Cannabinoids for People with ASD: A Systematic Review of Published and Ongoing Studies

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
3. Results
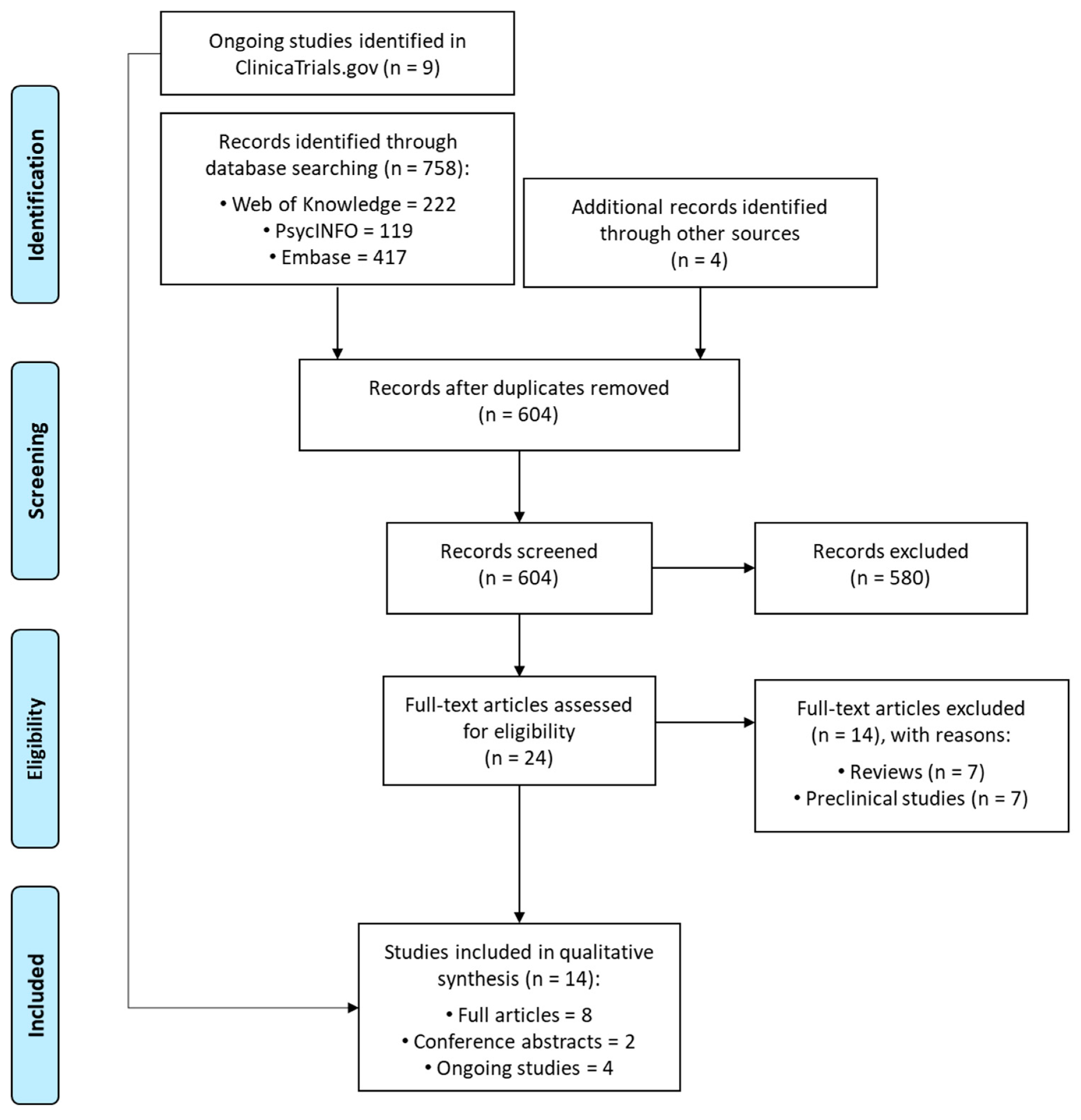
3.1. Search Results
3.2. Characteristics of Studies and Participants
3.3. Characteristics of Treatment
3.4. Outcomes and Findings
3.5. Ongoing Trials
4. Discussion
4.1. Efficacy and Safety of Cannabinoids in ASD
4.2. Mechanisms of Action: The Role of Excitatory/Inhibitory System
4.3. Limitation: Heterogeneity of Studies
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Baxter, A.J.; Brugha, T.; Erskine, H.E.; Scheurer, R.W.; Vos, T.; Scott, J.G. The epidemiology and global burden of autism spectrum disorders. Psychol. Med. 2015, 45, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.P.; Zuckerman, K.E.; Hagen, A.D.; Kriz, D.J.; Duvall, S.W.; Van Santen, J.; Nigg, J.; Fair, D.; Fombonne, E. Aggressive behavior problems in children with autism spectrum disorders: Prevalence and correlates in a large clinical sample. Res. Autism Spectr. Disord. 2014, 8, 1121–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steenfeldt-Kristensen, C.; Jones, C.A.; Richards, C. The prevalence of self-injurious behaviour in autism: A meta-analytic study. J. Autism Dev. Disord. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maenner, M.J.; Shaw, K.A.; Baio, J. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, united states, 2016. MMWR Surveill Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and depression in adults with autism spectrum disorder: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef] [PubMed]
- Lugo-Marín, J.; Magán-Maganto, M.; Rivero-Santana, A.; Cuellar-Pompa, L.; Alviani, M.; Jenaro-Rio, C.; Díez, E.; Canal-Bedia, R. Prevalence of psychiatric disorders in adults with autism spectrum disorder: A systematic review and meta-analysis. Res. Autism Spectr. Disord. 2019, 59, 22–33. [Google Scholar] [CrossRef]
- Lai, M.-C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Brondino, N.; Fusar-Poli, L.; Miceli, E.; Di Stefano, M.; Damiani, S.; Rocchetti, M.; Politi, P. Prevalence of medical comorbidities in adults with autism spectrum disorder. J. Gen. Intern. Med. 2019, 34, 1992–1994. [Google Scholar] [CrossRef]
- Doshi-Velez, F.; Ge, Y.; Kohane, I. Comorbidity clusters in autism spectrum disorders: An electronic health record time-series analysis. Pediatrics 2014, 133, e54–e63. [Google Scholar] [CrossRef] [Green Version]
- Muskens, J.B.; Velders, F.P.; Staal, W.G. Medical comorbidities in children and adolescents with autism spectrum disorders and attention deficit hyperactivity disorders: A systematic review. Eur. Child Adolesc. Psychiatry 2017, 26, 1093–1103. [Google Scholar] [CrossRef]
