Visualization and Interpretation of Convolutional Neural Network Predictions in Detecting Pneumonia in Pediatric Chest Radiographs




Abstract
:1. Introduction
2. Related Work
3. Materials and Methods
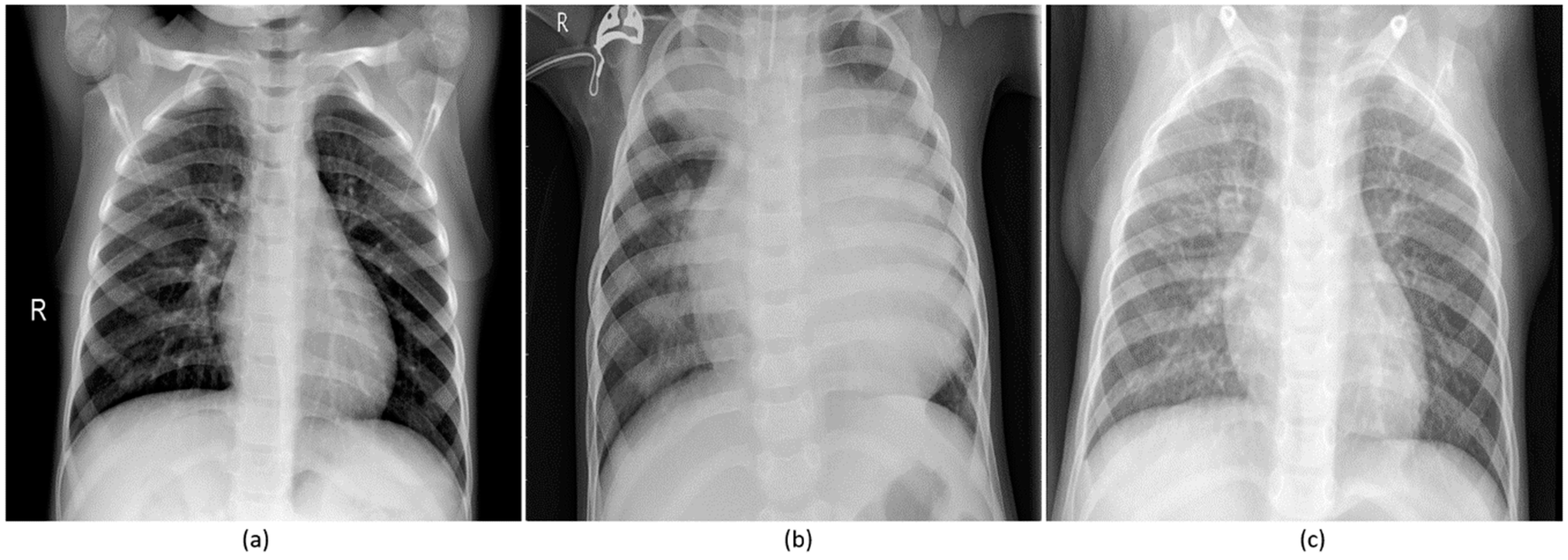
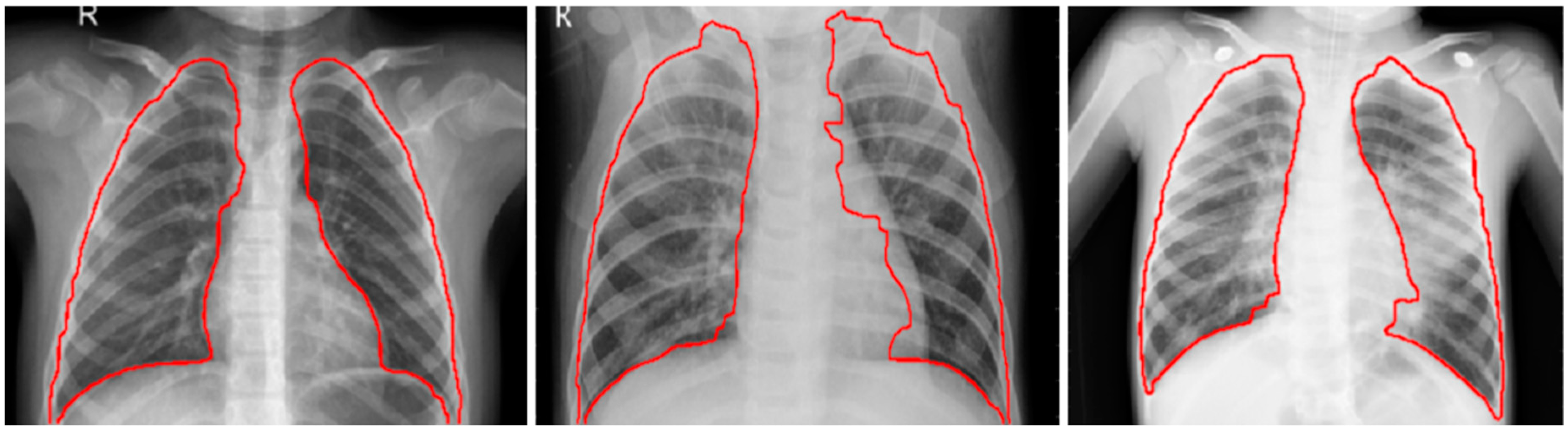
3.1. Data Collection and Preprocessing
3.2. Configuring CNNs for Pneumonia Detection
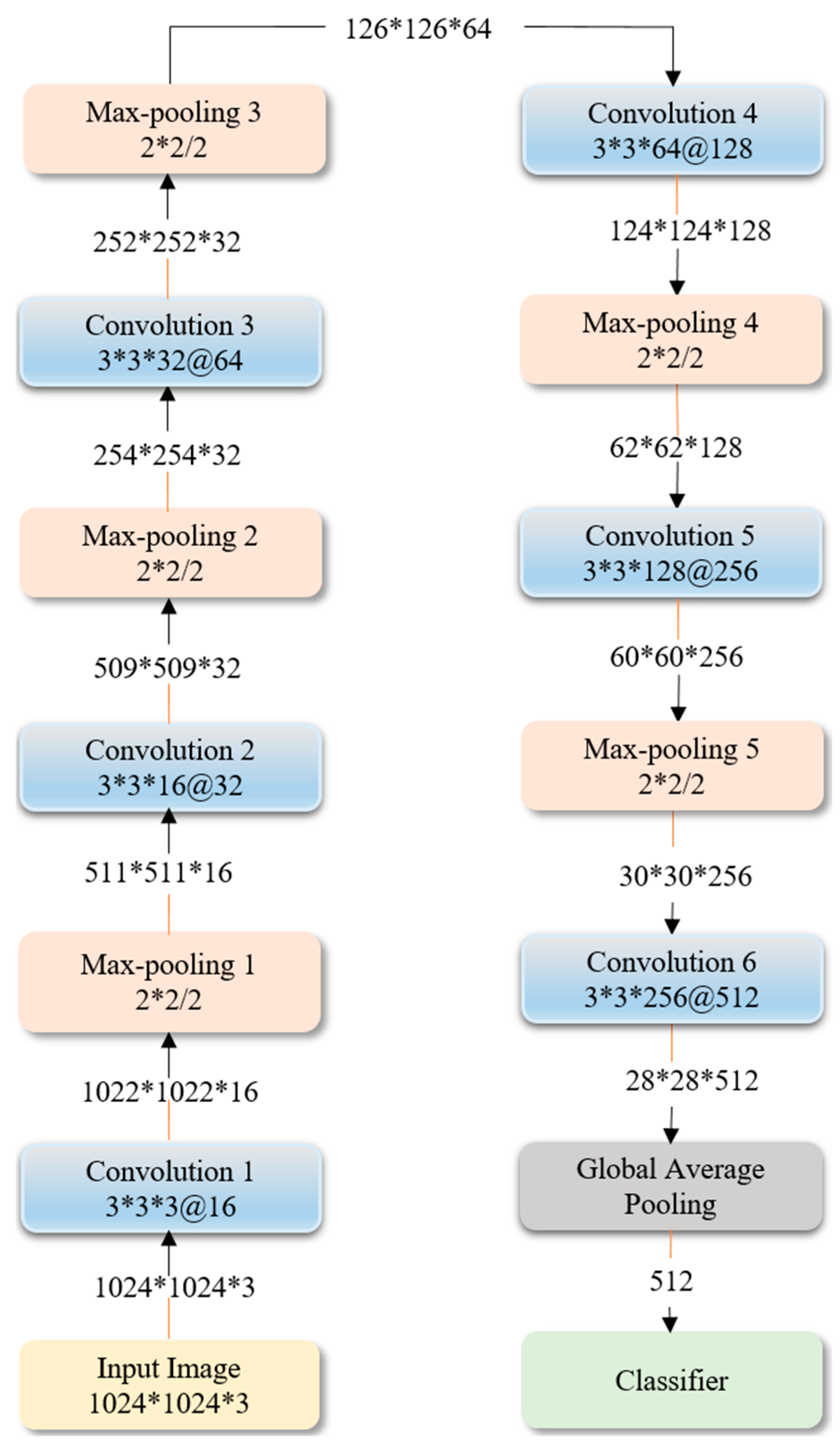
3.2.1. Sequential CNN
3.2.2. Residual CNN
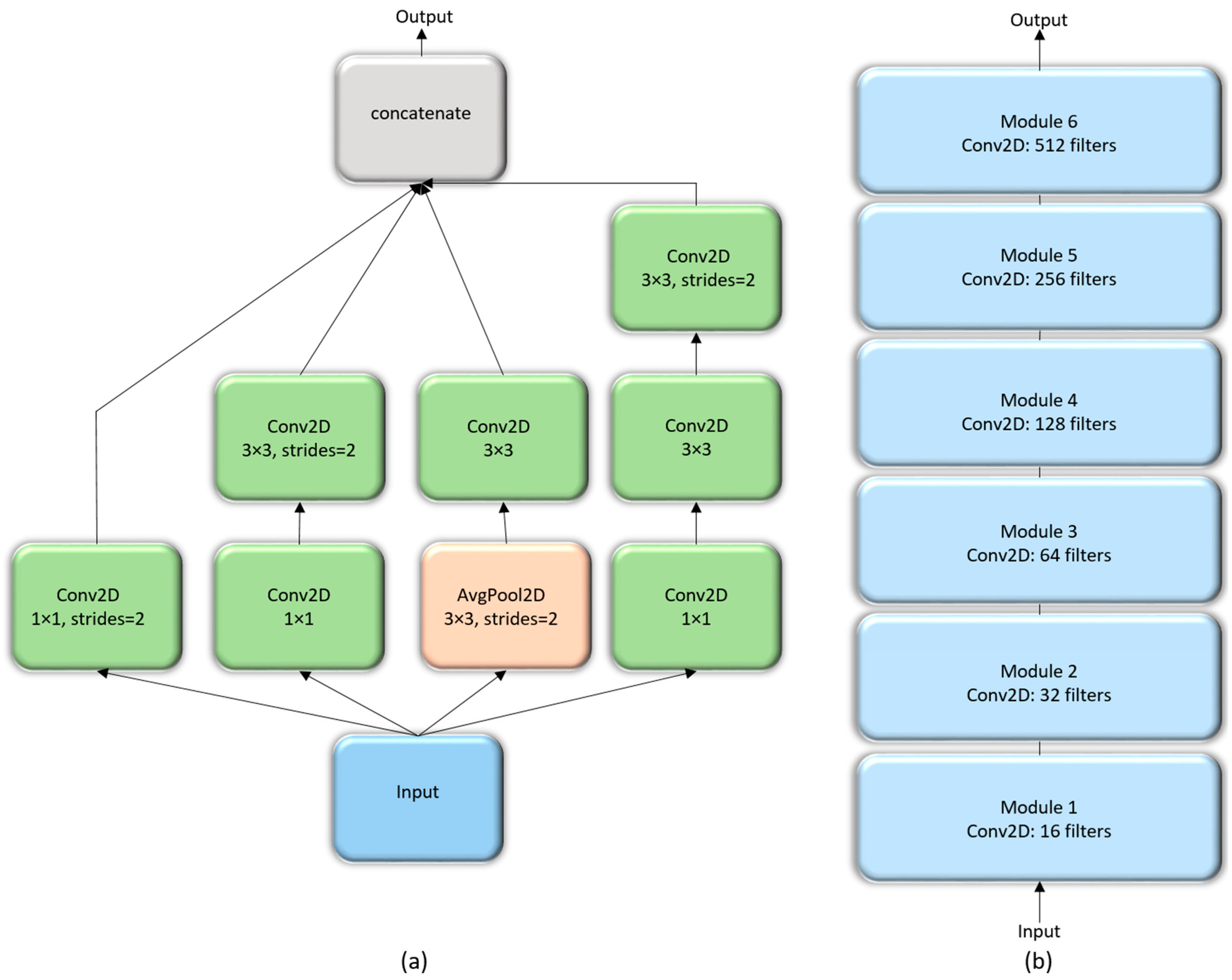
3.2.3. Inception CNN
3.2.4. Customized VGG16
3.3. Visualization Studies
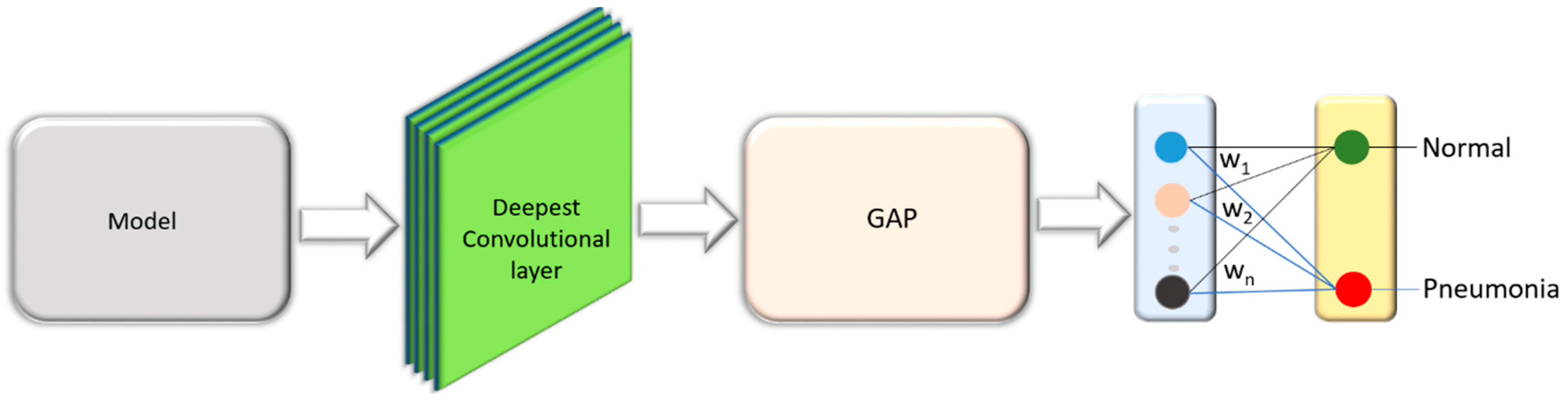
3.3.1. Visual Explanation through Discriminative Localization
3.3.2. Model-Agnostic Visual Explanations
4. Results and Discussion
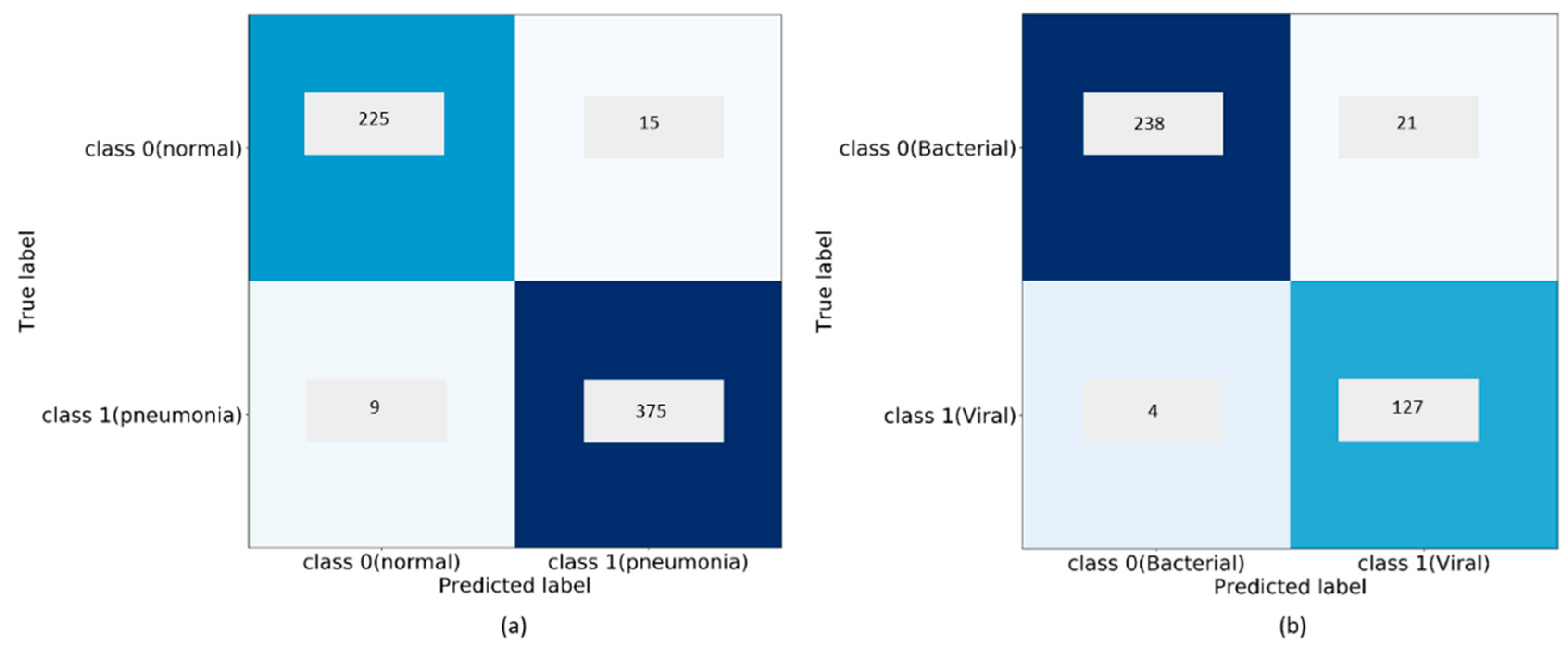
4.1. Performance Evaluation of Customized CNNs
