
Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Guidelines
2.2. Human Gingival Tissue Explantation
2.3. Culture of Human Gingival Fibroblasts (hGFs)
2.4. Subculture and Expansion of hGFs
2.5. Experimental Collagen Membrane Groups
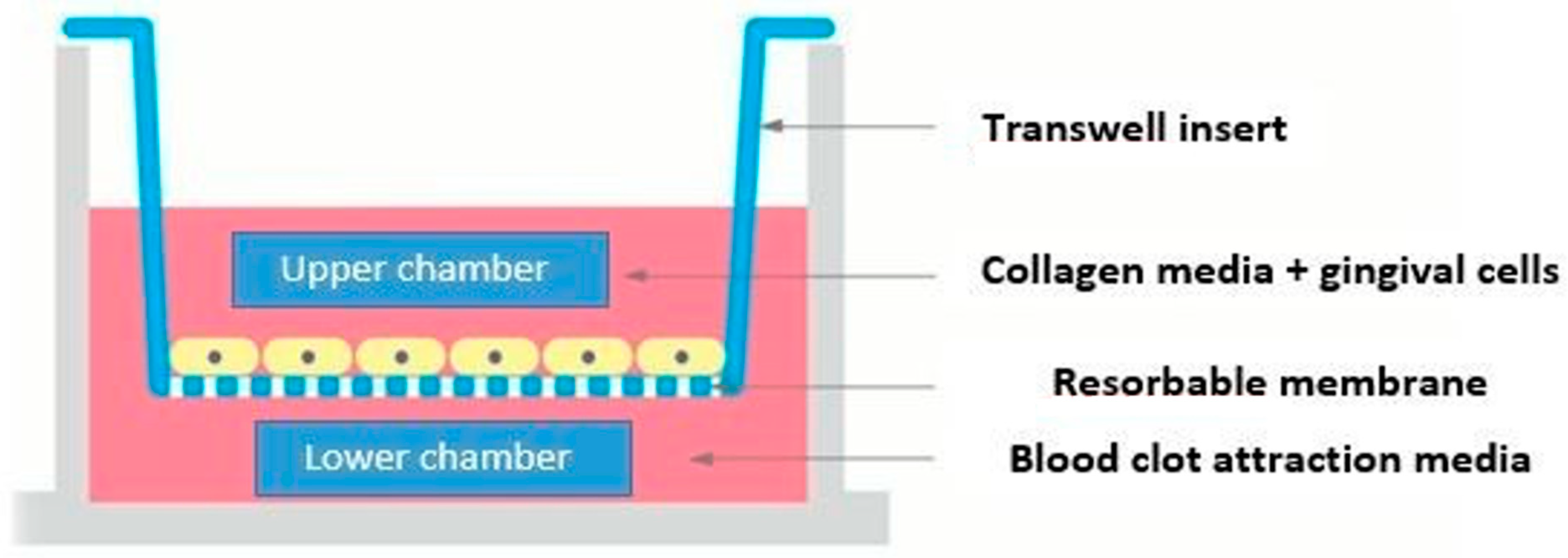
2.6. Assessment of Cell Viability and Proliferation/AlamarBlue® Assay Viability Test
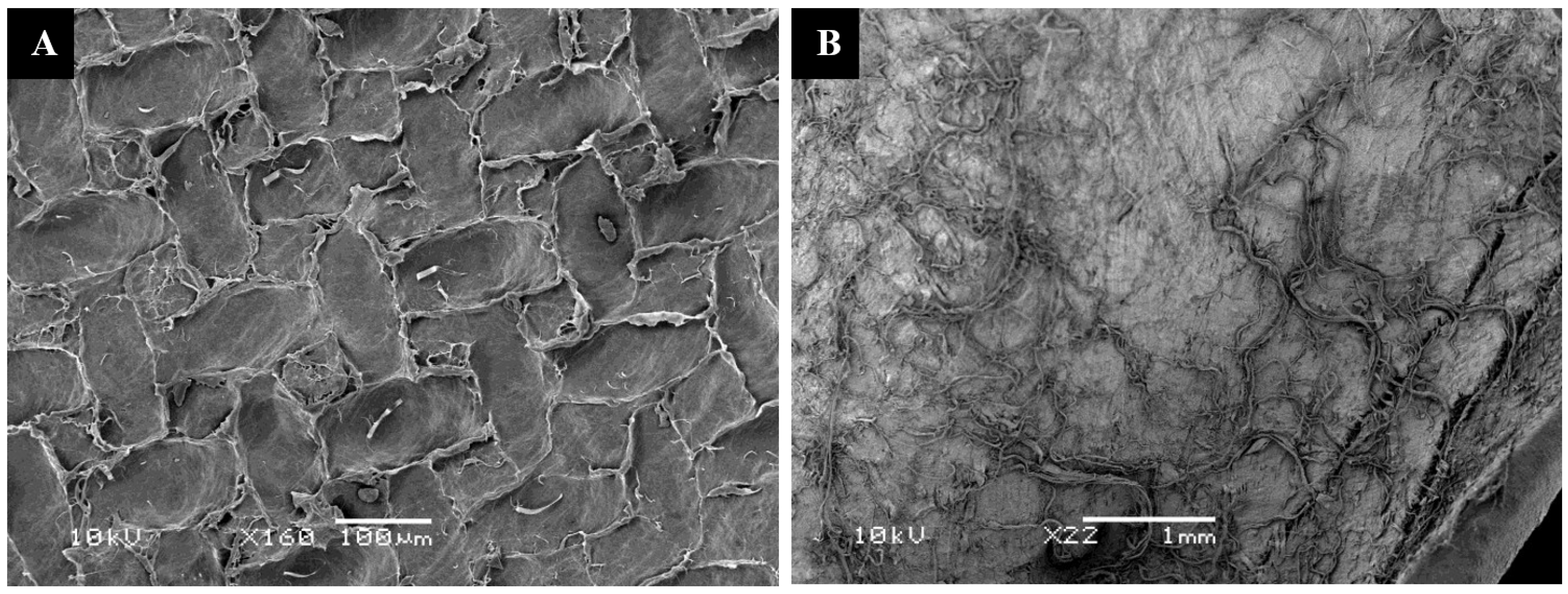
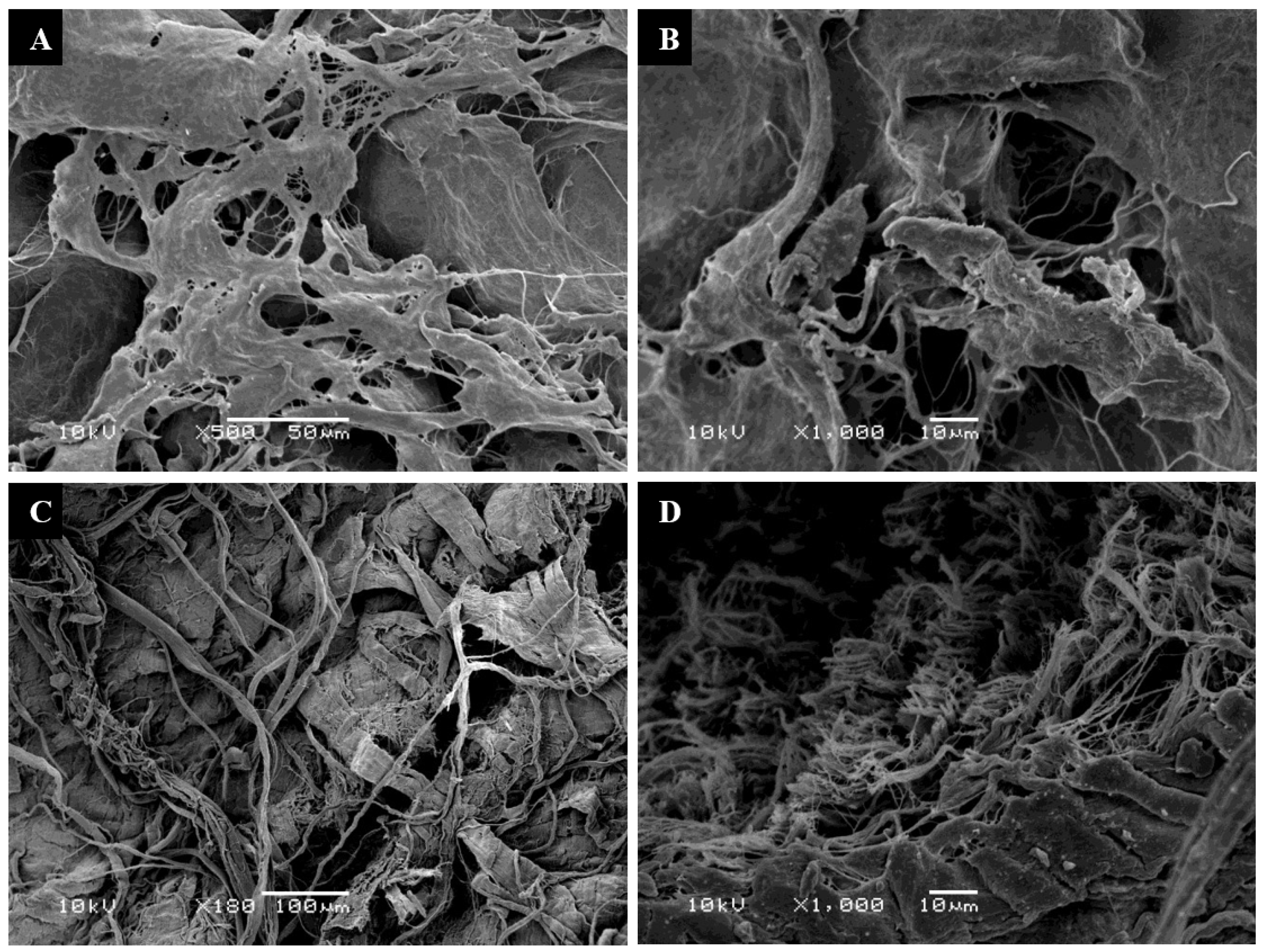
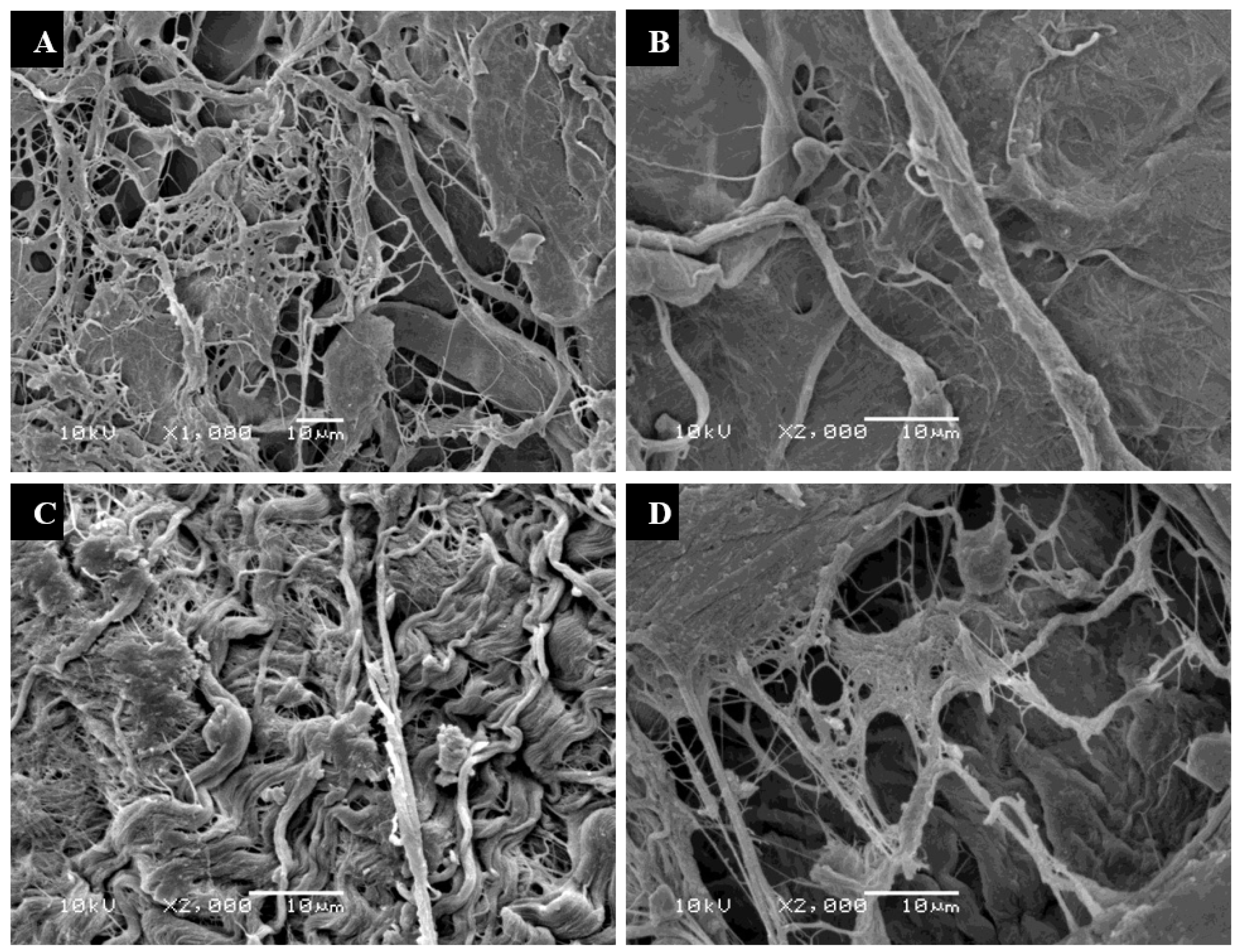
2.7. Evaluation of Cell Attachment/Scanning Electron Microscopy (SEM)
3. Statistical Analysis
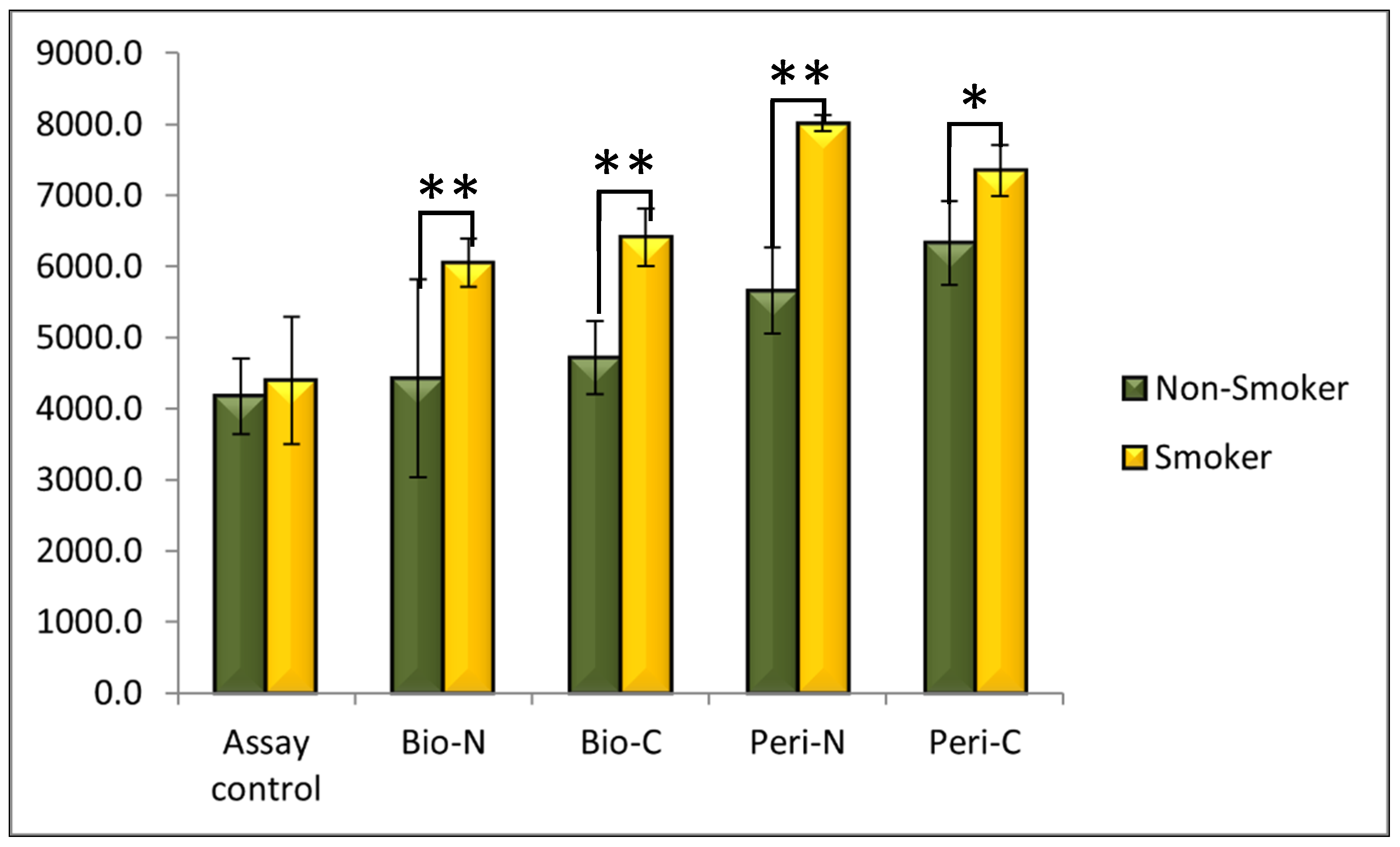
4. Results
5. Discussion
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Page, R.C.; Offenbacher, S.; Schroeder, H.E.; Seymour, G.J.; Kornman, K.S. Advances in the Pathogenesis of Periodontitis: Summary of Developments, Clinical Implications and Future Directions. Periodontology 2000 1997, 14, 216–248. [Google Scholar] [CrossRef] [PubMed]
- Bartold, P.M.; Gronthos, S.; Ivanovski, S.; Fisher, A.; Hutmacher, D.W. Tissue Engineered Periodontal Products. J. Periodontal Res. 2016, 51, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Karring, T.; Nyman, S.; Gottlow, J.; Laurell, L. Development of the Biological Concept of Guided Tissue Regeneration—Animal and Human Studies. Periodontology 2000 1993, 1, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P.; del Aguila, M.A.; DeRouen, T.A.; Bergström, J. A Hidden Periodontitis Epidemic during the 20th Century? Community Dent. Oral Epidemiol. 