Wearable Current-Based ECG Monitoring System with Non-Insulated Electrodes for Underwater Application

 , ,
, , 

Abstract
:1. Introduction
2. Circuit Design
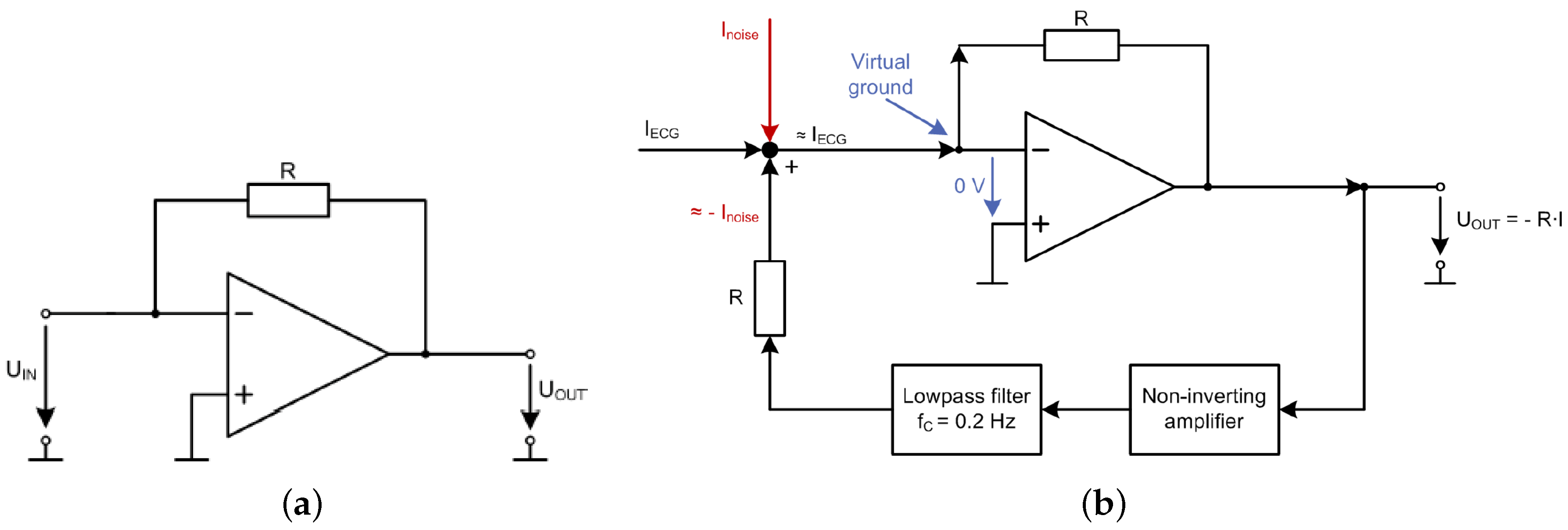
2.1. Transimpedance Amplifier
2.2. Signal Processing
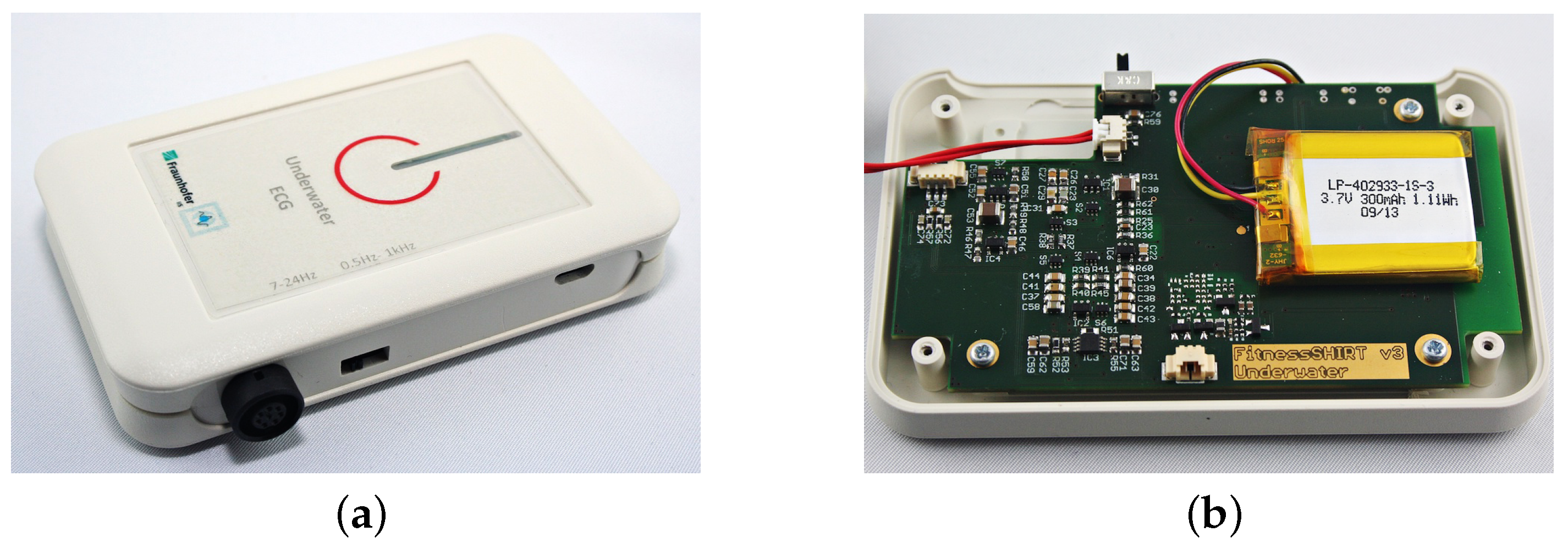
2.3. Power Supply and Housing
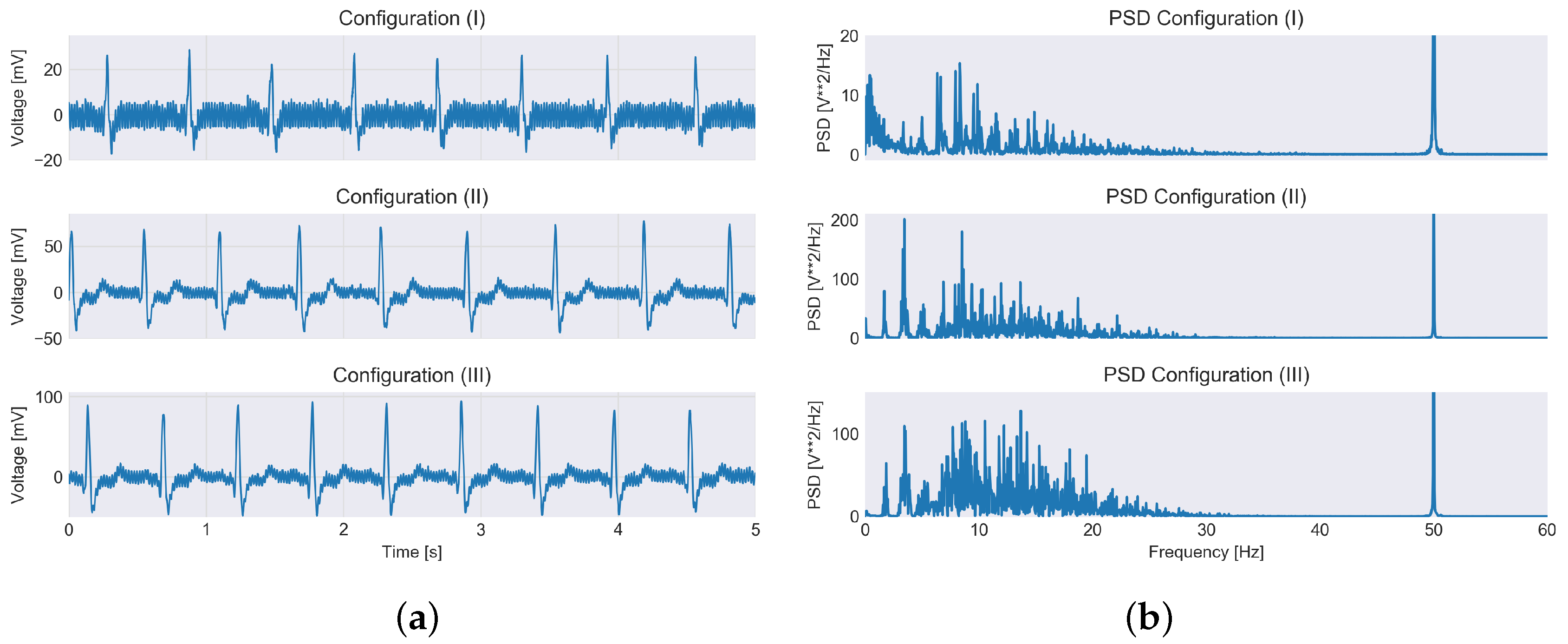
3. Physiological Measurements
4. Heart Rate Variability (HRV) Study
4.1. Subjects
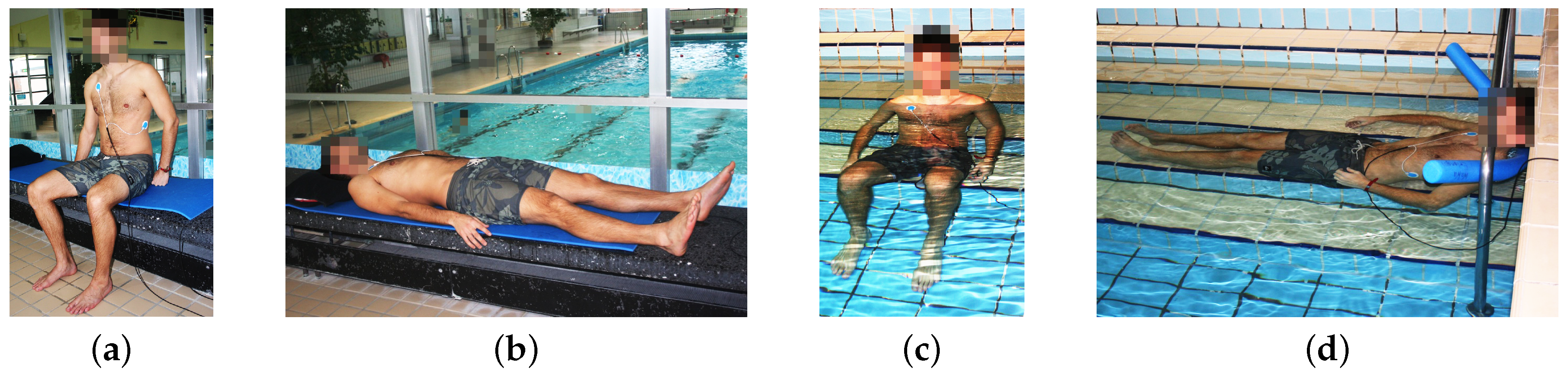
4.2. Method
4.3. Results
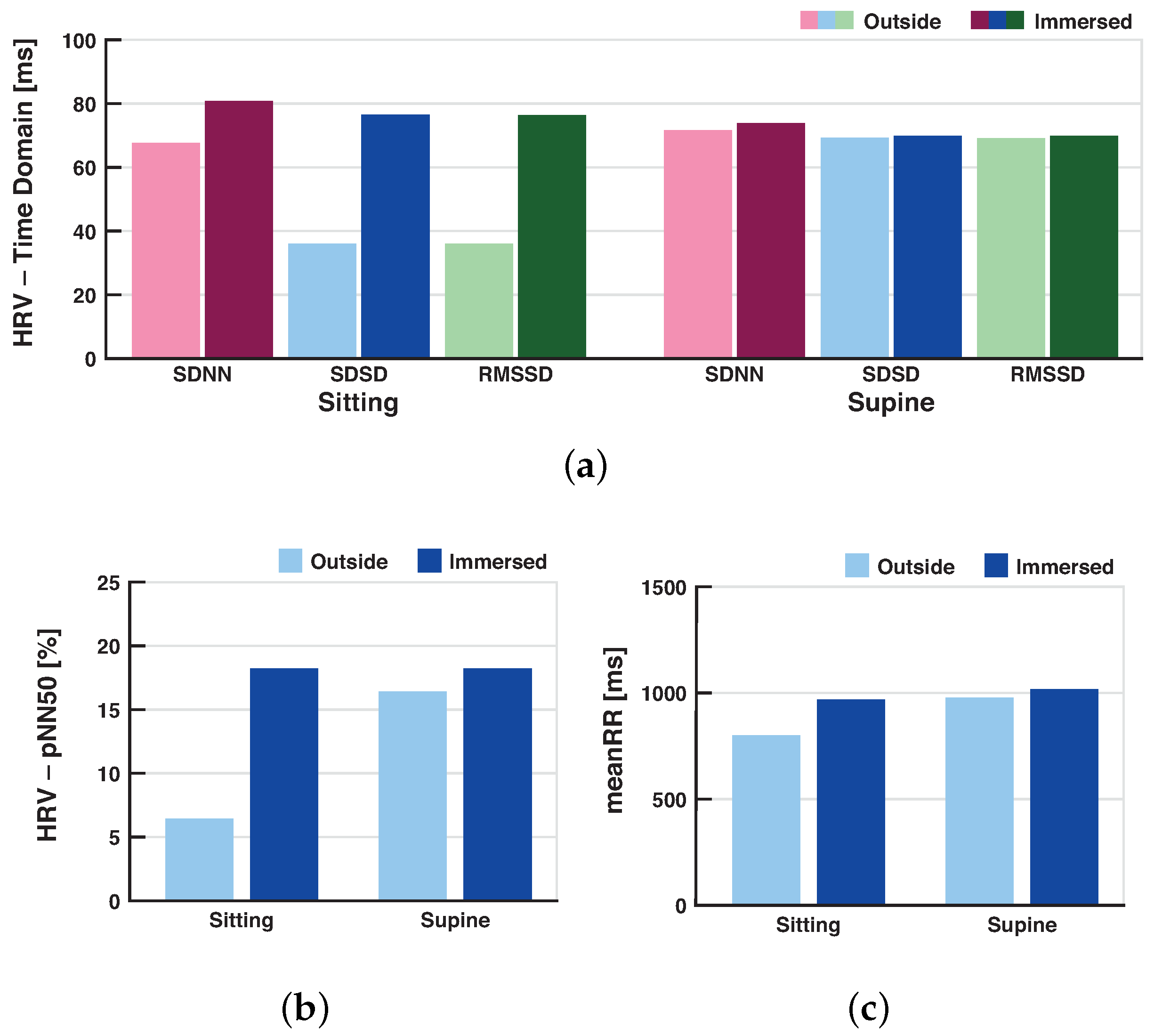
4.3.1. Time Domain Parameters
4.3.2. Frequency Domain Parameters
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Buzzacott, P. Dan Annual Diving Report; Divers Alert Network: Durham, NC, USA, 2015. [Google Scholar]
- Bennett, M. Cardiac Problems and Sudden Death. In Diving and Subaquatic Medicine, 5th ed.; Edmonds, C., Bennett, M., Lippmann, J., Mitchell, S., Eds.; CRC Press: Boca Raton, FL, USA, 2015; pp. 449–457. [Google Scholar]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart Rate Variability: Standards of Measurement, Physiological Interpretation and Clinical Use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Schipke, J.D.; Pelzer, M. Effect of Immersion, Submersion, and Scuba Diving on Heart Rate Variability. Br. J. Sport Med. 2001, 35, 174–180. [Google Scholar] [CrossRef]
- Salahuddin, L.; Cho, J.; Jeong, M.G.; Kim, D. Ultra Short Term Analysis of Heart Rate Variability for Monitoring Mental Stress in Mobile Settings. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; Volume 2007, pp. 4656–4659. [Google Scholar]