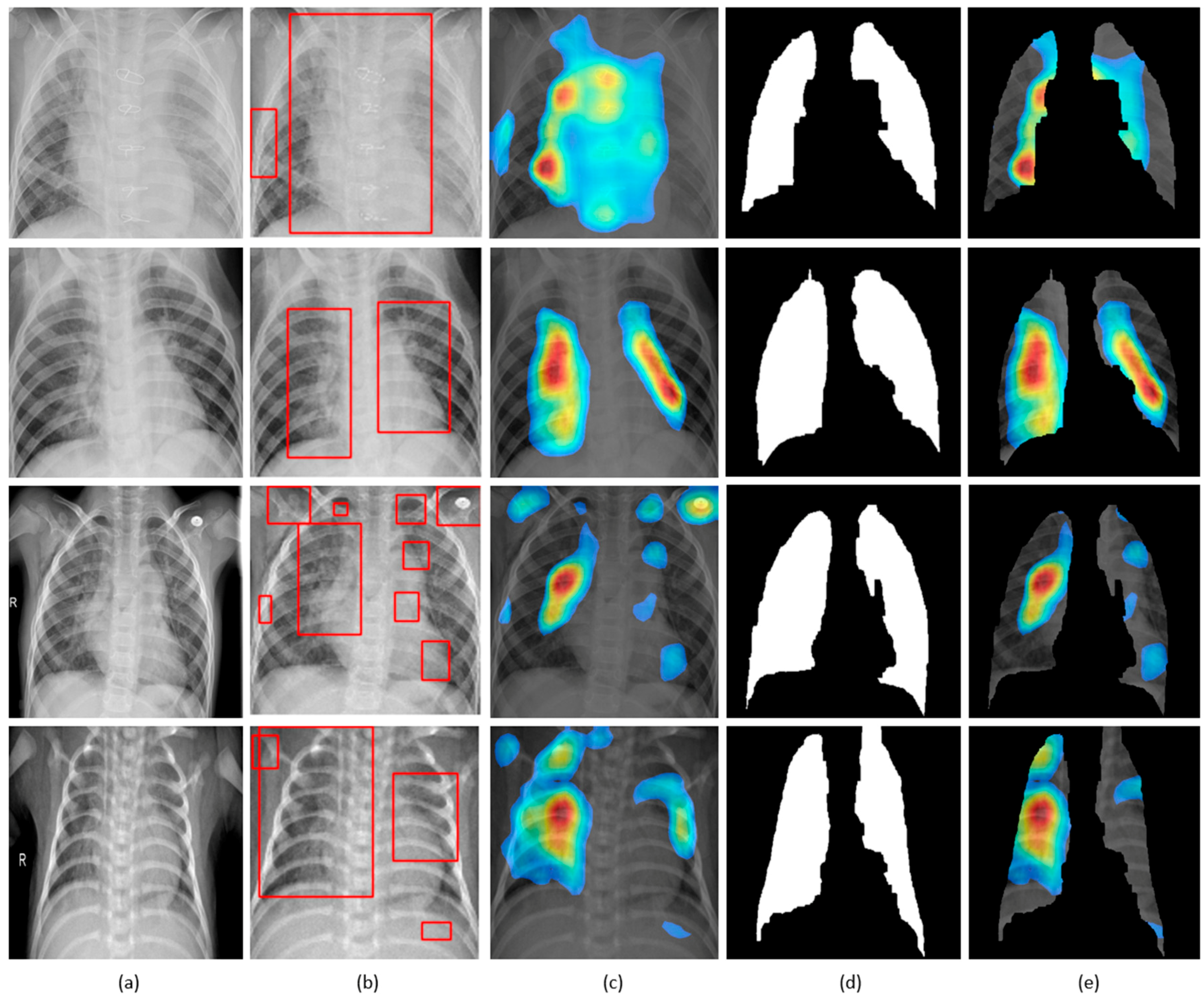
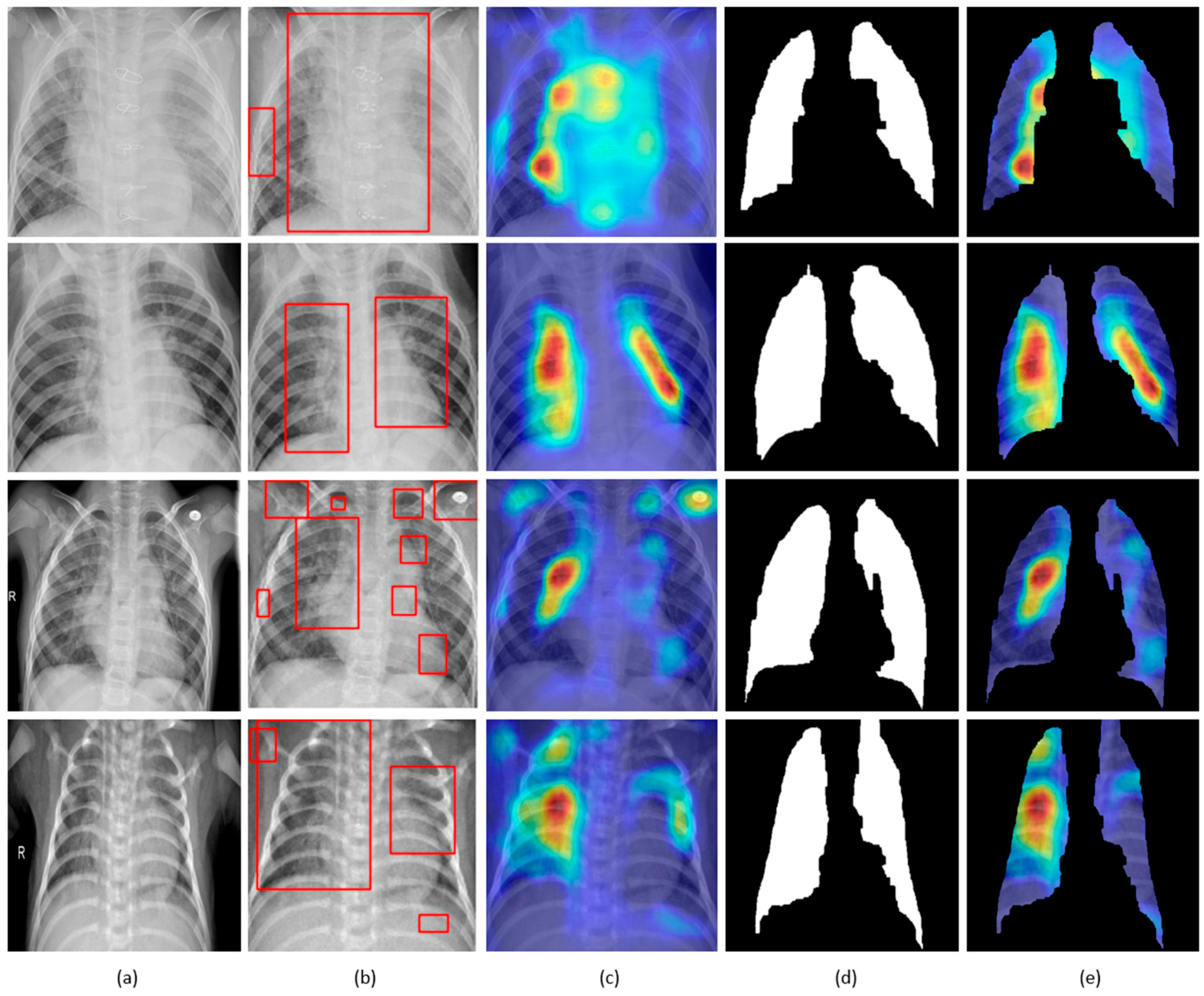
4.2. Visualization through Discriminative Localization
4.3. Visual Explanations with LIME
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Le Roux, D.M.; Myer, L.; Nicol, M.P. Incidence and severity of childhood pneumonia in the first year of life in a South African birth cohort: The Drakenstein Child Health Study. Lancet Glob. Health 2015, 3, e95–e103. [Google Scholar] [CrossRef]
- Mcluckie, A. Respiratory Disease and Its Management, 1st ed.; Springer: London, UK, 2009; pp. 51–59. ISBN 978-1-84882-094-4. [Google Scholar]
- Cherian, T.; Mulholland, E.K.; Carlin, J.B.; Ostensen, H.; Amin, R.; De Campo, M.; Greenberg, D.; Lagos, R.; Lucero, M.; Madhi, S.A.; et al. Standardized interpretation of paediatric chest radiographs for the diagnosis of pneumonia in epidemiological studies. Bull. World Health Organ. 