Comparison of the Operator and Surrounding Dose When Using Portable Intraoral X-ray Devices

 , , ,
, , , 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Devices and Equipment
2.2. Measurement of the X-ray Output
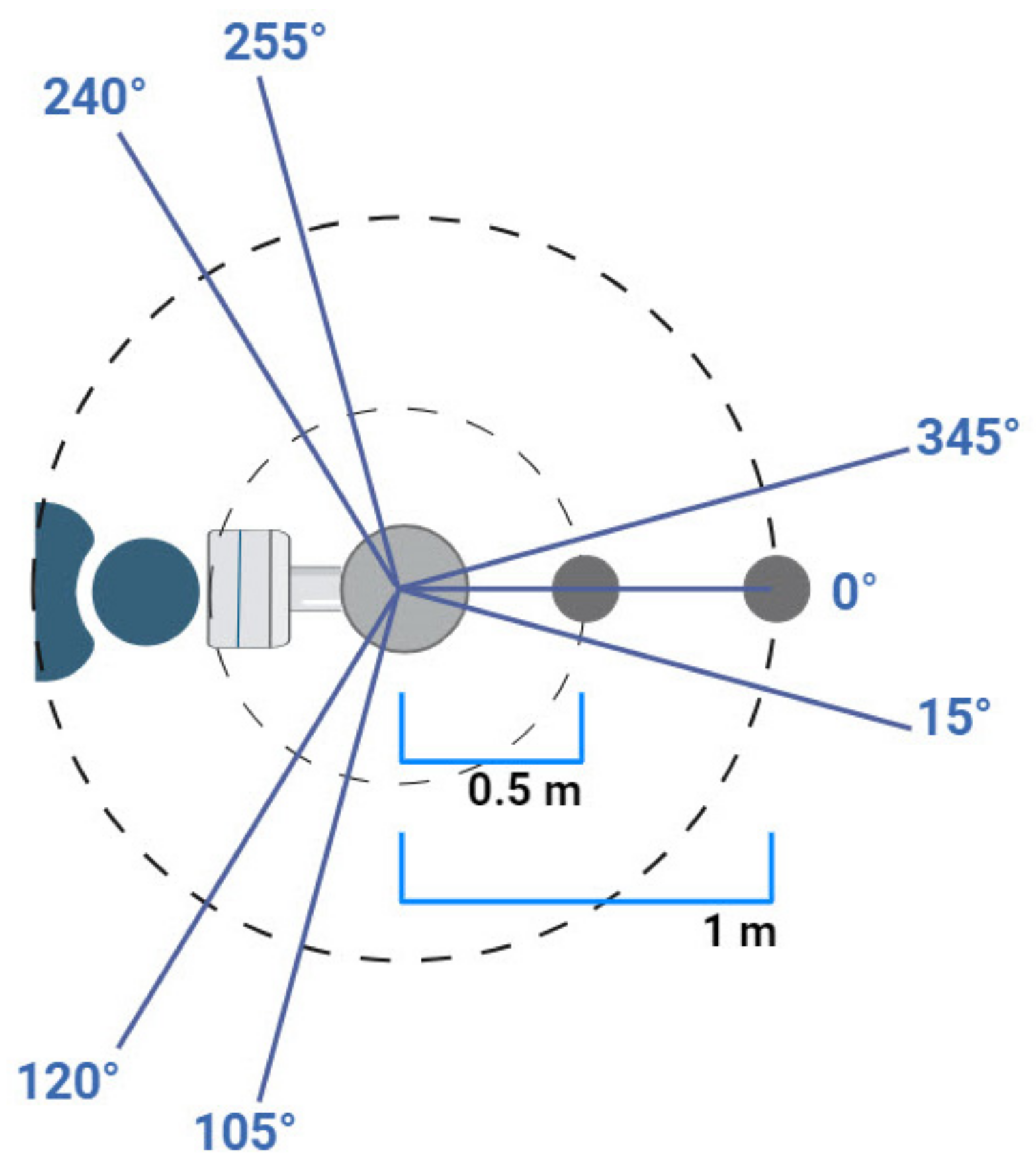
2.3. Measurement of the Scattered Dose
2.4. Measurement Based on the Operator Dose Limits
3. Results
3.1. Output Measurements
3.2. Scattered Dose Measurements
3.3. Dose Limit Considerations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, S.C.; Pharoah, M.J. White and Pharoah’s Oral Radiology E-Book: Principles and Interpretation; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Charlton, D.G. Portable dental equipment: Dental units and X-ray equipment. Gen. Dent. 2009, 57, 336–341. [Google Scholar]
- Coy, J. Hand-held dental X-ray (HDX) with medical collimator: Use in casualty radiology. Mil. Med. 1996, 161, 428–431. [Google Scholar] [CrossRef]
- Coy, J.; Vandre, R.H.; Davidson, W.R. Use of the hand-held dental X-ray machine during joint operation, NATO exercise Display Determination-92. Mil. Med. 1997, 162, 575–577. [Google Scholar] [CrossRef]
- Van Dis, M.L.; Miles, D.A.; Parks, E.T.; Razmus, T.F. Information yield from a hand-held dental X-ray unit. Oral. Surg. Oral. Med. Oral. Pathol. 1993, 76, 381–385. [Google Scholar] [CrossRef]
- Varghese, S.; Kimmel, A.; Radmer, T.; Bradley, T.G.; Bahcall, J. In vitro evaluation of the XR-15 portable X-ray unit for forensic odontology. J. Forensic Odontostomatol. 2004, 22, 5–8. [Google Scholar]
- McGiff, T.J.; Danforth, R.A.; Herschaft, E.E. Maintaining radiation exposures as low as reasonably achievable (ALARA) for dental personnel operating portable hand-held X-ray equipment. Health Phys. 2012, 103, S179–S185. [Google Scholar] [CrossRef] [PubMed]
- Makdissi, J.; Pawar, R.R.; Johnson, B.; Chong, B.S. The effects of device position on the operator’s radiation dose when using a handheld portable X-ray device. Dentomaxillofac. Radiol. 2016, 45, 20150245. [Google Scholar] [CrossRef] [PubMed]
- Geist, J.R. Handheld intraoral dental X-ray devices should supplement but not replace conventional radiographic equipment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Hosseini Pooya, S.; Hafezi, L.; Manafi, F.; Talaeipour, A. Assessment of the radiological safety of a Genoray portable dental X-ray unit. Dentomaxillofac. Radiol. 2015, 44, 20140255. [Google Scholar] [CrossRef] [PubMed]
