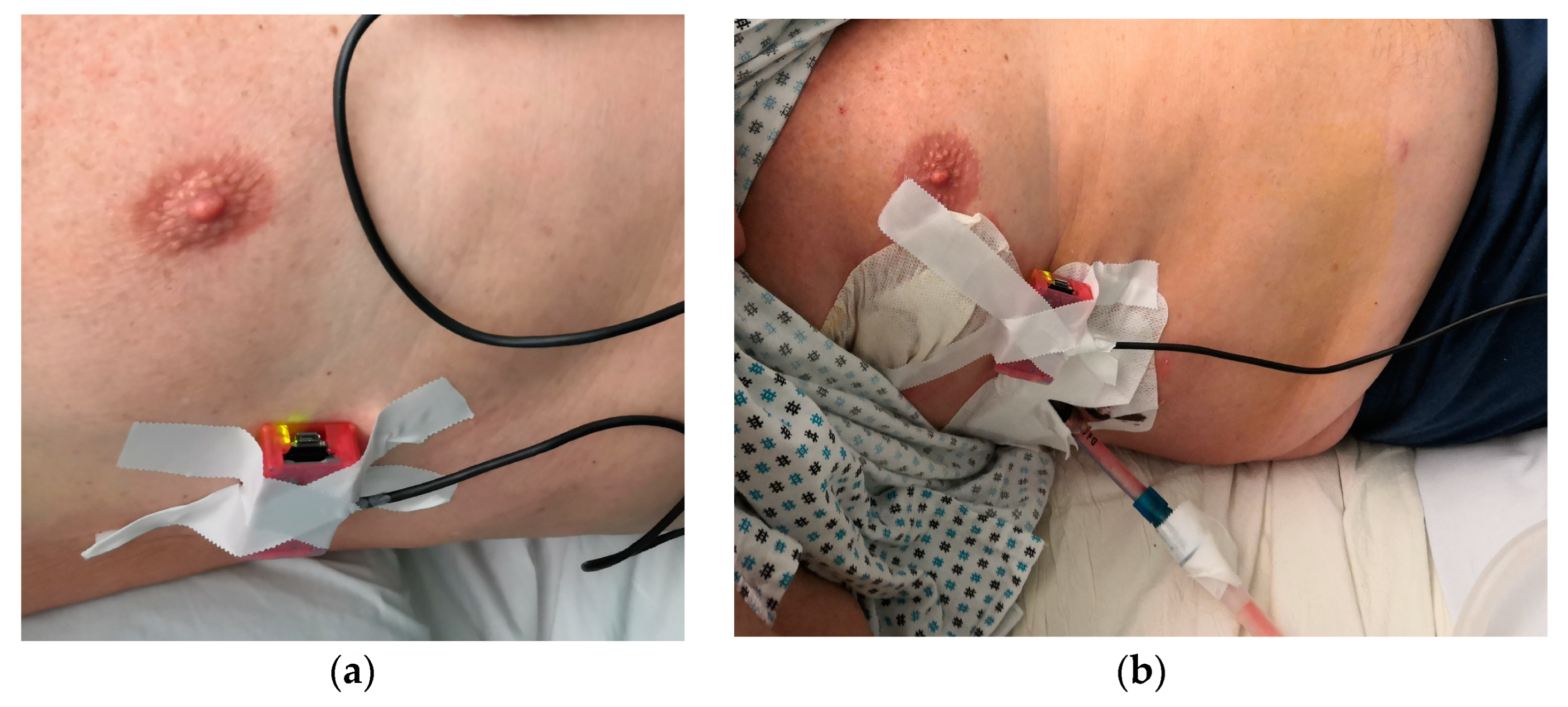
2.2. Respiration Evaluation by Means of RESPIRholter
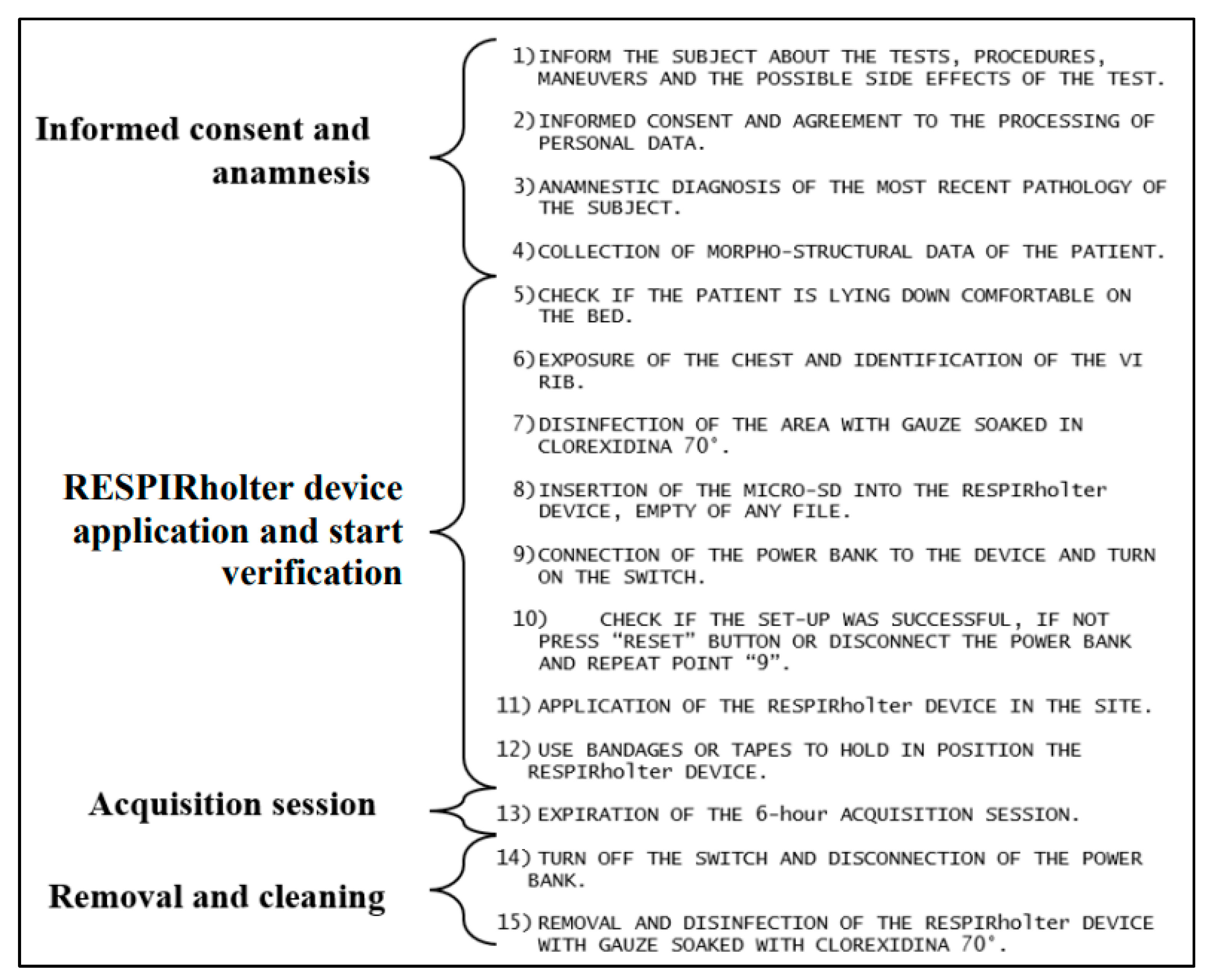
2.3. Procedure for a Campain of Testing
3. Results
3.1. Results of an Illustrative Case of Study
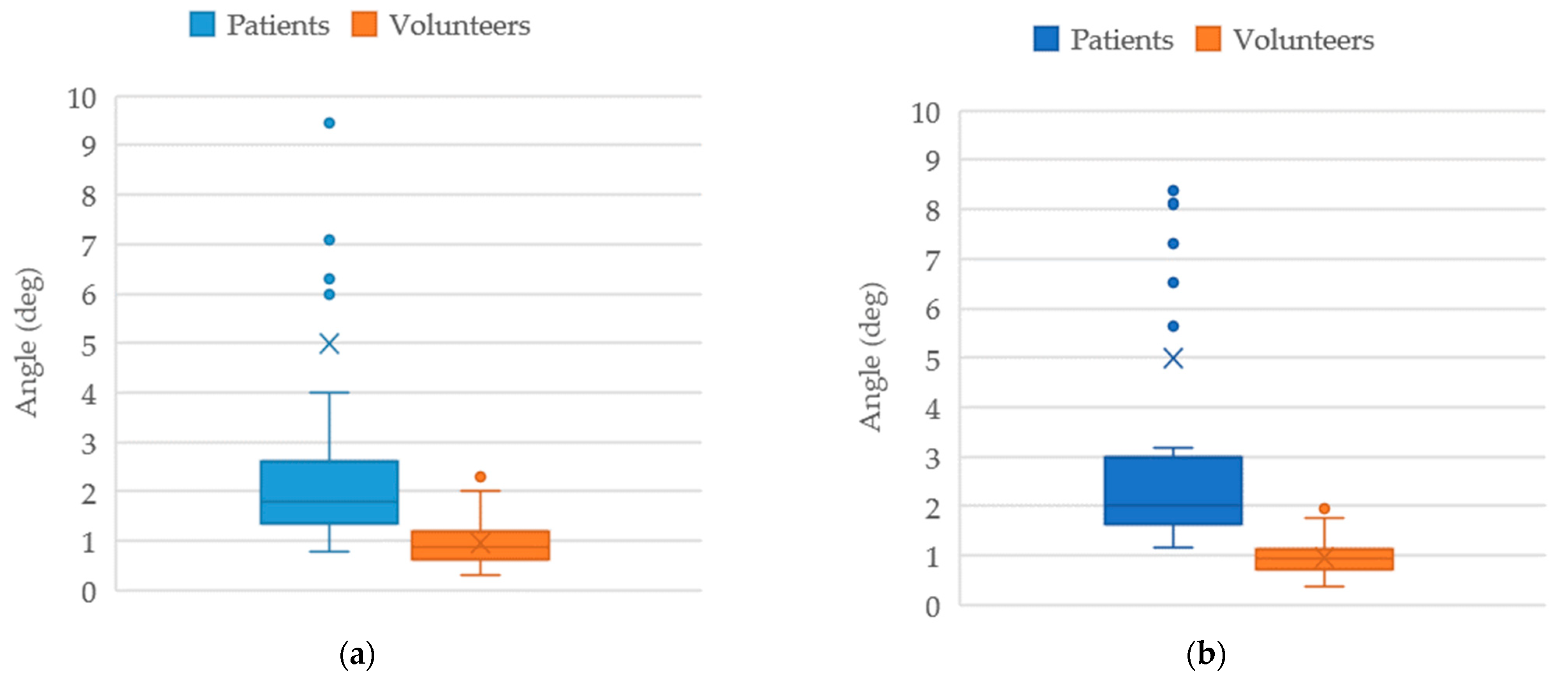
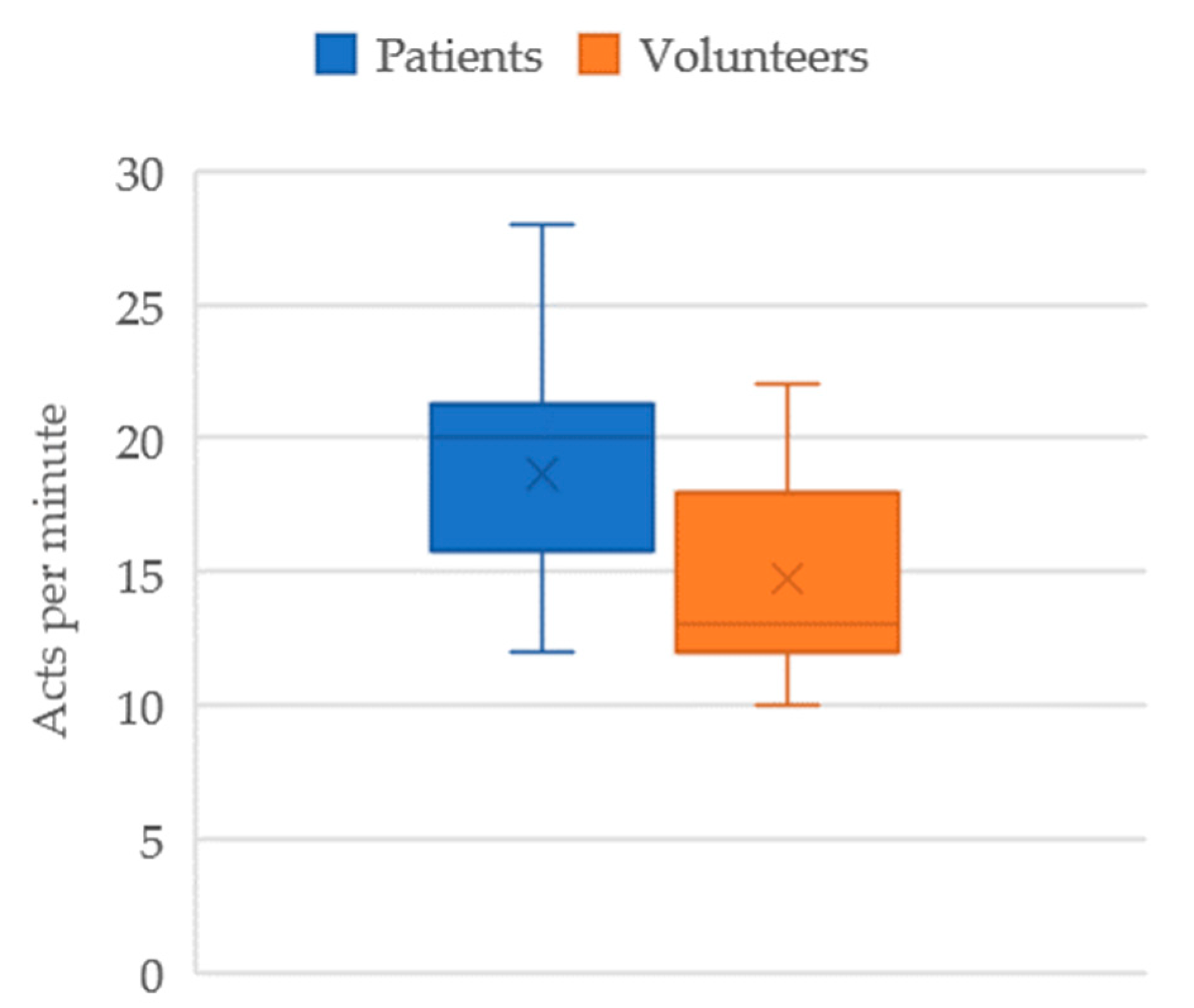
3.2. Statistic Elaboration of Testing Results
4. Conclusions
5. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, H.; Allen, J.; Zheng, D.; Chen, F. Recent development of respiratory rate measurement technologies. Physiol. Meas. 2019, 40, 07TR01. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krehel, M.; Schmid, M.; Rossi, R.; Boesel, L.; Bona, G.L.; Scherer, L. An Optical Fibre-Based Sensor for Respiratory Monitoring. Sensors 2014, 14, 13088–13101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Chen, B.; Zhou, J.; Lv, Z. A Low-Power and Portable Biomedical Device for Respiratory Monitoring with a Stable Power Source. Sensors 2015, 15, 19618–19632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfverti, A.; Cesareo, A. A Wearable Device for the Continuous Monitoring of the Respiratory Rate. International Patent Application No. WO 2019/012384, 11 January 2019. [Google Scholar]
