Dreaming and Insomnia: Link between Physiological REM Parameters and Mentation Characteristics


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Questionnaires
2.4. PSG and EEG Analyses
2.5. Awakening Procedure
2.6. Statistical Analyses
3. Results
3.1. Sample Description
3.2. Number of Arousals and REM Density
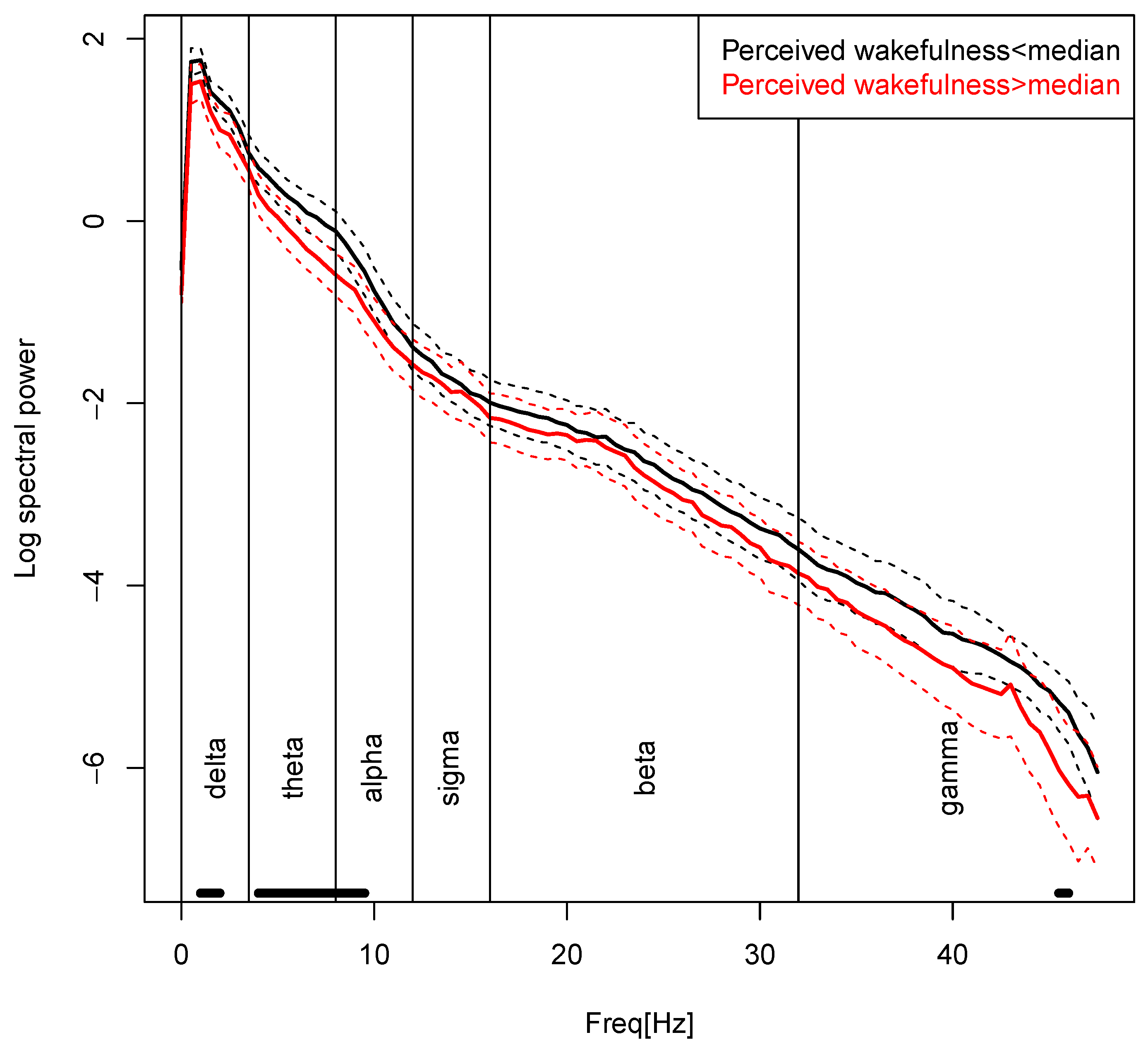
3.3. Spectral Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Morin, C.M.; Drake, C.L.; Harvey, A.G.; Krystal, A.D.; Manber, R.; Riemann, D.; Spiegelhalder, K. Insomnia disorder. Nat. Rev. Dis. Primer 2015, 1, 15026. [Google Scholar] [CrossRef]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef]
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kyle, S.D.; Morgan, K.; Espie, C.A. Insomnia and health-related quality of life. Sleep Med. Rev. 2010, 14, 69–82. [Google Scholar] [CrossRef]
- Sofi, F.; Cesari, F.; Casini, A.; Macchi, C.; Abbate, R.; Gensini, G.F. Insomnia and risk of cardiovascular disease: A meta-analysis. Eur. J. Prev. Cardiol. 2014, 21, 57–64. [Google Scholar] [CrossRef]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Fröjmark, M.; Palagini, L.; Rücker, G.; Riemann, D.; et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef]
- Harvey, A.G.; Tang, N.K.Y. (Mis)perception of sleep in insomnia: A puzzle and a resolution. Psychol. Bull. 2012, 138, 77–101. [Google Scholar] [CrossRef] [PubMed]
- Mercer, J.D.; Bootzin, R.R.; Lack, L.C. Insomniacs’ Perception of Wake Instead of Sleep. Sleep 2002, 25, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Means, M. Accuracy of sleep perceptions among insomnia sufferers and normal sleepers. Sleep Med. 2003, 4, 285–296. [Google Scholar] [CrossRef]
- Feige, B.; Nissen, C.; Voderholzer, U.; Hornyak, M.; Spiegelhalder, K.; Kloepfer, C.; Perlis, M.; Riemann, D.; Al-Shajlawi, A. Does REM sleep contribute to subjective wake time in primary insomnia? A comparison of polysomnographic and subjective sleep in 100 patients. J. Sleep Res. 2008, 17, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, M.H.; Arand, D.L. Hyperarousal and insomnia: State of the science. Sleep Med. Rev. 2010, 14, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.L.; Nissen, C. The hyperarousal model of insomnia: A review of the concept and its evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Spiegelhalder, K.; Nissen, C.; Hirscher, V.; Baglioni, C.; Feige, B. REM Sleep Instability—A New Pathway for Insomnia? Pharmacopsychiatry 2012, 45, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Maquet, P.; Peters, J.-M.; Aerts, J.; Delfiore, G.; Degueldre, C.; Luxen, A.; Franck, G. Functional neuroanatomy of human rapid-eye-movement sleep and dreaming. Nature 1996, 383, 163–166. [Google Scholar] [CrossRef]
