Effects of the Whole-Body Vibration and Auriculotherapy on the Functionality of Knee Osteoarthritis Individuals

 , ,
, ,  ,
,  ,
,  and
and 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Sample Size
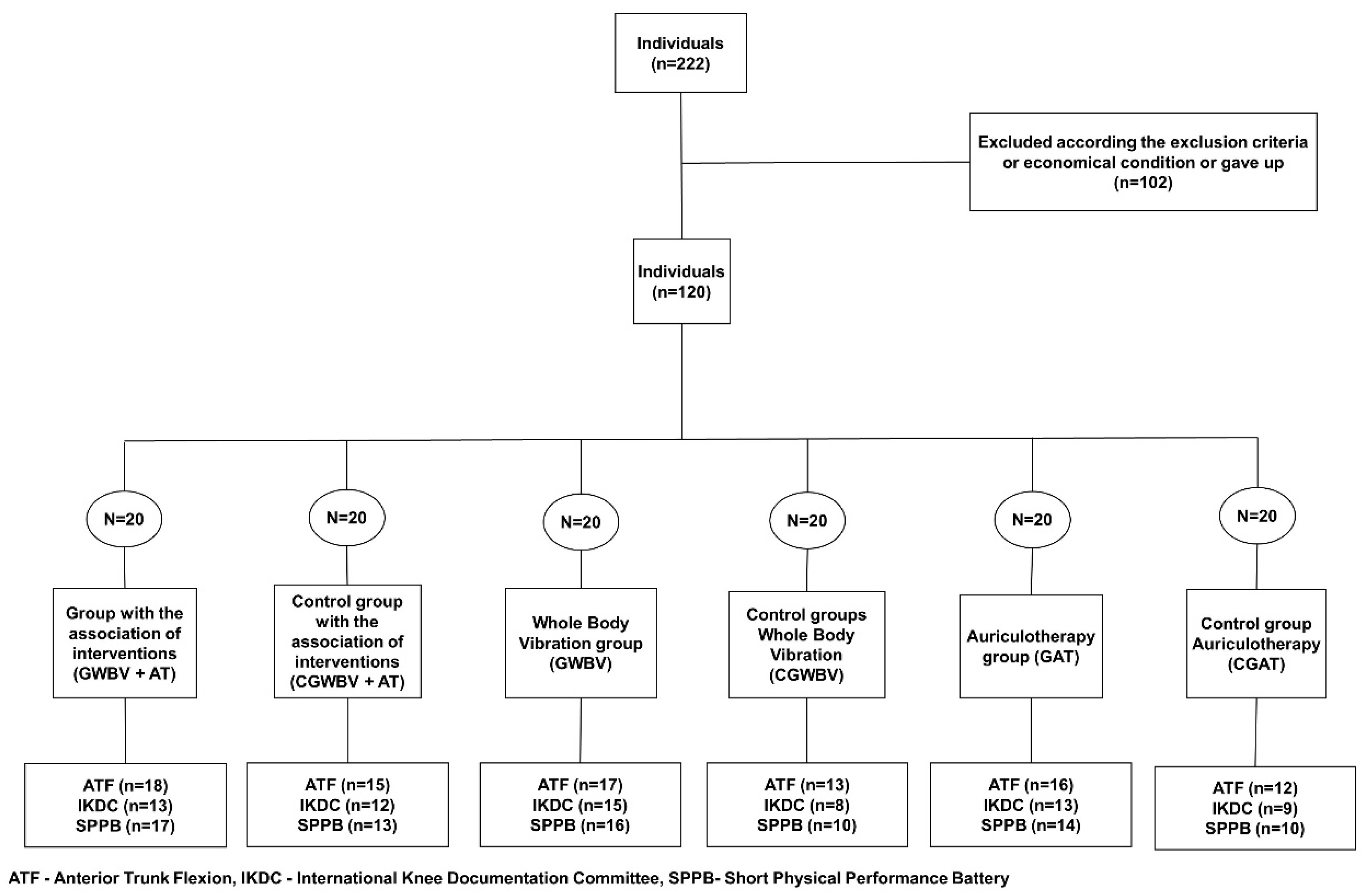
2.4. Participants
2.5. Whole-Body Vibration Intervention
2.6. Auricular Intervention
3. Primary Outcome Measures
3.1. Anterior Trunk Flexion (ATF)
3.2. International Knee Documentation Committee
3.3. Short Physical Performance Battery (SPPB)
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Dulay, G.S.; Cooper, C.; Dennison, E.M. Knee pain, knee injury, knee osteoarthritis & work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 454–461. [Google Scholar] [PubMed]
- Ferreira, R.; Duarte, J.; Gonçalves, R. Non-pharmacological and non-surgical interventions to manage patients with knee osteoarthritis: An umbrella review. Acta Reumatol. Port. 2018, 43, 182–200. [Google Scholar] [PubMed]
- Zhang, W.; Moskowitz, R.W.; Nuki, G.; Abramson, S.; Altman, R.D.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr. Cartil. 2008, 16, 137–162. [Google Scholar] [CrossRef]
- Neto, S.B.S.; Marconi, E.M.; Kutter, C.R.; Frederico, E.H.F.F.; de Paiva, P.d.C.; Meyer, P.F.; Chang, S.; Sá-Caputo, D.; Bernardo-Filho, M. Beneficial effects of whole body mechanical vibration alone or combined with auriculotherapy in the pain and in flexion of knee of individuals with knee osteoarthritis. Acupunct. Electrother. Res. 2017, 42, 185–201. [Google Scholar] [CrossRef]
- ACR. ACR OA Guidelines Non-Pharmacological—Knee and Hip; American College of Rheumatology: Chicago, IL, USA, 2009; pp. 4–30. [Google Scholar]
- Allen, K.D.; Bierma-Zeinstra, S.M.A.; Foster, N.E.; Golightly, Y.M.; Hawker, G. OARSI Clinical Trials Recommendations: Design and conduct ofimplementation trials of interventions for osteoarthritis. Osteoarthr. Cartil. 2015, 23, 826–838. [Google Scholar] [CrossRef]
- Asher, G.N.; Jonas, D.E.; Coeytaux, R.R.; Reilly, A.C.; Loh, Y.L.; Motsinger-Reif, A.A.; Winham, S.J. Auriculotherapy for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Altern. Complement. Med. 2010, 16, 1097–1108. [Google Scholar] [CrossRef]
- Hou, P.W.; Hsu, H.C.; Lin, Y.W.; Tang, N.Y.; Cheng, C.Y.; Hsieh, C.L. The history, mechanism, and clinical application of auricular therapy in traditional Chinese medicine. Evid.-Based Complement. Altern. Med. 2015, 2015, 495684. [Google Scholar] [CrossRef]
- Huang, L. Auricular Medicine: A Complete Manual of Auricular Diagnosis and Treatment; Auricular International Research and Training: Orlando, FL, USA, 2005. [Google Scholar]
- Rabischong, P.; Terral, C. Scientific Basis of Auriculotherapy: State of the Art. Med. Acupunct. 2014, 26, 84–96. [Google Scholar] [CrossRef]