- Besag, F.M. Epilepsy in patients with autism: Links, risks and treatment challenges. Neuropsychiatr. Dis. Treat. 2018, 14, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, M.L.; Kesler, M.; Candy, S.A.; Rho, J.M.; Pittman, Q.J. Comorbid epilepsy in autism spectrum disorder: Implications of postnatal inflammation for brain excitability. Epilepsia 2018, 59, 1316–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukmanji, S.; Manji, S.A.; Kadhim, S.; Sauro, K.M.; Wirrell, E.C.; Kwon, C.-S.; Jetté, N. The co-occurrence of epilepsy and autism: A systematic review. Epilepsy Behav. 2019, 98, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Li, J.; Zhang, Y.; Jin, X.; Ma, J. Epilepsy and autism spectrum disorder: An epidemiological study in shanghai, china. Front. Psychiatry 2019, 10, 658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frye, R.E. Prevalence, significance and clinical characteristics of seizures, epilepsy and subclinical electrical activity in autism. N. Am. J. Med. Sci. 2016, 8, 3. [Google Scholar]
- Brondino, N.; Fusar-Poli, L.; Panisi, C.; Damiani, S.; Barale, F.; Politi, P. Pharmacological modulation of GABA function in autism spectrum disorders: A systematic review of human studies. J. Autism Dev. Disord. 2016, 46, 825–839. [Google Scholar] [CrossRef]
- Grove, J.; Ripke, S.; Als, T.D.; Mattheisen, M.; Walters, R.K.; Won, H.; Pallesen, J.; Agerbo, E.; Andreassen, O.A.; Anney, R. Identification of common genetic risk variants for autism spectrum disorder. Nat. Genet. 2019, 51, 431–444. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Geng, H.; Liu, W.; Zhang, G. Prenatal, perinatal, and postnatal factors associated with autism: A meta-analysis. Medicine 2017, 96, e6696. [Google Scholar] [CrossRef]
- Getahun, D.; Fassett, M.J.; Peltier, M.R.; Wing, D.A.; Xiang, A.H.; Chiu, V.; Jacobsen, S.J. Association of perinatal risk factors with autism spectrum disorder. Am. J. Perinatol. 2017, 7, 295–304. [Google Scholar]
- Emberti Gialloreti, L.; Mazzone, L.; Benvenuto, A.; Fasano, A.; Garcia Alcon, A.; Kraneveld, A.; Moavero, R.; Raz, R.; Riccio, M.P.; Siracusano, M. Risk and protective environmental factors associated with autism spectrum disorder: Evidence-based principles and recommendations. J. Clin. Med. 2019, 8, 217. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Son, M.J.; Son, C.Y.; Radua, J.; Eisenhut, M.; Gressier, F.; Koyanagi, A.; Carvalho, A.F.; Stubbs, B.; Solmi, M. Environmental risk factors and biomarkers for autism spectrum disorder: An umbrella review of the evidence. Lancet Psychiatry 2019, 6, 590–600. [Google Scholar] [CrossRef] [Green Version]
- Marotta, R.; Risoleo, M.C.; Messina, G.; Parisi, L.; Carotenuto, M.; Vetri, L.; Roccella, M. The neurochemistry of autism. Brain Sci. 2020, 10, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, C.L.; Anacker, A.M.; Veenstra-VanderWeele, J. The serotonin system in autism spectrum disorder: From biomarker to animal models. Neuroscience 2016, 321, 24–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.; Lee, J.; Kim, E. Excitation/inhibition imbalance in animal models of autism spectrum disorders. Biol. Psychiatry 2017, 81, 838–847. [Google Scholar] [CrossRef] [Green Version]
- Chakrabarti, B.; Persico, A.; Battista, N.; Maccarrone, M. Endocannabinoid signaling in autism. Neurotherapeutics 2015, 12, 837–847. [Google Scholar] [CrossRef] [Green Version]
