Rehabilitative Ultrasound Imaging Evaluation in Physiotherapy: Piloting a Systematic Review

 ,
,  ,
,  and
and
Abstract
:Featured Application
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search
2.5. Study Selection
2.6. Data Collection Process
2.7. Risk of Bias in Individual Studies
2.8. Synthesis of Results
2.9. Additional Analyses
2.10. Ethical Considerations
3. Results
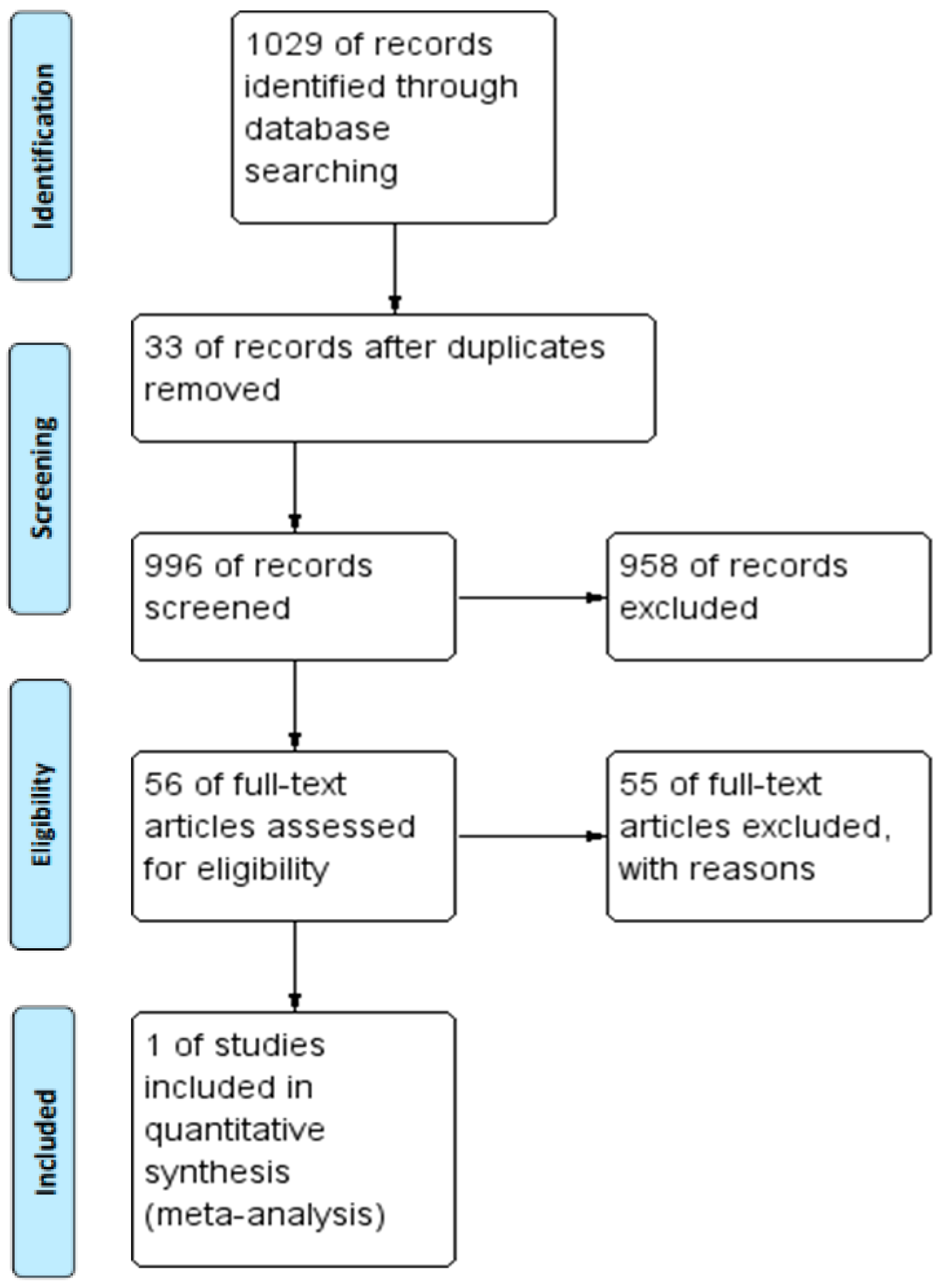
3.1. Study Selection
3.2. Study Characteristics
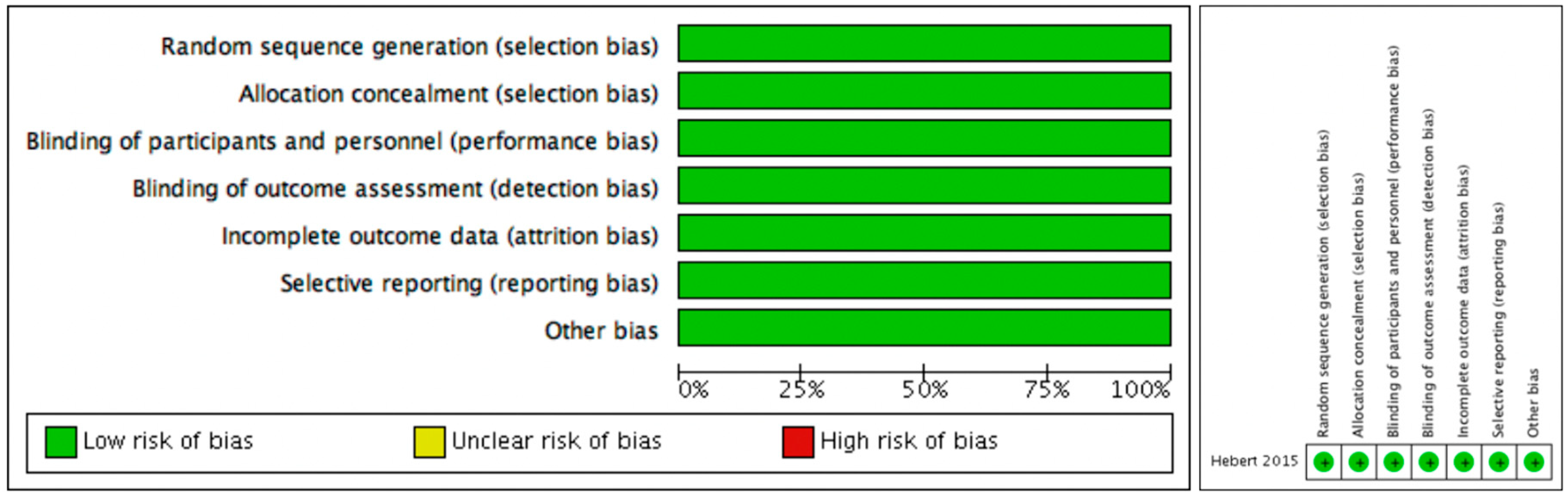
3.3. Risk of Bias within Studies
3.4. Additional Analysis
4. Discussion
4.1. Summary of Evidence
4.2. Case Control Studies
4.3. Case Report
4.4. Cohort Studies
4.5. Observational Studies
4.6. Validity and Reliability Studies
4.7. Future Studies
5. Conclusions
Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BOS | Base of support |
| EMG | Electromyography |
| ICC | Intraclass Correlation Coefficient |
| ISEAPT | International Society for Electrophysical Agents in Physical Therapy |
| MRI | Magnetic Resonance Imaging |
| MESH | Medical Subjects Headings |
| PROSPERO | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCT | Randomized Clinical Trial |
| RUSI | Rehabilitative Ultrasound Imagine |
| US | Ultrasound |
| VAS | Visual Analogue Scale |
| WCPT | World Confederation for Physical Therapy |
References
- Ikai, M.; Fukunaga, T. Calculation of muscle strength per unit cross-sectional area of human muscle by means of ultrasonic measurement. Eur. J. Appl. Physiol. 1968, 26, 26–32. [Google Scholar] [CrossRef]
- Huang, Q.; Zhang, Y.; Li, D.; Yang, D.; Huo, M.; Maruyama, H. The Evaluation of Chronic Low Back Pain by Determining the Ratio of the Lumbar Multifidus Muscle Cross-sectional Areas of the Unaffected and Affected Sides. J. Phys. Ther. Sci. 2014, 26, 1613–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teyhen, D. Rehabilitative Ultrasound Imaging Symposium San Antonio, TX, 8–10 May 2006. J. Orthop. Sports Phys. Ther. 2006, 36, A1–A3. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Carnero, S.; Calvo-Lobo, C.; Garrido-Marin, A.; Arias-Buría, J.L. 2nd Rehabilitative Ultrasound Imaging Symposium in Physiotherapy—Madrid, Spain, 3–5 June 2016. Br. J. Sports Med. 2018, 52, A1. [Google Scholar]
- Woolf, A.D. Bone and Joint Decade report: Moving together beyond the decade. Preface. Best Pract. Res. Clin. Rheumatol. 2012, 26, 167–168. [Google Scholar] [CrossRef]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56 (Suppl. 2), S243–S255. [Google Scholar] [CrossRef]
- Djordjevic, O.; Djordjevic, A.; Konstantinovic, L. Interrater and intrarater reliability of transverse abdominal and lumbar multifidus muscle thickness in subjects with and without low back pain. J. Orthop. Sports Phys. Ther. 2014, 44, 979–988. [Google Scholar] [CrossRef]
- Hides, J.A.; Richardson, C.A.; Jull, G.A. Magnetic resonance imaging and ultrasonography of the lumbar multifidus muscle: Comparison of two different modalities. Spine 1995, 20, 54–58. [Google Scholar] [CrossRef]
