
3D-Printed Metal Surgical Guide for Endodontic Microsurgery (a Proof of Concept)


Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
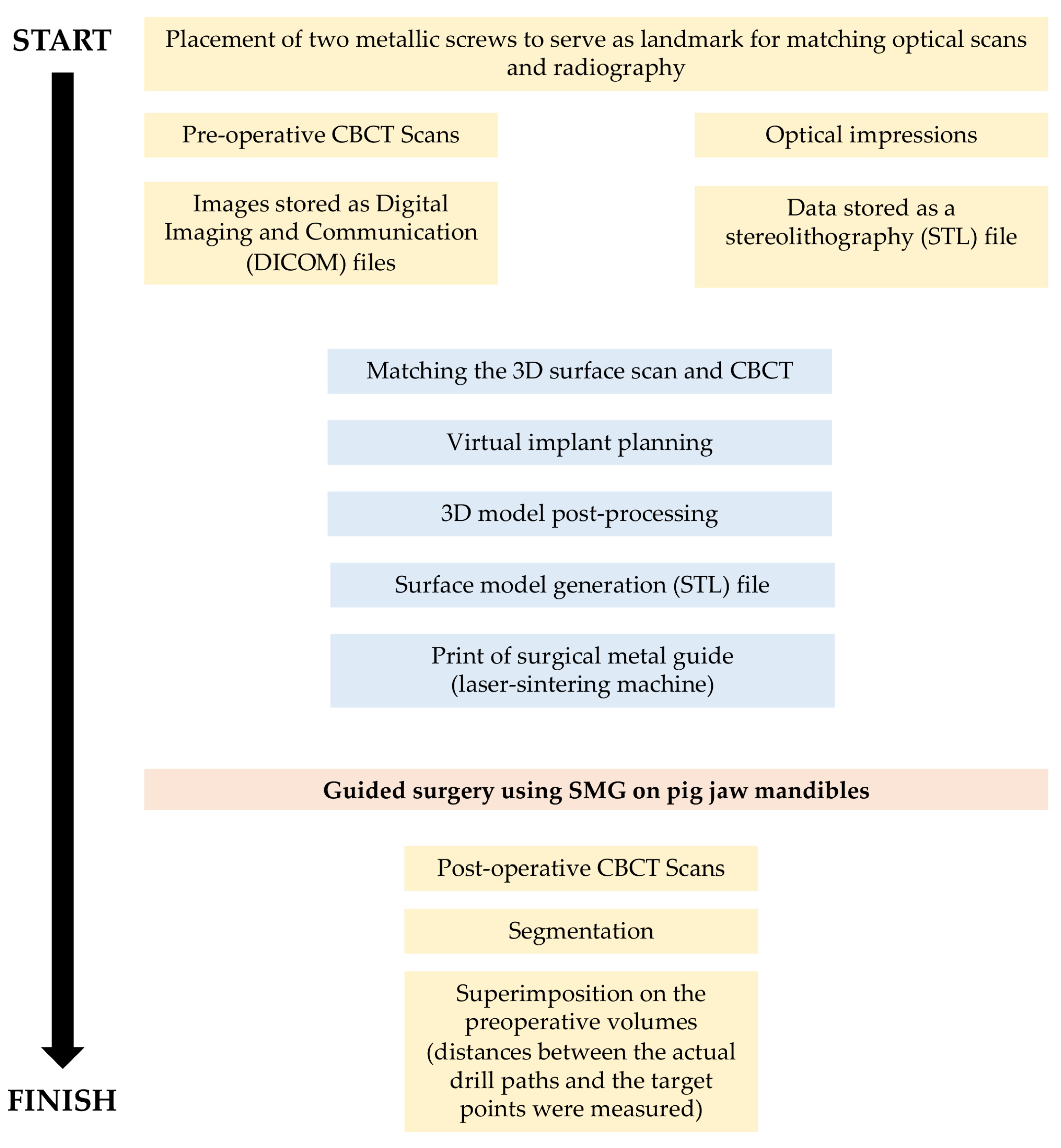
2.1. Study Design
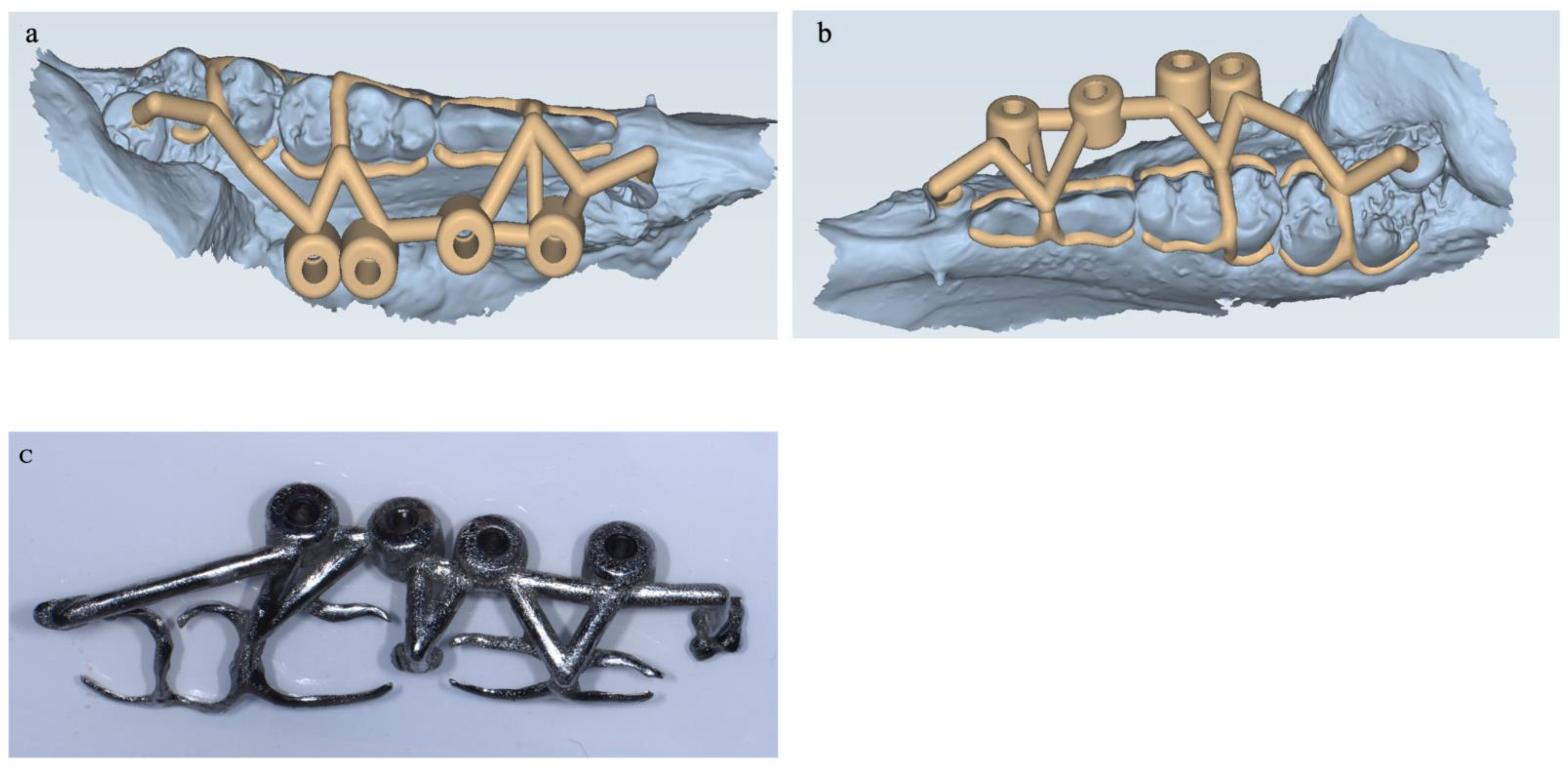
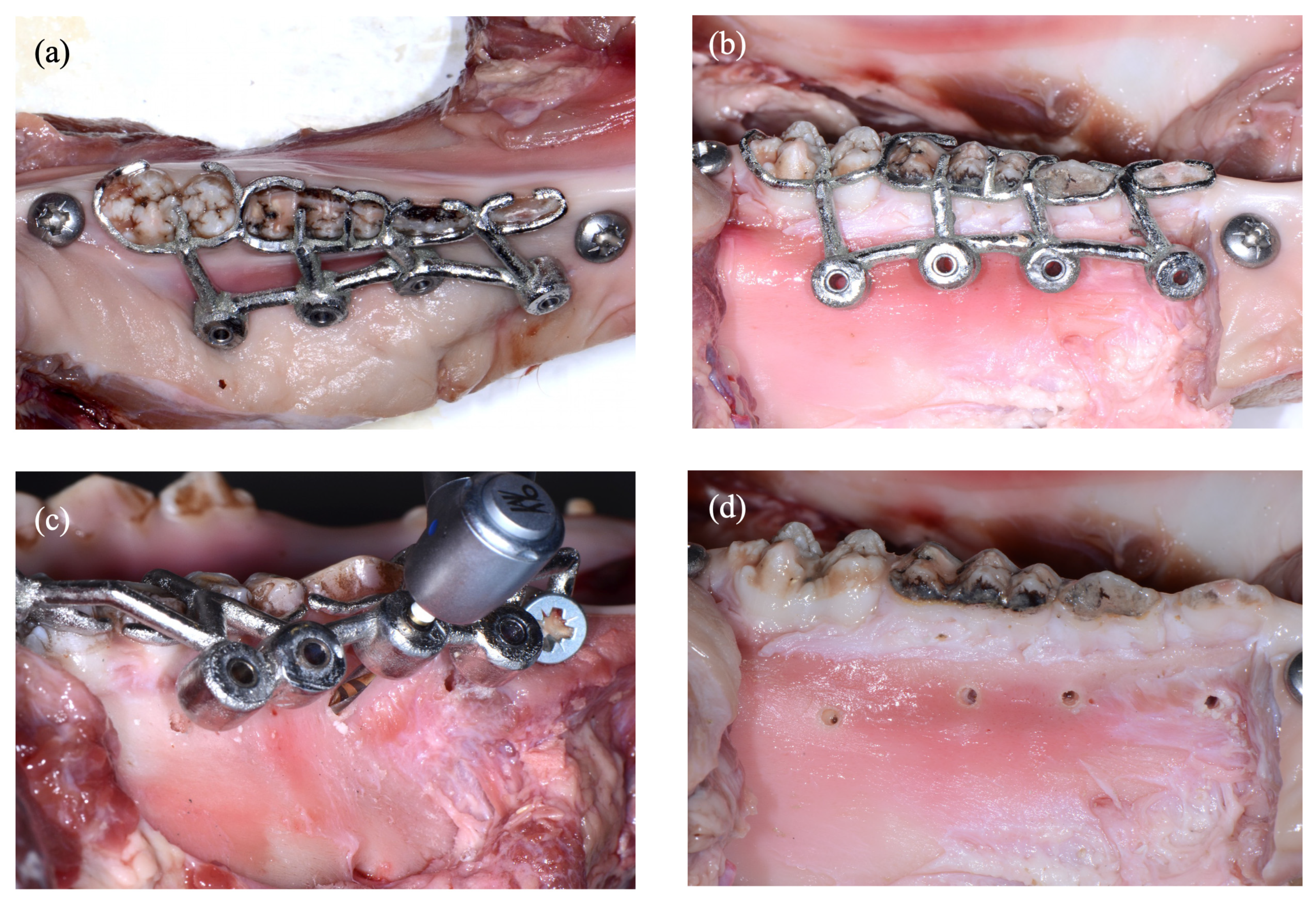
2.2. Experimental Procedure
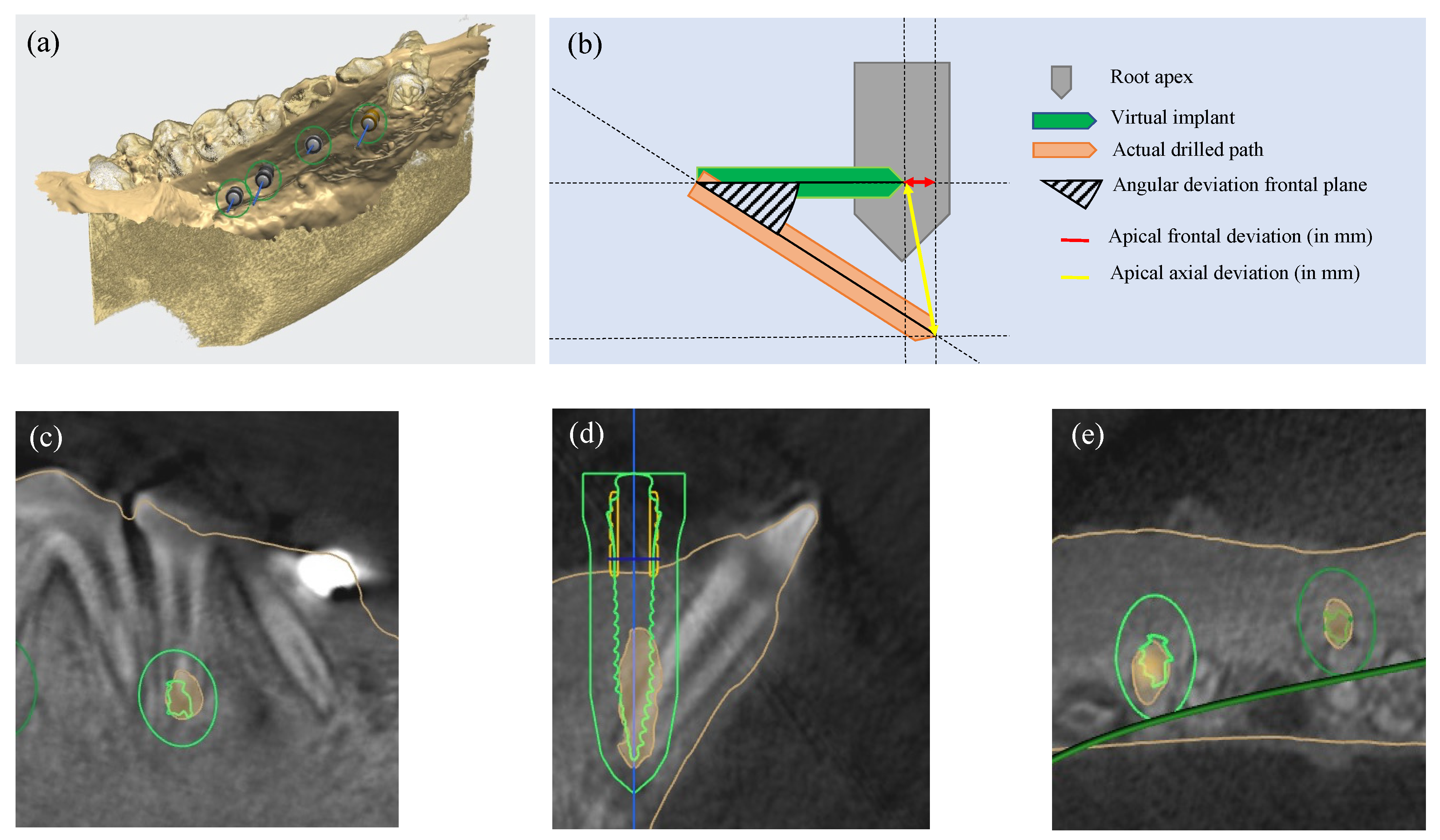
2.3. Measurement Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahn, S.Y.; Kim, N.H.; Kim, S.; Karabucak, B.; Kim, E. Computer-Aided Design/Computer-Aided Manufacturing–Guided Endodontic Surgery: Guided Osteotomy and Apex Localization in a Mandibular Molar with a Thick Buccal Bone Plate. J. Endod. 2018, 44, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Hajihassani, N.; Ramezani, M.; Tofangchiha, M.; Bayereh, F.; Ranjbaran, M.; Zanza, A.; Reda, R.; Testarelli, L. Pattern of Endodontic Lesions of Maxillary and Mandibular Posterior Teeth: A Cone-Beam Computed Tomography Study. J. Imaging 2022, 8, 290. [Google Scholar] [CrossRef] [PubMed]
- Reda, R.; Zanza, A.; Bhandi, S.; Biase, A.D.; Testarelli, L.; Miccoli, G. Surgical-Anatomical Evaluation of Mandibular Premolars by CBCT among the Italian Population. Dent. Med. Probl. 2022, 59, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Arx, T.V.; Hänni, S.; von Arx, T.; Hänni, S.; Jensen, S.S. Correlation of Bone Defect Dimensions with Healing Outcome One Year after Apical Surgery. J. Endod. 2007, 33, 1044–1048. [Google Scholar] [CrossRef]