- Zamberletti, E.; Gabaglio, M.; Parolaro, D. The endocannabinoid system and autism spectrum disorders: Insights from animal models. Int. J. Mol. Sci. 2017, 18, 1916. [Google Scholar] [CrossRef]
- Schultz, S.; Siniscalco, D. Endocannabinoid system involvement in autism spectrum disorder: An overview with potential therapeutic applications. Aims Mol. Sci. 2019, 6, 27–37. [Google Scholar] [CrossRef]
- Kerr, D.; Downey, L.; Conboy, M.; Finn, D.; Roche, M. Alterations in the endocannabinoid system in the rat valproic acid model of autism. Behav. Brain Res. 2013, 249, 124–132. [Google Scholar] [CrossRef]
- Karhson, D.S.; Krasinska, K.M.; Dallaire, J.A.; Libove, R.A.; Phillips, J.M.; Chien, A.S.; Garner, J.P.; Hardan, A.Y.; Parker, K.J. Plasma anandamide concentrations are lower in children with autism spectrum disorder. Mol. Autism 2018, 9, 1–6. [Google Scholar] [CrossRef]
- Aran, A.; Eylon, M.; Harel, M.; Polianski, L.; Nemirovski, A.; Tepper, S.; Schnapp, A.; Cassuto, H.; Wattad, N.; Tam, J. Lower circulating endocannabinoid levels in children with autism spectrum disorder. Mol. Autism 2019, 10, 1–11. [Google Scholar] [CrossRef]
- Marco, E.M.; MacRì, S.; Laviola, G. Critical age windows for neurodevelopmental psychiatric disorders: Evidence from animal models. Neurotox. Res. 2011, 19, 286–307. [Google Scholar] [CrossRef] [PubMed]
- Cheng, D.; Low, J.K.; Logge, W.; Garner, B.; Karl, T. Chronic cannabidiol treatment improves social and object recognition in double transgenic app swe/ps1∆ e9 mice. Psychopharmacology 2014, 231, 3009–3017. [Google Scholar] [CrossRef] [PubMed]
- Osborne, A.L.; Solowij, N.; Babic, I.; Huang, X.-F.; Weston-Green, K. Improved social interaction, recognition and working memory with cannabidiol treatment in a prenatal infection (Poly I: C) rat model. Neuropsychopharmacology 2017, 42, 1447–1457. [Google Scholar] [CrossRef] [PubMed]
- Servadio, M.; Melancia, F.; Manduca, A.; Di Masi, A.; Schiavi, S.; Cartocci, V.; Pallottini, V.; Campolongo, P.; Ascenzi, P.; Trezza, V. Targeting anandamide metabolism rescues core and associated autistic-like symptoms in rats prenatally exposed to valproic acid. Transl. Psychiatry 2016, 6, e902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.W.; Borgelt, L.M.; Blackmer, A.B. Cannabidiol: A new hope for patients with Dravet or Lennox-Gastaut syndromes. Ann. Pharmacother. 2019, 53, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Austin, J.K.; Dunn, D.W. Progressive behavioral changes in children with epilepsy. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2002; Volume 135, pp. 419–427. [Google Scholar]
- Frye, R.E.; Casanova, M.F.; Fatemi, S.H.; Folsom, T.D.; Reutiman, T.J.; Brown, G.L.; Edelson, S.M.; Slattery, J.C.; Adams, J.B. Neuropathological mechanisms of seizures in autism spectrum disorder. Front. Neurosci. 2016, 10, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cifelli, P.; Ruffolo, G.; De Felice, E.; Alfano, V.; van Vliet, E.A.; Aronica, E.; Palma, E. Phytocannabinoids in neurological diseases: Could they restore a physiological GABAergic transmission? Int. J. Mol. Sci. 2020, 21, 723. [Google Scholar] [CrossRef] [Green Version]