- Suen, L.K.P.; Wong, T.K.S.; Leung, A.W.N. Is there a place for auricular therapy in the realm of nursing? Complement. Ther. Nurs. Midwifery 2001, 7, 132–139. [Google Scholar] [CrossRef]
- Suen, L.K.P.; Yeh, C.H.; Yeung, S.K.W. Erratum to Using auriculotherapy for osteoarthritic knee among elders: A double-blinded randomised feasibility study. BMC Complement. Altern. Med. 2016, 16, 257. [Google Scholar] [CrossRef] [PubMed]
- Round, R.; Litscher, G.; Bahr, F. Auricular acupuncture with laser. Evid.-Based Complement. Altern. Med. 2013, 2013, 984763. [Google Scholar] [CrossRef] [PubMed]
- Rubach, A. Principles of Ear Acupuncture-Microsystem of the Auricle: Microsystem of the Auricle, 2nd ed.; Thieme Publishers: Stuttgart, Germany, 2001. [Google Scholar]
- Gori, L.; Firenzuoli, F. Ear acupuncture in European traditional medicine. Evid.-Based Complement. Altern. Med. 2007, 4, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Suen, L.K.P.; Wong, T.K.S.; Leung, A.W.N. Auricular therapy using magnetic pearls on sleep: A standardized protocol for the elderly with insomnia. Clin. Acupunct. Orient. Med. 2002, 3, 39–50. [Google Scholar] [CrossRef]
- Alimi, D.; Rubino, C.; Pichard-Léandri, E.; Fermand-Brulé, S.; Dubreuil-Lemaire, M.L.; Hill, C. Analgesic effect of auricular acupuncture for cancer pain: A randomized, blinded, controlled trial. J. Clin. Oncol. 2003, 21, 4120–4126. [Google Scholar] [CrossRef]
- Usichenko, T.I.; Dinse, M.; Hermsen, M.; Witstruck, T.; Pavlovic, D.; Lehmann, C. Auricular acupuncture for pain relief after total hip arthroplasty—A randomized controlled study. Pain 2005, 114, 320–327. [Google Scholar] [CrossRef]
- Sitjà-Rabert, M.; Rigau, D.; Fort Vanmeerghaeghe, A.; Romero-Rodríguez, D.; Bonastre Subirana, M.; Bonfill, X. Efficacy of whole body vibration exercise in older people: A systematic review. Disabil. Rehabil. 2012, 34, 883–893. [Google Scholar] [CrossRef]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef]
- Rauch, F.; Sievanen, H.; Boonen, S.; Cardinale, M.; Degens, H.; Felsenberg, D.; Roth, J.; Schoenau, E.; Verschueren, S.; Rittweger, J. Reporting whole-body vibration intervention studies: Recommendations of the International Society of Musculoskeletal and Neuronal Interactions. J. Musculoskelet. Neuronal Interact. 2010, 10, 193–198. [Google Scholar]
- da Costa, P.R.; da Cunha S&a-Caputo, D.U.; Arn&obio, A.; Pacheco, R.; Kutter, C.; Costa, R.; Giehl, P.M.; Paiva, D.N.; Marin, P.J.; Salmon, J.R.; et al. Whole-body vibration and benefits for people with osteoarthritis: A systematic review. Int. J. Med. Med. Sci. 2014, 6, 201–210. [Google Scholar]
- Di Giminiani, R.; Manno, R.; Scrimaglio, R.; Sementilli, G.; Tihanyi, J. Effects of individualized whole-body vibration on muscle flexibility and mechanical power. J. Sports Med. 2010, 50, 139–151. [Google Scholar]
