
Salivary Volatile Organic Compound Analysis: An Optimised Methodology and Longitudinal Assessment Using Direct Injection Mass Spectrometry

Abstract
:1. Introduction
2. Material and Methods
2.1. Participant Selection
2.2. Optimal Saliva Sampling Parameters
2.3. Longitudinal Assessment of Salivary VOCs
3. Statistical Analysis
4. Results
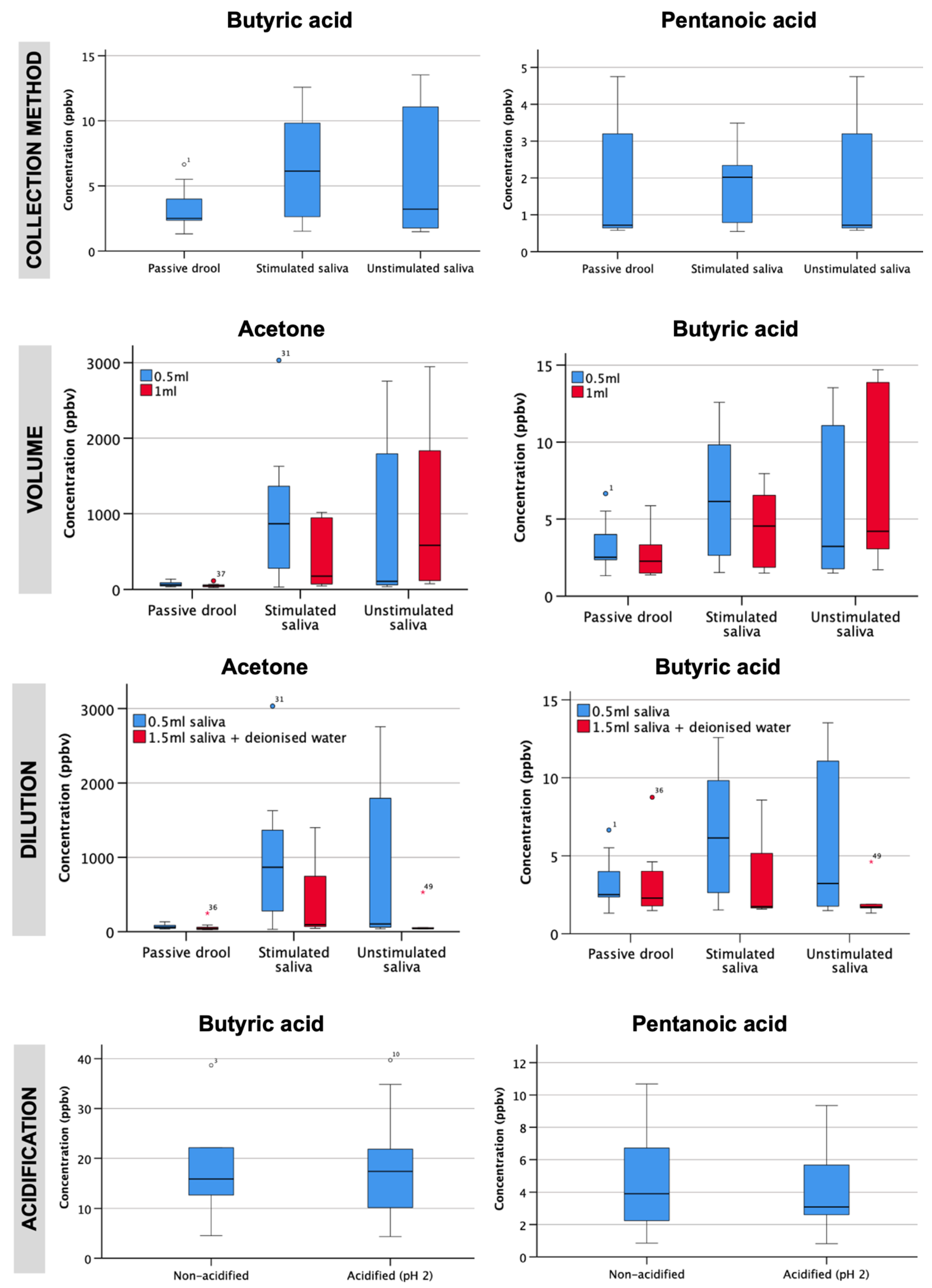
4.1. Optimal Saliva Sampling Parameters
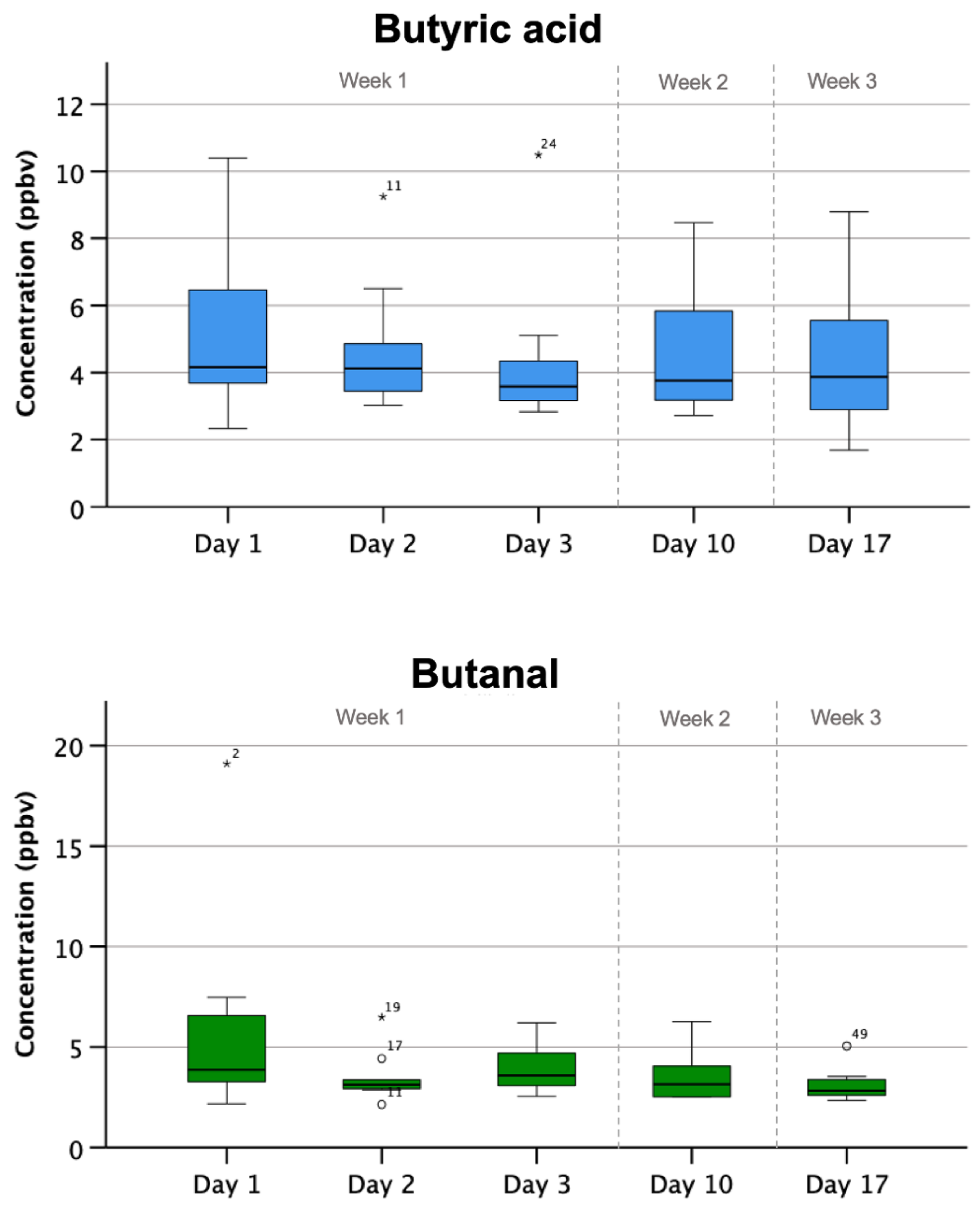
4.2. Longitudinal Assessment of Salivary VOCs
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Phillips, M.; Herrera, J.; Krishnan, S.; Zain, M.; Greenberg, J.; Cataneo, R.N. Variation in volatile organic compounds in the breath of normal humans. J. Chromatogr. B Biomed. Sci. Appl. 1999, 729, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Pal, V.K.; Li, A.J.; Zhu, H.; Kannan, K. Diurnal variability in urinary volatile organic compound metabolites and its association with oxidative stress biomarkers. Sci.Total Environ. 2022, 818, 151704. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow, and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Bel’skaya, L.V.; Sarf, E.A.; Shalygin, S.P.; Postnova, T.V.; Kosenok, V.K. Identification of salivary volatile organic compounds as potential markers of stomach and colorectal cancer: A pilot study. J. Oral Biosci. 2020, 62, 212–221. [Google Scholar] [CrossRef]
- Monedeiro, F.; Milanowski, M.; Ratiu, I.A.; Zmysłowski, H.; Ligor, T.; Buszewski, B. VOC Profiles of Saliva in Assessment of Halitosis and Submandibular Abscesses Using HS-SPME-GC/MS Technique. Molecules 2019, 24, 2977. [Google Scholar] [CrossRef] [Green Version]
- Vadhwana, B.; Belluomo, I.; Boshier, P.R.; Pavlou, C.; Španěl, P.; Hanna, G.B. Impact of oral cleansing strategies on exhaled volatile organic compound levels. Rapid Commun. Mass Spectrom. 2020, 34, e8706. [Google Scholar] [CrossRef]