- Silvestro, S.; Mammana, S.; Cavalli, E.; Bramanti, P.; Mazzon, E. Use of cannabidiol in the treatment of epilepsy: Efficacy and security in clinical trials. Molecules 2019, 24, 1459. [Google Scholar] [CrossRef] [Green Version]
- Linge, R.; Jiménez-Sánchez, L.; Campa, L.; Pilar-Cuéllar, F.; Vidal, R.; Pazos, A.; Adell, A.; Díaz, Á. Cannabidiol induces rapid-acting antidepressant-like effects and enhances cortical 5-HT/glutamate neurotransmission: Role of 5-HT1a receptors. Neuropharmacology 2016, 103, 16–26. [Google Scholar] [CrossRef] [Green Version]
- Russo, E.B.; Burnett, A.; Hall, B.; Parker, K.K. Agonistic properties of cannabidiol at 5-HT1a receptors. Neurochem. Res. 2005, 30, 1037–1043. [Google Scholar] [CrossRef]
- Skelley, J.W.; Deas, C.M.; Curren, Z.; Ennis, J. Use of cannabidiol in anxiety and anxiety-related disorders. J. Am. Pharm. Assoc. 2020, 60, 253–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, C.; Bhattacharyya, S. Cannabidiol as a potential treatment for psychosis. Ther. Adv. Psychopharmacol. 2019, 9, 2045125319881916. [Google Scholar] [CrossRef] [PubMed]
- Zamberletti, E.; Gabaglio, M.; Piscitelli, F.; Brodie, J.S.; Woolley-Roberts, M.; Barbiero, I.; Tramarin, M.; Binelli, G.; Landsberger, N.; Kilstrup-Nielsen, C. Cannabidivarin completely rescues cognitive deficits and delays neurological and motor defects in male MECP2 mutant mice. J. Psychopharmacol. 2019, 33, 894–907. [Google Scholar] [CrossRef]
- Hill, A.; Mercier, M.; Hill, T.; Glyn, S.; Jones, N.; Yamasaki, Y.; Futamura, T.; Duncan, M.; Stott, C.; Stephens, G. Cannabidivarin is anticonvulsant in mouse and rat. Br. J. Pharmacol. 2012, 167, 1629–1642. [Google Scholar] [CrossRef] [PubMed]
- Chagas, M.H.N.; Crippa, J.A.S.; Zuardi, A.W.; Hallak, J.E.; Machado-de-Sousa, J.P.; Hirotsu, C.; Maia, L.; Tufik, S.; Andersen, M.L. Effects of acute systemic administration of cannabidiol on sleep-wake cycle in rats. J. Psychopharmacol. 2013, 27, 312–316. [Google Scholar] [CrossRef]
- Bruijnzeel, A.W.; Qi, X.; Guzhva, L.V.; Wall, S.; Deng, J.V.; Gold, M.S.; Febo, M.; Setlow, B. Behavioral characterization of the effects of cannabis smoke and anandamide in rats. PLoS ONE 2016, 11, e0153327. [Google Scholar] [CrossRef]
- Cooper, R.E.; Williams, E.; Seegobin, S.; Tye, C.; Kuntsi, J.; Asherson, P. Cannabinoids in attention-deficit/hyperactivity disorder: A randomised-controlled trial. Eur. Neuropsychopharmacol. 2017, 27, 795–808. [Google Scholar] [CrossRef]