- Schredl, M.; Schäfer, G.; Weber, B.; Heuser, I. Dreaming and insomnia: Dream recall and dream content of patients with insomnia. J. Sleep Res. 1998, 7, 191–198. [Google Scholar] [CrossRef]
- Pérusse, A.D.; De Koninck, J.; Pedneault-Drolet, M.; Ellis, J.; Bastien, C. REM dream activity of insomnia sufferers: A systematic comparison with good sleepers. Sleep Med. 2016, 20, 147–154. [Google Scholar] [CrossRef]
- Schredl, M. Dreams in patients with sleep disorders. Sleep Med. Rev. 2009, 13, 215–221. [Google Scholar] [CrossRef]
- Hall, C.; Nordby, V. The Individual and His Dreams; New American Library: New York, NY, USA, 1972. [Google Scholar]
- Ermann, M. Die Traumerinnerung bei Patienten mit psychogenen Schlafstörungen: Empirische Befunde und einige Folgerungen für das Verständnis des Träumens. In Traum und Gedächtnis: Neue Ergebnisse aus Psychologischer, Psychoanalytischer und Neurophysiologischer Forschung; Leuschner, W., Hau, S., Eds.; LIT Verlag: Münster, Germany, 1995; pp. 165–186. [Google Scholar]
- Feige, B.; Nanovska, S.; Baglioni, C.; Bier, B.; Cabrera, L.; Diemers, S.; Quellmalz, M.; Siegel, M.; Xeni, I.; Szentkiralyi, A.; et al. Insomnia—perchance a dream? Results from a NREM/REM sleep awakening study in good sleepers and patients with insomnia. Sleep 2018, 41. [Google Scholar] [CrossRef]
- Pivik, R. Tonic states and phasic events in relation to sleep mentation. In The Mind in Sleep: Psychology and Psychophysiology; Wiley Series on Personality Processes; Ellman, S.J., Antrobus, J.S., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 1991; pp. 214–247. [Google Scholar]
- Sallinen, M.; Kaartinen, J.; Lyytinen, H. Processing of auditory stimuli during tonic and phasic periods of REM sleep as revealed by event-related brain potentials. J. Sleep Res. 1996, 5, 220–228. [Google Scholar] [CrossRef]
- Schädlich, S.; Warmuth, R.; Rodenbeck, A.; Danker-Hopfe, H.; Frohnhofen, H.; Penzel, T.; Popp, R.; Raschke, F.; Bögel, M.; Orth, M.; et al. Leitfaden und Kriterien für die Akkreditierung von Schlaflaboren der Deutschen Gesellschaft für Schlafforschung und Schlafmedizin (DGSM). Somnologie 2017, 21, 200–209. [Google Scholar] [CrossRef]
- Wittchen, H. Strukturiertes Klinisches Interview Für DSM-IV; Hogrefe: Göttingen, Germany, 1991. [Google Scholar]