- Ciocchetti, M.; Massaroni, C.; Saccomandi, P.; Caponero, M.A.; Polimadei, A.; Formica, D.; Schena, E. Smart textile based on fiber bragg grating sensors for respiratory monitoring: Design and preliminary trials. Biosensors 2015, 5, 602–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, J.E.; Lalli, M.; Mattfolk, A.; Panasyuk, A.; Jahnke, C.; Steiger, N.; Panasyuk, S.; Nagpal, A.; Toy, J.F. Devices and Methods for Respiratory Variation Monitoring by Measurement of Respiratory Volumes, Motion and Variability. European Patent WO2012021900A1, 16 February 2012. [Google Scholar]
- Peng, C.-K.; Goldberger, A.L.; Mietus, J.E.; Thomas, R.J. Evaluation of Sleep Quality and Breathing Problems during Sleep Based on the Cardiopulmonary Coupling. Patent ES 2348985T3, 28 March 2007. [Google Scholar]
- Gentili Biffi, G. Device for Monitoring of Respiration Functions. European Patent IT1222263B, 21 June 1990. [Google Scholar]
- Ceccarelli, M. Portable Device for Measuring the Movement of Human Ribs. European Patent 102021000005726, 13 March 2021. [Google Scholar]
- Ceccarelli, M.; Puglisi, L.; Mesiti, F.; Aquilini, M.; Ambrogi, V. A device for experimental characterization of biomechanics of breathing and coughing. In Proceedings of the 26th ABCM International Congress of Mechanical Engineering, Florianópolis, Brazil, 22–26 November 2021. Paper COB-2021-0273. [Google Scholar]
- Ceccarelli, M.; Papuc, P.E.; Taje, R.; Aquilini, M.; Ambrogi, V. A Biomechanics Analysis of Ventilation in Thorax Operated Patients. Int. J. Clin. Stud. Med. Case Rep. 2021, 15, 1–3. [Google Scholar] [CrossRef]
- Ceccarelli, M.; Ambrogi, M.; Puglisi, L.; Aquilini, M. Ventilatory Holter Device. European Patent IT102021000008585, 18 April 2023. [Google Scholar]
- Aquilini, M. RESPIRholter a Device for Breathing Monitoring. Master’s Thesis, University of Tor Vergata, Rome, Italy, 2022. [Google Scholar]
- Aquilini, M.; Ceccarelli, M. Design and Testing of RESPIRholter Device for Respiratory Monitoring. In Advances in Italian Mechanism Science; Niola, V., Gasparetto, A., Quaglia, G., Carbone, G., Eds.; Springer: Cham, Switzerland, 2022; pp. 480–488. [Google Scholar] [CrossRef]
