
Ergonomic Sports Mouthguards: A Narrative Literature Review and Future Perspectives

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Narrative Literature Review Search Strategy
2.1. Mouthguards
2.2. Characteristics and Mechanisms of Protection
2.3. Classification
2.3.1. Stock Mouthguards (Pre-Fabricated)
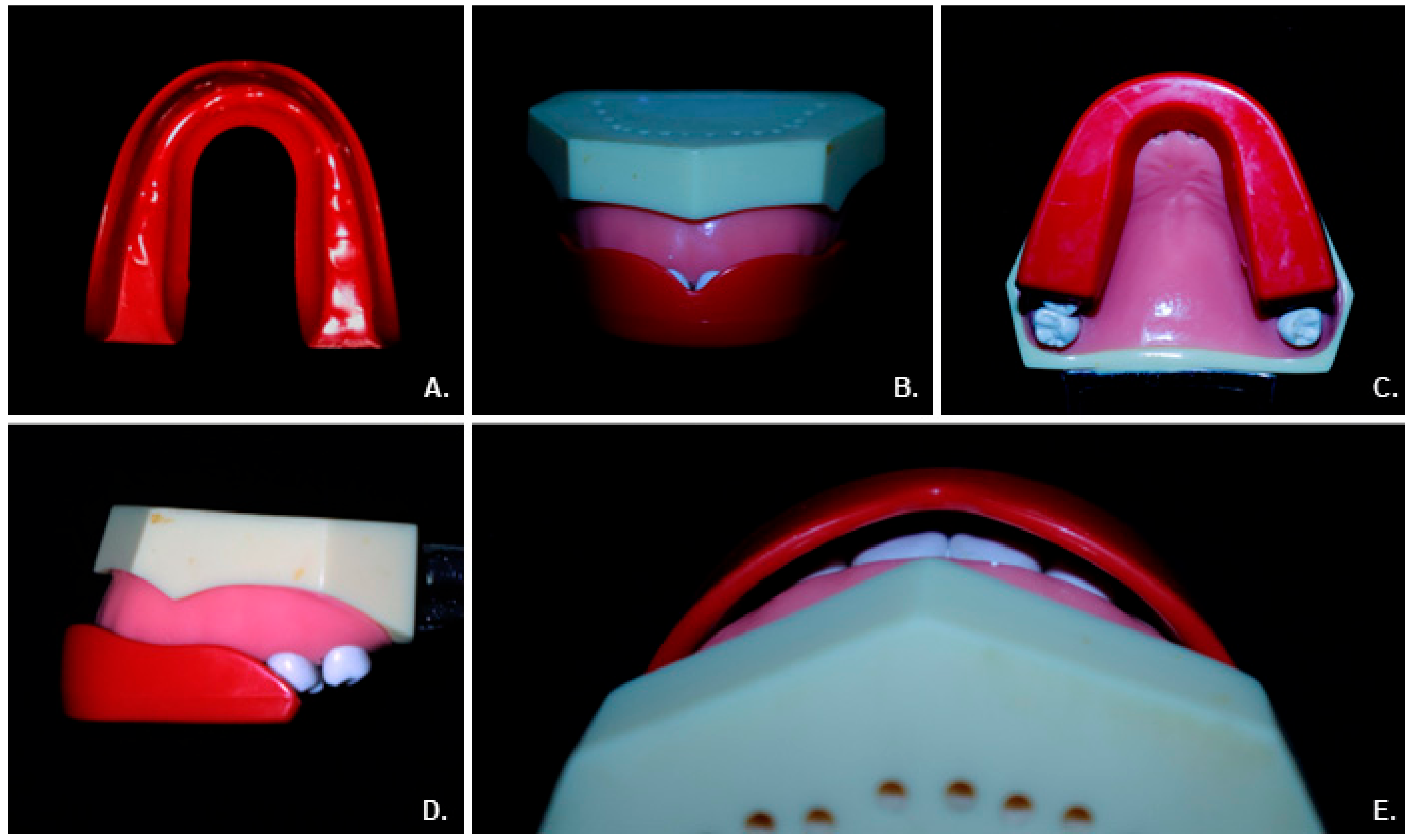
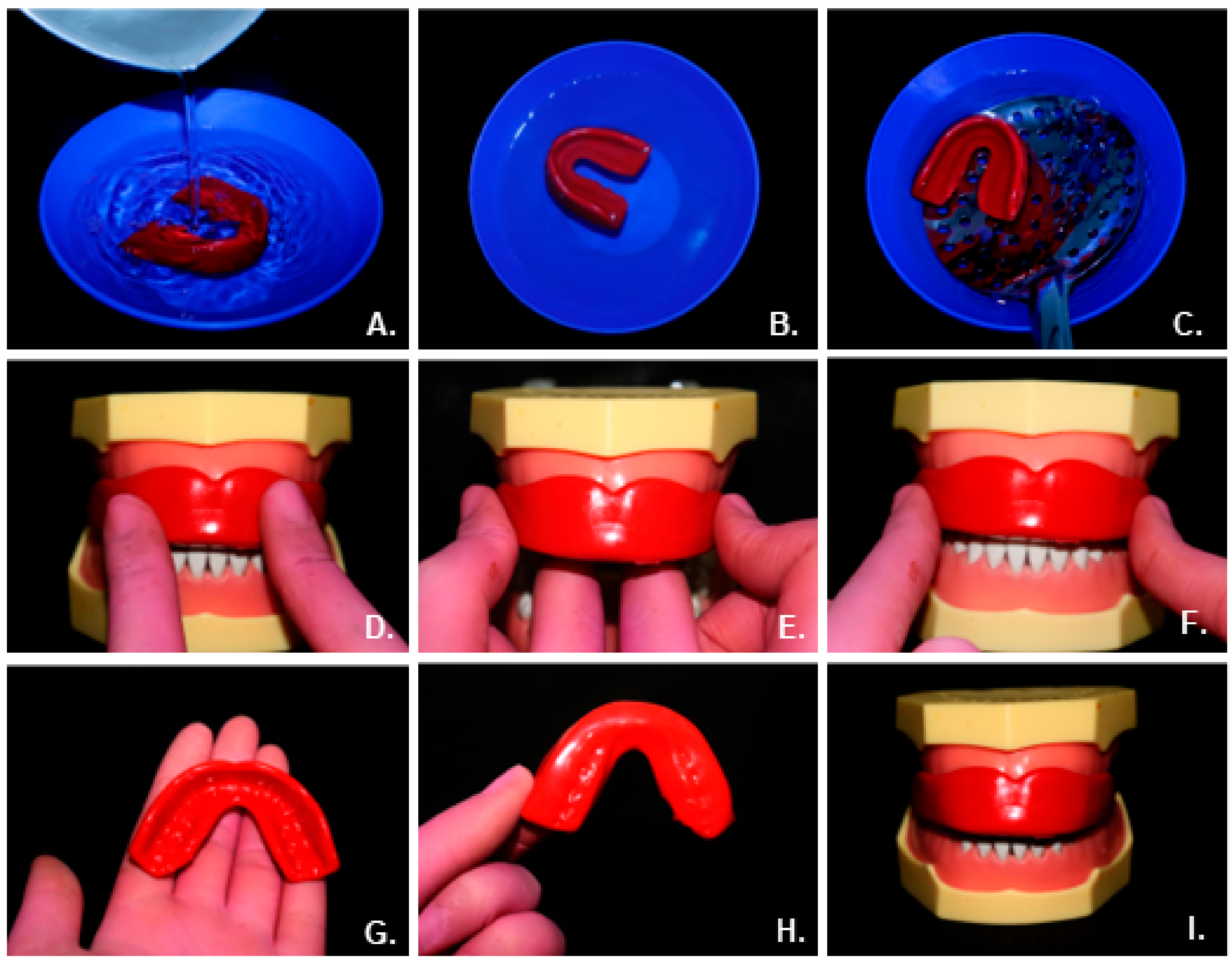
2.3.2. Mouth-Formed Mouthguards (Boil and Bite)
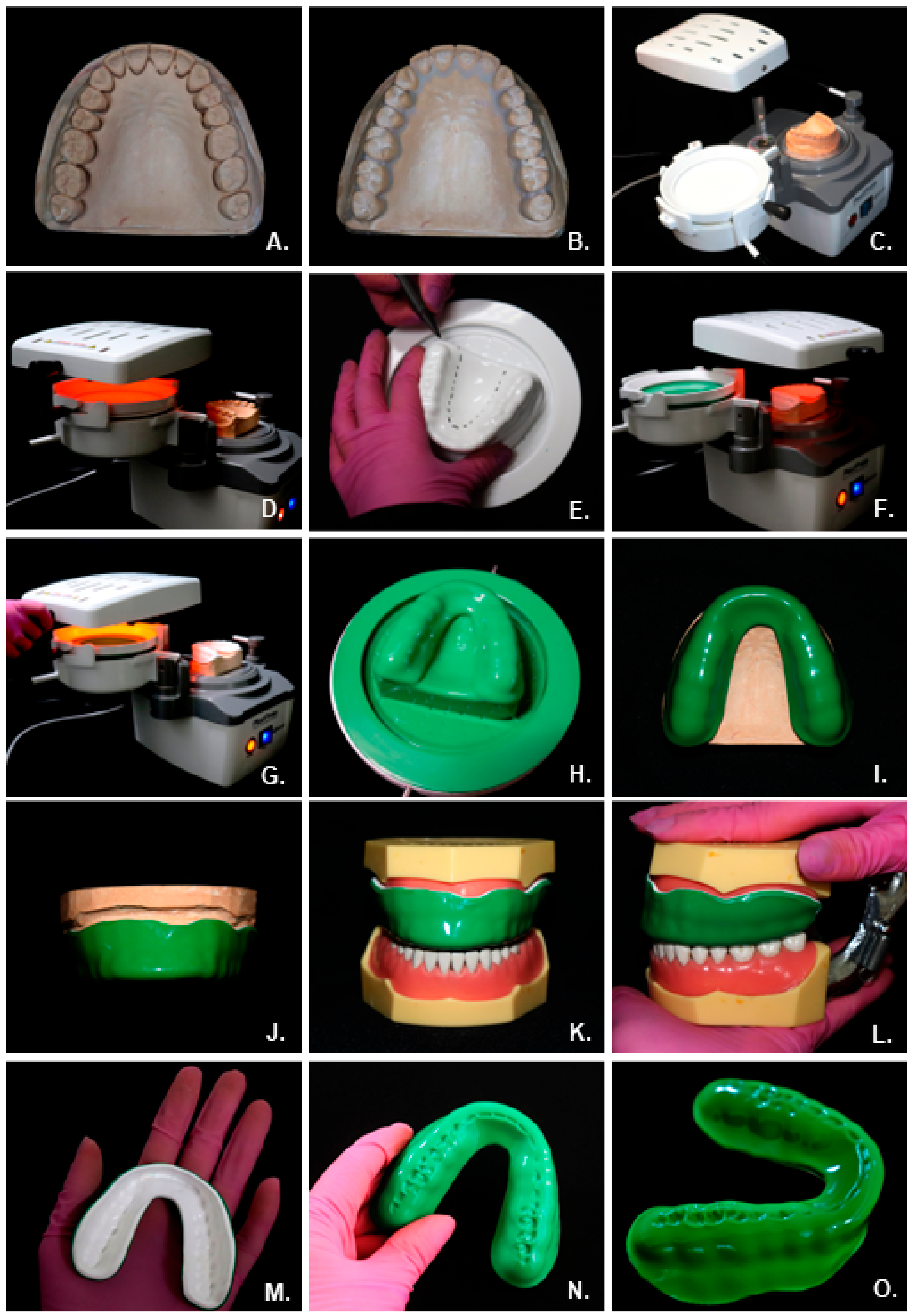
2.3.3. Ergonomic Custom-Made Mouthguards
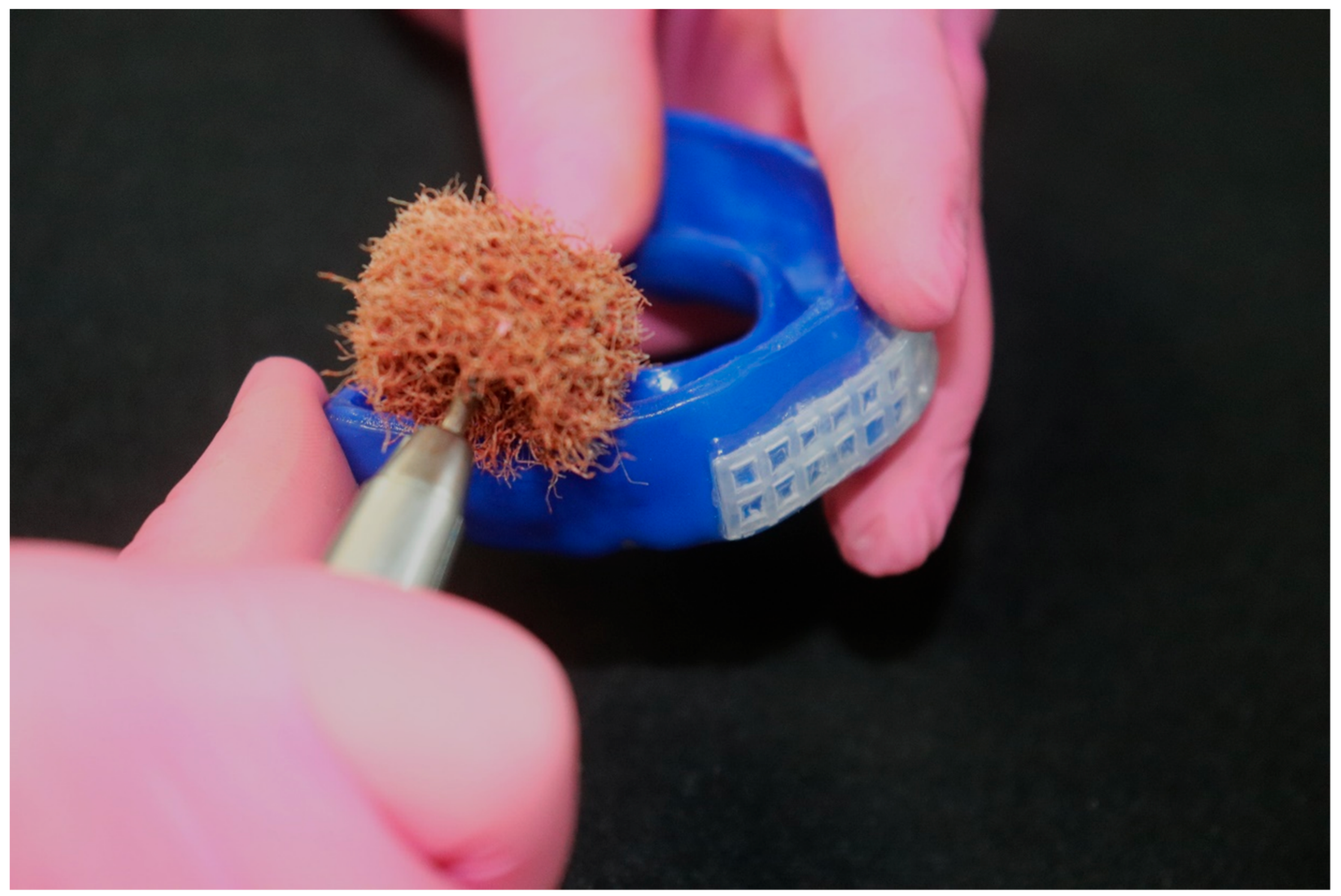
2.4. Reinforcements in Mouthguards
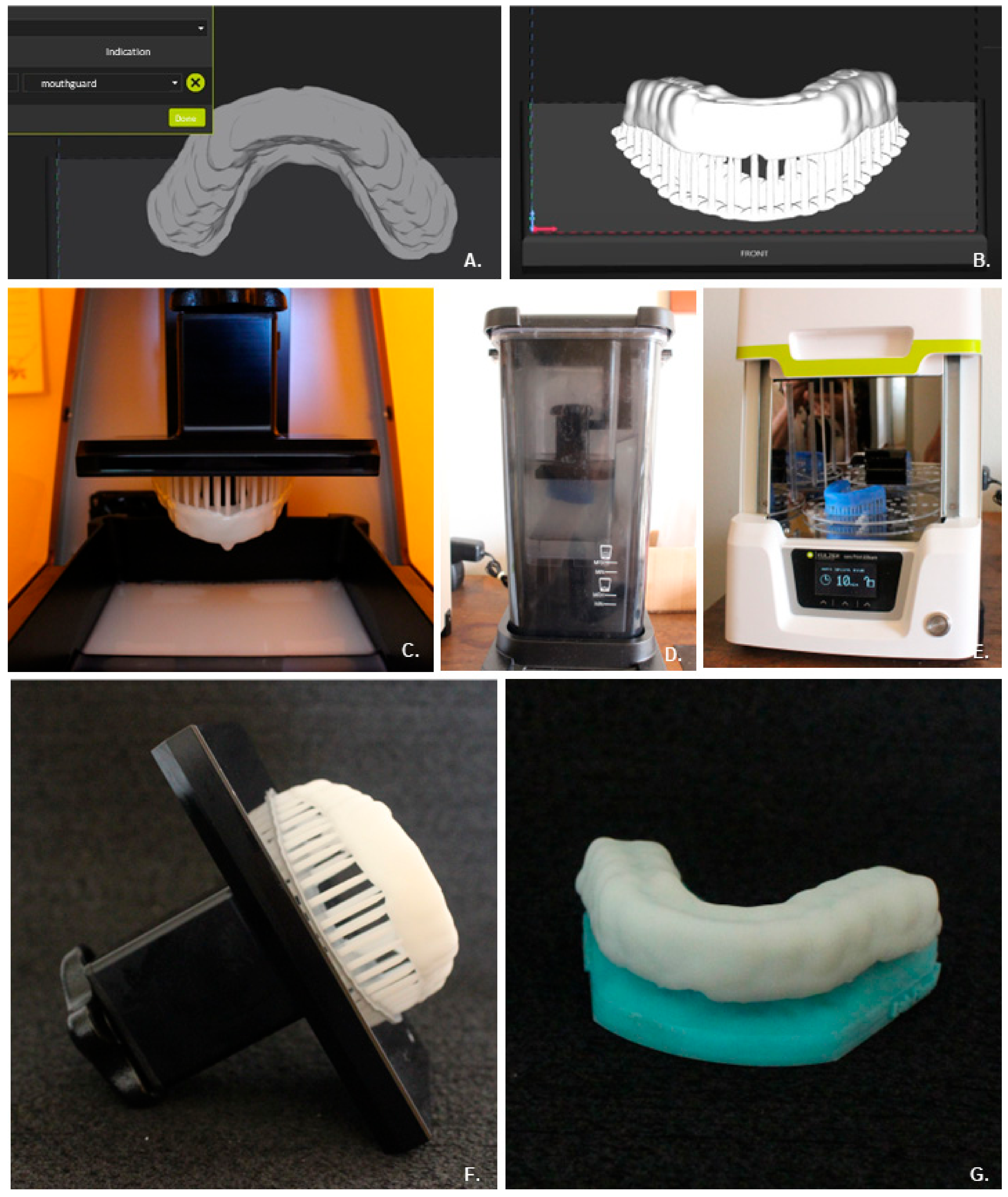
2.5. Additive Manufacturing
3. Discussion
4. Final Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saini, R. Sports Dentistry. Natl. J. Maxillofac. Surg. 2011, 2, 129. [Google Scholar] [CrossRef]
- Knapik, J.J.; Marshall, S.W.; Lee, R.B.; Darakjy, S.S.; Jones, S.B.; Mitchener, T.A.; Dela Cruz, G.G.; Jones, B.H. Mouthguards in sports activities history, physical properties, and injury prevention effectiveness. Sports Med. 2007, 37, 117–144. [Google Scholar] [CrossRef] [PubMed]
- Lam, R. Epidemiology and outcomes of traumatic dental injuries: A review of the literature. Aust. Dent. J. 2016, 61, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Piccininni, P.; Clough, A.; Padilla, R.; Piccininni, G. Dental and orofacial injuries. Clin. Sports Med. 2017, 36, 369–405. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, L.M.; Neto, J.C.; Lima, T.F.; Magno, M.B.; Santiago, B.M.; Cavalcanti, Y.W.; de Almeida, L.D. The use of mouthguards and prevalence of dento-alveolar trauma among athletes: A systematic review and meta-analysis. Dent. Traumatol. 