- Bastien, C. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broomfield, N.M.; Espie, C.A. Towards a valid, reliable measure of sleep effort. J. Sleep Res. 2005, 14, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.L.; Richardson, G.; Roehrs, T.; Scofield, H.; Roth, T. Vulnerability to Stress-related Sleep Disturbance and Hyperarousal. Sleep 2004, 27, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Jarrin, D.C.; Chen, I.Y.; Ivers, H.; Drake, C.L.; Morin, C.M. Temporal Stability of the Ford Insomnia Response to Stress Test (FIRST). J. Clin. Sleep Med. 2016, 12, 1373–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional Beliefs and Attitudes about Sleep (DBAS): Validation of a Brief Version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Nicassio, P.M.; Mendlowitz, D.R.; Fussell, J.J.; Petras, L. The phenomenology of the pre-sleep state: The development of the pre-sleep arousal scale. Behav. Res. Ther. 1985, 23, 263–271. [Google Scholar] [CrossRef]
- Beck, A.T. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561. [Google Scholar] [CrossRef] [Green Version]
- Spielberger, C.D. State-Trait Anxiety Inventory. In The Corsini Encyclopedia of Psychology; Weiner, I.B., Craighead, W.E., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar] [CrossRef]
- Rechtschaffen, A. Manual of Standardized Terminology, Techniques, and Scoring System for Sleep Stages of Human Subjects; US Government Printing Office, National Institutes of Health: Washington, DC, USA, 1968. [Google Scholar]
- Iber, C. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Westchester, NY, USA, 2007. [Google Scholar]
- Sleep Disorders Atlas Task Force of the American Sleep Disorders Association. EEG arousals: Scoring rules and examples. Sleep 1992, 15, 173–184. [Google Scholar] [CrossRef]
- Feige, B. Fluoxetine and Sleep EEG Effects of a Single Dose, Subchronic Treatment, and Discontinuation in Healthy Subjects. Neuropsychopharmacology 2002, 26, 246–258. [Google Scholar] [CrossRef]
- Feige, B.; Voderholzer, U.; Riemann, D.; Hohagen, F.; Berger, M. Independent sleep EEG slow-wave and spindle band dynamics associated with 4 weeks of continuous application of short-half-life hypnotics in healthy subjects. Clin. Neurophysiol. 1999, 110, 1965–1974. [Google Scholar] [CrossRef]
- Weigand, D.; Michael, L.; Schulz, H. When sleep is perceived as wakefulness: An experimental study on state perception during physiological sleep. J. Sleep Res. 2007, 16, 346–353. [Google Scholar] [CrossRef]
- Wittmann, L.; Palmy, C.; Schredl, M. NREM sleep dream recall, dream report length and cortical activation. Sleep Hypn. 2004, 6, 54–58. [Google Scholar]
