Physical Activity Amount and Cognitive Impairment in Korean Elderly Population


Abstract
:1. Introduction
2. Methodology
2.1. Participants
2.2. Korean Dementia Screening Questionnaire Cognition (KDSQ-C)
2.3. The International Physical Activity Questionnaire (IPAQ)
2.4. Blood Collection and Hemoglobin, Creatinine, and Serum Lipid Analysis
2.5. Statistical Analysis
3. Results
3.1. Associations between Physical Activity and Cognitive Function
3.2. Hemoglobin, Creatinine, and Serum Lipids
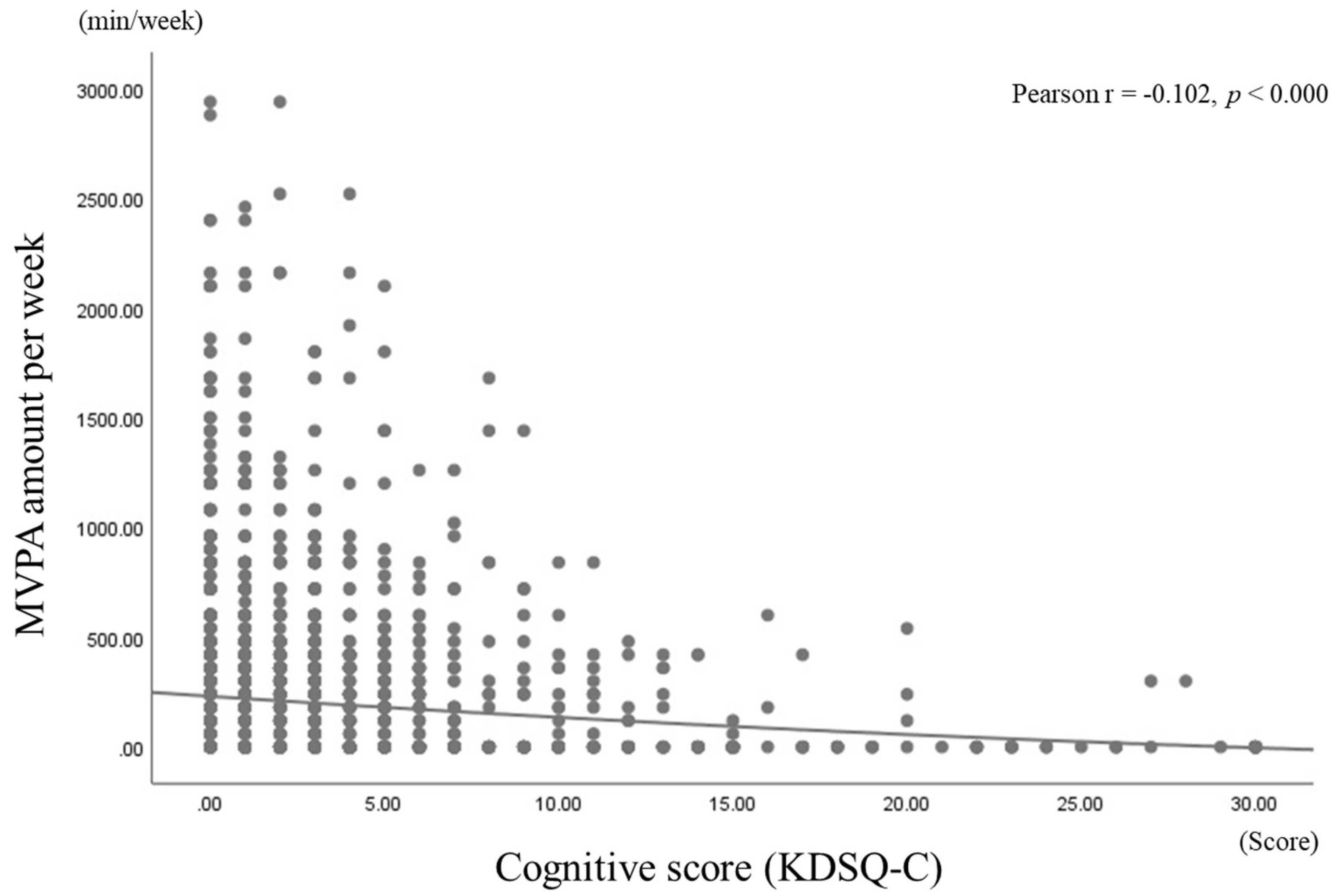
3.3. Correlations Coefficients between KDSQ-C Scores and MVPA Amounts
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s disease |
| ACSM | American College of Sports Medicine |
| CDC | Centers for Disease Control and Prevention (CDC) |
| KDSQ-C | Korean Dementia Screening Questionnaire Cognition |
| IPAQ | International Physical Activity Questionnaire |
| MVPA | Moderate-to-vigorous physical activity |
| NIHMID | Nasaret International Hospital Medical Informatics Data |
| TC | Total cholesterol |
| TG | Triglycerides |
| HDL-C | High-density lipoprotein cholesterol |
| LDL-C | Low-density lipoprotein cholesterol |
| ORs | Odds ratios |
| CIs | Confidence intervals |
| MMSE | Mini-Mental State Examination |
| WHO | World Health Organization |
| SPSS | Statistical package for social science |
References
- Choi, Y.S.; Kim, M.J.; Lee, G.Y.; Seo, Y.M.; Seo, A.R.; Kim, B.; Yoo, J.I.; Park, K.S. The Association between Frailty and Disability among the Elderly in Rural Areas of Korea. Int. J. Environ. Res. Public Health 2019, 16, 2481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontis, V.; Bennett, J.E.; Mathers, C.D.; Li, G.; Foreman, K.; Ezzati, M. Future life expectancy in 35 industrialised countries: Projections with a Bayesian model ensemble. Lancet 2017, 389, 1323–1335. [Google Scholar] [CrossRef] [Green Version]
- Au, B.; Dale-McGrath, S.; Tierney, M.C. Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing Res. Rev. 2017, 35, 176–199. [Google Scholar] [CrossRef]
- Langa, K.M.; Levine, D.A. The diagnosis and management of mild cognitive impairment: A clinical review. JAMA 2014, 312, 2551–2561. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, D.W.; Cho, S.J.; Na, D.L.; Jeon, H.J.; Kim, S.K.; Lee, Y.R.; Youn, J.H.; Kwon, M.; Lee, J.H.; et al. Brief screening for mild cognitive impairment in elderly outpatient clinic: Validation of the Korean version of the Montreal Cognitive Assessment. J. Geriatr. Psychiatry Neurol. 2008, 21, 104–110. [Google Scholar] [CrossRef]
