The Evaluation of AREG, MMP-2, CHI3L1, GFAP, and OPN Serum Combined Value in Astrocytic Glioma Patients’ Diagnosis and Prognosis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group and Blood Collection
2.2. Protein Concentration Measurement
2.3. Statistical Analysis
3. Results
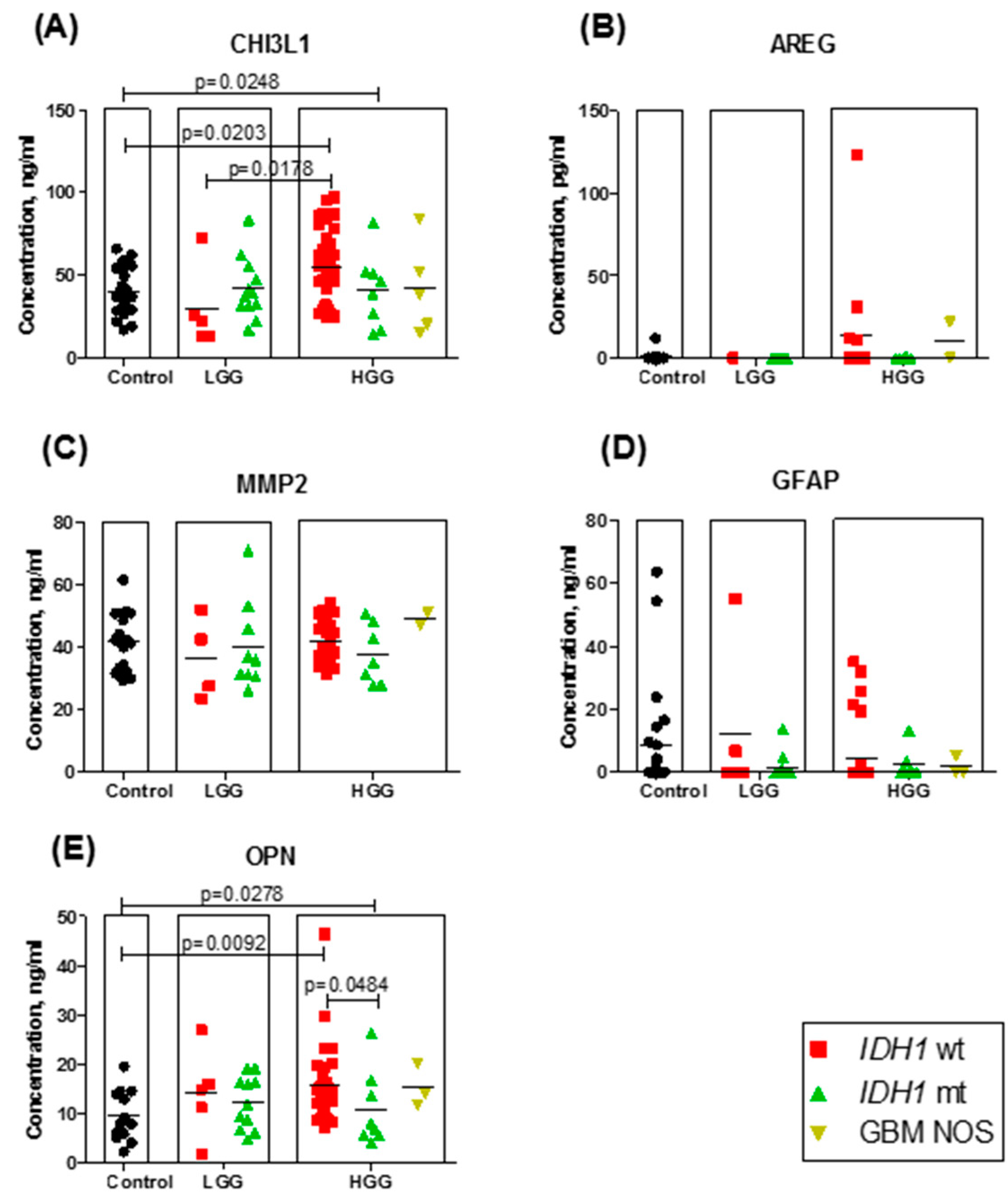
3.1. Protein Serum Concentration Dependence on Tumor Grade and IDH Mutational Status within Grades
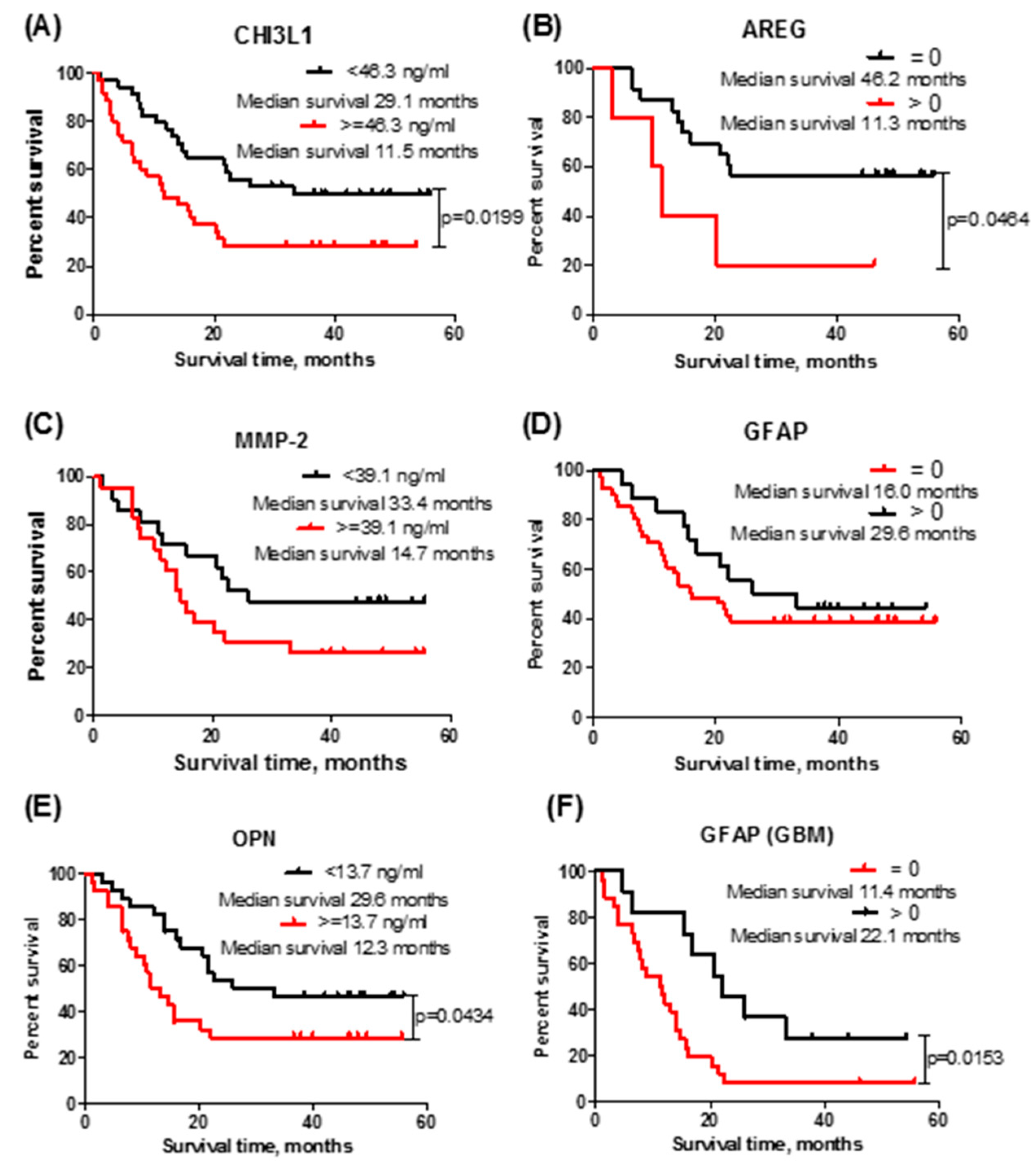
3.2. Protein Serum Concentrations Associated with Patient Survival
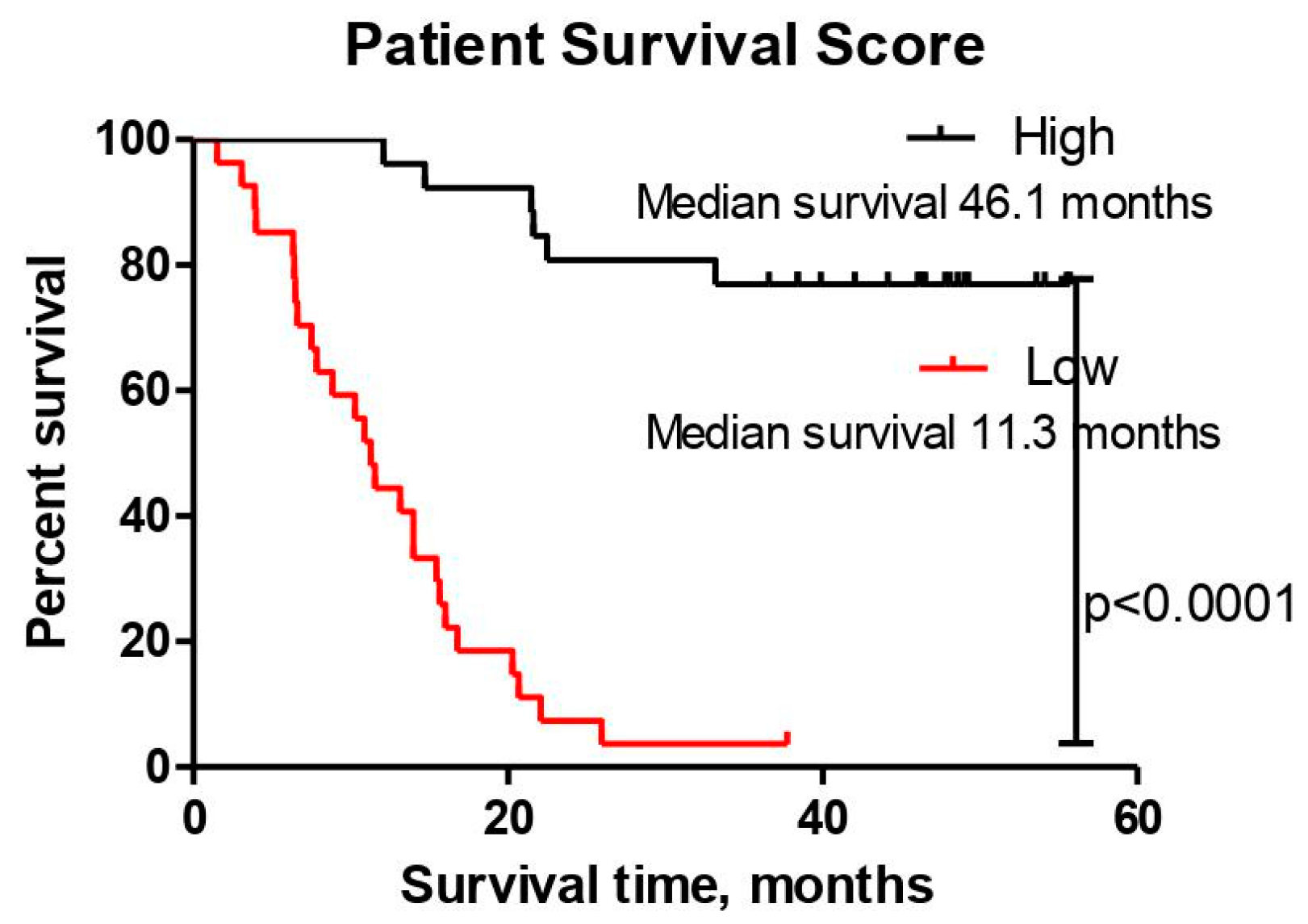
3.3. The Patient Survival Score in Predicting Glioma Patient Outcome
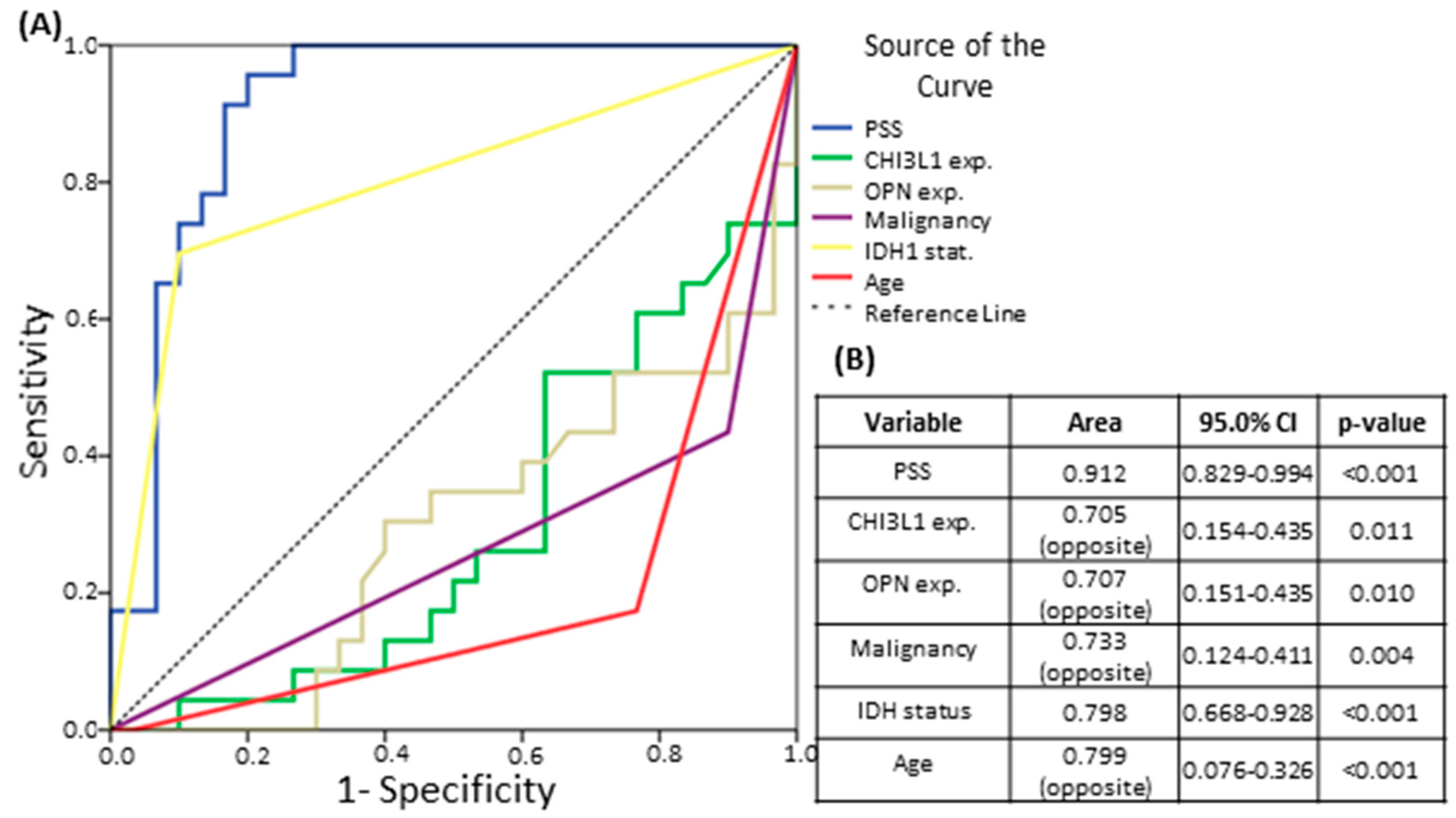
3.4. The Patient Survival Score’s Ability to Predict Survival in Comparison to IDH Mutational Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hofer, S.; Rushing, E.; Preusser, M.; Marosi, C. Molecular biology of high-grade gliomas: What should the clinician know? Chin. J. Cancer 2014, 33, 4–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostrom, Q.T.; Bauchet, L.; Davis, F.G.; Deltour, I.; Fisher, J.L.; Langer, C.E.; Pekmezci, M.; Schwartzbaum, J.A.; Turner, M.C.; Walsh, K.M.; et al. The epidemiology of glioma in adults: A “state of the science” review. Neuro. Oncol. 2014, 16, 896–913. [Google Scholar] [CrossRef] [Green Version]
- Johansen, J.S.; Schultz, N.A.; Jensen, B. V Plasma YKL-40: A potential new cancer biomarker? Future Oncol. 2009, 5, 1065–1082. [Google Scholar] [CrossRef]
