The Evolution of Tissue Engineered Vascular Graft Technologies: From Preclinical Trials to Advancing Patient Care


Abstract
:1. Introduction
- (I)
- Cells (i.e., progenitor cells, stem cells);
- (II)
- Scaffolds (i.e., synthetic, decellularized extracellular matrix);
- (III)
- Signals (growth factors, chemotactic factors) [6].
2. Material and Methods
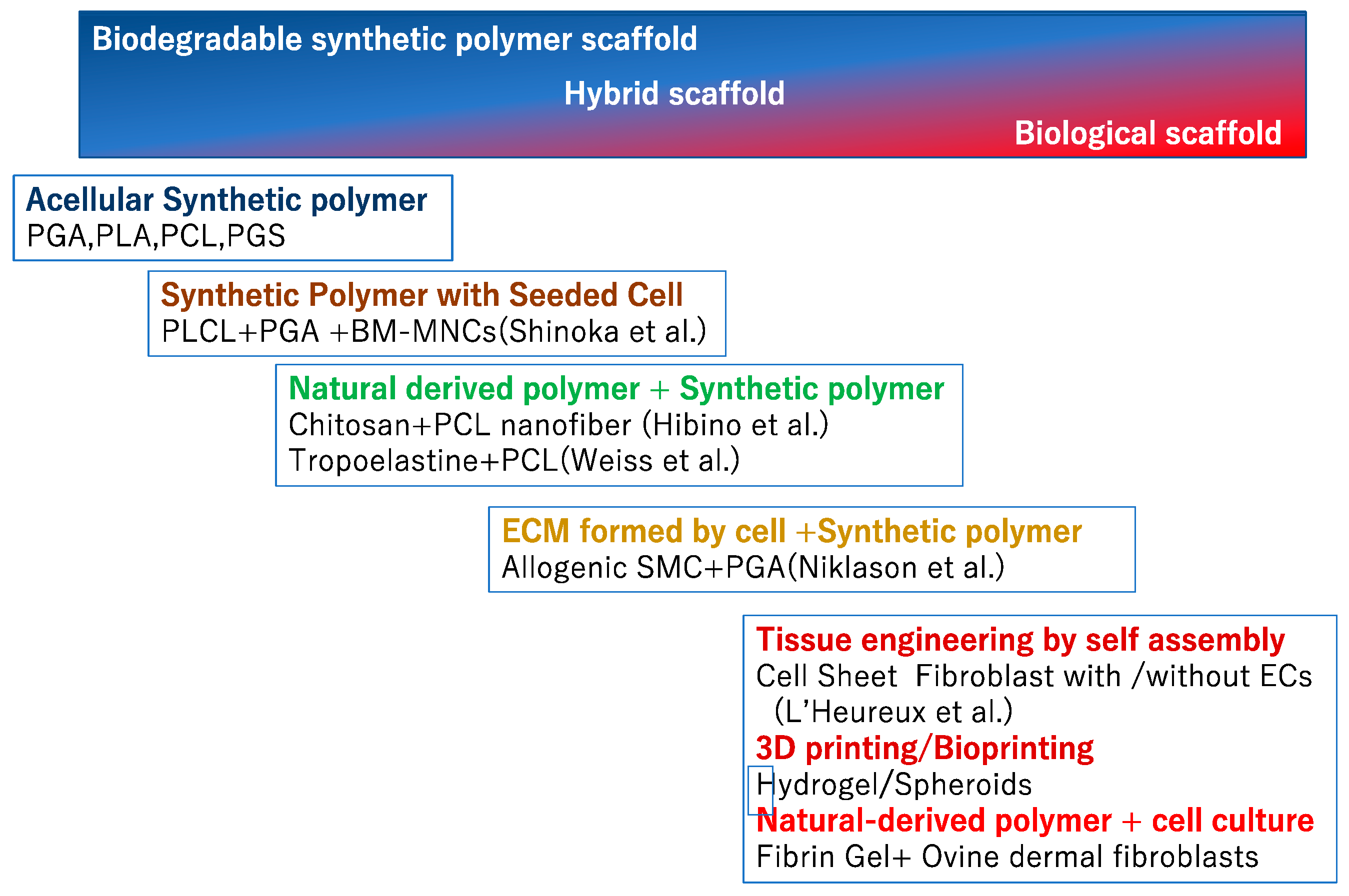
2.1. Biodegradable Synthetic Vascular Grafts
- Poly (glycolic acid) (PGA)
- Poly (lactic acid) (PLA)
- Poly (ε-caprolactone) (PCL)
- Poly (glycerol) sebacate (PGS)
2.1.1. PGA
2.1.2. PLA
2.1.3. PCL
2.1.4. PGS
2.2. Natural Polymeric Biomaterials
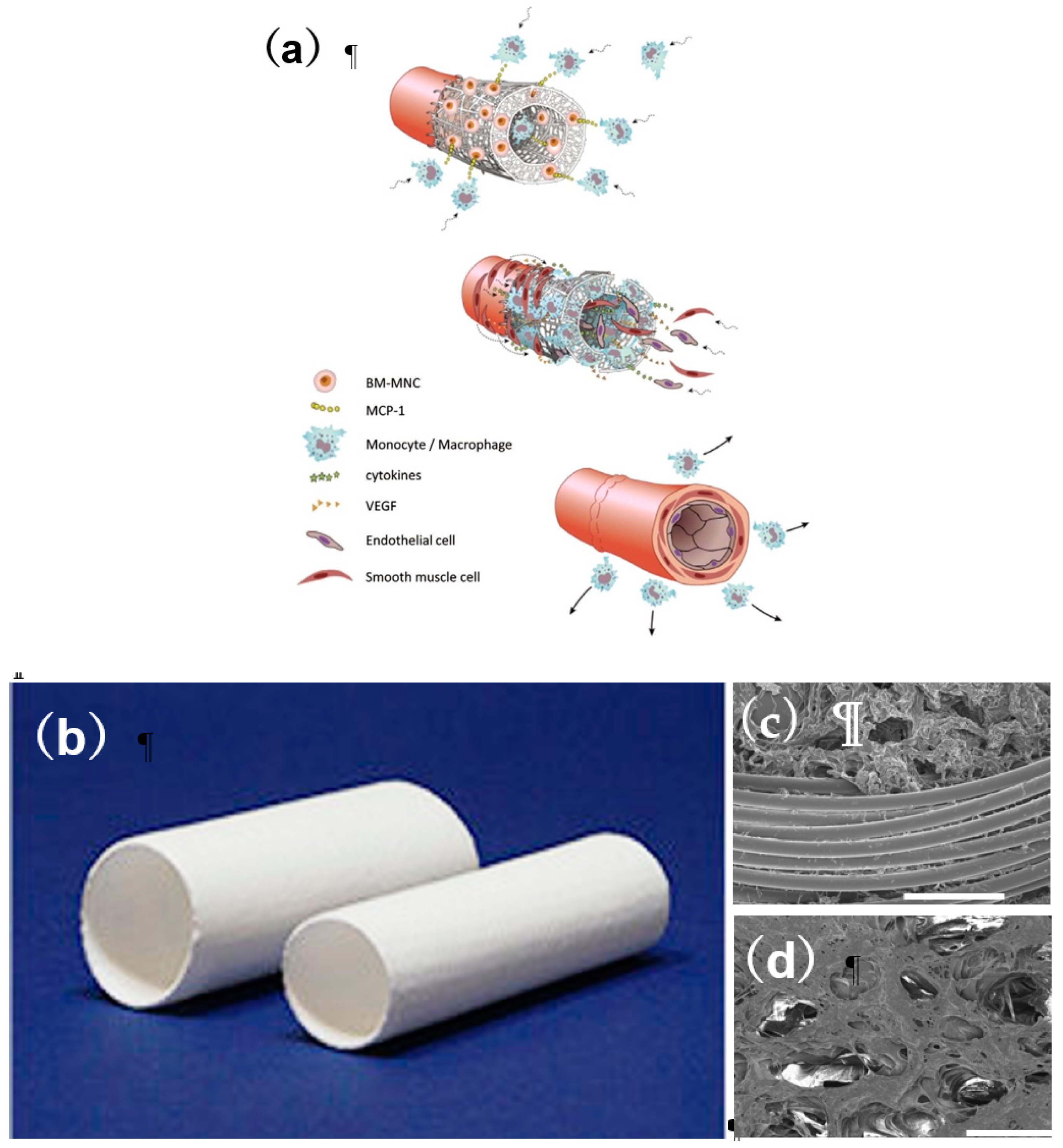
2.3. Application of Cell Biology to TEVG
2.4. Application of 3D Printing TEVG
3. Clinical Study in Venous Model
4. Clinical Study in Arterial Model
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [PubMed]
- Simeone, R.M.; Oster, M.E.; Cassell, C.H.; Armour, B.S.; Gray, D.T.; Honein, M.A. Pediatric inpatient hospital resource use for congenital heart defects. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. Heart Disease and Stroke Statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed]
- van der Slegt, J.; Steunenberg, S.L.; Donker, J.M. The current position of precuffed expanded polytetrafluoroethylene bypass grafts in peripheral vascular surgery. J. Vasc. Surg. 2014, 60, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Drews, J.D.; Miyachi, H.; Shinoka, T. Tissue-engineered vascular grafts for congenital cardiac disease: Clinicalexperience and current status. Trends Cardiovasc. Med. 2017, 27, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Langer, R.; Vacanti, J.P. Tissue engineering. Science 1993, 260, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, C.B.; Bell, E. A blood vessel model constructed from collagen and cultured vascular cells. Science 1986, 231, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, G.; Hibino, N.; Ikada, Y.; Kurosawa, H.; Shinoka, T. Successful application of tissue engineered vascular autografts: Clinical experience. Biomaterials 2003, 24, 2303–2308. [Google Scholar] [CrossRef]
- Lawson, J.H.; Glickman, M.H.; Ilzecki, M.; Jakimowics, T.; Jaroszynski, A.; Peden, E.K.; Piglim, A.J.; Prichaed, H.L.; Guziewics, M.; Przywana, S.; et al. Bioengineered human acellular vessels for dialysis access in patients with end-stage renal disease: Two phase 2 single-arm trials. Lancet 2016, 387, 2026–2034. [Google Scholar] [CrossRef]