- Etgen, T.; Sander, D.; Huntgeburth, U.; Poppert, H.; Förstl, H.; Bickel, H. Physical activity and incident cognitive impairment in elderly persons: The INVADE study. Arch. Intern. Med. 2010, 170, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlager, N.T.; Cox, K.; Kurz, A.F. Physical activity and mild cognitive impairment and Alzheimer’s disease. Curr. Neurol. Neurosci. Rep. 2010, 10, 352–358. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.H.; King, A.C. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef]
- Barnes, D.E.; Yaffe, K.; Satariano, W.A.; Tager, I.B. A longitudinal study of cardiorespiratory fitness and cognitive function in healthy older adults. J. Am. Geriatr. Soc. 2003, 51, 459–465. [Google Scholar] [CrossRef]
- Colcombe, S.J.; Erickson, K.I.; Scalf, P.E.; Kim, J.S.; Prakash, R.; McAuley, D.; Elavsky, S.; Marquez, D.X.; Hu, L.; Kramer, A.F. Aerobic exercise training increases brain volume in aging humans. J. Gerontol. Ser. A 2006, 61, 1166–1170. [Google Scholar] [CrossRef] [Green Version]
- Rajani, S.; Archana, R.; Indla, Y.R.; Rajesh, P. Correlation between hemoglobin levels and visual memory among an older adult population in Chennai. Natl. J. Physiol. Pharm. Pharmacol. 2020, 10, 604–608. [Google Scholar]
- Yaffe, K.; Lindquist, K.; Shlipak, M.G.; Simonsick, E.; Fried, L.; Rosano, C.; Satterfield, S.; Atkinson, H.; Windham, B.G.; Kurella-Tamura, M. Cystatin C as a marker of cognitive function in elders: Findings from the health ABC study. Ann. Neurol. 2008, 63, 798–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Cao, Y.; Xiao, C. Subgroup analysis of the influence of body mass index on the association between serum lipids and cognitive function in Chinese population. Lipids Health Dis. 2020, 19, 130. [Google Scholar] [CrossRef] [PubMed]
- Rabadi, M.H.; Vincent, A.S. Do vascular risk factors contribute to the prevalence of pressure ulcer in veterans with spinal cord injury? J. Spinal Cord Med. 2011, 34, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Liu, X.; Xia, R.; Li, N.; Liao, X.; Chen, Z. Chinese herbal medicine for vascular cognitive impairment in cerebral small vessel disease: A protocol for systematic review and meta-analysis of randomized controlled trials. Medicine 2020, 99, e22455. [Google Scholar] [CrossRef]
- Zakai, N.A.; Katz, R.; Hirsch, C.; Shlipak, M.G.; Chaves, P.H.M.; Newman, A.B.; Cushman, M. A prospective study of anemia status, hemoglobin concentration, and mortality in an elderly cohort: The Cardiovascular Health Study. Arch. Intern. Med. 2005, 165, 2214–2220. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health and Welfare. 2018 National Health Examination Doctor Consultation Manual; Korea Centers for Disease Control & Prevention: Cheongju-si, Korea, 2018. [Google Scholar]
- Yang, D.W.; Cho, B.; Chey, J.Y.; Kim, S.Y.; Kim, B.S. The development and validation of Korean Dementia Screening Questionnaire (KDSQ). J. Korean Neurol. Assoc. 2002, 20, 135–141. [Google Scholar]