- Myers, G.A.; Martin, G.J.; Magid, N.M.; Barnett, P.S.; Schaad, J.W.; Weiss, J.S.; Lesch, M.; Singer, D.H. Power Spectral Analysis of Heart Rate Varability in Sudden Cardiac Death: Comparison to Other Methods. IEEE Trans. Biomed. Eng. 1986, 33, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Richer, R.; Groh, B.H.; Blank, P.; Dorschky, E.; Martindale, C.; Klucken, J.; Eskofier, B.M. Unobtrusive Real-Time Heart Rate Variability Analysis for the Detection of Orthostatic Dysregulation. In Proceedings of the IEEE 13th International Conference on Wearable and Implantable Body Sensor Networks (BSN), San Francisco, CA, USA, 14–17 June 2016. [Google Scholar]
- Cibis, T.; McEwan, A.; Eskofier, B.; Lippmann, J.; Friedl, K.; Bennett, M. Diving into Research of Biomedical Engineering in Scuba Diving. IEEE Rev. Biomed. Eng. 2017. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.M.; Gholamhosseini, H.; Connolly, M.J. A Comprehensive Survey of Wearable and Wireless Ecg Monitoring Systems for Older Adults. Med. Biol. Eng. Comput. 2013, 51, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Bosco, G.; De Marzi, E.; Michieli, P.; Omar, H.R.; Camporesi, E.M.; Padulo, J.; Paoli, A.; Mangar, D.; Schiavon, M. 12-Lead Holter Monitoring in Diving and Water Sports: A Preliminary Investigation. Diving Hyperb. Med. 2014, 44, 202–207. [Google Scholar] [PubMed]
- Cibis, T.; Groh, B.H.; Gatermann, H.; Leutheuser, H.; Eskofier, B.M. Wearable Real-Time Ecg Monitoring with Emergency Alert System for Scuba Diving. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 6074–6077. [Google Scholar]
- Gradl, S.; Kugler, P.; Lohmüller, C.; Eskofier, B. Real-Time Ecg Monitoring and Arrhythmia Detection Using Android-Based Mobile Devices. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 2452–2455. [Google Scholar] [CrossRef]