- Tanwar, M.K.; Gilbert, M.R.; Holland, E.C. Gene expression microarray analysis reveals YKL-40 to be a potential serum marker for malignant character in human glioma. Cancer Res. 2002, 62, 4364–4368. [Google Scholar] [PubMed]
- Hormigo, A.; Gu, B.; Karimi, S.; Riedel, E.; Panageas, K.S.; Edgar, M.A.; Tanwar, M.K.; Rao, J.S.; Fleisher, M.; DeAngelis, L.M.; et al. YKL-40 and matrix metalloproteinase-9 as potential serum biomarkers for patients with high-grade gliomas. Clin. Cancer Res. 2006, 12, 5698–5704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazakova, M.H.; Staneva, D.N.; Koev, I.G.; Staikov, D.G.; Mateva, N.; Timonov, P.T.; Miloshev, G.A.; Sarafian, V.S. Protein and mRNA levels of YKL-40 in high-grade glioma. Folia Biol. 2014, 60, 261. [Google Scholar]
- Bernardi, D.; Padoan, A.; Ballin, A.; Sartori, M.T.; Manara, R.; Scienza, R.; Plebani, M.; Della Puppa, A. Serum YKL-40 following resection for cerebral glioblastoma. J. Neurooncol. 2012, 107, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Koev, I.G.; Feodorova, Y.N.; Kazakova, M.H.; Staykov, D.G.; Kitov, B.D.; Sarafian, V.S. Glioblastoma Multiforme Classified as Mesenchymal Subtype. Folia Med. 2014, 56, 215–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berasain, C.; Avila, M.A. Amphiregulin. Semin. Cell Dev. Biol. 2014, 28, 31–41. [Google Scholar] [CrossRef]