2003, 31, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S173–S182. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and Grading of Periodontitis: Framework and Proposal of a New Classification and Case Definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef]
- Lallier, T.E.; Moylan, J.T.; Maturin, E. Greater Sensitivity of Oral Fibroblasts to Smoked Versus Smokeless Tobacco. J. Periodontol. 2017, 88, 1356–1365. [Google Scholar] [CrossRef]
- Sehgal, V.; Ruangsawasdi, N.; Kiattavorncharoen, S.; Bencharit, S.; Thanasrisuebwong, P. Occlusive and Proliferative Properties of Different Collagen Membranes—An In Vitro Study. Materials 2023, 16, 1657. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Sculean, A. Current Status of Regenerative Periodontal Treatment. Curr. Oral Health Rep. 2017, 4, 34–43. [Google Scholar] [CrossRef]
- Aprile, P.; Letourneur, D.; Simon-Yarza, T. Membranes for Guided Bone Regeneration: A Road from Bench to Bedside. Adv. Healthc. Mater. 2020, 9, 2000707. [Google Scholar] [CrossRef] [PubMed]
- Rothamel, D.; Schwarz, F.; Sculean, A.; Herten, M.; Scherbaum, W.; Becker, J. Biocompatibility of Various Collagen Membranes in Cultures of Human PDL Fibroblasts and Human Osteoblast-like Cells. Clin. Oral Implants Res. 2004, 15, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Sam, G.; Pillai, B.R.M. Evolution of Barrier Membranes in Periodontal Regeneration—“Are the Third Generation Membranes Really Here?”. J. Clin. Diagn. Res. JCDR 2014, 8, ZE14–ZE17. [Google Scholar] [CrossRef]