- Aquilini, M.; Ceccarelli, M.; D’onofrio, M.; Ambrogi, V. An Experimental Characterization of Respiration Biomechanics by a Holter Device. In Proceedings of the 5th Jc-IFToMM International, Kyoto, Japan, 16 July 2022; Volume 5, pp. 80–87. [Google Scholar] [CrossRef]
- Chiaromonte, C. Calculation of the Sample Number; Internal Report; University of Rome Tor Vergata: Rome, Italy, 2020. (In Italian) [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Seg. | aXm (g) | aXM (g) | aYm (g) | aYM (g) | aZm (g) | aZM (g) | am (g) | aM (g) | rM (deg) | pM (deg) | RR (act/min) | ERG |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 0.84 | 0.91 | −0.37 | −0.31 | 0.31 | 0.33 | −0.31 | 0.16 | 0.89 | 1.05 | 12 | 8 |
| 2 | 0.84 | 0.89 | −0.35 | −0.32 | 0.28 | 0.34 | −0.47 | 0.05 | 1 | 1.24 | 12 | 8 |
| 3 | 0.81 | 0.87 | −0.5 | −0.44 | 0.23 | 0.25 | −0.20 | 0.06 | 1.03 | 1.23 | 12 | 8 |
| 4 | −0.75 | −0.69 | 0.25 | 0.31 | 0.59 | 0.66 | −0.13 | 0.04 | 1.47 | 1.54 | 12 | 8 |
| 5 | −0.75 | −0.69 | 0.28 | 0.31 | 0.6 | 0.66 | 0.00 | 0.04 | 1.66 | 1.75 | 12 | 8 |
| 6 | 0.77 | 0.81 | −0.34 | −0.28 | 0.5 | 0.56 | −0.21 | 0.23 | 0.49 | 1.31 | 12 | 8 |
| 7 | 0.85 | 0.85 | −0.49 | −0.47 | 0.2 | 0.22 | 0.01 | −0.04 | 0.54 | 0.84 | 12 | 8 |
