Amplified Concern for Social Risk in Adolescence: Development and Validation of a New Measure


Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Questionnaire Development: The Health and Social Risk Questionnaire (HSRQ)
2.3. Measures Used for Construct Validation
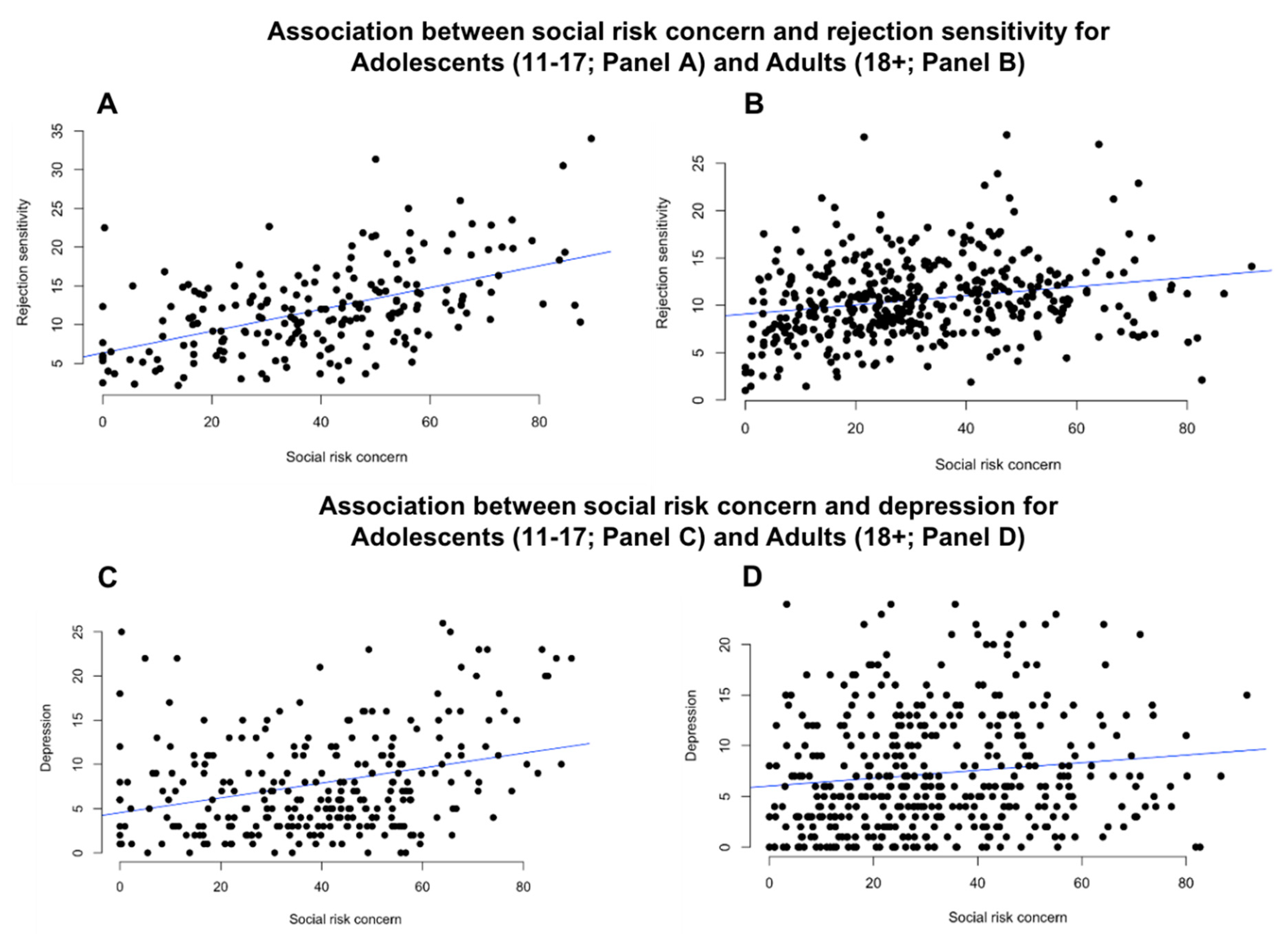
2.4. Rejection Sensitivity
2.5. Depression
2.6. Social Risk Taking
2.7. Analyses
2.7.1. Exploratory and Confirmatory Factor Analysis
2.7.2. Validation and Test–Retest Reliability
2.7.3. Age Differences in Concern for Health and Social Risk
3. Results
3.1. Sample 1: Exploratory Factor Analysis (EFA)
3.2. Sample 2: Confirmatory factor analysis (CFA; Adult Sample)
3.2.1. Test–Retest Reliability
3.2.2. Validation
3.3. Sample 3: Confirmatory Factor Analysis (CFA; Adolescent Sample)
3.4. Age Differences in Strength of Correlations
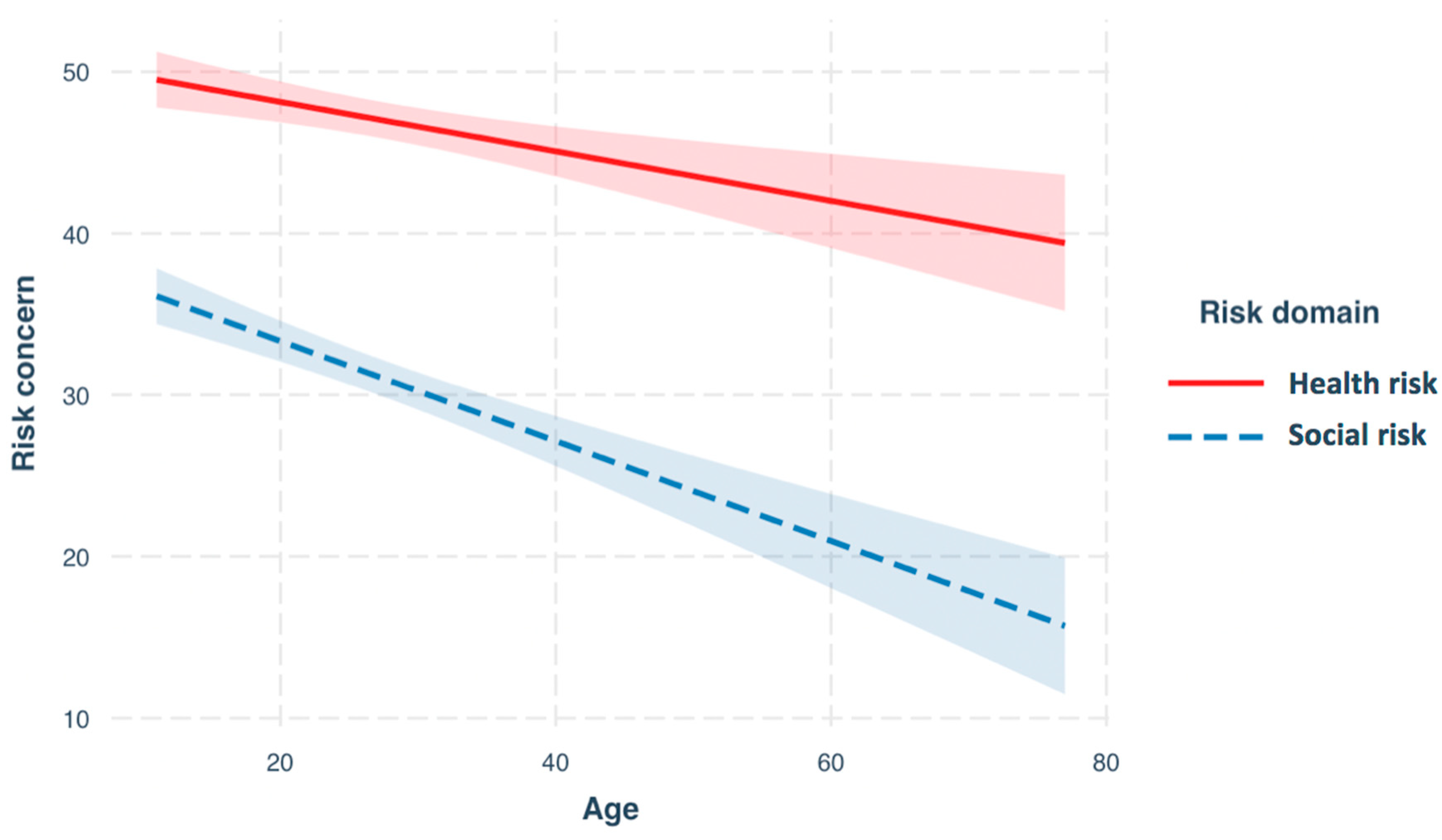
3.5. Age Differences in Concern for Health and Social Risk
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blakemore, S.-J.; Mills, K.L. Is Adolescence a Sensitive Period for Sociocultural Processing? Annu. Rev. Psychol. 2014, 65, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Durant, R.; Smith, J.A.; Kreiter, S.R.; Krowchuk, D.P. The relationship between early age of onset of initial substance use and engaging in multiple health risk behaviors among young adolescents. Arch. Pediatr. Adolesc. Med. 1999, 153, 286–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Nieuwenhuijzen, M.; Junger, M.; Velderman, M.K.; Wiefferink, K.H.; Paulussen, T.W.; Hox, J.; Reijneveld, S.A. Clustering of health-compromising behavior and delinquency in adolescents and adults in the Dutch population. Prev. Med. 2009, 48, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-H.; Baker, S.P.; Braver, E.R.; Li, G. Carrying passengers as a risk factor for crashes fatal to 16- and 17-year-old drivers. JAMA 2000, 283, 1578–1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, M.; Steinberg, L. Peer Influence on Risk Taking, Risk Preference, and Risky Decision Making in Adolescence and Adulthood: An Experimental Study. Dev. Psychol. 2005, 41, 625–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reniers, R.L.E.P.; Beavan, A.; Keogan, L.; Furneaux, A.; Mayhew, S.; Wood, S.J. Is it all in the reward? Peers influence risk-taking behaviour in young adulthood. Br. J. Psychol. 2016, 108, 276–295. [Google Scholar] [CrossRef]