- Bhattarai, K.R.; Kim, H.R.; Chae, H.J. Compliance with Saliva Collection Protocol in Healthy Volunteers: Strategies for Managing Risk and Errors. Int. J. Med. Sci. 2018, 15, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Inui, T.; Palmer, R.J., Jr.; Shah, N.; Li, W.; Cisar, J.O.; Wu, C.D. Effect of mechanically stimulated saliva on initial human dental biofilm formation. Sci. Rep. 2019, 9, 11805. [Google Scholar] [CrossRef] [Green Version]
- Iorgulescu, G. Saliva between normal and pathological. Important factors in determining systemic and oral health. J. Med. Life 2009, 2, 303–307. [Google Scholar] [PubMed]
- Al-Kateb, H.; de Lacy Costello, B.; Ratcliffe, N. An investigation of volatile organic compounds from the saliva of healthy individuals using headspace-trap/GC-MS. J. Breath Res. 2013, 7, 036004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, H.J.; Riazanskaia, S.; Thomas, C.L. Sampling and characterisation of volatile organic compound profiles in human saliva using a polydimethylsiloxane coupon placed within the oral cavity. Analyst 2012, 137, 3627–3634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markar, S.R.; Wiggins, T.; Antonowicz, S.; Chin, S.T.; Romano, A.; Nikolic, K.; Evans, B.; Cunningham, D.; Mughal, M.; Lagergren, J.; et al. Assessment of a Noninvasive Exhaled Breath Test for the Diagnosis of Oesophagogastric Cancer. JAMA Oncol. 2018, 4, 970–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawes, C. Circadian rhythms in human salivary flow rate and composition. J Physiol. 1972, 220, 529–545. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Seon, Y.J.; McHugh, J.; Papagerakis, S.; Papagerakis, P. Clock genes show circadian rhythms in salivary glands. J Dent. Res. 2012, 91, 783–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Acetone (m/z 59) | Acetic Acid (m/z 61) | Butyric Acid (m/z 89) | Pentanoic Acid (m/z 103) | Hexanoic Acid (m/z 117) | |
|---|---|---|---|---|---|
| Saliva collection | |||||
| Passive drool | 60 (46–86) | 14 (13–14) | 2.5 (2.4–4.0) | 1.0 (0.8–1.1) | 0.8 (0.7–0.9) |