- Howes, O.D.; Rogdaki, M.; Findon, J.L.; Wichers, R.H.; Charman, T.; King, B.H.; Loth, E.; McAlonan, G.M.; McCracken, J.T.; Parr, J.R. Autism spectrum disorder: Consensus guidelines on assessment, treatment and research from the british association for psychopharmacology. J. Psychopharmacol. 2018, 32, 3–29. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Brondino, N.; Rocchetti, M.; Petrosino, B.; Arillotta, D.; Damiani, S.; Provenzani, U.; Petrosino, C.; Aguglia, E.; Politi, P. Prevalence and predictors of psychotropic medication use in adolescents and adults with autism spectrum disorder in italy: A cross-sectional study. Psychiatry Res. 2019, 276, 203–209. [Google Scholar] [CrossRef]
- Agarwal, R.; Burke, S.L.; Maddux, M. Current state of evidence of cannabis utilization for treatment of autism spectrum disorders. BMC Psychiatry 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Poleg, S.; Golubchik, P.; Offen, D.; Weizman, A. Cannabidiol as a suggested candidate for treatment of autism spectrum disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 89, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurz, R.; Blaas, K. Use of dronabinol (delta-9-thc) in autism: A prospective single-case-study with an early infantile autistic child. Cannabinoids 2010, 5, 4–6. [Google Scholar]
- Schleider, B.-L.; Mechoulam, R.; Saban, N.; Meiri, G.; Novack, V. Real life experience of medical cannabis treatment in autism: Analysis of safety and efficacy. Sci. Rep. 2019, 9, 200. [Google Scholar] [CrossRef] [PubMed]
- Barchel, D.; Stolar, O.; De-Haan, T.; Ziv-Baran, T.; Saban, N.; Fuchs, D.O.; Koren, G.; Berkovitch, M. Oral cannabidiol use in children with autism spectrum disorder to treat related symptoms and co-morbidities. Front. Pharmacol. 2019, 9, 1521. [Google Scholar] [CrossRef]
- Kuester, G.; Vergara, K.; Ahumada, A.; Gazmuri, A.M. Oral cannabis extracts as a promising treatment for the core symptoms of autism spectrum disorder: Preliminary experience in chilean patients. J. Neurol. Sci. 2017, 381, 932–933. [Google Scholar] [CrossRef]
- Pretzsch, C.M.; Freyberg, J.; Voinescu, B.; Lythgoe, D.; Horder, J.; Mendez, M.A.; Wichers, R.; Ajram, L.; Ivin, G.; Heasman, M.; et al. Effects of cannabidiol on brain excitation and inhibition systems; a randomised placebo-controlled single dose trial during magnetic resonance spectroscopy in adults with and without autism spectrum disorder. Neuropsychopharmacology 2019, 44, 1398–1405. [Google Scholar] [CrossRef] [Green Version]
- Pretzsch, C.M.; Voinescu, B.; Lythgoe, D.; Horder, J.; Mendez, M.A.; Wichers, R.; Ajram, L.; Ivin, G.; Heasman, M.; Edden, R.A.E.; et al. Effects of cannabidivarin (CBDV) on brain excitation and inhibition systems in adults with and without autism spectrum disorder (ASD): A single dose trial during magnetic resonance spectroscopy. Transl. Psychiatry 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Pretzsch, C.M.; Voinescu, B.; Mendez, M.A.; Wichers, R.; Ajram, L.; Ivin, G.; Heasman, M.; Williams, S.; Murphy, D.G.M.; Daly, E.; et al. The effect of cannabidiol (CBD) on low-frequency activity and functional connectivity in the brain of adults with and without autism spectrum disorder (ASD). J. Psychopharmacol. 2019, 33, 1141–1148. [Google Scholar] [CrossRef]