- Barrett, P.M.; Komatireddy, R.; Haaser, S.; Topol, S.; Sheard, J.; Encinas, J.; Fought, A.J.; Topol, E.J. Comparison of 24-Hour Holter Monitoring with 14-Day Novel Adhesive Patch Electrocardiographic Monitoring. Am. J. Med. 2014, 127. [Google Scholar] [CrossRef] [PubMed]
- Ohtsu, M.; Fukuoka, Y.; Ueno, A. Underwater Electromyographic Measurement Using a Waterproof Insulated Electrode. Adv. Biomed. Eng. 2012, 1, 81–88. [Google Scholar] [CrossRef]
- Reyes, B.A.; Posada-Quintero, H.F.; Bales, J.R.; Clement, A.L.; Pins, G.D.; Swiston, A.; Riistama, J.; Florian, J.P.; Shykoff, B.; Qin, M. Novel Electrodes for Underwater Ecg Monitoring. IEEE Trans. Biomed. Eng. 2014, 61, 1863–1876. [Google Scholar] [CrossRef] [PubMed]
- Reyes, B. Performance Evaluation of Carbon Black Based Electrodes for Underwater Ecg Monitoring. In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Chicago, IL, USA, 26–30 August 2014. [Google Scholar]
- Noh, Y.; Bales, J.R.; Reyes, B.A.; Molignano, J.; Clement, A.L.; Pins, G.D.; Florian, J.P.; Chon, K.H. Novel Conductive Carbon Black and Polydimethlysiloxane Ecg Electrode: A Comparison with Commercial Electrodes in Fresh, Chlorinated, and Salt Water. Ann. Biomed. Eng. 2016, 44, 2464–2479. [Google Scholar] [CrossRef] [PubMed]
- Von Tscharner, V.; Maurer, C.; Ruf, F.; Nigg, B.M. Comparison of Electromyographic Signals from Monopolar Current and Potential Amplifiers Derived from a Penniform Muscle, the Gastrocnemius Medialis. J. Electromyogr. Kinesiol. 2013, 23, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Whitting, J.W.; von Tscharner, V. Monopolar Electromyographic Signals Recorded by a Current Amplifier in Air and under Water without Insulation. J. Electromyogr. Kinesiol. 