- Pinsky, H.M.; Champleboux, G.; Sarment, D.P. Periapical Surgery Using CAD/CAM Guidance: Preclinical Results. J. Endod. 2007, 33, 148–151. [Google Scholar] [CrossRef]
- Sarment, D.P.; Sukovic, P.; Clinthorne, N. Accuracy of Implant Placement with a Stereolithographic Surgical Guide. Int. J. Oral Maxillofac. Implant. 2003, 18, 571–577. [Google Scholar]
- Younes, F.; Cosyn, J.; De Bruyckere, T.; Cleymaet, R.; Bouckaert, E.; Eghbali, A. A Randomized Controlled Study on the Accuracy of Free-Handed, Pilot-Drill Guided and Fully Guided Implant Surgery in Partially Edentulous Patients. J. Clin. Periodontol. 2018, 45, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Kernen, F.; Benic, G.I.; Payer, M.; Schär, A.; Müller-Gerbl, M.; Filippi, A.; Kühl, S. Accuracy of Three-Dimensional Printed Templates for Guided Implant Placement Based on Matching a Surface Scan with CBCT. Clin. Implant Dent. Relat. Res. 2016, 18, 762–768. [Google Scholar] [CrossRef]
- Schneider, D.; Marquardt, P.; Zwahlen, M.; Jung, R.E. A Systematic Review on the Accuracy and the Clinical Outcome of Computer-Guided Template-Based Implant Dentistry. Clin. Oral Implants Res. 2009, 20, 73–86. [Google Scholar] [CrossRef] [Green Version]
- Dawood, A.; Marti, B.M.; Sauret-Jackson, V.; Darwood, A. 3D Printing in Dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef]