- Rosso, F.; Marino, G.; Giordano, A.; Barbarisi, M.; Parmeggiani, D.; Barbarisi, A. Smart materials as scaffolds for tissue engineering. J. Cell. Physiol. 2005, 203, 465–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crapo, P.M.; Gilbert, T.W.; Badylak, S.F. An overview of tissue and whole organ decellularization processes. Biomaterials 2011, 32, 3233–3243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashi, C.K.; Zhu, Y.; Yang, G.Y.; Young, W.L.; Hsiao, B.S.; Wang, K.; Chu, B.; Li, S. Antithrombogenic property of bone marrow mesenchymal stem cells in nanofibrous vascular grafts. Proc. Natl. Acad. Sci. USA 2007, 104, 11915–11920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, L.; Greisler, H.P. Biomaterials in the development and future of vascular grafts. J. Vasc. Surg. 2003, 37, 472–480. [Google Scholar] [CrossRef] [Green Version]
- Tara, S.; Rocco, K.A.; Hibino, N.; Sugiura, T.; Kurobe, H.; Breuer, C.K.; Shinoka, T. Vessel bioengineering. Circ. J. 2014, 78, 12–19. [Google Scholar] [CrossRef]
- Hajiali, H.; Shahgasempour, S.; Naimi-Jamal, M.R.; Peirovi, H. Electrospun PGA/gelatin nanofibrous scaffolds and their potential application in vascular tissue engineering. J. Mater. Sci. 2010, 21, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Treiser, M.; Abramson, S.; Langer, R.; Kohn, J. Degradable and resorbable materials. In Biomaterials Science An Introduction to Materials in Medicine. Chapeter I.2.6. Degradable and Resorbable Biomaterials; Elsevier: London, UK, 2013. [Google Scholar] [CrossRef]
- Hashi, C.K.; Derugin, N.; Janairo, R.R.; Lee, R.; Schultz, D.; Lotz, J.; Li, S. Antithrombogenic modification of small-diameter microfibrous vascular grafts. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, T.; Tara, S.; Nakayama, H.; Kurobe, H.; Yi, T.; Lee, A.Y.; Breuer, C.K.; Shinoka, T. Novel Bioresorbable Vascular Graft With Sponge-Type Scaffold as a Small-Diameter Arterial Graft. Ann. Thorac. Surg. 2016, 102, 720–727. [Google Scholar] [CrossRef]
- Garg, K.; Pullen, N.A.; Oskeritzian, C.A.; Ryan, J.J.; Bowlin, G.L. Macrophage functional polarization (M1/M2) in response to varying fiber and pore dimensions of electrospun scaffolds. Biomaterials 2013, 34, 4439–4451. [Google Scholar] [CrossRef]
- Miyamoto, S.; Shoji, T.; MIyachi, H.; Shinoka, T. Smart Biomaterials for Cardiovascular Tissue Engineering. In Smart Materials for Tissue Engineering: Application; Royal Society of Chemistry: London, UK, 2017; pp. 230–257. [Google Scholar]