- Storheim, K.; Bø, K.; Pederstad, O.; Jahnsen, R. Intra-tester reproducibility of pressure biofeedback in measurement of transversus abdominis function. Physiother. Res. Int. 2002, 7, 239–249. [Google Scholar] [CrossRef]
- Kidd, A.W.; Magee, S.; Richardson, C.A. Reliability of real-time ultrasound for the assessment of transversus abdominis function. J. Gravit. Physiol. 2002, 9, P131–P132. [Google Scholar]
- Dankaerts, W.; O’Sullivan, P.B.; Burnett, A.F.; Straker, L.M.; Danneels, L.A. Reliability of EMG measurements for trunk muscles during maximal and sub-maximal voluntary isometric contractions in healthy controls and CLBP patients. J. Electromyogr. Kinesiol. 2004, 14, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Teyhen, D.S. Reliability of ultrasound imaging to measure muscle thickness of the lateral abdominal muscles. J. Orthop. Sports Phys. Ther. 2006, 36, A-8–A-9. [Google Scholar]
- O’Sullivan, C.; Bentman, S.; Bennett, K.; Stokes, M. Rehabilitative ultrasound imaging of the lower trapezius muscle: Technical description and reliability. J. Orthop. Sports Phys. Ther. 2007, 37, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.A.; Miokovic, T.; Belavy, D.L.; Stanton, W.R.; Richardson, C.A. Ultrasound imaging assessment of abdominal muscle function during drawing-in of the abdominal wall: An intrarater reliability study. J. Orthop. Sports Phys. Ther. 2007, 37, 480–486. [Google Scholar] [CrossRef]
- Wallwork, T.L.; Hides, J.A.; Stanton, W.R. Intrarater and interrater reliability of assessment of lumbar multifidus muscle thickness using rehabilitative ultrasound imaging. J. Orthop. Sports Phys. Ther. 2007, 37, 608–612. [Google Scholar] [CrossRef]
- Ellis, R.; Hing, W.; Dilley, A.; McNair, P. Reliability of measuring sciatic and tibial nerve movement with diagnostic ultrasound during a neural mobilisation technique. Ultrasound Med. Biol. 2008, 34, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Koppenhaver, S.L.; Hebert, J.J.; Fritz, J.M.; Parent, E.C.; Teyhen, D.S.; Magel, J.S. Original article: Reliability of Rehabilitative Ultrasound Imaging of the Transversus Abdominis and Lumbar Multifidus Muscles. Arch. Phys. Med. Rehabil. 2009, 90, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.J.; Chai, H.M.; Wang, S.F. Reliability of thickness measurements of the dorsal muscles of the upper cervical spine: An ultrasonographic study. J. Orthop. Sports Phys. Ther. 2009, 39, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Cagnie, B.; Derese, E.; Vandamme, L.; Verstraete, K.; Cambier, D.; Danneels, L. Original Article: Validity and reliability of ultrasonography for the longus colli in asymptomatic subjects. Man. Ther. 2009, 14, 421–426. [Google Scholar] [CrossRef]
- Abiko, T.; Takei, H.; Shimamura, R.; Abiko, Y.; Yamamoto, J.; Sakasai, T.; Soma, M.; Ogawa, D.; Yamaguchi, T.; Hata, M. Reliability of Rehabilitative Ultrasound Imaging of the Lumbar Multifidus. Rigakuryoho Kagaku 2011, 26, 693–697. [Google Scholar] [CrossRef] [Green Version]