- Zaiss, D.M.W.; Gause, W.C.; Osborne, L.C.; Artis, D. Emerging functions of amphiregulin in orchestrating immunity, inflammation, and tissue repair. Immunity 2015, 42, 216–226. [Google Scholar] [CrossRef] [Green Version]
- Han, S.X.; Bai, E.; Jin, G.H.; He, C.C.; Guo, X.J.; Wang, L.J.; Li, M.; Ying, X.; Zhu, Q. Expression and clinical significance of YAP, TAZ, and AREG in hepatocellular carcinoma. J. Immunol. Res. 2014, 2014. [Google Scholar] [CrossRef]
- Marie, S.K.N.; Okamoto, O.K.; Uno, M.; Hasegawa, A.P.G.; Oba-Shinjo, S.M.; Cohen, T.; Camargo, A.A.; Kosoy, A.; Carlotti, C.G.; Toledo, S.; et al. Maternal embryonic leucine zipper kinase transcript abundance correlates with malignancy grade in human astrocytomas. Int. J. Cancer 2008, 122, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Lorente, M.; Carracedo, A.; Torres, S.; Natali, F.; Agia, A.; Hernanández-Tiedra, S.; Salazar, M.; Blázquez, C.; Guzmán, M.; Velasco, G. Amphiregulin is a factor for resistance of glioma cells to cannabinoid-induced apoptosis. Glia 2009, 57, 1374–1385. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Werb, Z. The many faces of metalloproteases: Cell growth, invasion, angiogenesis and metastasis. Trends Cell Biol. 2001, 11, S37–S43. [Google Scholar] [CrossRef]
- Smith, E.R.; Zurakowski, D.; Saad, A.; Scott, R.M.; Moses, M.A. Urinary biomarkers predict brain tumor presence and response to therapy. Clin. Cancer Res. 2008, 14, 2378–2386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, M. Role of GFAP in CNS injuries. Neurosci. Lett. 2014, 565, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Jung, C.S.; Foerch, C.; Schänzer, A.; Heck, A.; Plate, K.H.; Seifert, V.; Steinmetz, H.; Raabe, A.; Sitzer, M. Serum GFAP is a diagnostic marker for glioblastoma multiforme. Brain 2007, 130, 3336–3341. [Google Scholar] [CrossRef]
- van Bodegraven, E.J.; van Asperen, J.V.; Robe, P.A.J.; Hol, E.M. Importance of GFAP isoform-specific analyses in astrocytoma. Glia 2019, 67, 1417–1433. [Google Scholar] [CrossRef]
- Lund, S.A.; Giachelli, C.M.; Scatena, M. The role of osteopontin in inflammatory processes. J. Cell Commun. Signal. 2009, 3, 311–322. [Google Scholar] [CrossRef] [Green Version]
- Sase, S.P.; Ganu, J.V.; Nagane, N. Osteopontin: A Novel Protein Molecule. Ind. Med. Gaz. 2012, 146, 62–66. [Google Scholar]
- Sreekanthreddy, P.; Srinivasan, H.; Kumar, D.M.; Nijaguna, M.B.; Sridevi, S.; Vrinda, M.; Arivazhagan, A.; Balasubramaniam, A.; Hegde, A.S.; Chandramouli, B.A.; et al. Identification of potential serum biomarkers of glioblastoma: Serum osteopontin levels correlate with poor prognosis. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1409–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, M.G.; Sol, N.; Zijl, S.; Reijneveld, J.C.; Wesseling, P.; Wurdinger, T. Liquid biopsies in patients with diffuse glioma. Acta Neuropathol. 2015, 129, 849–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabouret, E.; Bertucci, F.; Pierga, J.-Y.; Petit, T.; Levy, C.; Ferrero, J.