- Pektok, E.; Nottelet, B.; Tille, J.C. Degradation and healing characteristics of small-diameter poly(epsilon-caprolactone) vascular grafts in the rat systemic arterial circulation. Circulation 2008, 118, 2563–2570. [Google Scholar] [CrossRef]
- de Valence, S.; Tille, J.C.; Mugnai, D. Long term performance of polycaprolactone vascular grafts in a rat abdominal aorta replacement model. Biomaterials 2012, 33, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Nottelet, B.; Pektok, E.; Mandracchia, D.; Tille, J.C.; Walpoth, B.; Gurny, R.; Moller, M. Factorial design optimization and in vivo feasibility of poly(epsilon-caprolactone)-micro- and nanofiber-based small diameter vascular grafts. J. Biomed. Mater. Res. Part A 2009, 89, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Tara, S.; Kurobe, H.; Rocco, K.A.; Maxfield, M.W.; Best, C.A.; Yi, T.; Breuer, C.K.; Shinoka, T. Well-organized neointima of large-pore poly(L-lactic acid) vascular graft coated with poly(L-lactic-co-ε-caprolactone) prevents calcific deposition compared to small-pore electrospun poly(L-lactic acid) graft in a mouse aortic implantation model. Athelioscrerosis 2014, 237, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ameer, G.A.; Sheppard, B.J.; Langer, R. A tough biodegradable elastomer. Nat. Biotechnol. 2002, 20, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.A.; Wu, W.; Yao, M.; Dutta, D.; Duan, X.; Bachman, T.N. Nerve regeneration and elastin formation within poly(glycerol sebacate)-based synthetic arterial grafts one-year post-implantation in a rat model. Biomaterials 2014, 35, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Yokota, T.; Ichikawa, H.; Matsumiya, G.; Kuratani, T.; Sakaguchi, T.; Iwai, S. In situ tissue regeneration using a novel tissue-engineered, small-caliber vascular graft without cell seeding. J. Thorac. Cardiovasc. Surg. 2008, 136, e900–e907. [Google Scholar] [CrossRef] [PubMed]
- Pektok, E.; Nottelet, B.; Tille, J.C.; Gurny, R.; Kalangos, A.; Moeller, M. Degradation and healing characteristics of small-diameter poly(ε-capro-lactone) vascular grafts in the rat systemic arterial circulation. Circulation 2008, 118, 2563–2570. [Google Scholar] [CrossRef]
- Taylor, M.S.; Shalaby, S.W. Sutures. In Biomaterials Science: An Introduction to Materials in Medicine; Elsevier: Amsterdam, The Netherlands, 2013; pp. 1010–1024. [Google Scholar]