2019, 35, 54–72. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.O.; de Carvalho, P.C.; Gonçalves, P.H.P.; Borges, A.L.S.; Paes-Junior, T.J. Does silica–nylon mesh improves the biomechanical response of custom-made mouthguards? Sport Sci. Health 2020, 16, 75–84. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.O.; Bottino, M.A.; Kleverlaan, C.J.; Koolstra, J.H. Mouthguard use and TMJ injury prevention with different occlusions: A three-dimensional finite element analysis. Dent. Traumatol. 2020, 36, 662–669. [Google Scholar] [CrossRef]
- Sousa, A.M.; Pinho, A.C.; Messias, A.; Piedade, A.P. Present status in polymeric mouthguards. A future area for additive manufacturing? Polymers 2020, 12, 1490. [Google Scholar] [CrossRef]
- Tulunoglu, I.; Özbek, M. Oral trauma, mouthguard awareness, and use in two contact sports in Turkey. Dent. Traumatol. 2006, 22, 242–246. [Google Scholar] [CrossRef]
- Emerich, K.; Kaczmarek, J. First aid for dental trauma caused by sports activities: State of knowledge, treatment and prevention. Sports Med. 2010, 40, 361–366. [Google Scholar] [CrossRef]
- Ahmed, I.; Fine, P. ‘Injury prevention versus performance’: Has the time come to mandate the use of mouthguards in all contact sports? BMJ Open Sport Exerc. Med. 2021, 7, e000828. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Ishigami, K.; Handa, J.; Naitoh, K.; Kurokawa, K.; Shibusawa, M.; Nakajima, K.; Kawamura, S. Does hard insertion and space improve shock absorption ability of mouthguard? Dent. Traumatol. 2006, 22, 77–82. [Google Scholar] [CrossRef]