- Aran, A.; Cassuto, H.; Lubotzky, A.; Wattad, N.; Hazan, E. Brief report: Cannabidiol-rich cannabis in children with autism spectrum disorder and severe behavioral problems-a retrospective feasibility study. J. Autism Dev. Disord. 2019, 49, 1284–1288. [Google Scholar] [CrossRef]
- Fleury-Teixeira, P.; Caixeta, F.V.; da Silva, L.C.R.; Brasil-Neto, J.P.; Malcher-Lopes, R. Effects of CBD-enriched cannabis sativa extract on autism spectrum disorder symptoms: An observational study of 18 participants undergoing compassionate use. Front. Neurol. 2019, 10, 1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McVige, J.; Headd, V.; Alwahaidy, M.; Lis, D.; Kaur, D.; Albert, B.; Mechtler, L. Medical Cannabis in the Treatment of Patients with Autism Spectrum Disorder (1648). Neurology 2020, 94, 1648. [Google Scholar]
- Lai, M.-C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Baribeau, D.A.; Anagnostou, E. An update on medication management of behavioral disorders in autism. Curr. Psychiatry Rep. 2014, 16, 437. [Google Scholar] [CrossRef]
- Hsia, Y.; Wong, A.Y.; Murphy, D.G.; Simonoff, E.; Buitelaar, J.K.; Wong, I.C. Psychopharmacological prescriptions for people with autism spectrum disorder (ASD): A multinational study. Psychopharmacology 2014, 231, 999–1009. [Google Scholar] [CrossRef]
- Simon, V.; Winkel, R.v.; Hert, M.d. Are weight gain and metabolic side effects of atypical antipsychotics dose dependent? A literature review. J. Clin. Psychiatry 2009, 70, 1041–1050. [Google Scholar] [CrossRef]
- Adams, J.B.; Audhya, T.; McDonough-Means, S.; Rubin, R.A.; Quig, D.; Geis, E.; Gehn, E.; Loresto, M.; Mitchell, J.; Atwood, S. Nutritional and metabolic status of children with autism vs. Neurotypical children, and the association with autism severity. Nutr. Metab. 2011, 8, 34. [Google Scholar] [CrossRef] [Green Version]
- Marí-Bauset, S.; Zazpe, I.; Mari-Sanchis, A.; Llopis-González, A.; Morales-Suárez-Varela, M. Food selectivity in autism spectrum disorders: A systematic review. J. Child Neurol. 2014, 29, 1554–1561. [Google Scholar] [CrossRef]
- Panerai, S.; Ferri, R.; Catania, V.; Zingale, M.; Ruccella, D.; Gelardi, D.; Fasciana, D.; Elia, M. Sensory profiles of children with autism spectrum disorder with and without feeding problems: A comparative study in sicilian subjects. Brain Sci. 2020, 10, 336. [Google Scholar] [CrossRef]
- Garcia, G. Antipsychotics medication use and its metabolic challenges for autism spectrum disorders. N. Am. J. Med. Sci. 2012, 5, 3. [Google Scholar] [CrossRef]
- Maayan, L.; Correll, C.U. Weight gain and metabolic risks associated with antipsychotic medications in children and adolescents. J. Child Adolesc. Psychopharmacol. 2011, 21, 517–535. [Google Scholar] [CrossRef]
- Yood, M.U.; DeLorenze, G.N.; Quesenberry, C.P.; Oliveria, S.A.; Tsai, A.-L.; Kim, E.; Cziraky, M.J.; McQuade, R.D.; Newcomer, J.W.; Gilbert, J.L. Association between second-generation antipsychotics and newly diagnosed treated diabetes mellitus: Does the effect differ by dose? BMC Psychiatry 2011, 11, 197. [Google Scholar]