- Raboud, M.; Lefebvre, F.; Ducassou, D. In vitro association of type III collagen with elastin and with its solubilized peptides. Biomaterials 1991, 12, 313–319. [Google Scholar] [CrossRef]
- Wise, S.; Byrom, M.J.; Waterhouse, A.; Bannon, P.G.; Weiss, A.S.; Ng, M.K. A multilayered synthetic human elastin/polycaprolactone hybrid vascular graft with tailored mechanical properties. Acta Biomater. 2011, 7, 295–303. [Google Scholar] [CrossRef]
- Kim, I.Y.; Seo, S.J.; Moon, H.S.; Yoo, M.K.; Park, I.Y.; Kim, B.C.; Cho, C.S. Chitosan and its derivatives for tissue engineering applications. Biotechnol. Adv. 2008, 26, 21–32. [Google Scholar] [CrossRef]
- Fukunishi, T.; Best, C.A.; Sugiura, T.; Shoji, T.; Yi, T.; Udelsman, B.; Ohst, D.; Ong, C.S.; Zhang, H.; Shinoka, T.; Breuer, C.K.; Johnson, J.; Hibino, N. Tissue-engineered small diameter arterial vascular grafts from cell-free nanofiber PCL/chitosan scaffolds in a sheep model. PLoS ONE 2016, 11, e0158555. [Google Scholar] [CrossRef]
- Greisler, H.P.; Joyce, K.A.; Kim, D.U.; Pham, S.M.; Berceli, S.A.; Borovetz, H.S. Spatial and temporal changes in compliance following implantation of bio-resorbable vascular grafts. J. Biomed. Mater. Res. 1992, 26, 1449–1461. [Google Scholar] [CrossRef]
- Greisler, H.P.; Cabusao, E.B.; Lam, T.M.; Murchan, P.M.; Ellinger, J.; Kim, D.U. Kinetics of collagen deposition within bioresorbable and nonresorbable vascular prostheses. ASAIO Trans. 1991, 37, M472–M475. [Google Scholar]
- Wang, Z.; Cui, Y.; Wang, J.; Yang, X.; Wu, Y.; Wang, K.; Gao, X.; Li, D.; Li, Y.; Zheng, X.L.; Kong, D.; Zhao, Q. The effect of thick fibers and large pores of electrospun poly (epsilon-caprolactone) vascular grafts on macrophage polarization and arterial regeneration. Biomaterials 2014, 35, 5700–5710. [Google Scholar] [CrossRef]
- Janairo, R.R.R.; Zhu, Y.; Chen, T.; Li, S. Mucin covalently bonded to microfibers improves the patency of vascular grafts. Tissue Eng. Part A 2014, 20, e285–e293. [Google Scholar] [CrossRef]
- Walles, T.; Gorler, H.; Puschmann, C.; Mertsching, H. Functional neointima characterization of vascular prostheses in human. Ann. Thorac. Surg. 2004, 77, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Rosenman, J.E.; Kempczinski, R.F.; Pearce, W.H.; Edward, B.S. Kinetics of endothelial cell seeding. J. Vasc. Surg. 1985, 2, 778–784. [Google Scholar] [CrossRef]