- Sá-Caputo, D.D.; Ronikeili-Costa, P.; Carvalho-Lima, R.P.; Bernardo, L.C.; Bravo-Monteiro, M.O.; Costa, R.; Moraes-Silva, J.D.; Paiva, D.N.; Machado, C.B.; Mantilla-Giehl, P.; et al. Whole Body Vibration Exercises and the Improvement of the Flexibility in Patient with Metabolic Syndrome. J. Rehabil. Res. Dev. 2014, 2014, 628518. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Seo, D. The effects of whole body vibration on static balance, spinal curvature, pain, and disability of patients with low back pain. J. Phys. Ther. Sci. 2015, 27, 805–808. [Google Scholar] [CrossRef]
- Wang, P.; Yang, X.; Yang, Y.; Yang, L.; Zhou, Y.; Liu, C.; Reinhardt, J.D.; He, C. Effects of whole body vibration on pain, stiffness and physical functions in patients with knee osteoarthritis: A systematic review and meta-analysis. Clin. Rehabil. 2015, 29, 939–951. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.J.; Misra, D. Measures of Knee Function. Arthritis Care Res. 2011, 63, 208–228. [Google Scholar] [CrossRef] [PubMed]
- Marshall, C.J.; Dobson, F.; Hinman, R.S.; Sayer, T.; Anderson, C.; Newcomb, N.; Bennell, K.L. Reliability of the osteoarthritis research society international recommended performance-based tests of physical function in people with hip and knee osteoarthritis. Osteoarthr. Cartil. 2015, 23, A343–A344. [Google Scholar] [CrossRef]
- Bennell, K.; Dobson, F.; Hinman, R. Measures of physical performance assessments: Self-Paced Walk Test (SPWT), Stair Climb Test (SCT), Six-Minute Walk Test (6MWT), Chair Stand Test (CST), Timed Up & Go (TUG), Sock Test, Lift and Carry Test (LCT), and Car Task. Arthritis Care Res. 2011, 63, S350–S370. [Google Scholar]
- Avelar, N.C.P.; Simão, A.P.; Tossige-Gomes, R.; Neves, C.D.C.; Rocha-Vieira, E.; Coimbra, C.C.; Lacerda, A.C.R. The Effect of Adding Whole-Body Vibration to Squat Training on the Functional Performance and Self-Report of Disease Status in Elderly Patients with Knee Osteoarthritis: A Randomized, Controlled Clinical Study. J. Altern. Complement. Med. 2011, 17, 1149–1155. [Google Scholar] [CrossRef]
- Paineiras-Domingos, L.L.; da Cunha Sá-Caputo, D.; Reis, A.S.; Francisca Santos, A.; Sousa-Gonçalves, C.R.; Dos Anjos, E.M.; dos Santos Pereira, M.J.; Sartorio, A.; Bernardo-Filho, M. Assessment through the short physical performance battery of the functionality in individuals with metabolic syndrome exposed to whole-body vibration exercises. Dose-Response 2018, 16. [Google Scholar] [CrossRef]
- Sá-Caputo, D.C.; Paineiras-Domingos, L.L.; Oliveira, R.; Neves, M.F.T.; Brandão, A.; Marin, P.J.; Sañudo, B.; Furness, T.; Taiar, R.; Bernardo-Filho, M. Acute Effects of Whole-Body Vibration on the Pain Level, Flexibility, and Cardiovascular Responses in Individuals With Metabolic Syndrome. Dose-Response 2018, 16. [Google Scholar] [CrossRef]