- Naidu, K.A. Vitamin C in Human Health and Disease Is Still a Mystery? An Overview. Nutr. J. 2003, 2, 7. [Google Scholar] [CrossRef] [PubMed]
- D’Aniello, C.; Cermola, F.; Patriarca, E.J.; Minchiotti, G. Vitamin C in Stem Cell Biology: Impact on Extracellular Matrix Homeostasis and Epigenetics. Stem Cells Int. 2017, 2017, 8936156. [Google Scholar] [CrossRef] [PubMed]
- San Miguel, S.M.; Opperman, L.A.; Allen, E.P.; Zielinski, J.; Svoboda, K.K.H. Bioactive Antioxidant Mixtures Promote Proliferation and Migration on Human Oral Fibroblasts. Arch. Oral Biol. 2011, 56, 812–822. [Google Scholar] [CrossRef]
- San Miguel, S.M.; Opperman, L.A.; Allen, E.P.; Zielinski, J.; Svoboda, K.K.H. Antioxidants Counteract Nicotine and Promote Migration via RacGTP in Oral Fibroblast Cells. J. Periodontol. 2010, 81, 1675–1690. [Google Scholar] [CrossRef]
- Nishida, M.; Grossi, S.G.; Dunford, R.G.; Ho, A.W.; Trevisan, M.; Genco, R.J. Dietary Vitamin C and the Risk for Periodontal Disease. J. Periodontol. 2000, 71, 1215–1223. [Google Scholar] [CrossRef]
- Takamizawa, S.; Maehata, Y.; Imai, K.; Senoo, H.; Sato, S.; Hata, R.-I. Effects of Ascorbic Acid and Ascorbic Acid 2-Phosphate, a Long-Acting Vitamin C Derivative, on the Proliferation and Differentiation of Human Osteoblast-like Cells. Cell Biol. Int. 2004, 28, 255–265. [Google Scholar] [CrossRef]