- Gnat, R.; Saulicz, E.; Miądowicz, B. Reliability of real-time ultrasound measurement of transversus abdominis thickness in healthy trained subjects. Eur. Spine J. 2012, 21, 1508–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, P.O.d.P.; de Oliveira, R.R.; de Moura Filho, A.G.; Raposo, M.C.F.; Costa, L.O.P.; Laurentino, G.E.C. Reliability Study: Reproducibility of the pressure biofeedback unit in measuring transversus abdominis muscle activity in patients with chronic nonspecific low back pain. J. Bodyw. Mov. Ther. 2012, 16, 251–257. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.L.; Watson, T. Reproducibility of ultrasound measurement of transversus abdominis during loaded, functional tasks in asymptomatic young adults. PM&R 2012, 4, 402–412. [Google Scholar]
- Wong, A.Y.L.; Parent, E.C.; Kawchuk, G.N. Reliability of 2 ultrasonic imaging analysis methods in quantifying lumbar multifidus thickness. J. Orthop. Sports Phys. Ther. 2013, 43, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Linek, P.; Saulicz, E.; Wolny, T.; Myśliwiec, A. Reliability of B-mode sonography of the abdominal muscles in healthy adolescents in different body positions. J. Ultrasound Med. 2014, 33, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Tahan, N.; Rasouli, O.; Arab, A.M.; Khademi, K.; Samani, E.N. Reliability of the ultrasound measurements of abdominal muscles activity when activated with and without pelvic floor muscles contraction. J. Back Musculoskelet. Rehabil. 2014, 27, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.-H.; Park, D.-J. Reliability of ultrasound in combination with surface electromyogram for evaluating the activity of abdominal muscles in individuals with and without low back pain. J. Exerc. Rehabil. 2014, 10, 230–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneebeli, A.; Egloff, M.; Giampietro, A.; Clijsen, R.; Barbero, M. Rehabilitative ultrasound imaging of the supraspinatus muscle: Intra- and interrater reliability of thickness and cross-sectional area. J. Bodyw. Mov. Ther. 2014, 18, 266–272. [Google Scholar] [CrossRef]
- Talbott, N.R.; Witt, D.W. Ultrasound examination of the serratus anterior during scapular protraction in asymptomatic individuals: Reliability and changes with contraction. PM&R 2014, 6, 227–234. [Google Scholar]
- Yang, H.S.; Yoo, J.W.; Lee, B.A.; Choi, C.K.; You, J.H. Inter-tester and intra-tester reliability of ultrasound imaging measurements of abdominal muscles in adolescents with and without idiopathic scoliosis: A case-controlled study. Bio.-Med. Mater. Eng. 2014, 24, 453–458. [Google Scholar]