- van der Meer, W.J.; Vissink, A.; Ng, Y.L.; Gulabivala, K. 3D Computer Aided Treatment Planning in Endodontics. J. Dent. 2016, 45, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, G.; Nitsch, S.; Edelmayer, M.; Janjić, K.; Müller, A.S.; Agis, H. 3D Printing—Encompassing the Facets of Dentistry. Front. Bioeng. Biotechnol. 2018, 6, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, S.; Zhao, S.; Wang, W.; Jiang, Q.; Yang, X. A Novel Method for Periapical Microsurgery with the Aid of 3D Technology: A Case Report. BMC Oral. Health 2018, 18, 85. [Google Scholar] [CrossRef] [Green Version]
- Antal, M.; Nagy, E.; Braunitzer, G.; Fráter, M.; Piffkó, J. Accuracy and Clinical Safety of Guided Root End Resection with a Trephine: A Case Series. Head Face Med. 2019, 15, 30. [Google Scholar] [CrossRef] [Green Version]
- Giacomino, C.M.; Ray, J.J.; Wealleans, J.A. Targeted Endodontic Microsurgery: A Novel Approach to Anatomically Challenging Scenarios Using 3-Dimensional–Printed Guides and Trephine Burs—A Report of 3 Cases. J. Endod. 2018, 44, 671–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ackerman, S.; Aguilera, F.C.; Buie, J.M.; Glickman, G.N.; Umorin, M.; Wang, Q.; Jalali, P. Accuracy of 3-Dimensional—Printed Endodontic Surgical Guide: A Human Cadaver Study. J. Endod. 2019, 45, 615–618. [Google Scholar] [CrossRef]
- Mouhyi, J.; Salama, M.A.; Mangano, F.G.; Mangano, C.; Margiani, B.; Admakin, O. A Novel Guided Surgery System with a Sleeveless Open Frame Structure: A Retrospective Clinical Study on 38 Partially Edentulous Patients with 1 Year of Follow-Up. BMC Oral Health 2019, 19, 253. [Google Scholar] [CrossRef] [Green Version]