- Bulsara, Y.R.; Matthew, I.R. Forces transmitted through a laminated mouthguard material with a Sorbothane insert. Dent. Traumatol. 1998, 14, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, S.H.; Setzer, F.C.; Gondim, E., Jr.; Caldeira, C.L. Impact absorption and force dissipation of protective mouthguards with or without titanium reinforcement. J. Am. Dent. Assoc. 2014, 145, 956–959. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, Y.; Nakajima, K.; Saitou, M.; Katano, K.; Kanemitsu, A.; Takeda, T.; Fukuda, K. The effect of light-cured resin with a glass fiber net as an intermediate material for Hard & Space mouthguard. Dent. Traumatol. 2020, 36, 654–661. [Google Scholar] [CrossRef]
- Kumamoto, D.P. Sports dentistry. Compendium 1993, 14, 492–502. [Google Scholar]
- Frontera, R.R.; Zanin, L.; Ambrosano, G.M.B.; Flório, F.M. Orofacial trauma in Brazilian basketball players and level of information concerning trauma and mouthguards. Dent. Traumatol. 2011, 27, 208–216. [Google Scholar] [CrossRef]
- Bhalla, A.; Grewal, N.; Tiwari, U.; Mishra, V.; Mehla, N.S.; Raviprakash, S.; Kapur, P. Shock absorption ability of laminate mouth guards in two different malocclusions using fiber Bragg grating (FBG) sensor. Dent. Traumatol. 2013, 29, 218–225. [Google Scholar] [CrossRef]
- Ozawa, T.; Takeda, T.; Ishigami, K.; Narimatsu, K.; Hasegawa, K.; Nakajima, K.; Noh, K. Shock absorption ability of mouthguard against forceful, traumatic mandibular closure. Dent. Traumatol. 2014, 30, 204–210. [Google Scholar] [CrossRef]
- Tuna, E.B.; Ozel, E. Factors affecting sports-related orofacial injuries and the importance of mouthguards. Sports Med. 2014, 44, 777–783. [Google Scholar] [CrossRef]