- Chen, Y.-H.; Chai, H.-M.; Yang, J.-L.; Lin, Y.-J.; Wang, S.-F. Original Article: Reliability and Validity of Transversus Abdominis Measurement at the Posterior Muscle-Fascia Junction with Ultrasonography in Asymptomatic Participants. J. Manip. Physiol. Ther. 2015, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Keshwani, N.; Mathur, S.; McLean, L. Validity of Inter-rectus Distance Measurement in Postpartum Women Using Extended Field-of-View Ultrasound Imaging Techniques. J. Orthop. Sports Phys. Ther. 2015, 45, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Koppenhaver, S.; Harris, D.; Harris, A.; O’Connor, E.; Dummar, M.; Croy, T.; Walker, M.; Flynn, T. The reliability of rehabilitative ultrasound imaging in the measurement of infraspinatus muscle function in the symptomatic and asymptomatic shoulders of patients with unilateral shoulder impingement syndrome. Int. J. Sports Phys. Ther. 2015, 10, 128–135. [Google Scholar]
- Sobczak, S.; Dugailly, P.-M.; Gilbert, K.K.; Hooper, T.L.; Sizer, P.S., Jr.; James, C.R.; Poortmans, B.; Matthijs, O.C.; Brismée, J.-M. Reliability and validation of in vitro lumbar spine height measurements using musculoskeletal ultrasound: A preliminary investigation. J. Back Musculoskelet. Rehabil. 2016, 29, 171–182. [Google Scholar] [CrossRef]
- Ludwig, O.; Hammes, A.; Kelm, J.; Schmitt, E. Validity & reliability study: Assessment of the posture of adolescents in everyday clinical practice: Intra-rater and inter-rater reliability and validity of a posture index. J. Bodyw. Mov. Ther. 2016, 20, 761–766. [Google Scholar]
- Salavati, M.; Akhbari, B.; Takamjani, I.E.; Ezzati, K.; Haghighatkhah, H. Reliability of the Upper trapezius Muscle and Fascia Thickness and Strain Ratio Measures by Ultrasonography and Sonoelastography in Subjects with Myofascial Pain Syndrome. J. Chiropr. Med. 2017, 16, 316–323. [Google Scholar] [CrossRef] [PubMed]
- History World Confederation for Physical Therapy. Available online: https://www.wcpt.org/iseapt/about (accessed on 7 December 2018).
- Koppenhaver, S.L.; Hebert, J.J.; Parent, E.C.; Fritz, J.M. Rehabilitative ultrasound imaging is a valid measure of trunk muscle size and activation during most isometric sub-maximal contractions: A systematic review. Aust. J. Physiother. 2009, 55, 153–169. [Google Scholar] [CrossRef]
- Hebert, J.J.; Koppenhaver, S.L.; Parent, E.C.; Fritz, J.M. A systematic review of the reliability of rehabilitative ultrasound imaging for the quantitative assessment of the abdominal and lumbar trunk muscles. Spine 2009, 34, E848–E856. [Google Scholar] [CrossRef]
- The-Cochrane-Collaboration. Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration. 2014. Available online: https://www.cochrane.org/es/2017/about-us/citing-our-products (accessed on 7 December 2018).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Hodges, P.W. Ultrasound imaging in rehabilitation: Just a fad? J. Orthop. Sports Phys. Ther. 2005, 35, 333–337. [Google Scholar] [CrossRef]
- Sweeney, N.; O’Sullivan, C.; Kelly, G. Multifidus muscle size and percentage thickness changes among patients with unilateral chronic low back pain (CLBP) and healthy controls in prone and standing. Man. Ther. 2014, 19, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Wang-Price, S.; Zafereo, J.; Brizzolara, K.; Sokolowski, L.; Turner, D. Effects of different verbal instructions on change of lumbar multifidus muscle thickness in asymptomatic adults and in patients with low back pain. J. Man. Manip. Ther. 2017, 25, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.A.; Lambrecht, G.; Stanton, W.R.; Damann, V. Changes in multifidus and abdominal muscle size in response to microgravity: Possible implications for low back pain research. Eur. Spine J. 2016, 25 (Suppl. 1), S175–S182. [Google Scholar] [CrossRef]