- Tatsumi, M.; Yanagita, M.; Yamashita, M.; Hasegawa, S.; Ikegami, K.; Kitamura, M.; Murakami, S. Long-Term Exposure to Cigarette Smoke Influences Characteristics in Human Gingival Fibroblasts. J. Periodontal Res. 2021, 56, 951–963. [Google Scholar] [CrossRef]
- Alyami, R.; Al Jasser, R.; Alshehri, F.A.; Alshibani, N.; Bin Hamdan, S.; Alyami, R.A.; Niazy, A.A. Vitamin C Influences Antioxidative, Anti-Inflammatory and Wound Healing Markers in Smokers’ Gingival Fibroblasts in Vitro. Saudi Dent. J. 2023, 35, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Alyami, R.; Alshehri, F.A.; Al Jasser, R.; Shaheen, S.; Mahmood, A.; Elsafadi, M.A. Vitamin C Stimulates RNA Expression of Human Gingival Fibroblasts Proliferation and Adhesion in Cigarette Smokers: An in Vitro Study. Saudi Dent. J. 2022, 34, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Torshabi, M.; Rezaei Esfahrood, Z.; Jamshidi, M.; Mansuri Torshizi, A.; Sotoudeh, S. Efficacy of Vitamins E and C for Reversing the Cytotoxic Effects of Nicotine and Cotinine. Eur. J. Oral Sci. 2017, 125, 426–437. [Google Scholar] [CrossRef] [PubMed]
- Akbari, A.; Jelodar, G.; Nazifi, S.; Sajedianfard, J. An Overview of the Characteristics and Function of Vitamin C in Various Tissues: Relying on Its Antioxidant Function. Zahedan J. Res. Med. Sci. 2016, 18, e4037. [Google Scholar] [CrossRef]