2005, 83, 353–359. [Google Scholar] [PubMed]
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R.M. ChestX-Ray8: Hospital-Scale Chest X-Ray Database and Benchmarks on Weakly-Supervised Classification and Localization of Common Thorax Diseases. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 3462–3471. [Google Scholar]
- Karargyris, A.; Siegelman, J.; Tzortzis, D.; Jaeger, S.; Candemir, S.; Xue, Z.; KC, S.; Vajda, S.; Antani, S.K.; Folio, L.; et al. Combination of texture and shape features to detect pulmonary abnormalities in digital chest X-rays. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.I.; Lee, E.Y.; Bixby, S.; Diperna, S.; Hellinger, J.; Markowitz, R.; Servaes, S.; Monuteaux, M.C.; Shah, S.S. Variability in the Interpretation of Chest Radiographs for the Diagnosis of Pneumonia in Children. J. Hosp. Med. 2012, 7, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. In Proceedings of the Advances in Neural Information Processing Systems (NIPS), Lake Tahoe, NV, USA, 3–6 December 2012; pp. 1097–1105. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Li, F.F. ImageNet: A Large-Scale Hierarchical Image Database. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR), Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Zeiler, M.D.; Fergus, R. Visualizing and understanding convolutional networks. In Proceedings of the European Conference on Computer Vision (ECCV), Zurich, Switzerland, 6–12 September 2014; Springer: Cham, Switzerland, 2014; pp. 818–833. [Google Scholar]