- Koppenhaver, S.L.; Fritz, J.M.; Hebert, J.J.; Kawchuk, G.N.; Parent, E.C.; Gill, N.W.; Childs, J.D.; Teyhen, D.S. Association between history and physical examination factors and change in lumbar multifidus muscle thickness after spinal manipulation in patients with low back pain. J. Electromyogr. Kinesiol. 2012, 22, 724–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zielinski, K.A.; Henry, S.M.; Ouellette-Morton, R.H.; DeSarno, M.J. Lumbar Multifidus Muscle Thickness Does Not Predict Patients With Low Back Pain Who Improve With Trunk Stabilization Exercises. Arch. Phys. Med. Rehabil. 2013, 94, 1132–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debuse, D.; Birch, O.; St Clair Gibson, A.; Caplan, N. Low impact weight-bearing exercise in an upright posture increases the activation of two key local muscles of the lumbo-pelvic region. Physiother. Theory Pract. 2013, 29, 51–60. [Google Scholar] [CrossRef]
- Maraschin, M.; Ferrari, S.; Cacciatori, C. The effect of functional stabilization training on the cross sectional area of the deep stabilizers muscles in healthcare workers with chronic low back pain: A pilot study. Sci. Riabil. 2014, 16, 12–21. [Google Scholar]
- Joseph, L.H.; Hussain, R.I.; Naicker, A.S.; Ohnmar, H.; Ubon, P.; Aatit, P. Pattern of changes in local and global muscle thickness among individuals with sacroiliac joint dysfunction. Hong Kong Physiother. J. 2015, 33, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Masaki, M.; Ikezoe, T.; Fukumoto, Y.; Minami, S.; Aoyama, J.; Ibuki, S.; Kimura, M.; Ichihashi, N. Association of walking speed with sagittal spinal alignment, muscle thickness, and echo intensity of lumbar back muscles in middle-aged and elderly women. Aging Clin. Exp. Res. 2016, 28, 429–434. [Google Scholar] [CrossRef]
- MacKenzie, J.F.; Grimshaw, P.N.; Jones, C.D.S.; Thoirs, K.; Petkov, J. Muscle activity during lifting: Examining the effect of core conditioning of multifidus and transversus abdominis. Work 2014, 47, 453–462. [Google Scholar]
- Kim, C.-Y.; Choi, J.-D.; Kim, S.-Y.; Oh, D.-W.; Kim, J.-K.; Park, J.-W. Comparison between muscle activation measured by electromyography and muscle thickness measured using ultrasonography for effective muscle assessment. J. Electromyogr. Kinesiol. 