- Andrade, R.A.; Modesto, A.; Evans, P.L.; Almeida, A.L.; de Jesus Rodrigues da Silva, J.; Guedes, A.M.; Guedes, F.R.; Ranalli, D.N.; Tinoco, E.M. Prevalence of oral trauma in Para-Pan American Games athletes. Dent. Traumatol. 2013, 29, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Cummins, N.K.; Spears, I.R. The effect of mouthguard design on stresses in the tooth-bone complex. Med. Sci. Sports Exerc. 2002, 34, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Ishigami, K.; Nakajima, K.; Naitoh, K.; Kurokawa, K.; Handa, J.; Shomura, M.; Regner, C.W. Are all mouthguards the same and safe to use? Part 2. The influence of anterior occlusion against a direct impact on maxillary incisors. Dent. Traumatol. 2008, 24, 360–365. [Google Scholar] [CrossRef]
- Patrick, D.G.; Van Noort, R.; Found, M.S. Evaluation of laminated structures for sports mouthguards. Key Eng. Mater. 2001, 221, 133–144. [Google Scholar] [CrossRef]
- Park, H.K.; Park, J.Y.; Choi, N.R.; Kim, U.K.; Hwang, D.S. Sports-related oral and maxillofacial injuries: A 5-year retrospective study, Pusan National University Dental Hospital. J. Oral Maxillofac. Surg. 2021, 79, 203.e1–203.e8. [Google Scholar] [CrossRef] [PubMed]
- Parker, K.; Marlow, B.; Patel, N.; Gill, D.S. A review of mouthguards: Effectiveness, types, characteristics and indications for use. Br. Dent. J. 2017, 222, 629–633. [Google Scholar] [CrossRef]
- Crout, D.K. Anatomy of an occlusal splint. Gen Dent. 2017, 65, 52–59. [Google Scholar]
- Verissimo, C.; Costa, P.V.; Santos-Filho, P.C.; Tantbirojn, D.; Versluis, A.; Soares, C.J. Custom-Fitted EVA Mouthguards: What is the ideal thickness? A dynamic finite element impact study. Dent. Traumatol. 2016, 32, 95–102. [Google Scholar] [CrossRef]