- Kaldahl, W.B.; Johnson, G.K.; Patil, K.D.; Kalkwarf, K.L. Levels of Cigarette Consumption and Response to Periodontal Therapy. J. Periodontol. 1996, 67, 675–681. [Google Scholar] [CrossRef]
- Hakeem, L.; Al-Kindi, M.; AlMuraikhi, N.; BinHamdan, S.; Al-Zahrani, A. Evaluation of the Regenerative Potential of Decellularized Skeletal Muscle Seeded with Mesenchymal Stromal Cells in Critical-Sized Bone Defect of Rat Models. Saudi Dent. J. 2021, 33, 248–255. [Google Scholar] [CrossRef]
- McGuire, M.K.; Scheyer, E.T.; Nevins, M.L.; Neiva, R.; Cochran, D.L.; Mellonig, J.T.; Giannobile, W.V.; Bates, D. Living Cellular Construct for Increasing the Width of Keratinized Gingiva: Results from a Randomized, within-Patient, Controlled Trial. J. Periodontol. 2011, 82, 1414–1423. [Google Scholar] [CrossRef]
- Minabe, M.; Kodama, T.; Kogou, T.; Tamura, T.; Hori, T.; Watanabe, Y.; Miyata, T. Different Cross-Linked Types of Collagen Implanted in Rat Palatal Gingiva. J. Periodontol. 1989, 60, 35–43. [Google Scholar] [CrossRef]
- Capella-Monsonís, H.; Zeugolis, D.I. Decellularized Xenografts in Regenerative Medicine: From Processing to Clinical Application. Xenotransplantation 2021, 28, e12683. [Google Scholar] [CrossRef]
- Wong, L.S.; Martins-Green, M. Firsthand Cigarette Smoke Alters Fibroblast Migration and Survival: Implications for Impaired Healing. Wound Repair Regen. Off. Publ. Wound Heal. Soc. Eur. Tissue Repair Soc. 2004, 12, 471–484. [Google Scholar] [CrossRef]