2014, 24, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Li, D.; Zhang, Y.; Hu, A.; Huo, M.; Maruyama, H. The Reliability of Rehabilitative Ultrasound Imaging of the Cross-sectional Area of the Lumbar Multifidus Muscles in the PNF Pattern. J. Phys. Ther. Sci. 2014, 26, 1539–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sions, J.M.; Velasco, T.O.; Teyhen, D.S.; Hicks, G.E. Ultrasound imaging: Intraexaminer and interexaminer reliability for multifidus muscle thickness assessment in adults aged 60 to 85 years versus younger adults. J. Orthop. Sports Phys. Ther. 2014, 44, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Liu, I.S.; Chai, H.M.; Yang, J.L.; Wang, S.F. Inter-session reliability of the measurement of the deep and superficial layer of lumbar multifidus in young asymptomatic people and patients with low back pain using ultrasonography. Man. Ther. 2013, 18, 481–486. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Allocation: Randomized using a number generator. Duration: 6 months follow up. Setting: Patients from academic and private neurological and orthopedic spine surgery practices in Salt Lake City, Utah, USA. |
| Participants | Diagnosis: Post-discectomy surgery. N = 61 Age: Average age Sex: Male and Female. Inclusion: Age 18–60 years, presurgical radiographic confirmation of lumbar disc herniation through MRI or CT and scheduled to undergo single-level lumbar discectomy. Exclusion: Prior lumbar spine surgery, surgery at more than one level, a surgical procedure other than discectomy (e.g., fusion) or perioperative complications representing a contraindication to exercise. |
| Interventions | * Group 1: General trunk exercise protocol (GEN) N = 32. This protocol comprised three components: (1) aerobic exercise, (2) range of motion exercise and (3) strengthening exercise. * Group 2: Specific trunk exercise protocol (SPEC) N = 29. The SPEC included all components of the GEN. In addition, participants performed specific trunk muscle exercises similar to protocols used to treat patients with non-specific, non-surgical low back pain. This approach also included similar contractions of the transversus abdominis (TrA) using the abdominal drawing-in maneuver. Once these skills were acquired and confirmed by the physical therapist through palpation and/or ultrasound imaging, participants were instructed to perform isometric TrA and LM cocontractions. During the supervised exercise sessions, tactile and visual feedback through palpation and real-time ultrasound imaging were used to enhance skill acquisition and the treating physical therapists used this information to ensure appropriate technique. |
| Outcomes | -Low back pain-related disability: Oswestry Disability Questionnaire (OSW). -Low back and lower extremity pain: Numeric Pain Rating Scale. 30–32 Global rating of change (GRC) was assessed with a 15-point Likert-type scale ranging from −7 (“a very great deal worse”) to 0 (“about the same”) to +7 (“a very great deal better”). -Sciatica frequency and bothersomeness were estimated using the Sciatica Frequency and Sciatica Bothersomeness indices resulting in possible scores of 0–25.34 -Muscle function was assessed using brightness-mode, real-time ultrasound images of LM thickness |
| Notes |
| Bias | Authors’ Judgement | Support for Judgement |
|---|---|---|