- Karaganeva, R.; Pinner, S.; Tomlinson, D.; Burden, A.; Taylor, R.; Yates, J.; Winwood, K. Effect of mouthguard design on retention and potential issues arising with usability in sport. Dent. Traumatol. 2019, 35, 73–79. [Google Scholar] [CrossRef]
- Takeda, T.; Ishigami, K.; Ogawa, T.; Nakajima, K.; Shibusawa, M.; Shimada, A.; Regner, C.W. Are all mouthguards the same and safe to use? The influence of occlusal supporting mouthguards in decreasing bone distortion and fractures. Dent. Traumatol. 2004, 20, 150–156. [Google Scholar] [CrossRef]
- Bishop, B.M.; Davies, E.H.; von Fraunhofer, J.A. Materials for mouth protectors. J. Prosthet. Dent. 1985, 53, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Green, J.I. The role of mouthguards in preventing and reducing sports-related trauma. Prim. Dent. J. 2017, 6, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.G.; Van Noort, R.; Found, M.S. Scale of protection and the various types of sports mouthguard. Br. J. Sports Med. 2005, 39, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Caneppele, T.M.; Borges, A.B.; Pereira, D.M.; Fagundes, A.A.; Fidalgo, T.K.; Maia, L.C. Mouthguard use and cardiopulmonary capacity: A systematic review and meta-analysis. Sports Med. Int. Open. 2017, 1, E172–E182. [Google Scholar] [CrossRef] [PubMed]
- Mizuhashi, F.; Koide, K. Appropriate fabrication method for vacuum-formed mouthguards. Dent. Traumatol. 2017, 33, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Handa, J.; Takeda, T.; Kurokawa, K.; Ozawa, T.; Nakajima, K.; Ishigami, K. Influence of pre-laminated material on shock absorption ability in specially designed mouthguard with hard insert and space. J. Prosthodont. Res. 2011, 55, 214–220. [Google Scholar] [CrossRef]