- Wehrle, R.; CzischM, M.; Kaufmann, C.; Wetter, T.C.; Holsboer, F.; Auer, D.P.; Pollmächer, T. Rapid eye movement-related brain activation in human sleep: A functional magnetic resonance imaging study. Neuroreport 2005, 16, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Callaway, C.W.; Lydic, R.; Baghdoyan, H.A.; Hobson, J.A. Pontogeniculooccipital waves: Spontaneous visual system activity during rapid eye movement sleep. Cell. Mol. Neurobiol. 1987, 7, 105–149. [Google Scholar] [CrossRef]
- Wehrle, R.; Kaufmann, C.; Wetter, T.C.; Holsboer, F.; Auer, D.; Pollmächer, T.; Czisch, M. Functional microstates within human REM sleep: First evidence from fMRI of a thalamocortical network specific for phasic REM periods: Thalamocortical network in phasic REM sleep. Eur. J. Neurosci. 2007, 25, 863–871. [Google Scholar] [CrossRef]
- Merica, H.; Blois, R.; Gaillard, J.-M. Spectral characteristics of sleep EEG in chronic insomnia: Sleep EEG spectral characteristics in insomnia. Eur. J. Neurosci. 1998, 10, 1826–1834. [Google Scholar] [CrossRef]
- St-Jean, G.; Turcotte, I.; Pérusse, A.D.; Bastien, C.H. REM and NREM power spectral analysis on two consecutive nights in psychophysiological and paradoxical insomnia sufferers. Int. J. Psychophysiol. 2013, 89, 181–194. [Google Scholar] [CrossRef]
- Krystal, A.D.; Edinger, J.D.; Wohlgemuth, W.K.; Marsh, G.R. NREM Sleep EEG Frequency Spectral Correlates of Sleep Complaints in Primary Insomnia Subtypes. Sleep 2002, 25, 626–636. [Google Scholar] [CrossRef] [Green Version]
- Perlis, M.L.; Nielsen, T.A. Mood regulation, dreaming and nightmares: Evaluation of a desensitization function for REM sleep. Dreaming 1993, 3, 243–257. [Google Scholar] [CrossRef]
- Goldstein, A.N.; Walker, M.P. The Role of Sleep in Emotional Brain Function. Annu. Rev. Clin. Psychol. 2014, 10, 679–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollmächer, T.; Mullington, J.; Lauer, C.J. REM Sleep Disinhibition at Sleep Onset: A Comparison between Narcolepsy and Depression. Biol. Psychiatry 1997, 42, 713–720. [Google Scholar] [CrossRef]
- Ermis, U.; Krakow, K.; Voss, U. Arousal thresholds during human tonic and phasic REM sleep: Arousal threshold in tonic and phasic REM. J. Sleep Res. 2010, 19, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.A. A review of mentation in REM and NREM sleep: “Covert” REM sleep as a possible reconciliation of two opposing models. Behav. Brain Sci. 2000, 23, 851–866. [Google Scholar] [CrossRef]


{kind=link}
| M | F | M | F | |||
|---|---|---|---|---|---|---|
| n | 10 | 13 | 8 | 14 | ||
| Mean ± SD | Mean ± SD | t | p | |||