- Tallarico, M.; Martinolli, M.; Kim, Y.; Cocchi, F.; Meloni, S.M.; Alushi, A.; Xhanari, E. Accuracy of Computer-Assisted Template-Based Implant Placement Using Two Different Surgical Templates Designed with or without Metallic Sleeves: A Randomized Controlled Trial. Dent. J. 2019, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Koop, R.; Vercruyssen, M.; Vermeulen, K.; Quirynen, M. Tolerance within the Sleeve Inserts of Different Surgical Guides for Guided Implant Surgery. Clin. Oral Implants Res. 2013, 24, 630–634. [Google Scholar] [CrossRef]
- Anderson, J.; Wealleans, J.; Ray, J. Endodontic Applications of 3D Printing. Int. Endod. J. 2018, 51, 1005–1018. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.D.O.; Borges, A.L.S.; Araújo, R.M.; da Silva, J.M.F.; Bottino, M.A.; Kleverlaan, C.J.; de Jager, N. Effect of Different Materials and Undercut on the Removal Force and Stress Distribution in Circumferential Clasps during Direct Retainer Action in Removable Partial Dentures. Dent. Mater. 2020, 36, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Kwon, K.-R. A CAD-CAM Device for Preparing Guide Planes for Removable Partial Dentures: A Dental Technique. J. Prosthet. Dent. 2019, 122, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kratchman, S. Modern Endodontic Surgery Concepts and Practice: A Review. J. Endod. 