-M.; Campone, M.; Gligorov, J.; Lerebours, F.; Roché, H.; et al. MMP2 and MMP9 serum levels are associated with favorable outcome in patients with inflammatory breast cancer treated with bevacizumab-based neoadjuvant chemotherapy in the BEVERLY-2 study. Oncotarget 2016, 7, 18531–18540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiss, Y.; Machein, M.R.; Plate, K.H. The role of angiopoietins during angiogenesis in gliomas. Brain Pathol. 2005, 15, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Güttler, A.; Giebler, M.; Cuno, P.; Wichmann, H.; Keßler, J.; Ostheimer, C.; Söling, A.; Strauss, C.; Illert, J.; Kappler, M.; et al. Osteopontin and splice variant expression level in human malignant glioma: Radiobiologic effects and prognosis after radiotherapy. Radiother. Oncol. 2013, 108, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Sincevičiūtė, R.; Vaitkienė, P.; Urbanavičiūtė, R.; Steponaitis, G.; Tamašauskas, A.; Skiriutė, D. MMP2 is associated with glioma malignancy and patient outcome. Int. J. Clin. Exp. Pathol. 2018, 11, 3010–3018. [Google Scholar]
- Steponaitis, G.; Kazlauskas, A.; Skiriute, D.; Vaitkiene, P.; Skauminas, K.; Tamasauskas, A. Significance of Amphiregulin (AREG) for the Outcome of Low and High Grade Astrocytoma Patients. J. Cancer 2019, 10, 1479–1488. [Google Scholar] [CrossRef]
- Håvik, A.B.; Brandal, P.; Honne, H.; Dahlback, H.S.S.; Scheie, D.; Hektoen, M.; Meling, T.R.; Helseth, E.; Heim, S.; Lothe, R.A.; et al. MGMT promoter methylation in gliomas-assessment by pyrosequencing and quantitative methylation-specific PCR. J. Transl. Med. 2012, 10, 36. [Google Scholar] [CrossRef] [Green Version]