2014, 24, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Inan, O.T.; Kovacs, G.T. An 11 Mu W, Two-Electrode Transimpedance Biosignal Amplifier with Active Current Feedback Stabilization. IEEE Trans. Biomed. Circuits Syst. 2010, 4, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Leutheuser, H.; Lang, N.R.; Gradl, S.; Struck, M.; Tobola, A.; Hofmann, C.; Anneken, L.; Eskofier, B.M. Textile Integrated Wearable Technologies for Sports and Medical Applications. In Smart Textiles; Springer: Berlin, Germany, 2017; pp. 359–382. [Google Scholar]
- Thakor, N.V.; Webster, J.G.; Tompkins, W.J. Estimation of Qrs Complex Power Spectra for Design of a Qrs Filter. IEEE Trans. Biomed. Eng. 1984, 31, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Kwatra, S.C.; Jain, V.K. A New Technique for Monitoring Heart Signals-Part I: Instrumentation Design. IEEE Trans. Biomed. Eng. 1986, BME-33, 35–41. [Google Scholar] [CrossRef]
- Wittling, W.; Wittling, R.A. Herzschlagvariabilität: Frühwarnsystem, Stress-Und Fitnessindikator: Grundlagen—Messmethoden—Anwendungen; Eichsfeld-Verlag: Heilbad Heiligenstadt, Germany, 2012. [Google Scholar]
- Elgendi, M. Fast Qrs Detection with an Optimized Knowledge-Based Method: Evaluation on 11 Standard Ecg Databases. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Gradl, S.; Leutheuser, H.; Elgendi, M.; Lang, N.; Eskofier, B.M. Temporal Correction of Detected R-Peaks in Ecg Signals: A Crucial Step to Improve Qrs Detection Algorithms. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2015, 522–525. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Prineas, R.J.; Crow, R.S.; Zhang, Z.M. The Minnesota Code Manual of Electrocardiographic Findings; Springer Science & Business Media: Berlin, Germany, 2009. [Google Scholar]