| Unstimulated saliva | 104 (61–1793) | 14 (14–37) | 3.2 (1.8–11.1) | 0.7 (0.6–3.2) | 0.7 (0.6–2.3) |
| Stimulated saliva | 866 (278–1365) | 24 (16–27) | 6.1 (2.6–9.8) | 2.0 (0.8–2.3) | 1.1 (0.8–1.5) |
| Volume | |||||
| Passive drool | |||||
| 500 µL | 57 (46–90) | 14 (13–14) | 2.5 (2.3–3.9) | 0.9 (0.8–1.1) | 0.8 (0.7–0.9) |
| 1000 µL | 51 (37–58) | 13 (13–14) | 2.3 (1.6–3.2) | 0.8 (0.7–1.0) | 0.8 (0.5–0.8) |
| Unstimulated saliva | |||||
| 500 µL | 1430 (390–1883) | 28 (16–44) | 8.2 (4.0–12) | 2.0 (0.9–3.9) | 1.8 (0.8–2.3) |
| 1000 µL | 581 (213–1538) | 18 (15–44) | 4.2 (3.3–12) | 1.2 (0.8–4.3) | 1.0 (0.7–2.4) |
| Stimulated saliva | |||||
| 500 µL | 866 (453–1365) | 24 (19–27) | 6.1 (3.2–9.7) | 2.0 (1.3–2.6) | 1.3 (0.9–1.6) |
| 1000 µL | 173 (71–946) | 14 (13–26) | 4.5 (1.9–6.5) | 0.8 (0.6–2.9) | 0.7 (0.6–1.6) |
| Dilution | |||||
| Passive drool | |||||
| 500 µL saliva | 60 (46–86) | 14 (13–14) | 2.5 (2.4–4.0) | 1.0 (0.8–1.1) | 0.8 (0.7–0.9) |
| 500 µL saliva + 1 mL deionised water | 41 (29–59) | 13 (13–14) | 2.3 (1.8–4.0) | 0.9 (0.7–0.9) | 0.8 (0.7–0.9) |
| Unstimulated saliva * | |||||
| 500 µL saliva | 104 (55–104) | 14 (14–14) | 1.8 (1.6–3.2) | 0.7 (0.6–0.7) | 0.6 (0.6–0.7) |
| 500 µL saliva + 1 mL deionised water | 43 (40–55) | 14 (14–15) | 1.7 (1.7–1.9) | 0.7 (0.7–0.7) | 0.6 (0.6–0.7) |
| Stimulated saliva † | |||||
| 500 µL saliva | 1589 | 28 | 8.9 | 2.2 | 1.8 |
| 500 µL saliva + 1 mL deionised water | 512 | 19 | 4.0 | 1.3 | 1.0 |
| Acidification | |||||
| Non-acidified | 761 (635–1500) | 85 (43–108) | 16 (13–21) | 3.9 (2.6–6.0) | 2.0 (1.2–2.7) |
| Acidified (pH 2.0) | 692 (556–932) | 91 (47–160) | 17 (10–22) | 3.1 (2.6–5.7) | 2.0 (1.2–2.5) |
| Compound | Median Concentration (ppbv) | CV% | p Value | ||||
|---|---|---|---|---|---|---|---|
| Day 1 | Day 2 | Day 3 | Day 10 | Day 17 | |||
| Acetone | 179 | 145 | 184 | 196 | 246 | 19 | 0.06 |
| Short chain fatty acids | |||||||
| Acetic acid | 8.2 | 6.7 | 6.5 | 6.9 | 6.7 | 9.6 | 0.03 |
| Butanoic acid | 4.2 | 4.1 | 3.6 | 3.8 | 3.9 | 6.3 | 0.28 |