- Fiano, V.; Trevisan, M.; Trevisan, E.; Senetta, R.; Castiglione, A.; Sacerdote, C.; Gillio-Tos, A.; De Marco, L.; Grasso, C.; Magistrello, M.; et al. MGMT promoter methylation in plasma of glioma patients receiving temozolomide. J. Neurooncol. 2014, 117, 347–357. [Google Scholar] [CrossRef] [Green Version]
- Lv, S.; Teugels, E.; Sadones, J.; Quartier, E.; Huylebrouck, M.; Du Four, S.; Le Mercier, M.; De Witte, O.; Salmon, I.; Michotte, A.; et al. Correlation between IDH1 gene mutation status and survival of patients treated for recurrent glioma. Anticancer Res. 2011, 31, 4457–4463. [Google Scholar]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, E.A.; Shabbeer, S.; Kenny, P.A. Normal range of serum Amphiregulin in healthy adult human females. Clin. Biochem. 2012, 45, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Kai, H.; Ikeda, H.; Yasukawa, H.; Kai, M.; Seki, Y.; Kuwahara, F.; Ueno, T.; Sugi, K.; Imaizumi, T. Peripheral blood levels of matrix metalloproteases-2 and -9 are elevated in patients with acute coronary syndromes. J. Am. Coll. Cardiol. 1998, 32, 368–372. [Google Scholar] [CrossRef] [Green Version]
- RayBiotech. Human Amphiregulin ELISA. Available online: https://www.raybiotech.com/human-ar-amphiregulin-elisa-kit-available-serum-plasma-cell-culture-supernatant-and-urine/ (accessed on 9 July 2020).