- Brubakk, A.; Neuman, T.S. Bennett and Elliotts’ Physiology and Medicine of Diving, 5th ed.; W.B. Saunders: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Boussuges, A.; Blanc, F.; Carturan, D. Hemodynamic Changes Induced by Recreational Scuba Diving. CHEST J. 2006, 129, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Flouris, A.D.; Scott, J.M. Heart Rate Variability Responses to a Psychologically Challenging Scuba Dive. J. Sports Med. Phys. Fit. 2009, 49, 382–386. [Google Scholar]
- Kinoshita, T.; Nagata, S.; Baba, R.; Kohmoto, T.; Iwagaki, S. Cold-Water Face Immersion Per Se Elicits Cardiac Parasympathetic Activity. Circ. J. 2006, 70, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Kiviniemi, A.M.; Breskovic, T.; Uglesic, L.; Kuch, B.; Maslov, P.Z.; Sieber, A.; Seppanen, T.; Tulppo, M.P.; Dujic, Z. Heart Rate Variability During Static and Dynamic Breath-Hold Dives in Elite Divers. Auton. Neurosci. 2012, 169, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Perini, R.; Milesi, S.; Biancardi, L.; Pendergast, D.R.; Veicsteinas, A. Heart Rate Variability in Exercising Humans: Effect of Water Immersion. Eur. J. Appl. Physiol. 1998, 77, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Kornreich, F.; Rautaharju, P.M.; Warren, J.; Montague, T.J.; Horacek, B. Multigroup Diagnosis of Body Surface Potential Maps. Am. J. Cardiol. 1985, 56, 169–178. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Sitting Outside Water | Sitting Inside Water | Supine Outside Water | Supine Inside Water |
|---|---|---|---|---|
| SDNN [ms] | 67.63 | 80.74 * | 71.65 | 73.80 |
| RMSSD [ms] | 36.03 | 76.33 * | 69.13 | 69.81 |
| SDSD [ms] | 36.08 | 76.46 ** | 69.24 | 69.92 |
| pNN50 [%] | 6.43 | 18.24 ** | 16.43 | 18.24 |