- Zemrak, W.R.; Kenna, G.A. Association of antipsychotic and antidepressant drugs with QT interval prolongation. Am. J. Health-Syst. Pharm. 2008, 65, 1029–1038. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, J.; Merzenich, M.M. Model of autism: Increased ratio of excitation/inhibition in key neural systems. Genes Brain Behav. 2003, 2, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.B.; Valakh, V. Excitatory/inhibitory balance and circuit homeostasis in autism spectrum disorders. Neuron 2015, 87, 684–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, C.L.; Evans, V.F.; DeMarse, T.B.; Febo, M.; Johnson, C.R.; Carney, P.R. Cannabidiol for the treatment of drug-resistant epilepsy in children: Current state of research. J. Pediatr. Neurol. 2017, 15, 143–150. [Google Scholar]
- Gu, B. Cannabidiol provides viable treatment opportunity for multiple neurological pathologies of autism spectrum disorder. Glob. Drugs Ther. 2017, 2, 3–4. [Google Scholar] [CrossRef] [Green Version]
- Bozzi, Y.; Provenzano, G.; Casarosa, S. Neurobiological bases of autism–epilepsy comorbidity: A focus on excitation/inhibition imbalance. Eur. J. Neurosci. 2018, 47, 534–548. [Google Scholar] [CrossRef] [Green Version]
- Hartley-McAndrew, M.; Weinstock, A. Autism spectrum disorder: Correlation between aberrant behaviors, EEG abnormalities and seizures. Neurol. Int. 2010, 2, e10. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.N.; Sun, J.C.; Tse, M.T.; Gorzalka, B.B. Altered responsiveness of serotonin receptor subtypes following long-term cannabinoid treatment. Int. J. Neuropsychopharmacol. 2006, 9, 277–286. [Google Scholar] [CrossRef]
- Campos, A.C.; de Paula Soares, V.; Carvalho, M.C.; Ferreira, F.R.; Vicente, M.A.; Brandão, M.L.; Zuardi, A.W.; Zangrossi, H.; Guimarães, F.S. Involvement of serotonin-mediated neurotransmission in the dorsal periaqueductal gray matter on cannabidiol chronic effects in panic-like responses in rats. Psychopharmacology 2013, 226, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Renard, J.; Norris, C.; Rushlow, W.; Laviolette, S.R. Neuronal and molecular effects of cannabidiol on the mesolimbic dopamine system: Implications for novel schizophrenia treatments. Neurosci. Biobehav. Rev. 2017, 75, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Provenzani, U.; Fusar-Poli, L.; Brondino, N.; Damiani, S.; Vercesi, M.; Meyer, N.; Rocchetti, M.; Politi, P. What are we targeting when we treat autism spectrum disorder? A systematic review of 406 clinical trials. Autism 2020, 24, 274–284. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Characteristics | Characteristics of Participants with ASD | Treatment Characteristics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Authors | Year | Country | Study Design | N of Participants with ASD | Mean Age, Years (Range) | Intellectual Disability, n (%) | Concomitant Medication | Participants with Epilepsy, n (%) | Active Treatment | Daily Dosage | Control Treatment | Mean Follow-Up, Months (Range) |