- Choi, S.H.; Park, M.H. Three screening methods for cognitive dysfunction using the Mini-Mental State Examination and Korean Dementia Screening Questionnaire. Geriatr. Gerontol. Int. 2016, 16, 252–258. [Google Scholar] [CrossRef]
- Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)–Short and Long Forms. 2011. Available online: www.ipaq.ki.se (accessed on 24 January 2011).
- Boustani, M.; Peterson, B.; Hanson, L.; Harris, R.; Lohr, K.N. Screening for dementia in primary care: A summary of the evidence for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2003, 138, 927–937. [Google Scholar] [CrossRef]
- Brown, P.J.; Devanand, D.P.; Liu, X.; Caccappolo, E. Functional impairment in elderly patients with mild cognitive impairment and mild Alzheimer disease. Arch. Gen. Psychiatry 2011, 68, 617–626. [Google Scholar] [CrossRef] [Green Version]
- Auyeung, T.W.; Kwok, T.; Lee, J.; Leung, P.C.; Leung, J.; Woo, J. Functional decline in cognitive impairment--the relationship between physical and cognitive function. Neuroepidemiology 2008, 31, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Hebert, L.E.; Bienias, J.L.; McCann, J.J.; Scherr, P.A.; Wilson, R.S.; Evans, D.A. Upper and lower extremity motor performance and functional impairment in Alzheimer’s disease. Am. J. Alzheimer Dis. Other Dement. 2010, 25, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Svantesson, U.; Jones, J.; Wolbert, K.; Alricsson, M. Impact of Physical Activity on the Self-Perceived Quality of Life in Non-Frail Older Adults. J. Clin. Med. Res. 2015, 7, 585–593. [Google Scholar] [CrossRef] [Green Version]
- Kirkendall, D.T.; Garrett, W.E. The effects of aging and training on skeletal muscle. Am. J. Sports Med. 1998, 26, 598–602. [Google Scholar] [CrossRef]
- Laurin, D.; Verreault, R.; Lindsay, J.; MacPherson, K.; Rockwood, K. Physical activity and risk of cognitive impairment and dementia in elderly persons. Arch. Neurol. 2001, 58, 498–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psaltopoulou, T.; Kyrozis, A.; Stathopoulos, P.; Trichopoulos, D.; Vassilopoulos, D.; Trichopoulou, A. Diet, physical activity and cognitive impairment among elders: The EPIC-Greece cohort (European Prospective Investigation into Cancer and Nutrition). Public Health Nutr. 2008, 11, 1054–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, A.; Kim, S.; Park, K.W.; Park, K.H.; Youn, Y.C.; Lee, D.W.; Lee, J.Y.; Lee, J.H.; Jeong, J.H.; Choi, S.H.; et al. A Comparative Evaluation of the KDSQ-C, AD8, and SMCQ as a Cognitive Screening Test to Be Used in National Medical Check-ups in Korea. J. Korean Med. Sci. 2019, 34, e111. [Google Scholar] [CrossRef] [PubMed]