- Van Duijvenvoorde, A.C.; Huizenga, H.M.; Somerville, L.H.; Delgado, M.R.; Powers, A.; Weeda, W.D.; Casey, B.J.; Weber, E.U.; Figner, B. Neural Correlates of Expected Risks and Returns in Risky Choice across Development. J. Neurosci. 2015, 35, 1549–1560. [Google Scholar] [CrossRef]
- Knoll, L.J.; Leung, J.T.; Foulkes, L.; Blakemore, S.-J. Age-related differences in social influence on risk perception depend on the direction of influence. J. Adolesc. 2017, 60, 53–63. [Google Scholar] [CrossRef]
- Knoll, L.J.; Magis-Weinberg, L.; Speekenbrink, M.; Blakemore, S.-J. Social Influence on Risk Perception During Adolescence. Psychol. Sci. 2015, 26, 583–592. [Google Scholar] [CrossRef] [Green Version]
- Sebastian, C.L.; Viding, E.; Williams, K.D.; Blakemore, S.-J. Social brain development and the affective consequences of ostracism in adolescence. Brain Cogn. 2010, 72, 134–145. [Google Scholar] [CrossRef]
- Somerville, L.H. The Teenage Brain: Sensitivity to Social Evaluation. Curr. Dir. Psychol. Sci. 2013, 22, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Peake, S.J.; Dishion, T.J.; Stormshak, E.A.; Moore, W.; Pfeifer, J.H. Risk-taking and social exclusion in adolescence: Neural mechanisms underlying peer influences on decision-making. NeuroImage 2013, 82, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blakemore, S.-J. Avoiding Social Risk in Adolescence. Curr. Dir. Psychol. Sci. 2018, 27, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Almquist, Y.B. Peer status in school and adult disease risk: A 30-year follow-up study of disease-specific morbidity in a Stockholm cohort. J. Epidemiol. Commun. Heal. 2009, 63, 1028–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Harmelen, A.-L.; Kievit, R.A.; Ioannidis, K.; Neufeld, S.; Jones, P.B.; Bullmore, E.; Dolan, R.; Fonagy, P.; Goodyer, I. The NSPN Consortium Adolescent friendships predict later resilient functioning across psychosocial domains in a healthy community cohort. Psychol. Med. 2017, 47, 2312–2322. [Google Scholar] [CrossRef] [PubMed]
- Noel, J.G.; Wann, D.L.; Branscombe, N.R. Peripheral ingroup membership status and public negativity toward outgroups. J. Pers. Soc. Psychol. 1995, 68, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Steinel, W.; A Van Kleef, G.; Van Knippenberg, D.; Hogg, M.A.; Homan, A.C.; Moffitt, G. How intragroup dynamics affect behavior in intergroup conflict: The role of group norms, prototypicality, and need to belong. Group Process. Intergroup Relat. 2010, 13, 779–794. [Google Scholar] [CrossRef]