| Random sequence generation (selection bias) | Low risk | A random number generator was used to create a permuted block randomization list with variable block sizes of 4–6. |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered, opaque envelopes containing the participant’s group assignment were prepared by research staff not affiliated with this trial. |
| Blinding of participants and personnel (performance bias) | Low risk | The envelope was opened after the 2-week postoperative assessment by the treating physical therapist. Group assignments were concealed from participants and outcome assessors. |
| Blinding of outcome assessment (detection bias) | Low risk | The envelope was opened after the 2-week postoperative assessment by the treating physical therapist. Group assignments were concealed from participants and outcome assessors. |
| Incomplete outcome data (attrition bias) | Low risk | There were significant main effects of time (p < 0.01) indicating improvements from baseline in disability, pain, sciatica frequency, sciatica bothersomeness, and LM function (Table 3 and Figure 2). |
| Selective reporting (reporting bias) | Low risk | The results of the intention-to-treat analyses revealed no time by group interactions. There were no statistically significant or clinically important between-group differences in disability, pain, global change, sciatica frequency, sciatica bothersomeness or LM muscle function at 10 weeks or 6 months (Table 3 and Figure 2). |
| Other bias | Low risk | None. |
| Reference | ICC | Intra-Rater | Inter-Rater |
|---|---|---|---|
| Wong et al. 2013 | 0.99 | 0.99–0.98 | |
| Liu et al. 2013 | 0.84–1.00 | ||
| Sions et al. 2014 (older) | 0.78–0.95 | 0.74–0.94 | |
| Sions et al. 2014 (younger) | 0.87–0.97 | 0.80–0.95 | |
| Djordevic et al. 2014 | 0.99–1.00 | 0.99–1.00 | |
| Huang et al. 2016 | 0.93–0.99 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández Carnero, S.; Arias Buria, J.L.; Cuenca Zaldivar, J.N.; Leal Quiñones, A.; Calvo-Lobo, C.; Martin Saborido, C. Rehabilitative Ultrasound Imaging Evaluation in Physiotherapy: Piloting a Systematic Review. Appl. Sci. 2019, 9, 181. https://doi.org/10.3390/app9010181
Fernández Carnero S, Arias Buria JL, Cuenca Zaldivar JN, Leal Quiñones A, Calvo-Lobo C, Martin Saborido C. Rehabilitative Ultrasound Imaging Evaluation in Physiotherapy: Piloting a Systematic Review. Applied Sciences. 2019; 9(1):181. https://doi.org/10.3390/app9010181
Chicago/Turabian StyleFernández Carnero, Samuel, José Luis Arias Buria, Juan Nicolás Cuenca Zaldivar, Alejandro Leal Quiñones, Cesar Calvo-Lobo, and Carlos Martin Saborido. 2019. "Rehabilitative Ultrasound Imaging Evaluation in Physiotherapy: Piloting a Systematic Review" Applied Sciences 9, no. 1: 181. https://doi.org/10.3390/app9010181
APA StyleFernández Carnero, S., Arias Buria, J. L., Cuenca Zaldivar, J. N., Leal Quiñones, A., Calvo-Lobo, C., & Martin Saborido, C. (2019). Rehabilitative Ultrasound Imaging Evaluation in Physiotherapy: Piloting a Systematic Review. Applied Sciences, 9(1), 181. https://doi.org/10.3390/app9010181