| meanRR [ms] | 801 | 969 ** | 977 | 1017 |
| Parameter | Sitting Outside Water | Sitting Inside Water | Supine Outside Water | Supine Inside Water |
|---|---|---|---|---|
| VLF [] | 590.8 | 767.4 | 523.8 | 442.4 |
| LF [] | 831.6 | 698.6 | 654.6 | 680.8 |
| HF [] | 188.5 | 711.7 ** | 699.4 | 583.7 |
| TP [] | 1611 | 2178 ** | 1878 | 1707 |
| LF/HF | 6.20 | 1.15 ** | 1.76 | 1.32 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gradl, S.; Cibis, T.; Lauber, J.; Richer, R.; Rybalko, R.; Pfeiffer, N.; Leutheuser, H.; Wirth, M.; Von Tscharner, V.; Eskofier, B.M. Wearable Current-Based ECG Monitoring System with Non-Insulated Electrodes for Underwater Application. Appl. Sci. 2017, 7, 1277. https://doi.org/10.3390/app7121277
Gradl S, Cibis T, Lauber J, Richer R, Rybalko R, Pfeiffer N, Leutheuser H, Wirth M, Von Tscharner V, Eskofier BM. Wearable Current-Based ECG Monitoring System with Non-Insulated Electrodes for Underwater Application. Applied Sciences. 2017; 7(12):1277. https://doi.org/10.3390/app7121277
Chicago/Turabian StyleGradl, Stefan, Tobias Cibis, Jasmine Lauber, Robert Richer, Ruslan Rybalko, Norman Pfeiffer, Heike Leutheuser, Markus Wirth, Vinzenz Von Tscharner, and Bjoern M. Eskofier. 2017. "Wearable Current-Based ECG Monitoring System with Non-Insulated Electrodes for Underwater Application" Applied Sciences 7, no. 12: 1277. https://doi.org/10.3390/app7121277
APA StyleGradl, S., Cibis, T., Lauber, J., Richer, R., Rybalko, R., Pfeiffer, N., Leutheuser, H., Wirth, M., Von Tscharner, V., & Eskofier, B. M. (2017). Wearable Current-Based ECG Monitoring System with Non-Insulated Electrodes for Underwater Application. Applied Sciences, 7(12), 1277. https://doi.org/10.3390/app7121277