2006, 32, 601–623. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, A.; Kero, T.; Gillot, L.; Cannas, B.; Fäldt, J.; Söderberg, R.; Näsström, K. Accuracy of CAD/CAM-Guided Surgical Template Implant Surgery on Human Cadavers: Part I. J. Prosthet. Dent. 2010, 103, 334–342. [Google Scholar] [CrossRef]
- Behneke, A.; Burwinkel, M.; Behneke, N. Factors Influencing Transfer Accuracy of Cone Beam CT-Derived Template-Based Implant Placement. Clin. Oral Implant. Res. 2012, 23, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Schelbert, T.; Gander, T.; Blumer, M.; Jung, R.; Rücker, M.; Rostetter, C. Accuracy of Computer-Guided Template-Based Implant Surgery: A Computed Tomography–Based Clinical Follow-up Study. Implant. Dent. 2019, 28, 556–563. [Google Scholar] [CrossRef]
- Widmann, G.; Bale, R.J. Accuracy in Computer-Aided Implant Surgery—A Review. Int. J. Oral Maxillofac. Implant. 2006, 21, 305–313. [Google Scholar]
- Fan, Y.; Glickman, G.N.; Umorin, M.; Nair, M.K.; Jalali, P. A Novel Prefabricated Grid for Guided Endodontic Microsurgery. J. Endod. 2019, 45, 606–610. [Google Scholar] [CrossRef]
- Moreno-Rabié, C.; Torres, A.; Lambrechts, P.; Jacobs, R. Clinical Applications, Accuracy and Limitations of Guided Endodontics: A Systematic Review. Int. Endod. J. 2020, 53, 214–231. [Google Scholar] [CrossRef] [Green Version]