- Sawhney, A.; Ralli, M.; Dhar, S.; Gupta, B.; Ghodke, S.S.; Purao, S. Role of Smoking and Its Impact on Periodontium. J. Int. Clin. Dent. Res. Organ. 2021, 13, 3–9. [Google Scholar] [CrossRef]
- Tipton, D.A.; Dabbous, M.K.H. Effects of Nicotine on Proliferation and Extracellular Matrix Production of Human Gingival Fibroblasts In Vitro. J. Periodontol. 1995, 66, 1056–1064. [Google Scholar] [CrossRef]
- Møller, P.; Viscovich, M.; Lykkesfeldt, J.; Loft, S.; Jensen, A.; Poulsen, H.E. Vitamin C Supplementation Decreases Oxidative DNA Damage in Mononuclear Blood Cells of Smokers. Eur. J. Nutr. 2004, 43, 267–274. [Google Scholar] [CrossRef]
- Falsafi, P.; Nasrabadi, E.T.; Nasrabadi, H.T.; Khiyavi, R.K.; Eslami, H. Comparison of Total Antioxidant Capacity and Vitamin C in Smokers and Non-Smokers. Biomed. Pharmacol. J. 2016, 9, 299–304. [Google Scholar] [CrossRef]
- Talebi Ardakani, M.R.; Hajizadeh, F.; Yadegari, Z. Comparison of Attachment and Proliferation of Human Gingival Fibroblasts on Different Collagen Membranes. Ann. Maxillofac. Surg. 2018, 8, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Rampersad, S.N. Multiple Applications of Alamar Blue as an Indicator of Metabolic Function and Cellular Health in Cell Viability Bioassays. Sensors 2012, 12, 12347–12360. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Smoker (N) Groups | Smoker (S) Groups |
|---|---|
| BioMend membrane without vitamin C (Bio-N-N) | BioMend membrane without vitamin C (Bio-S-N) |