- Nogier, R. Auriculotherapy; Ed.Thieme: Stuttgart, Germany; New York, NY, USA, 2009; Volume 14. [Google Scholar]
- Metsavaht, L.; Leporace, G.; Riberto, M.; de Mello Sposito, M.M.; Batista, L.A. Translation and Cross-Cultural Adaptation of the Brazilian Version of the International Knee Documentation Committee Subjective Knee Form. Am. J. Sports Med. 2010, 38, 1894–1899. [Google Scholar] [CrossRef] [PubMed]
- Costa-Cavalcanti, R.G.; de Sá-Caputo, D.D.; Moreira-Marconi, E.; Küter, C.R.; Brandão-Sobrinho-Neto, S.; Paineiras-Domingos, L.L.; Moura-Fernandes, M.C.; da Costa, J.M.; de Moraes Carmo, J.M.; Nogueira-Neto, J.F.; et al. Effect of Auriculotherapy on the Plasma Concentration of Biomarkers in Individuals with Knee Osteoarthritis. J. Acupunct. Meridian Stud. 2018, 11, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Marconi, E.; Dionello, C.F.; Morel, D.S.; Sá-Caputo, D.C.; Sousa-gonçalves, C.R.; José, M.; Bernardo-Filho, M. Whole body vibration and auriculotherapy improve handgrip strength in individuals with knee osteoarthritis. J. Tradit. Chin. Med. 2019, 39, 707–715. [Google Scholar]
- Coffey, V.G.; Hawley, J.A. Concurrent exercise training: Do opposites distract? J. Physiol. 2017, 595, 2883–2896. [Google Scholar] [CrossRef]
- Mann, T.N.; Lamberts, R.P.; Lambert, M.I. High Responders and Low Responders: Factors Associated with Individual Variation in Response to Standardized Training. Sport. Med. 2014, 44, 1113–1124. [Google Scholar] [CrossRef]
- Park, Y.G.; Kwon, S.; Park, J.-W.; Cha, D.Y.; Nam, K.Y.; Sim, K.B.; Chang, J.; Lee, H.J. Therapeutic Effect of Whole Body Vibration on Chronic Knee Osteoarthritis. Ann. Rehabil. Med. 2013, 37, 505–515. [Google Scholar] [CrossRef]
- Trans, T.; Aaboe, J.; Henriksen, M.; Christensen, R.; Bliddal, H.; Lund, H. Effect of whole body vibration exercise on muscle strength and proprioception in females with knee osteoarthritis. Knee 2009, 16, 256–261. [Google Scholar] [CrossRef]
- Wang, P.; Yang, L.; Li, H.; Lei, Z.; Yang, X.; Liu, C.; Jiang, H.; Zhang, L.; Zhou, Z.; Reinhardt, J.D.D.; et al. Effects of whole-body vibration training with quadriceps strengthening exercise on functioning and gait parameters in patients with medial compartment knee osteoarthritis: A randomised controlled preliminary study. Physiotherapy 2016, 102, 86–92. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Age (Year) (Md ± SD) | Stature (m) (Md ± SD) | Body Mass (kg) (Md ± SD) |
|---|---|---|---|
| CGAT | 63.00 ± 7.00 | 1.60 ± 0.08 | 85.67 ± 14.98 |
| GAT | 64.00 ± 7.00 | 1.59 ± 0.09 | 84.58 ± 14.90 |
| CGWBV | 66.00 ± 12.00 | 1.57 ± 0.07 | 84.50 ± 13.38 |
| GWBV | 67.00 ± 10.00 | 1.57 ± 0.05 | 84.59 ± 14.15 |
| CGWBV + AT | 65.00 ± 7.00 | 1.55 ± 0.04 | 84.96 ± 14.59 |