- Danforth, R.A.; Herschaft, E.E.; Leonowich, J.A. Operator Exposure to Scatter Radiation from a Portable Hand-held Dental Radiation Emitting Device (Aribex™ NOMAD™) While Making 915 Intraoral Dental Radiographs. J. Forensic Sci. 2009, 54, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Leadbeatter, J.; Diffey, J. Evaluation of radiation exposure to operators of portable hand-held dental X-ray units. Phys. Eng. Sci. Med. 2021, 44, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Ghafari, R.; Khabiri, M.; Rafieian, M.; Khorrami, E.; Nikzad, S. Determination of scattered radiation around PORT-XII portable dental radiography unit. J. Isfahan Dent. Sch. 2013, 9, 329–336. [Google Scholar]
- ICRP. The 2007 Recommendations of the International Commission on Radiological Protection; ICRP: Ottawa, ON, Canada, 2007; pp. 2–4. [Google Scholar]
- Iwawaki, A.; Otaka, Y.; Asami, R.; Ozawa, T.; Izawa, M.; Saka, H. The study of protection of operators and surrounding workers at the time of using portable intraoral X-ray unit. Leg. Med. 2018, 33, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Otaka, Y.; Harata, Y.; Izawa, M.; Iwawaki, A.; Asami, R.; Saka, H.; Okumura, Y. On the safe use of portable intraoral X-ray units in large-scale disasters. Jpn. J. Oral. Diag./Oral Med. 2017, 30, 311–326. [Google Scholar] [CrossRef]
- Altındağ, A.; Eren, H.; Orhan, K.; Görgün, S. Evaluation of Operator and Patient Doses after Irradiation with Handheld X-ray Devices. Appl. Sci. 2023, 13, 10414. [Google Scholar] [CrossRef]
- Kim, E.; Park, H.; Choi, H.; Kim, J. An assessment of the usefulness of handheld X-ray devices in general radiography based on a performance evaluation experiment. Int. J. Radiat. Res. 2023, 21, 545–551. [Google Scholar] [CrossRef]
- Hoogeveen, R.C.; Ouchene, S.; Berkhout, W. Diagnostic image quality of hand-held and wall-mounted X-ray devices in bitewing radiography: A non-inferiority clinical trial. Dentomaxillofac. Radiol. 2021, 50, 20200471. [Google Scholar] [CrossRef] [PubMed]
- Amani, T.; Surenthar, M.; Umamaheswari, T.; Prethipa, R.; Kumar, L. Image Quality Assessment of Digital Radiographs Captured by Hand-Held Devices versus Wall-Mounted Devices: A Retrospective Comparative Study. Cureus 2024, 16, e52900. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, W.K. Radiation protection recommendations on dose limits: The role on the NCRP and the ICRP and future developments. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 387–392. [Google Scholar] [CrossRef]
- Wei, Y.; Dewji, S. A comprehensive review of dose limits, triage systems and measurement tools for consequence management of nuclear and radiological emergencies. Radiat. Phys. Chem. 2024, 217, 111533. [Google Scholar] [CrossRef]
- Laurier, D.; Billarand, Y.; Klokov, D.; Leuraud, K. The scientific basis for the use of the linear no-threshold (LNT) model at low doses and dose rates in radiological protection. J. Radiol. Prot. 2023, 43, 024003. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.C.; Kloos, D.K.; Morton, R. Radiation safety characteristics of the NOMAD™ portable X-ray system. Qual. Regul. Serv. 2005, 95648, 57. [Google Scholar]