| Age | 43.09 ± 11.47 | 44.32 ± 11.87 | 0.35 | 0.725 | ||
| Duration of insomnia (years) | 0.00 ± 0.00 | 12.53 ± 16.07 | 3.66 | 0.001 | ||
| BDI | 1.30 ± 2.03 | 9.36 ± 7.03 | 5.17 | 0.000 | ||
| STAI | 27.83 ± 5.13 | 39.19 ± 9.67 | 4.80 | 0.000 | ||
| ISI | 1.96 ± 1.94 | 16.27 ± 4.23 | 14.47 | 0.000 | ||
| ESS | 4.35 ± 2.59 | 7.86 ± 4.11 | 3.42 | 0.002 | ||
| GSES | 0.48 ± 0.85 | 6.36 ± 3.50 | 7.68 | 0.000 | ||
| FIRST | 17.83 ± 4.13 | 24.95 ± 5.35 | 4.99 | 0.000 | ||
| DBAS-16 | 29.09 ± 17.13 | 73.91 ± 22.52 | 7.49 | 0.000 | ||
| PSAS-SA | 8.74 ± 1.25 | 12.45 ± 3.66 | 4.51 | 0.000 | ||
| PSAS-CA | 10.57 ± 2.79 | 19.73 ± 7.90 | 5.14 | 0.000 | ||
| PSQI | 2.57 ± 1.47 | 10.68 ± 3.50 | 10.07 | 0.000 | ||
| Sleep diary | ||||||
| TIB | 483.50 ± 47.33 | 504.41 ± 59.08 | 1.30 | 0.203 | ||
| TST | 439.44 ± 51.04 | 343.70 ± 57.21 | −5.86 | 0.000 | ||
| SEI | 90.84 ± 5.32 | 68.78 ± 12.90 | −7.42 | 0.000 | ||
| SOL | 10.75 ± 4.56 | 42.52 ± 31.02 | 4.75 | 0.000 | ||
| WAKE | 8.14 ± 8.53 | 48.77 ± 46.71 | 4.01 | 0.001 | ||
| EMA | 25.18 ± 21.99 | 69.42 ± 50.82 | 3.75 | 0.001 | ||
| NAP | 5.89 ± 6.41 | 8.55 ± 21.52 | 0.56 | 0.583 | ||
| MOOD_EVE | 4.83 ± 0.94 | 3.89 ± 0.91 | −3.37 | 0.002 | ||
| PERFORMANCE_EVE | 2.00 ± 0.76 | 3.00 ± 0.62 | 4.78 | 0.000 | ||
| EXHAUSTION_EVE | 1.65 ± 0.42 | 1.93 ± 0.51 | 1.98 | 0.055 | ||
| RECOVERY_MOR | 1.80 ± 0.56 | 3.02 ± 0.63 | 6.81 | 0.000 | ||
| MOOD_MOR | 4.95 ± 0.83 | 3.69 ± 0.78 | −5.18 | 0.000 | ||
| GSC (n = 23) Mean ± SD | Patients with ID (n = 22) Mean ± SD | Group | Age | Mentation Clarity | Mentation Visuality | Mentation Control | Positive Feelings | Negative Feelings | Perceived Wakefulness | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | B | F | p | B | F | p | B | F | p | B | F | p | B | F | p | B | F | p | B | F | p | |||
| Multivariate analysis (Wilk’s Lambda) | 0.98 | 0.686 | 0.98 | 0.652 | 0.94 | 0.346 | 0.94 | 0.334 | 0.99 | 0.792 | 0.93 | 0.261 | 0.96 | 0.489 | 0.88 | 0.116 | |||||||||
| Number of arousals | 0.25 ± 0.27 | 0.23 ± 0.36 | 0.04 | 0.844 | 0.00 | 0.01 | 0.906 | 0.01 | 1.20 | 0.280 | −0.19 | 0.15 | 0.701 | −0.06 | 0.00 | 0.973 | 0.06 | 0.26 | 0.615 | 0.12 | 0.91 | 0.347 | −0.14 | 4.68 | 0.037 |
| REM density (%) | 7.28 ± 3.77 | 8.17 ± 3.36 | 0.78 | 0.383 | −0.04 | 0.74 | 0.395 | 0.08 | 0.43 | 0.515 | 3.48 | 1.69 | 0.202 | 1.19 | 0.43 | 0.517 | 0.87 | 1.95 | 0.171 | −1.28 | 1.04 | 0.316 | 0.60 | 0.65 | 0.427 |