- Takeda, T.; Ishigami, K.; Mishima, O.; Karasawa, K.; Kurokawa, K.; Kajima, T.; Nakajima, K. Easy fabrication of a new type of mouthguard incorporating a hard insert and space and offering improved shock absorption ability. Dent. Traumatol. 2011, 27, 489–495. [Google Scholar] [CrossRef]
- Kamenskikh, A.A.; Ustjugova, T.N.; Kuchumov, A.G. Modelling of the tooth contact through one-layered mouthguard. J. Phys. Conf. Ser. 2018, 1129, 012014. [Google Scholar] [CrossRef]
- Abdulrahim, R.; Yanikoğlu, N. Evaluation of Fracture Resistance for Autopolymerizing Acrylic Resin Materials Reinforced with Glass Fiber Mesh, Metal Mesh and Metal Wire Materials: An In Vitro Study. Open J. Stomatol. 2022, 12, 33–41. [Google Scholar] [CrossRef]
- Meireles, A.B.; Corrêa, D.K.; da Silveira, J.V.; Millás, A.L.; Bittencourt, E.; de Brito-Melo, G.E.; González-Torres, L.A. Trends in Polymeric Electrospun Fibers and Their Use as Oral Biomaterials. Exp. Biol. Med. 2018, 243, 665–676. [Google Scholar] [CrossRef]
- Firmino, A.S.; Tribst, J.P.M.; Nakano, L.J.N.; de Oliveira Dal Piva, A.M.; Borges, A.L.S.; Paes-Junior, T.J.A. Silica-Nylon Reinforcement Effect on the Fracture Load and Stress Distribution of a Resin-Bonded Partial Dental Prosthesis. Int. J. Periodontics Restor. Dent. 2021, 41, e45–e54. [Google Scholar] [CrossRef] [PubMed]
- Schewe, P.; Roehler, A.; Spintzyk, S.; Huettig, F. Shock absorption behavior of elastic polymers for sports mouthguards: An In Vitro comparison of thermoplastic forming and additive manufacturing. Materials 2022, 15, 2928. [Google Scholar] [CrossRef] [PubMed]