- Iwawaki, A.; Otaka, Y.; Asami, R.; Ishii, T.; Kito, S.; Tamatsu, Y.; Aboshi, H.; Saka, H. Comparison of air dose and operator exposure from portable X-ray units. Leg. Med. 2020, 47, 101787. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Model | Tube Voltage | Tube Current | Exposure Time | Focal Spot | Total Filtration |
|---|---|---|---|---|---|
| iRay D3 | 60 kV (fixed) | 2 mA (fixed) | 0.05–1.35 s | 0.8 mm | 2.3 mmAl |
| EZRay Air | 60–65 kV | 2.5–3 mA | 0.05–1 s | 0.4 mm | 1.5 mmAl (min) |
| Epix | 60 kV (fixed) | 2 mA (fixed) | 1 s | 0.8 mm | 1.6 mmAl |
| Radiographic Unit | Region | 0.5 m | 1 m |
|---|---|---|---|
| iRay D3 | Anterior | 1.43 | 0.09 |
| Sides | 0.16 | 0.00 | |
| Posterior | 0.20 | 0.00 | |
| EZRay Air | Anterior | 0.82 | 0.51 |
| Sides | 0.48 | 0.15 | |
| Posterior | 0.34 | 0.24 | |
| Epix | Anterior | 5.51 | 0.80 |
| Sides | 4.22 | 1.30 | |
| Posterior | 5.04 | 1.01 |
| Radiographic Unit | Region | 0.5 m | 1 m |
|---|---|---|---|
| iRay D3 | Anterior | 789.27 | 47.22 |
| Sides | 89.51 | 0.00 | |
| Posterior | 93.43 | 0.00 | |
| EZRay Air | Anterior | 228.77 | 140.64 |
| Sides | 134.10 | 42.35 | |
| Posterior | 95.33 | 67.33 | |
| Epix | Anterior | 616.84 | 89.34 |
| Sides | 472.22 | 145.31 | |
| Posterior | 564.66 | 112.85 |
| Radiographic Unit | 0.5 m | 1 m |
|---|---|---|
| iRay D3 | 961 | - |
| EZRay Air | 565 | 801 |
| Epix | 38 | 190 |
| Radiographic Unit | 0.5 m | 1 m |
|---|---|---|
| iRay D3 | 384 | - |
| EZRay Air | 226 | 320 |
| Epix | 15 | 76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdinian, M.; Aminian, M.; Keymasi, F.; Soltani, P.; Cernera, M.; Armogida, N.G.; Spagnuolo, G. Comparison of the Operator and Surrounding Dose When Using Portable Intraoral X-ray Devices. Appl. Sci. 2024, 14, 3515. https://doi.org/10.3390/app14083515
Abdinian M, Aminian M, Keymasi F, Soltani P, Cernera M, Armogida NG, Spagnuolo G. Comparison of the Operator and Surrounding Dose When Using Portable Intraoral X-ray Devices. Applied Sciences. 2024; 14(8):3515. https://doi.org/10.3390/app14083515
Chicago/Turabian StyleAbdinian, Mehrdad, Maedeh Aminian, Forouzan Keymasi, Parisa Soltani, Mariangela Cernera, Niccolo Giuseppe Armogida, and Gianrico Spagnuolo. 2024. "Comparison of the Operator and Surrounding Dose When Using Portable Intraoral X-ray Devices" Applied Sciences 14, no. 8: 3515. https://doi.org/10.3390/app14083515
APA StyleAbdinian, M., Aminian, M., Keymasi, F., Soltani, P., Cernera, M., Armogida, N. G., & Spagnuolo, G. (2024). Comparison of the Operator and Surrounding Dose When Using Portable Intraoral X-ray Devices. Applied Sciences, 14(8), 3515. https://doi.org/10.3390/app14083515