| Hexanoic acid | 1.4 | 1.3 | 1.0 | 1.2 | 1.0 | 15 | 0.15 |
| Pentanoic acid | 4.3 | 3.7 | 3.7 | 3.5 | 3.8 | 7.9 | 0.12 |
| Propanoic acid | 5.3 | 4.2 | 3.9 | 3.6 | 4.2 | 16 | <0.001 |
| Aldehydes | |||||||
| Acetaldehyde | 153 | 175 | 207 | 135 | 210 | 19 | 0.049 |
| Butanal | 3.9 | 3.1 | 3.6 | 3.1 | 2.8 | 13 | 0.05 |
| Decanal | 1.6 | 1.5 | 1.8 | 1.8 | 1.5 | 8.1 | 0.71 |
| Heptanal | 2.4 | 2.3 | 2.6 | 2.5 | 1.8 | 13 | 0.02 |
| Hexanal | 6.7 | 4.8 | 5.6 | 4.3 | 4.5 | 19 | 0.4 |
| Nonanal | 3.2 | 2.9 | 3.4 | 3.1 | 2.9 | 6.7 | 0.03 |
| Octanal | 2.8 | 2.2 | 2.6 | 2.3 | 2.2 | 11 | 0.69 |
| Pentanal | 14.8 | 13.5 | 12.0 | 11.5 | 12.6 | 10 | 0.3 |
| Propanal | 28.2 | 20.0 | 28.5 | 19.9 | 28.3 | 18.4 | 0.69 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vadhwana, B.; James, J.; Pelling, M.; Belluomo, I.; Boshier, P.R.; Hanna, G.B. Salivary Volatile Organic Compound Analysis: An Optimised Methodology and Longitudinal Assessment Using Direct Injection Mass Spectrometry. Appl. Sci. 2023, 13, 4084. https://doi.org/10.3390/app13074084
Vadhwana B, James J, Pelling M, Belluomo I, Boshier PR, Hanna GB. Salivary Volatile Organic Compound Analysis: An Optimised Methodology and Longitudinal Assessment Using Direct Injection Mass Spectrometry. Applied Sciences. 2023; 13(7):4084. https://doi.org/10.3390/app13074084
Chicago/Turabian StyleVadhwana, Bhamini, Jack James, Melina Pelling, Ilaria Belluomo, Piers R. Boshier, and George B. Hanna. 2023. "Salivary Volatile Organic Compound Analysis: An Optimised Methodology and Longitudinal Assessment Using Direct Injection Mass Spectrometry" Applied Sciences 13, no. 7: 4084. https://doi.org/10.3390/app13074084
APA StyleVadhwana, B., James, J., Pelling, M., Belluomo, I., Boshier, P. R., & Hanna, G. B. (2023). Salivary Volatile Organic Compound Analysis: An Optimised Methodology and Longitudinal Assessment Using Direct Injection Mass Spectrometry. Applied Sciences, 13(7), 4084. https://doi.org/10.3390/app13074084