- Bar, Y.; Diamant, I.; Wolf, L.; Lieberman, S.; Konen, E.; Greenspan, H. Chest Pathology Detection Using Deep Learning with Non-Medical Training. In Proceedings of the IEEE International Symposium on Biomedical Imaging (ISBI), Brooklyn, NY, USA, 16–19 April 2015; pp. 294–297. [Google Scholar]
- Oliveira, L.L.G.; Silva, S.A.E.; Ribeiro, L.H.V.; De Oliveira, R.M.; Coelho, C.J.; Ana Lúcia, A.L.S. Computer-Aided Diagnosis in Chest Radiography for Detection of Childhood Pneumonia. Int. J. Med. Inform. 2008, 77, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Abe, H.; Macmahon, H.; Shiraishi, J.; Li, Q.; Engelmann, R.; Doi, K. Computer-aided diagnosis in chest radiology. Semin. Ultrasound CT MR 2004, 25, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Giger, M.; MacMahon, H. Image processing and computer-aided diagnosis. Radiol. Clin. N. Am. 1996, 34, 565–596. [Google Scholar] [PubMed]
- Monnier-Cholley, L.; MacMahon, H.; Katsuragawa, S.; Morishita, J.; Ishida, T.; Doi, K. Computer-aided diagnosis for detection of interstitial opacities on chest radiographs. AJR Am. J. Roentgenol. 1998, 171, 1651–1656. [Google Scholar] [CrossRef] [PubMed]
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.S.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying Medical Diagnoses and Treatable Diseases by Image-Based Deep Learning. Cell 2018, 172, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. CheXNet: Radiologist-Level Pneumonia Detection on Chest X-Rays with Deep Learning. arXiv. 2018. Available online: https://arxiv.org/abs/1711.05225 (accessed on 23 January 2018).