| GSC (n = 23) Mean ± SD | Patients with ID (n = 21) Mean ± SD | Group | Age | Mentation Clarity | Mentation Visuality | Mentation Control | Positive Feelings | Negative Feelings | Perceived Wakefulness | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | B | F | p | B | F | p | B | F | p | B | F | p | B | F | p | B | F | p | B | F | p | |||
| Multivariate analysis (Wilk’s Lambda) | 0.92 | 0.863 | 0.75 | 0.171 | 0.88 | 0.688 | 0.89 | 0.734 | 0.97 | 0.990 | 0.92 | 0.861 | 0.83 | 0.412 | 0.64 | 0.025 | |||||||||
| delta 0.1–3.5 Hz | 3.30 ± 0.35 | 3.22 ± 0.37 | 0.69 | 0.413 | 0.00 | 0.26 | 0.616 | −0.11 | 0.66 | 0.422 | −0.14 | 0.31 | 0.581 | −0.04 | 0.00 | 0.981 | −0.09 | 1.78 | 0.191 | −0.07 | 0.45 | 0.509 | −0.18 | 4.96 | 0.032 |
| theta 3.5–8 Hz | 2.36 ± 0.46 | 2.27 ± 0.51 | 0.44 | 0.513 | 0.01 | 0.49 | 0.490 | −0.19 | 0.59 | 0.448 | −0.15 | 0.99 | 0.327 | −0.12 | 0.03 | 0.860 | −0.11 | 1.66 | 0.206 | 0.04 | 0.02 | 0.885 | −0.24 | 5.00 | 0.032 |
| alpha 8–12 Hz | 1.26 ± 0.58 | 1.24 ± 0.64 | 0.06 | 0.810 | 0.01 | 2.32 | 0.137 | −0.08 | 0.08 | 0.779 | −0.16 | 1.33 | 0.257 | −0.09 | 0.00 | 0.950 | −0.15 | 2.01 | 0.165 | −0.14 | 0.79 | 0.381 | −0.35 | 7.59 | 0.009 |
| sigma 12–16 Hz | 0.25 ± 0.68 | 0.31 ± 0.57 | 0.03 | 0.864 | 0.02 | 5.61 | 0.024 | −0.14 | 0.62 | 0.437 | −0.10 | 0.22 | 0.641 | −0.01 | 0.00 | 0.986 | −0.15 | 1.44 | 0.238 | −0.18 | 0.95 | 0.336 | −0.20 | 2.26 | 0.142 |
| beta 16–32 Hz | 0.83 ± 0.76 | 0.86 ± 0.63 | 0.00 | 0.982 | 0.02 | 7.00 | 0.012 | 0.01 | 0.06 | 0.810 | 0.13 | 0.32 | 0.573 | 0.14 | 0.07 | 0.795 | −0.16 | 1.17 | 0.287 | −0.25 | 1.35 | 0.253 | −0.10 | 0.41 | 0.524 |
| gamma 32–48 Hz | −1.01 ± 0.69 | −1.02 ± 0.86 | 0.03 | 0.865 | 0.02 | 2.58 | 0.118 | −0.11 | 0.14 | 0.710 | 0.21 | 0.54 | 0.468 | 0.30 | 0.44 | 0.512 | −0.15 | 0.74 | 0.396 | −0.36 | 2.04 | 0.162 | −0.14 | 0.68 | 0.416 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benz, F.; Riemann, D.; Feige, B. Dreaming and Insomnia: Link between Physiological REM Parameters and Mentation Characteristics. Brain Sci. 2020, 10, 378. https://doi.org/10.3390/brainsci10060378
Benz F, Riemann D, Feige B. Dreaming and Insomnia: Link between Physiological REM Parameters and Mentation Characteristics. Brain Sciences. 2020; 10(6):378. https://doi.org/10.3390/brainsci10060378
Chicago/Turabian StyleBenz, Fee, Dieter Riemann, and Bernd Feige. 2020. "Dreaming and Insomnia: Link between Physiological REM Parameters and Mentation Characteristics" Brain Sciences 10, no. 6: 378. https://doi.org/10.3390/brainsci10060378
APA StyleBenz, F., Riemann, D., & Feige, B. (2020). Dreaming and Insomnia: Link between Physiological REM Parameters and Mentation Characteristics. Brain Sciences, 10(6), 378. https://doi.org/10.3390/brainsci10060378