| 8 | −0.68 | −0.66 | 0.19 | 0.25 | 0.66 | 0.72 | −0.33 | 0.08 | 0.95 | 1.06 | 12 | 8 |
| 9 | −0.72 | −0.66 | 0.22 | 0.25 | 0.66 | 0.68 | 0.01 | −0.20 | 0.95 | 1.39 | 12 | 8 |
| 10 | −0.52 | −0.5 | 0.09 | 0.16 | 0.81 | 0.85 | −0.33 | −0.01 | 0.7 | 1.35 | 12 | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceccarelli, M.; D’Onofrio, M.; Ambrogi, V.; Russo, M. An Experimental Evaluation of Respiration by Monitoring Ribcage Motion. Appl. Sci. 2023, 13, 8938. https://doi.org/10.3390/app13158938
Ceccarelli M, D’Onofrio M, Ambrogi V, Russo M. An Experimental Evaluation of Respiration by Monitoring Ribcage Motion. Applied Sciences. 2023; 13(15):8938. https://doi.org/10.3390/app13158938
Chicago/Turabian StyleCeccarelli, Marco, Manuel D’Onofrio, Vincenzo Ambrogi, and Matteo Russo. 2023. "An Experimental Evaluation of Respiration by Monitoring Ribcage Motion" Applied Sciences 13, no. 15: 8938. https://doi.org/10.3390/app13158938
APA StyleCeccarelli, M., D’Onofrio, M., Ambrogi, V., & Russo, M. (2023). An Experimental Evaluation of Respiration by Monitoring Ribcage Motion. Applied Sciences, 13(15), 8938. https://doi.org/10.3390/app13158938