- Platt, B.; Kadosh, K.C.; Lau, J.Y. The role of peer rejection in adolescent depression. Depress. Anxiety 2013, 30, 809–821. [Google Scholar] [CrossRef]
- Brown, B.B.; Larson, J. Peer Relationships in Adolescence. In Handbook of Adolescent Psychology; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Allen, N.B.; Badcock, P.B.T. The Social Risk Hypothesis of Depressed Mood: Evolutionary, Psychosocial, and Neurobiological Perspectives. Psychol. Bull. 2003, 129, 887–913. [Google Scholar] [CrossRef]
- Allen, N.B.; Badcock, P.B.T. Darwinian models of depression: A review of evolutionary accounts of mood and mood disorders. Prog. Neuro-Psychopharmacol. Boil. Psychiatry 2006, 30, 815–826. [Google Scholar] [CrossRef]
- Blais, A.-R.; Weber, E.U. A Domain-Specific Risk-Taking (DOSPERT)Scale for Adult Populations. Judgm. Decis. Mak. 2006, 1, 33–47. [Google Scholar]
- Berenson, K.R.; Gyurak, A.; Ayduk, Ö.; Downey, G.; Garner, M.J.; Mogg, K.; Bradley, B.; Pine, D.S. Rejection sensitivity and disruption of attention by social threat cues. J. Res. Pers. 2009, 43, 1064–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downey, G.; Lebolt, A.; Rincón, C.; Freitas, A.L. Rejection Sensitivity and Children’s Interpersonal Difficulties. Child Dev. 1998, 69, 1074–1091. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Messer, S.C.; Angold, A.; Costello, E.J.; Loeber, R.; van Kammen, W.; Stouthamer-Loeber, M. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents: Factor composition and structure across development. Int. J. Methods Psychiatr. Res. 1995, 5, 251–262. [Google Scholar]
- Daviss, W.B.; Birmaher, B.; Melhem, N.A.; Axelson, D.A.; Michaels, S.M.; Brent, D.A. Criterion validity of the Mood and Feelings Questionnaire for depressive episodes in clinic and non-clinic subjects. J. Child Psychol. Psychiatry 2006, 47, 927–934. [Google Scholar] [CrossRef]
- Munro, B.H. Statistical Methods for Health Care Research; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Bentler, P.M.; Chou, C.-P. Practical Issues in Structural Modeling. Sociol. Methods Res. 1987, 16, 78–117. [Google Scholar] [CrossRef]
- O’Brien, S.F.; Bierman, K.L. Conceptions and Perceived Influence of Peer Groups: Interviews with Preadolescents and Adolescents. Child Dev. 1988, 59, 1360–1365. [Google Scholar] [CrossRef]