- Hay, S.I.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; Aboyans, V.; et al. Global, Regional, and National Disability-Adjusted Life-Years (DALYs) for 333 Diseases and Injuries and Healthy Life Expectancy (HALE) for 195 Countries and Territories, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef] [Green Version]
- Apostolakis, D.; Kourakis, G. CAD/CAM Implant Surgical Guides: Maximum Errors in Implant Positioning Attributable to the Properties of the Metal Sleeve/Osteotomy Drill Combination. Int. J. Implant Dent. 2018, 4, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.C.; Park, J.M.; Shim, J.S.; Kim, J.H.; Kim, J.E.; Kim, J.H. Assessment of Metal Sleeve-Free 3D-Printed Implant Surgical Guides. Dent. Mater. 2019, 35, 468–476. [Google Scholar] [CrossRef]
- Dahiya, K.; Kumar, N.; Bajaj, P.; Sharma, A.; Sikka, R.; Dahiya, S. Qualitative Assessment of Reliability of Cone-Beam Computed Tomography in Evaluating Bone Density at Posterior Mandibular Implant Site. J. Contemp. Dent. Pract. 2018, 19, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.M.; Hunter, S.A.; Gayton, J.C.; Boivin, G.P.; Prayson, M.J. Repeated Freeze-Thaw Cycles Do Not Alter the Biomechanical Properties of Fibular Allograft Bone. Clin. Orthop. Relat. Res. 2012, 470, 937–943. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Apical Deviation | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Min | Max | Median | SD | 95% CI LL | 95% CI UL | p | ||
| SMG 1 | 4 | 2.38 | 1.55 | 3.11 | 2.43 | 0.77 | 1.55 | 3.11 | 0.0087 |