- Abcam. Human Osteopontin ELISA Kit (ab192143). Available online: https://www.abcam.com/human-osteopontin-elisa-kit-ab192143.html (accessed on 9 July 2020).
- MMP2 Human ELISA Kit. Available online: https://www.thermofisher.com/elisa/product/MMP2-Human-ELISA-Kit/KHC3081 (accessed on 9 July 2020).
- Human GFAP DuoSet ELISA. Available online: https://www.rndsystems.com/products/human-gfap-duoset-elisa_dy2594-05 (accessed on 9 July 2020).
- Human Chitinase 3-like 1 DuoSet ELISA. Available online: https://www.rndsystems.com/products/human-chitinase-3-like-1-duoset-elisa_dy2599 (accessed on 9 July 2020).
- Zhou, M.; Zhang, Z.; Zhao, H.; Bao, S.; Sun, J. A novel lncRNA-focus expression signature for survival prediction in endometrial carcinoma. BMC Cancer 2018, 18, 39. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.-H.; Pan, Z.-Y.; Wang, Z.-F.; Ma, C.; Weng, H.; Li, Z.-Q. YKL-40 in high-grade glioma: Prognostic value of protein versus mRNA expression. Glioma 2018, 1, 104. [Google Scholar] [CrossRef]
- Akiyama, Y.; Ashizawa, T.; Komiyama, M.; Miyata, H.; Oshita, C.; Omiya, M.; Iizuka, A.; Kume, A.; Sugino, T.; Hayashi, N.; et al. YKL-40 downregulation is a key factor to overcome temozolomide resistance in a glioblastoma cell line. Oncol. Rep. 2014, 32, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, N.; Daigo, Y.; Takano, A.; Taniwaki, M.; Kato, T.; Hayama, S.; Murakami, H.; Takeshima, Y.; Inai, K.; Nishimura, H.; et al. Increases of amphiregulin and transforming growth factor-α in serum as predictors of poor response to gefitinib among patients with advanced non-small cell lung cancers. Cancer Res. 2005, 65, 9176–9184. [Google Scholar] [CrossRef] [Green Version]
- Ramachandran, R.K.; Sørensen, M.D.; Aaberg-Jessen, C.; Hermansen, S.K.; Kristensen, B.W. Expression and prognostic impact of matrix metalloproteinase-2 (MMP-2) in astrocytomas. PLoS ONE 2017, 12, e0172234. [Google Scholar] [CrossRef] [Green Version]
- Uyeda, C.T.; Eng, L.F.; Bignami, A. Immunological study of the glial fibrillary acidic protein. Brain Res. 1972, 37, 81–89. [Google Scholar] [CrossRef]
- Tichy, J.; Spechtmeyer, S.; Mittelbronn, M.; Hattingen, E.; Rieger, J.; Senft, C.; Foerch, C. Prospective evaluation of serum glial fibrillary acidic protein (GFAP) as a diagnostic marker for glioblastoma. J. Neurooncol. 2016, 126, 361–369. [Google Scholar] [CrossRef]
- Ilhan-Mutlu, A.; Wagner, L.; Widhalm, G.; Wöhrer, A.; Bartsch, S.; Czech, T.; Heinzl, H.; Leutmezer, F.; Prayer, D.; Marosi, C.; et al. Exploratory investigation of eight circulating plasma markers in brain tumor patients. Neurosurg. Rev. 2013, 36, 45–55; discussion 55–56. [Google Scholar] [CrossRef] [PubMed]
- Lange, R.P.; Everett, A.; Dulloor, P.; Korley, F.K.; Bettegowda, C.; Blair, C.; Grossman, S.A.; Holdhoff, M. Evaluation of eight plasma proteins as candidate blood-based biomarkers for malignant gliomas. Cancer Investig. 2014, 32, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, J.; Hol, E.M. GFAP in health and disease. Prog. Neurobiol. 2011, 93, 421–443. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Xu, H.; Liang, F.; He, J.; Zhang, J. Association of osteopontin expression with the prognosis of glioma patient: A meta-analysis. Tumor Biol. 2014, 36, 429–436. [Google Scholar] [CrossRef]