- Wang, R.A.H.; Davis, O.S.; Wootton, R.E.; Mottershaw, A.; Haworth, C.M. Social support and mental health in late adolescence are correlated for genetic, as well as environmental, reasons. Sci. Rep. 2017, 7, 13088. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; De Graaf, R.; Demyttenaere, K.; Gasquet, I.; De Girolamo, G.; Gluzman, S.; Gureje, O.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 6, 168–176. [Google Scholar] [PubMed]
- Andrews, J.L.; Foulkes, L.; Blakemore, S.-J. Peer Influence in Adolescence: Public-Health Implications for COVID-19. Trends Cogn. Sci. 2020. [Google Scholar] [CrossRef]
- Paluck, E.L.; Shepherd, H.; Aronow, P.M. Changing climates of conflict: A social network experiment in 56 schools. Proc. Natl. Acad. Sci. USA 2016, 113, 566–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, R.; Starkey, F.; Holliday, J.; Audrey, S.; Bloor, M.; Parry-Langdon, N.; Hughes, R.A.; Moore, L. An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): A cluster randomised trial. Lancet 2008, 371, 1595–1602. [Google Scholar] [CrossRef] [Green Version]
- Bonell, C.; Blakemore, S.-J.; Fletcher, A.; Patton, G. Role theory of schools and adolescent health. Lancet Child Adolesc. Heal. 2019, 3, 742–748. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Risk Item | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| 1. Defend an unpopular opinion that you believe in. | 0.86 | |||
| 2. Admit that you listen to a singer or band that none of your friends like. | 0.65 | |||
| 3. Argue with a popular friend in front of a group of people. | 0.83 | |||
| 4. Wear clothes that are really different to your friends’ clothes. | 0.5 | |||
| 7. Stand up for someone who is being mocked by your friends. | 0.76 | |||
| 8. Spend time with someone your friends don’t like. | 0.56 | |||
| 9. Eat food that has passed its sell-by date. | 0.57 | |||
| 10. Ride a bicycle without wearing a helmet. | 0.48 | |||
| 13. Cross a main road when the crossing light is red. | 0.64 | |||
| 15. Pick up broken glass with bare hands. | 0.78 | |||
| 16. Drink tap water in a foreign country. | 0.56 | |||
| 5. Miss a popular friend’s party that lots of people are attending. | 0.93 | |||
| 6. Choose to stay at home when your friends are going out. | 0.8 | |||
| 11. Spend an afternoon in the sun without wearing sun cream. | 0.35 | |||
| 12. Eat unhealthy (high fat/sugar content) foods. | 0.66 | |||
| 14. Avoid doing regular exercise. | 0.78 |
| Risk Item | Adult (CFA) | Adolescent (CFA) | ||