- L’Heureux, N.; Dusserre, N.; Konig, G.; Victor, B.; Keire, P.; Wight, T.N. Human tissue-engineered blood vessels for adult arterial revascularization. Nat. Med. 2006, 12, 361–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAllister, T.N.; Maruszewski, M.; Garrido, S.A.; Wystrychowski, W.; Dusserre, N.; Marini, A.; Zagaiski, K.; Fiorillo, A.; Avila, H.; Manglano, X.; et al. Effectiveness of haemodialysis access with an autologous tissue-engineered vascular graft: A multicentre cohort study. Lancet 2009, 373, 1440–1446. [Google Scholar] [CrossRef]
- Mount, C.; Dusserrre, N.; Mcallister, T.; L’Heureux, N. Tissue-engineered cardiovascular grafts and novel applications of tissue engineering by self-assembly (TESA): Biomaterials and tissue engineering. In Cardiac Regeneration and Repair; Li, R.-K., Weisel, R.D., Eds.; Woodhead Publishing: Sawston, UK, 2014; Volume 2, pp. 434–435. [Google Scholar]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef]
- Borovjagin, A.V.; Ogle, B.M.; Berry, J.L.; Zhang, J. From Microscale Devices to 3D Printing: Advances in Fabrication of 3D Cardiovascular Tissues. Circ. Res. 2017, 120, 150–165. [Google Scholar] [CrossRef] [PubMed]
- Mosadegh, B.; Xiong, G.; Dunham, S.; Min, J.K. Current progress in 3D printing for cardiovascular tissue engineering. Biomed. Mater. 2015, 10, 034002. [Google Scholar] [CrossRef] [PubMed]
- Mota, C.; Puppi, D.; Chiellini, F.; Chiellini, E. Additive manufacturing techniques for the production of tissue engineering constructs: Additive manufacturing techniques for the production of tissue engineering constructs. J. Tissue Eng. Regen. Med. 2015, 9, 174–190. [Google Scholar] [CrossRef]
- Hölzl, K.; Lin, S.; Tytgat, L.; Van Vlierberghe, S.; Gu, L.; Ovsianikov, A. Bioink properties before, during and after 3D bioprinting. Biofabrication 2016, 8, 032002. [Google Scholar] [CrossRef] [Green Version]
- Gopinathan, J.; Noh, I. Recent trends in bioinks for 3D printing. Biomater. Res. 2018, 22, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabriz, A.G.; Hermida, M.A.; Leslie, N.R.; Shu, W. Three-dimensional bioprinting of complex cell laden alginate hydrogel structures. Biofabrication 2015, 7, 045012. [Google Scholar] [CrossRef]
- Alemán, J.V.; Chadwick, A.V.; He, J.; Hess, M.; Horie, K.; Jones, R.G.; Kratochvíl, P.; Meisel, I.; Mita, I.; Moad, G. Definitions of terms relating to the structure and processing of sols, gels, networks, and inorganic-organic hybrid materials (IUPAC Recommendations 2007). Pure Appl. Chem. 2007, 79, 1801–1829. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, A.S. Hydrogels for biomedical applications. Adv. Drug Deliv. Rev. 2012, 64, 18–23. [Google Scholar] [CrossRef]