- Hada, T.; Komagamine, Y.; Kanazawa, M.; Minakuchi, S. Fabrication of sports mouthguards using a semi-digital workflow with 4D-printing technology. J. Prosthodont. Res. 2023. [CrossRef] [PubMed]
- Trzaskowski, M.; Mańka-Malara, K.; Szczesio-Włodarczyk, A.; Sokołowski, J.; Kostrzewa-Janicka, J.; Mierzwińska-Nastalska, E. Evaluation of Mechanical Properties of 3D-Printed Polymeric Materials for Possible Application in Mouthguards. Polymers 2023, 15, 898. [Google Scholar] [CrossRef]
- Li, Z.; Wang, S.; Ye, H.; Lv, L.; Zhao, X.; Liu, Y.; Zhou, Y. Preliminary clinical application of complete workflow of digitally designed and manufactured sports mouthguards. Int. J. Prosthodont. 2020, 33, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Sarao, S.K.; Levin, L. Prevention of maxillofacial injuries through analysis of mechanisms, patterns, and long-term sequelae. Dent. Traumatol. 2023, 39, 97–100. [Google Scholar] [CrossRef]
- Tribst, J.P.; de Oliveira Dal Piva, A.M.; Borges, A.L.; Bottino, M.A. Influence of custom-made and stock mouthguard thickness on biomechanical response to a simulated impact. Dent. Traumatol. 2018, 34, 429–437. [Google Scholar] [CrossRef]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. EVA mouthguards: How thick should they be? Dent. Traumatol. 2002, 18, 24–27. [Google Scholar] [CrossRef]
- Shelley, A.; Winwood, K.; Allen, T.; Horner, K. Effectiveness of hard inserts in sports mouthguards: A systematic review. Br. Dent. J. 2022, 1–9. [Google Scholar] [CrossRef]
- ASTM F697-16; Standard Practice for Care and Use of Athletic Mouth Protectors. ASTM International: West Conshohocken, PA, USA, 2016.