| SMG 2 | 4 | 4.90 | 2.67 | 6.38 | 5.28 | 1.66 | 2.67 | 6.38 | 0.0097 |
| SMG 3 | 4 | 4.24 | 2.46 | 6.58 | 3.95 | 1.72 | 2.46 | 6.58 | 0.016 |
| SMG 4 | 4 | 4.85 | 3.8 | 5.67 | 4.97 | 0.92 | 3.08 | 5.67 | 0.0019 |
| SMG 5 | 4 | 3.75 | 2.65 | 5.87 | 3.24 | 1.51 | 2.65 | 5.87 | 0.0156 |
| SMG 6 | 4 | 1.25 | 0.77 | 2.56 | 0.83 | 0.87 | 0.77 | 2.56 | 0.0646 |
| SMG 7 | 3 | 1.99 | 1.2 | 3.14 | 1.6 | 1.01 | 1.23 | 3.14 | 0.076 |
| SMG 8 | 2 | 1.86 | 1.24 | 2.47 | 1.86 | 0.86 | 1.24 | 2.47 | 0.2025 |
| Total | 29 | 3.28 | 0.77 | 6.58 | 2.97 | 1.76 | 2.61 | 3.95 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabezon, C.; Aubeux, D.; Pérez, F.; Gaudin, A. 3D-Printed Metal Surgical Guide for Endodontic Microsurgery (a Proof of Concept). Appl. Sci. 2023, 13, 1031. https://doi.org/10.3390/app13021031
Cabezon C, Aubeux D, Pérez F, Gaudin A. 3D-Printed Metal Surgical Guide for Endodontic Microsurgery (a Proof of Concept). Applied Sciences. 2023; 13(2):1031. https://doi.org/10.3390/app13021031
Chicago/Turabian StyleCabezon, Camille, Davy Aubeux, Fabienne Pérez, and Alexis Gaudin. 2023. "3D-Printed Metal Surgical Guide for Endodontic Microsurgery (a Proof of Concept)" Applied Sciences 13, no. 2: 1031. https://doi.org/10.3390/app13021031
APA StyleCabezon, C., Aubeux, D., Pérez, F., & Gaudin, A. (2023). 3D-Printed Metal Surgical Guide for Endodontic Microsurgery (a Proof of Concept). Applied Sciences, 13(2), 1031. https://doi.org/10.3390/app13021031