- Fukunishi, T.; Best, C.A.; Sugiura, T.; Opfermann, J.; Ong, C.S.; Shinoka, T.; Breuer, C.K.; Krieger, A.; Johnson, J.; Hibino, N. Preclinical study of patient-specific cell-free nanofiber tissue-engineered vascular grafts using 3-dimensional printing in a sheep model. J. Thorac. Cardiovasc. Surg. 2017, 153, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Guvendiren, M. Recent Advances in Bioink Design for 3D Bioprinting of Tissues and Organs. Front. Bioeng. Biotechnol. 2017, 5, 23. [Google Scholar] [CrossRef]
- Gelinsky, M. Biopolymer hydrogel bioinks. In 3D Bioprinting for Reconstructive Surgery; Thomas, D.J., Jessop, Z.M., Whitaker, I.S., Eds.; Elsevier Science & Technology: Cambridge, UK, 2018; pp. 125–136. [Google Scholar]
- Vijayavenkataraman, S.; Yan, W.-C.; Lu, W.F.; Wang, C.-H.; Fuh, J.Y.H. 3D bioprinting of tissues and organs for regenerative medicine. Adv. Drug Deliv. Rev. 2018, 13, 296–332. [Google Scholar] [CrossRef] [PubMed]
- Mironov, V.; Visconti, R.P.; Kasyanov, V.; Forgacs, G.; Drake, C.J.; Markwald, R.R. Organ printing: Tissue spheroids as building blocks. Biomaterials 2009, 30, 2164–2174. [Google Scholar] [CrossRef] [PubMed]
- Itoh, M.; Nakayama, K.; Noguchi, R.; Kamohara, K.; Furukawa, K.; Uchihashi, K.; et al. Correction: Scaffold-free tubular tissues created by a Bio-3D printer undergo remodeling and endothelialization when implante in rat aortae. PLoS ONE 2015, 10, e0145971. [Google Scholar] [CrossRef]
- Shinoka, T.; Imai, Y.; Ikada, Y. Transplantation of a tissue-engineered pulmonary artery. N. Engl. J. Med. 2001, 344, 532–533. [Google Scholar] [CrossRef] [PubMed]
- Shinoka, T.; Matsumura, G.; Hibino, N.; Naito, Y.; Watanabe, W.; Konuma, T.; Sakamoto, T.; Nagatsu, M.; Kurosawa, H. Midterm clinical result of tissue-engineered vascular autografts seeded with autologous bone marrow cells. J. Thorac. Cardiovasc. Surg. 2005, 129, 1330–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hibino, N.; McGillicuddy, E.; Matsumura, G.; Ichihara, Y.; Naito, Y.; Breuer, C.K.; Shinoka, T. Late-term results of tissue- engineered vascular grafts in humans. J. Thorac. Cardiovasc. Surg. 2010, 139, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, T.; Matsumura, G.; Miyamoto, S.; Miyachi, H.; Breuer, C.K.; Shinoka, T. Tissue-engineered Vascular Grafts in Children With Congenital Heart Disease: Intermediate Term Follow-up. Semin. Thoracic. Surg. 2018, 30, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Shinoka, T. What is the best material for extracardiac Fontan operation? J. Thorac. Cardiovasc. Surg. 2017, 153, 1551–1552. [Google Scholar] [CrossRef]