- Borges, A.L.S.; Dal Piva, A.M.D.O.; Concílio, L.R.D.S.; Paes-Junior, T.J.D.A.; Tribst, J.P.M. Mouthguard Use Effect on the Biomechanical Response of an Ankylosed Maxillary Central Incisor during a Traumatic Impact: A 3-Dimensional Finite Element Analysis. Life 2020, 10, 294. [Google Scholar] [CrossRef]
- Dal Piva, A.M.O.; Tribst, J.P.M.; Borges, A.L.S.; Kleverlaan, C.J.; Feilzer, A.J. The Ability of Mouthguards to Protect Veneered Teeth: A 3D Finite Element Analysis. Dent. Traumatol. 2023, 39, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Sarao, S.K.; Levin, L. Mouthguard Design, Pediatric Trauma, and Reporting Guidelines. Dent. Traumatol. 2023, 39, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.V.d.M.; Firmiano, T.C.; Borges, G.A.; Dantas, R.P.; Veríssimo, C. The Effect of the Simulated Aging by Thermocycling on the Elastic Modulus of Ethylene-Vinyl Acetate Brands and Stress/Strain Development during an Impact: An in Vitro and 3D-FEA Analysis. Dent. Traumatol. 2023. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Mouthguard | Level of Protection | Retention/Adaptation | Material | Manufacturing Process | Side Effects | Cost * |
|---|---|---|---|---|---|---|
| Stock Mouthguards (pre-fabricated) | Low | Poor | Polyurethane, polyvinyl chloride, or a copolymer of vinyl acetate and ethylene | Self-use; patients can use them as soon as they acquire them | Discomfort in speech and breathing; muscular fatigue due to the need to maintain constant occlusion | Low (most financially accessible and easiest to find on the market) |
| Mouth-formed mouthguards (boil and bite) | The lack of control over the fitting process can compromise the protective capabilities of this type of mouthguard | Prone to misfits and variations in thickness depending on the force applied to each area by the fingers | Thermoplastic materials | Self-use; patients need to put it in hot water and self-adapt it to their teeth | May not cover all the necessary regions for protection due to the limited availability of size options | Low/Medium |
| Ergonomic custom-made mouthguards | The highest level of protection against injuries for athletes when properly fabricated | The most precise and efficient technique | Thermoplastic materials; the most commonly used material is ethylene vinyl acetate (EVA) | Patients must visit a dentist to undergo oral impressions and create a plaster model that accurately replicates the mouth structure, including the final molars, labial frenum, palate, and complete vestibular extension | Insignificant when compared to the other types of mouthguards | More expensive than the other types of mouthguards, due to the need for professional expertise |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Queiroz, T.S.; da Cruz, B.S.; Demachkia, A.M.M.; Borges, A.L.S.; Tribst, J.P.M.; Paes Junior, T.J.d.A. Ergonomic Sports Mouthguards: A Narrative Literature Review and Future Perspectives. Appl. Sci. 2023, 13, 11353. https://doi.org/10.3390/app132011353
De Queiroz TS, da Cruz BS, Demachkia AMM, Borges ALS, Tribst JPM, Paes Junior TJdA. Ergonomic Sports Mouthguards: A Narrative Literature Review and Future Perspectives. Applied Sciences. 2023; 13(20):11353. https://doi.org/10.3390/app132011353
Chicago/Turabian StyleDe Queiroz, Talita Suelen, Beatriz Serralheiro da Cruz, Amir Mohidin Mohamed Demachkia, Alexandre Luiz Souto Borges, João Paulo Mendes Tribst, and Tarcisio José de Arruda Paes Junior. 2023. "Ergonomic Sports Mouthguards: A Narrative Literature Review and Future Perspectives" Applied Sciences 13, no. 20: 11353. https://doi.org/10.3390/app132011353
APA StyleDe Queiroz, T. S., da Cruz, B. S., Demachkia, A. M. M., Borges, A. L. S., Tribst, J. P. M., & Paes Junior, T. J. d. A. (2023). Ergonomic Sports Mouthguards: A Narrative Literature Review and Future Perspectives. Applied Sciences, 13(20), 11353. https://doi.org/10.3390/app132011353