| GWBV + AT | 65.00 ± 8.00 | 1.55 ± 0.08 | 85.49 ± 14.36 |
| p-value | 0.852 | 0.310 | 0.999 |
| Control | Intervention | |||||
|---|---|---|---|---|---|---|
| Before | After | Before | After | |||
| Md ± SD | Md ± SD | p-value* | Md ± SD | Md ± SD | p-value* | |
| /100 | /100 | /100 | /100 | |||
| GAT | 24.68 ± 9.85 | 27.58 ± 9.71 | 0.098 | 33.59 ± 16.84 | 35.91 ± 17.70 | 0.37 |
| GWBV | 28.87 ± 13.69 | 34.19 ± 11.45 | 0.299 | 31.55 ± 13.21 | 33.79 ± 9.07 | 0.43 |
| GWBV + AT | 27.07 ± 7.86 | 30.26 ± 8.42 | 0.059 | 31.03 ± 11.85 | 34.49 ± 14.67 | 0.14 |
| Control | Intervention | |||||
|---|---|---|---|---|---|---|
| Before | After | Before | After | |||
| Med ± IQR | Med ± IQR | p-value* | Med ± IQR | Med ± IQR | p-value* | |
| (score) | (score) | (score) | (score) | |||
| GAT | 7.00 ± 1.75 | 7.00 ± 2.00 | 0.529 | 7.00 ± 3.75 | 7.50 ± 2.00 | 0.29 |
| GWBV | 7.00 ± 2.00 | 7.00 ± 7.00 | 0.798 | 7.00 ± 2.00 | 8.00 ± 2.00 | 0.01* |
| GWBV + AT | 7.00 ± 4.00 | 7.00 ± 3.00 | 0.834 | 7.00 ± 1.50 | 8.50 ± 1.75 | 0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro Kütter, C.; Moreira-Marconi, E.; Teixeira-Silva, Y.; Cristina Moura-Fernandes, M.; Gonçalves de Meirelles, A.; José dos Santos Pereira, M.; Chang, S.; Alexandre Bachur, J.; Liane Paineiras-Domingos, L.; Taiar, R.; et al. Effects of the Whole-Body Vibration and Auriculotherapy on the Functionality of Knee Osteoarthritis Individuals. Appl. Sci. 2019, 9, 5194. https://doi.org/10.3390/app9235194
Ribeiro Kütter C, Moreira-Marconi E, Teixeira-Silva Y, Cristina Moura-Fernandes M, Gonçalves de Meirelles A, José dos Santos Pereira M, Chang S, Alexandre Bachur J, Liane Paineiras-Domingos L, Taiar R, et al. Effects of the Whole-Body Vibration and Auriculotherapy on the Functionality of Knee Osteoarthritis Individuals. Applied Sciences. 2019; 9(23):5194. https://doi.org/10.3390/app9235194
Chicago/Turabian StyleRibeiro Kütter, Cristiane, Eloá Moreira-Marconi, Ygor Teixeira-Silva, Marcia Cristina Moura-Fernandes, Alexandre Gonçalves de Meirelles, Mario José dos Santos Pereira, Shyang Chang, José Alexandre Bachur, Laisa Liane Paineiras-Domingos, Redha Taiar, and et al. 2019. "Effects of the Whole-Body Vibration and Auriculotherapy on the Functionality of Knee Osteoarthritis Individuals" Applied Sciences 9, no. 23: 5194. https://doi.org/10.3390/app9235194
APA StyleRibeiro Kütter, C., Moreira-Marconi, E., Teixeira-Silva, Y., Cristina Moura-Fernandes, M., Gonçalves de Meirelles, A., José dos Santos Pereira, M., Chang, S., Alexandre Bachur, J., Liane Paineiras-Domingos, L., Taiar, R., Bernardo-Filho, M., & da Cunha de Sá-Caputo, D. (2019). Effects of the Whole-Body Vibration and Auriculotherapy on the Functionality of Knee Osteoarthritis Individuals. Applied Sciences, 9(23), 5194. https://doi.org/10.3390/app9235194