|---|---|---|---|---|
| Social | Health | Social | Health | |
| 1. Defend an unpopular opinion that you believe in. | 0.6 | 0.77 | ||
| 2. Admit that you listen to a singer or band that none of your friends like. | 0.7 | 0.67 | ||
| 3. Argue with a popular friend in front of a group of people. | 0.44 | 0.79 | ||
| 4. Wear clothes that are really different to your friends’ clothes. | 0.63 | 0.59 | ||
| 7. Stand up for someone who is being mocked by your friends. | 0.76 | 0.69 | ||
| 8. Spend time with someone your friends don’t like. | 0.64 | 0.58 | ||
| 9. Eat food that has passed its sell-by date. | 0.42 | 0.54 | ||
| 10. Ride a bicycle without wearing a helmet. | 0.6 | 0.7 | ||
| 13. Cross a main road when the crossing light is red. | 0.62 | 0.77 | ||
| 15. Pick up broken glass with bare hands. | 0.53 | 0.73 | ||
| 16. Drink tap water in a foreign country. | 0.28 | 0.54 | ||
| Social | Health | |||
|---|---|---|---|---|
| Cronbach’s Alpha | McDonalds ω | Cronbach’s Alpha | McDonalds ω | |
| CFA (Adults) | 0.79 | 0.8 | 0.62 | 0.63 |
| CFA (Adolescents) | 0.84 | 0.84 | 0.79 | 0.79 |
| Predictor | β | SE | t | p |
|---|---|---|---|---|
| Intercept | 49.43 | 1.85 | 26.69 | <0.001 |
| Age | −0.15 | 0.04 | −3.68 | <0.001 |
| Risk domain (social risk) | −11.69 | 1.78 | −6.55 | <0.001 |
| Gender | 1.07 | 0.82 | 1.31 | 0.19 |
| Age * risk domain (social risk) | −0.016 | 0.06 | −2.7 | 0.008 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrews, J.L.; Foulkes, L.E.; Bone, J.K.; Blakemore, S.-J. Amplified Concern for Social Risk in Adolescence: Development and Validation of a New Measure. Brain Sci. 2020, 10, 397. https://doi.org/10.3390/brainsci10060397
Andrews JL, Foulkes LE, Bone JK, Blakemore S-J. Amplified Concern for Social Risk in Adolescence: Development and Validation of a New Measure. Brain Sciences. 2020; 10(6):397. https://doi.org/10.3390/brainsci10060397
Chicago/Turabian StyleAndrews, Jack L., Lucy E. Foulkes, Jessica K. Bone, and Sarah-Jayne Blakemore. 2020. "Amplified Concern for Social Risk in Adolescence: Development and Validation of a New Measure" Brain Sciences 10, no. 6: 397. https://doi.org/10.3390/brainsci10060397
APA StyleAndrews, J. L., Foulkes, L. E., Bone, J. K., & Blakemore, S. -J. (2020). Amplified Concern for Social Risk in Adolescence: Development and Validation of a New Measure. Brain Sciences, 10(6), 397. https://doi.org/10.3390/brainsci10060397