- Giraldez, R.R.; Sabatine, M.S.; Morrow, D.A.; Mohanavelu, S.; McCabe, C.H.; Antman, E.M.; Braunwald, E. Baseline hemoglobin concentration and creatinine clearance composite laboratory index improves risk stratification in ST-elevation myocardial infarction. Am. Heart J. 2009, 157, 517–524. [Google Scholar] [CrossRef]
- Schneider, A.L.; Jonassaint, C.; Sharrett, A.R.; Mosley, T.H.; Astor, B.C.; Selvin, E.; Coresh, C.; Gottesman, R.F. Hemoglobin, Anemia, and Cognitive Function: The Atherosclerosis Risk in Communities Study. J. Gerontol. Ser. A 2016, 71, 772–779. [Google Scholar] [CrossRef] [Green Version]
- Odden, M.C.; Shlipak, M.G.; Tager, I.B. Serum creatinine and functional limitation in elderly persons. J. Gerontol. Ser. A 2009, 64, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Elias, M.F.; Elias, P.K.; Seliger, S.L.; Narsipur, S.S.; Dore, G.A.; Robbins, M.A. Chronic kidney disease, creatinine and cognitive functioning. Nephrol. Dial. Transplant. 2009, 24, 2446–2452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, P.S.; Campos, A.S.D.; Corrêa, C.S.; Dias, C.J.M.; Mostarda, C.T.; Amorim, C.E.N.; Garcia, A.M.C. Effects of Chronic Physical Activity on Glomerular Filtration Rate, Creatinine, and the Markers of Anemia of Kidney Transplantation Patients. Transplant. Proc. 2018, 50, 746–749. [Google Scholar] [CrossRef]
- Fragala, M.S.; Bi, C.; Chaump, M.; Kaufman, H.W.; Kroll, M.H. Associations of aerobic and strength exercise with clinical laboratory test values. PLoS ONE 2017, 12, e0180840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimopoulos, N.; Piperi, C.; Salonicioti, A.; Psarra, V.; Mitsonis, C.; Liappas, I.; Lea, R.W.; Kalofoutis, A. Characterization of the lipid profile in dementia and depression in the elderly. J. Geriatr. Psychiatry Neurol. 2007, 20, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Castano, E.M.; Prelli, F.; Wisniewski, T.; Golabek, A.; Kumar, R.A.; Soto, C.; Frangione, B. Fibrillogenesis in Alzheimer’s disease of amyloid beta peptides and apolipoprotein E. Biochem. J. 1995, 306, 599–604. [Google Scholar] [CrossRef]
- Cockerill, G.W.; Rye, K.A.; Gamble, J.R.; Vadas, M.A.; Barter, P.J. High-density lipoproteins inhibit cytokine-induced expression of endothelial cell adhesion molecules. Arter. Thromb. Vasc. Biol. 1995, 15, 1987–1994. [Google Scholar] [CrossRef]
- He, Q.; Li, Q.; Zhao, J.; Wu, T.; Ji, L.; Huang, G.; Ma, F. Relationship between plasma lipids and mild cognitive impairment in the elderly Chinese: A case-control study. Lipids Health Dis. 2016, 15, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Male (n = 1348) | Female (n = 1398) | p-Value | Post-hoc | ||
|---|---|---|---|---|---|---|
| Normality (n = 1232) a | Cognitive Impairment (n = 116) b | Normality (n = 1153) c | Cognitive Impairment (n = 245) d | |||