- Harrington, J.K.; Chahboune, H.; Criscione, J.M.; Li, A.Y.; Hibino, N.; Yi, T.; Villalona, G.A.; Kobsa, S.; Meijas, D.; Duncan, D.R.; et al. Determining the fate of seeded cells in venous tissue-engineered vascular grafts using serial MRI. FASEB J. 2011, 25, 4150–4161. [Google Scholar] [CrossRef] [Green Version]
- Brennan, M.P.; Dardik, A.; Hibino, N.; Roh, J.D.; Nelson, G.N.; Papademitris, X.; SHinoka, T.; Breure, C.K. Tissue-engineered vascular grafts demonstrate evidence of growth and development when implanted in a juvenile animal model. Ann. Surg. 2008, 248, 370–377. [Google Scholar] [CrossRef]
- Hibino, N.; Yi, T.; Duncan, D.R.; Dean, E.; Naito, Y.; Dardik, A.; Kyriakides, T.; Madri, J.; Pober, J.S.; Shinoka, T.; Breuer, C.K. A critical role for macrophages in neovessel formation and the development of stenosis in tissue-engineered vascular grafts. FASEB J. 2011, 25, 4253–4263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, M.; Shin’oka, T.; Tohyama, S.; Hibino, N.; Konuma, T.; Matsumura, G.; Kosaka, Y.; Ishida, T.; Imai, Y.; Yamanaka, M.; et al. Tissue-engineered vascular autograft: Inferior vena cava replacement in a dog model. Tissue Eng. 2001, 7, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Best, C.; Tara, S.; Wiet, M.; Reinhardt, J.; Pepper, V.; Ball, M.; Yi, T.; Shinoka, T.; Breuer, C.K. Deconstructing the tissue engineered vascular graft; evaluating scaffold pre-wetting, conditioned media incubation, and determining the optimal mononuclear cell source. ACS Biomater. Sci. Eng. 2017, 3, 1972–1979. [Google Scholar] [CrossRef]
- Ruiz-Rosado, J.D.; Mahler, N.; Yi, T.; Robledo, A.F.; Martinez, S.D.; Lee, A.Y.; Shoji, T.; Lee, A.Y.; Heuer, E.; Yates, A.R. Angiotensin II receptor I blockade prevents stenosis of tissue engineered vascular grafts. FASEB J. 2018, 15, fj201800458. [Google Scholar] [CrossRef] [PubMed]
- Niklason, L.E.; Gao, J.; Abbott, W.M.; Hirschi, K.K.; Houser, S.; Marini, R.; Langer, R. Functional Arteries Grown in Vitro. Science 1999, 284, 489–493. [Google Scholar] [CrossRef]
- Prichard, H.L.; Manson, R.J.; Di Bernardo, L.; Nikalson, L.E.; Lawson, J.H.; Dash, S.L. An early study on the mechanisms that allow tissue-engineered vascular grafts to resist intimal hyperplasia. J. Cardiovasc. Transl. Res. J. Cardiovasc. Transl. 2011, 4, 674–682. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Main Diagnosis | Age | Graft Type | Graft Size |