- Denhardt, D.T.; Chambers, A.F. Overcoming obstacles to metastasis—Defenses against host defenses: Osteopontin (OPN) as a shield against attack by cytotoxic host cells. J. Cell. Biochem. 1994, 56, 48–51. [Google Scholar] [CrossRef]
- Wulfkuhle, J.D.; Liotta, L.A.; Petricoin, E.F. Proteomic applications for the early detection of cancer. Nat. Rev. Cancer 2003, 3, 267–275. [Google Scholar] [CrossRef]
- Elstner, A.; Stockhammer, F.; Nguyen-Dobinsky, T.N.; Nguyen, Q.L.; Pilgermann, I.; Gill, A.; Guhr, A.; Zhang, T.; Von Eckardstein, K.; Picht, T.; et al. Identification of diagnostic serum protein profiles of glioblastoma patients. J. Neurooncol. 2011, 102, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Zhang, G.; Zhang, J.; Gao, G.; Li, M.; Chen, Y.; Wang, J.; Li, G.; Song, S.W.; Qiu, X.; et al. A panel of four cytokines predicts the prognosis of patients with malignant gliomas. J. Neurooncol. 2013, 114, 199–208. [Google Scholar] [CrossRef]
- Pérez-Larraya, J.G.; Paris, S.; Idbaih, A.; Dehais, C.; Laigle-Donadey, F.; Navarro, S.; Capelle, L.; Mokhtari, K.; Marie, Y.; Sanson, M.; et al. Diagnostic and prognostic value of preoperative combined GFAP, IGFBP-2, and YKL-40 plasma levels in patients with glioblastoma. Cancer 2014, 120, 3972–3980. [Google Scholar] [CrossRef]
- Nijaguna, M.B.; Patil, V.; Hegde, A.S.; Chandramouli, B.A.; Arivazhagan, A.; Santosh, V.; Somasundaram, K. An eighteen serum cytokine signature for discriminating Glioma from normal healthy individuals. PLoS ONE 2015, 10, e0137524. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Univariate Cox Regression | Multivariate Cox Regression | ||||||
|---|---|---|---|---|---|---|---|
| Factor | HR | 95.0% CI for HR | p-Value | Step | HR | 95.0% CI for HR | p-Value |
| Age | 6.866 | 3.436–13.729 | <0.001 | ||||
| Gender | 1.310 | 0.726–2.361 | 0.370 | ||||
| Malignancy | 7.854 | 2.804–21.998 | <0.001 | ||||
| MGMT methylation | 0.793 | 0.429–1.466 | 0.459 | ||||
| IDH1 status | 6.786 | 2.828–16.287 | <0.001 | 3 | 0.113 | 0.038–0.339 | <0.001 |
| CHI3L1 expression | 1.013 | 1.001–1.025 | 0.039 | 3 | 1.023 | 1.007–1.040 | 0.005 |
| OPN expression | 1.094 | 1.046–1.144 | <0.001 | 3 | 1.092 | 1.038–1.149 | 0.001 |
| AREG expression | 1.050 | 1.009–1.093 | 0.017 | ||||
| MMP-2 expression | 1.013 | 0.983–1.051 | 0.343 | ||||
| GFAP expression | 1.005 | 0.974–1.038 | 0.742 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbanavičiūtė, R.; Skauminas, K.; Skiriutė, D. The Evaluation of AREG, MMP-2, CHI3L1, GFAP, and OPN Serum Combined Value in Astrocytic Glioma Patients’ Diagnosis and Prognosis. Brain Sci. 2020, 10, 872. https://doi.org/10.3390/brainsci10110872
Urbanavičiūtė R, Skauminas K, Skiriutė D. The Evaluation of AREG, MMP-2, CHI3L1, GFAP, and OPN Serum Combined Value in Astrocytic Glioma Patients’ Diagnosis and Prognosis. Brain Sciences. 2020; 10(11):872. https://doi.org/10.3390/brainsci10110872
Chicago/Turabian StyleUrbanavičiūtė, Rūta, Kęstutis Skauminas, and Daina Skiriutė. 2020. "The Evaluation of AREG, MMP-2, CHI3L1, GFAP, and OPN Serum Combined Value in Astrocytic Glioma Patients’ Diagnosis and Prognosis" Brain Sciences 10, no. 11: 872. https://doi.org/10.3390/brainsci10110872
APA StyleUrbanavičiūtė, R., Skauminas, K., & Skiriutė, D. (2020). The Evaluation of AREG, MMP-2, CHI3L1, GFAP, and OPN Serum Combined Value in Astrocytic Glioma Patients’ Diagnosis and Prognosis. Brain Sciences, 10(11), 872. https://doi.org/10.3390/brainsci10110872