| BioMend membrane with vitamin C (Bio-N-C) | BioMend membrane with vitamin C (Bio-S-C) |
| Pericardium membrane without vitamin C (Peri-N-N) | Pericardium membrane without vitamin C (Peri-S-N) |
| Pericardium membrane with vitamin C (Peri-N-C) | Pericardium membrane with vitamin C (Peri-S-C) |
| Group | n | Mean ± (SD) | p-Value * | |
|---|---|---|---|---|
| Non-smokers | Assay control | 6 | 4173.5 ± (532.8) | - |
| Bio-N-N | 6 | 4422.5 ± (1394.1) | 0.917 | |
| Bio-N-C | 6 | 4719.8 ± (515.6) | ||
| Peri-N-N | 6 | 5659.0 ± (600.4) | 0.028 | |
| Peri-N-C | 6 | 6329.8 ± (593.0) | ||
| Smokers | Assay control | 6 | 4399.5 ± (896.4) | - |
| Bio-S-N | 6 | 6055.2 ± (339.6) | 0.028 | |
| Bio-S-C | 6 | 6411.0 ± (401.1) | ||
| Peri-S-N | 6 | 8012.8 ± (112.9) | 0.028 | |
| Peri-S-C | 6 | 7349.0 ± (360.7) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshehri, F.A. Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study. Appl. Sci. 2023, 13, 10828. https://doi.org/10.3390/app131910828
Alshehri FA. Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study. Applied Sciences. 2023; 13(19):10828. https://doi.org/10.3390/app131910828
Chicago/Turabian StyleAlshehri, Fahad Ali. 2023. "Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study" Applied Sciences 13, no. 19: 10828. https://doi.org/10.3390/app131910828
APA StyleAlshehri, F. A. (2023). Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study. Applied Sciences, 13(19), 10828. https://doi.org/10.3390/app131910828