|---|---|---|---|---|
| 1 | Asplenia, AVSD(A), small RV | 2 | PLA | 16 |
| 2 | Asplenia, SRV, TAPVC(Ib+III) | 1 | PLA | 20 |
| 3 | Concordant criss-cross heart, DORV, PAA, MS | 8 | PLA | 18 |
| 4 | TA(Ib) | 22 | PLA | 24 |
| 5 | PPA, ASD(II), sinusoidal communication | 13 | PLA | 22 |
| 6 | SRV, DORV, AVVA | 4 | PLA | 20 |
| 7 | Total sinus defect, ASD, TR(IV) | 14 | PLA | 24 |
| 8 | Asplenia, SLV, CAVVR | 17 | PLA | 24 |
| 9 | TA(Ib) | 22 | PLA | 22 |
| 10 | Polysplenia, SRV | 4 | PLA | 12 |
| 11 | HLHS, MA, IAA(A) | 2 | PLA | 16 |
| 12 | Asplenia, SRV, PAA, non-confluent PA | 2 | PGA | 16 |
| 13 | SLV, lt AVVA | 2 | PGA | 16 |
| 14 | DORV, small LV, VSD, PS, ASD(II) | 2 | PGA | 18 |
| 15 | polysplenia, cAVSD, DORV, PS | 2 | PGA | 12 |
| 16 | Asplenia, SRV, CA, TAPVC(Ib) | 2 | PGA | 16 |
| 17 | PPA, RA thrombosis, AFL, af | 24 | PGA | 18 |
| 18 | SRV, DIRV, PA, ASD(II) | 1 | PGA | 16 |
| 19 | Asplenia, SRV, PS, CA | 11 | PGA | 18 |
| 20 | polysplenia, cAVSD, PS, CAVVR | 2 | PGA | 14 |
| 21 | DORV, VSD, small RV, PLSVC, TAPVC(IIb) | 3 | PGA | 16 |
| 22 | PPA, ASD(II), PS, Sinusoidal communication | 5 | PGA | 18 |
| 23 | SLV, DILV, PA, ASD, bilateral SVC | 4 | PGA | 18 |
| 24 | Asplenia, SRV | 13 | PGA | 16 |
| 25 | TA(IIc), SAS | 2 | PGA | 18 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuzaki, Y.; John, K.; Shoji, T.; Shinoka, T. The Evolution of Tissue Engineered Vascular Graft Technologies: From Preclinical Trials to Advancing Patient Care. Appl. Sci. 2019, 9, 1274. https://doi.org/10.3390/app9071274
Matsuzaki Y, John K, Shoji T, Shinoka T. The Evolution of Tissue Engineered Vascular Graft Technologies: From Preclinical Trials to Advancing Patient Care. Applied Sciences. 2019; 9(7):1274. https://doi.org/10.3390/app9071274
Chicago/Turabian StyleMatsuzaki, Yuichi, Kelly John, Toshihiro Shoji, and Toshiharu Shinoka. 2019. "The Evolution of Tissue Engineered Vascular Graft Technologies: From Preclinical Trials to Advancing Patient Care" Applied Sciences 9, no. 7: 1274. https://doi.org/10.3390/app9071274
APA StyleMatsuzaki, Y., John, K., Shoji, T., & Shinoka, T. (2019). The Evolution of Tissue Engineered Vascular Graft Technologies: From Preclinical Trials to Advancing Patient Care. Applied Sciences, 9(7), 1274. https://doi.org/10.3390/app9071274