- Guan, Q.; Huang, Y.; Zhong, Z.; Zheng, Z.; Zheng, L.; Yang, Y. Diagnose like a Radiologist: Attention Guided Convolutional Neural Network for Thorax Disease Classification. arXiv. 2018. Available online: https://arxiv.org/abs/1801.09927v1 (accessed on 17 June 2018).
- Candemir, S.; Jaeger, S.; Palaniappan, K.; Musco, J.P.; Singh, R.K.; Xue, Z.; Karargyris, A.; Antani, S.; Thoma, G.; McDonald, C.J. Lung Segmentation in Chest Radiographs Using Anatomical Atlases with Nonrigid Registration. IEEE Trans. Med. Imaging 2014, 33, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Candemir, S.; Antani, S.; Jaeger, S.; Browning, R.; Thoma, G. Lung Boundary Detection in Pediatric Chest X-Rays. In Proceedings of the SPIE Medical Imaging, Orlando, FL, USA, 21–26 February 2015; Volume 9418, p. 94180Q. [Google Scholar]
- Liu, C.; Yuen, J.; Torralba, A. SIFT Flow: Dense Correspondence across Scenes and Its Applications. IEEE Trans. Pattern Anal. Mach. Intell. 2011, 33, 978–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snoek, J.; Rippel, O.; Adams, R.P. Scalable Bayesian Optimization Using Deep Neural Networks. In Proceedings of the International Conference on Machine Learning (ICML), Lille, France, 6–11 July 2015; pp. 2171–2180. [Google Scholar]
- Deep Learning Using Bayesian Optimization. Available online: https://www.mathworks.com/help/nnet/examples/deep-learning-using-bayesian-optimization.html (accessed on 14 January 2018).
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. In Proceedings of the 3rd International Conference on Learning Representations (ICLR), San Diego, CA, USA, 7–9 May 2015; pp. 1–32. [Google Scholar]
- Bergstra, J.; Bengio, Y. Random Search for Hyper-Parameter Optimization. JMLR 2012, 13, 281–305. [Google Scholar]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning Deep Features for Discriminative Localization. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. In Proceedings of the IEEE International Conference of Computer Vision (ICCV), Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Ribeiro, M.T.; Singh, S.; Guestrin, C. “Why Should I Trust You?”: Explaining the Predictions of Any Classifier. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining (KDD), San Francisco, CA, USA, 13–17 August 2016; pp. 1135–1144. [Google Scholar]
- Sharma, S.; Maycher, B.; Eschun, G. Radiological imaging in pneumonia: Recent innovations. Curr. Opin. Pulm. Med. 2007, 13, 159–169. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Training Samples | Test Samples | File Type |
|---|---|---|---|
| Normal | 1349 | 234 | JPG |
| Bacterial | 2538 | 242 | JPG |
| Viral | 1345 | 148 | JPG |
| Model | Learning Rate | Momentum | L2 Regularization |
|---|---|---|---|
| Residual CNN | 1 × 10−3 | 0.9 | 1 × 10−6 |
| Inception CNN | 1 × 10−2 | 0.95 | 1 × 10−4 |
| Customized VGG16 | 1 × 10−4 | 0.99 | 1 × 10−6 |
| Task | Data | Models | Accuracy | AUC | Precision | Recall | Specificity | F-Score | MCC |
|---|---|---|---|---|---|---|---|---|---|
| Normal vs. Pneumonia | Baseline | Customized VGG16 | 0.957 | 0.990 | 0.951 | 0.983 | 0.915 | 0.967 | 0.908 |
| Sequential | 0.943 | 0.983 | 0.920 | 0.980 | 0.855 | 0.957 | 0.878 | ||
| Residual | 0.910 | 0.967 | 0.908 | 0.954 | 0.838 | 0.931 | 0.806 | ||
| Inception | 0.886 | 0.922 | 0.887 | 0.939 | 0.800 | 0.913 | 0.755 | ||