| Age (years) | 70.60 ± 5.03 | 74.50 ± 6.76 | 71.65 ± 5.39 | 74.73 ± 7.07 | <0.000 | a vs. b, c, d b vs. c c vs. d |
| Height (cm) | 166.3 ± 5.69 | 165.8 ± 5.86 | 152.9 ± 5.42 | 165.2 ± 5.75 | <0.000 | a vs. c, d b vs. c, d |
| Weight (kg) | 66.98 ± 9.32 | 65.50 ± 10.70 | 57.82 ± 8.62 | 56.30 ± 8.60 | <0.000 | a vs. c, d b vs. c, d |
| BMI (kg/m2) | 24.18 ± 2.83 | 23.79 ± 3.43 | 24.72 ± 3.27 | 24.27 ± 3.32 | <0.000 | a vs. c b vs. c |
| WC (cm) | 84.99 ± 7.65 | 84.00 ± 9.10 | 81.40 ± 8.29 | 81.70 ± 8.97 | <0.000 | a vs. c, d b vs. c |
| SBP (mmHg) | 131.0 ± 14.5 | 129.6 ± 15.5 | 132.8 ± 15.1 | 133.1 ± 17.5 | 0.007 | a vs. c |
| DBP (mmHg) | 76.46 ± 9.28 | 74.38 ± 9.89 | 76.78 ± 9.49 | 76.01 ± 10.06 | 0.071 | - |
| Unadjusted | Adjusted a | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Physical activity Engaging in 150 min MVPA per week Not engaging in 150 min MVPA per week | 1.00 1.63 (1.28–2.08) | <0.000 | 1.00 1.35 (1.05–1.74) | 0.019 |
| Variables | Normality Elderly | Cognitive Impairment Elderly | p-Value | Post-Hoc | ||
|---|---|---|---|---|---|---|
| ≥150 Min (n = 932) a | <150 Min (n = 1453) b | ≥150 Min (n = 102) c | <150 Min (n = 259) d | |||
| Hemoglobin (g/dL) | 14.76 ± 1.30 | 13.74 ± 1.38 | 14.51 ± 1.57 | 13.20 ± 1.31 | <0.000 | a vs. b, d b vs. c, d c vs. d |
| Creatinine (mg/dL) | 1.09 ± 0.56 | 0.90 ± 0.24 | 1.10 ± 0.26 | 0.93 ± 0.48 | <0.000 | a vs. b, d b vs. c c vs. d |
| TC (mg/dL) | 184.8 ± 37.7 | 191.3 ± 40.6 | 168.0 ± 40.9 | 191.8 ± 43.6 | <0.000 | a vs. b, c b vs. c c vs. d |
| TG (mg/dL) | 111.3 ± 64.2 | 120.7 ± 71.6 | 101.9 ± 54.0 | 117.6 ± 62.2 | 0.018 | - |
| LDL-C (mg/dL) | 108.8 ± 34.5 | 111.2 ± 36.5 | 95.6 ± 33.1 | 115.0 ± 36.8 | 0.002 | a vs. c b vs. c c vs. d |
| HDL-C (mg/dL) | 56.31 ± 13.3 | 53.58 ± 13.8 | 55.43 ± 12.5 | 53.21 ± 18.0 | 0.001 | a vs. b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.-T.; Jung, Y.Z.; Akama, T.; Lee, E. Physical Activity Amount and Cognitive Impairment in Korean Elderly Population. Brain Sci. 2020, 10, 804. https://doi.org/10.3390/brainsci10110804
Lim S-T, Jung YZ, Akama T, Lee E. Physical Activity Amount and Cognitive Impairment in Korean Elderly Population. Brain Sciences. 2020; 10(11):804. https://doi.org/10.3390/brainsci10110804
Chicago/Turabian StyleLim, Seung-Taek, Yung Zoon Jung, Takao Akama, and Eunjae Lee. 2020. "Physical Activity Amount and Cognitive Impairment in Korean Elderly Population" Brain Sciences 10, no. 11: 804. https://doi.org/10.3390/brainsci10110804
APA StyleLim, S. -T., Jung, Y. Z., Akama, T., & Lee, E. (2020). Physical Activity Amount and Cognitive Impairment in Korean Elderly Population. Brain Sciences, 10(11), 804. https://doi.org/10.3390/brainsci10110804