| Cropped ROI | Customized VGG16 | 0.962 | 0.993 | 0.977 | 0.962 | 0.962 | 0.970 | 0.918 | |
| Sequential | 0.941 | 0.984 | 0.930 | 0.995 | 0.877 | 0.955 | 0.873 | ||
| Residual | 0.917 | 0.971 | 0.913 | 0.959 | 0.847 | 0.936 | 0.820 | ||
| Inception | 0.897 | 0.932 | 0.896 | 0.947 | 0.817 | 0.921 | 0.778 | ||
| Bacterial vs. Viral Pneumonia | Baseline | Customized VGG16 | 0.936 | 0.962 | 0.920 | 0.984 | 0.860 | 0.951 | 0.862 |
| Sequential | 0.928 | 0.954 | 0.909 | 0.984 | 0.838 | 0.946 | 0.848 | ||
| Residual | 0.897 | 0.921 | 0.880 | 0.967 | 0.784 | 0.922 | 0.780 | ||
| Inception | 0.854 | 0.901 | 0.841 | 0.934 | 0.714 | 0.886 | 0.675 | ||
| Cropped ROI | Customized VGG16 | 0.936 | 0.962 | 0.920 | 0.984 | 0.860 | 0.951 | 0.862 | |
| Sequential | 0.928 | 0.956 | 0.909 | 0.984 | 0.838 | 0.946 | 0.848 | ||
| Residual | 0.908 | 0.933 | 0.888 | 0.976 | 0.798 | 0.930 | 0.802 | ||
| Inception | 0.872 | 0.919 | 0.853 | 0.959 | 0.730 | 0.903 | 0.725 | ||
| Normal vs. Bacterial vs. Viral Pneumonia | Baseline | Customized VGG16 | 0.917 | 0.938 | 0.917 | 0.905 | 0.958 | 0.911 | 0.873 |
| Sequential | 0.896 | 0.922 | 0.888 | 0.885 | 0.948 | 0.887 | 0.841 | ||
| Residual | 0.861 | 0.887 | 0.868 | 0.882 | 0.933 | 0.875 | 0.809 | ||
| Inception | 0.809 | 0.846 | 0.753 | 0.848 | 0.861 | 0.798 | 0.688 | ||
| Cropped ROI | Customized VGG16 | 0.918 | 0.939 | 0.920 | 0.900 | 0.960 | 0.910 | 0.876 | |
| Sequential | 0.897 | 0.923 | 0.898 | 0.898 | 0.949 | 0.898 | 0.844 | ||
| Residual | 0.879 | 0.909 | 0.883 | 0.890 | 0.941 | 0.887 | 0.825 | ||
| Inception | 0.821 | 0.865 | 0.778 | 0.855 | 0.878 | 0.815 | 0.714 |
| Task | Model | Accuracy | AUC | Precision | Recall | Specificity | F-Score | MCC |
|---|---|---|---|---|---|---|---|---|
| Normal v. Pneumonia | Customized VGG16 | 0.962 | 0.993 | 0.977 | 0.962 | 0.962 | 0.970 | 0.918 |
| Kermany et al. | 0.928 | 0.968 | - | 0.932 | 0.901 | - | - | |
| Bacterial v. Viral Pneumonia | Customized VGG16 | 0.936 | 0.962 | 0.920 | 0.984 | 0.860 | 0.951 | 0.862 |
| Kermany et al. | 0.907 | 0.940 | - | 0.886 | 0.909 | - | - | |
| Normal v. Bacterial v. Viral Pneumonia | Customized VGG16 | 0.918 | 0.939 | 0.920 | 0.900 | 0.960 | 0.910 | 0.876 |
| Kermany et al. | - | - | - | - | - | - | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajaraman, S.; Candemir, S.; Kim, I.; Thoma, G.; Antani, S. Visualization and Interpretation of Convolutional Neural Network Predictions in Detecting Pneumonia in Pediatric Chest Radiographs. Appl. Sci. 2018, 8, 1715. https://doi.org/10.3390/app8101715
Rajaraman S, Candemir S, Kim I, Thoma G, Antani S. Visualization and Interpretation of Convolutional Neural Network Predictions in Detecting Pneumonia in Pediatric Chest Radiographs. Applied Sciences. 2018; 8(10):1715. https://doi.org/10.3390/app8101715
Chicago/Turabian StyleRajaraman, Sivaramakrishnan, Sema Candemir, Incheol Kim, George Thoma, and Sameer Antani. 2018. "Visualization and Interpretation of Convolutional Neural Network Predictions in Detecting Pneumonia in Pediatric Chest Radiographs" Applied Sciences 8, no. 10: 1715. https://doi.org/10.3390/app8101715
APA StyleRajaraman, S., Candemir, S., Kim, I., Thoma, G., & Antani, S. (2018). Visualization and Interpretation of Convolutional Neural Network Predictions in Detecting Pneumonia in Pediatric Chest Radiographs. Applied Sciences, 8(10), 1715. https://doi.org/10.3390/app8101715