| Aran et al. [62] | 2019 | Israel | Retrospective cohort study | 60 | 11.8 (5–17.5) | 77% low functioning | All medications (82%), Antipsychotics (72%), Mood stabilizers (17%), Benzodiazepines (12%), SSRI (7%), Stimulants (7%) | 14 (23.3) | Cannabinoid oil solution at a 20:1 ratio of CBD and THC, | Sublingual assumption 2 or 3 times/daily with CBD doses started at 1 mg/kg/day and titrated up to 10 mg/kg/day. | None | 10.9 (7–13) |
| Barchel et al. [57] | 2019 | Israel | Prospective cohort study | 53 | 11 (4–22) | Not reported | Atypical antipsychotics (58.4%), Anti-epileptic (15%), Typical antipsychotics (11.3%), Stimulants (9.4%), Melatonin (7.5%), Other anti-muscarinic (5.6%), Anti-depressant (3.7%), Alpha agonist (1.8%) | Not reported | Cannabinoid oil solution at a concentration of 30% and 20:1 ratio of CBD and THC. | CBD: 16 mg/kg (maximal daily dose 600 mg), THC: 0.8 mg/kg (maximal daily dose of 40 mg). | None | Median 66 days (30–588 days) |
| Fleury-Teixeira et al. [63] | 2019 | Brazil | Prospective cohort study | 18 (15 analyzed) | 10.9 (6–17) | Not reported | Any medication (66.7%), Antipsychotics (46.7%), Mood stabilizers (33%), Phenobarbital (6.7%) | 5 (27.7) | Cannabis Sativa extract containing a 75:1 CBD:THC ratio | CBD: mean 175 mg/day (100–350); THC: 2.33 mg/day (1.33–2.33). | None | 12.4 (6–39) |
| Kuester et al. [58] | 2017 | Chile | Retrospective case series (abstract only) | 20 | 9.8 (2–22) | Not reported | Not reported | Part of the sample had seizures | 71.5% of patients received balanced CBD:THC extracts; 19% high-CBD; and 9.5% high-THC extracts. | Not reported | None | 7.6 (3–12) |
| Kurz and Blaas [55] | 2010 | Austria | Case report | One | 6 | Not reported | None | Not reported | Dronabinol (delta-9-THC) solved in sesame oil. | Initial dosage was one drop (0.62 mg) in the morning which was increased up to 3.62 mg/die | None | 6 |
| McVige et al. [64] | 2020 | United States | Retrospective case series (abstract only) | 20 | Not reported | Not reported | Each patient tried an average of 6.4 other medications. Current medication not specified. | 6 (30%) | Medical cannabis | Not reported | None | Not reported |
| Schleider et al. [56] | 2019 | Israel | Prospective cohort study | 188 | 12.9 (<5–18) | Not reported | Antipsychotics (56.9%), antiepileptics (26.0%), hypnotics and sedatives (14.9%), antidepressants (10.6%). | 27 (14.4%) | Most patients consumed oil with 30% CBD and 1.5% THC. Insomnia was treated with an evening dose of 3% THC oil. | On average 79.5 ± 61.5 mg CBD and 4.0 ± 3.0 mg THC, three times a day. Average additional 5.0 ± 4.5 mg THC daily for insomnia. | None | 6 |
| Pretzsch et al. [59] | 2019a | United Kingdom | RCT crossover | 17 | 31.3 | 0 (0) | No medication influencing GABA+ levels. Methylphenidate (n = 1), sertraline (n = 1) | 0 (0) | CBD | 600 mg | Placebo | Single administration |
| Pretzsch et al. [60] | 2019b | United Kingdom | RCT crossover | 17 | 31.3 | 0 (0) | No medication influencing GABA+ levels. | 0 (0) | CBDV | 600 mg | Placebo | Single administration |
| Pretzsch et al. [61] | 2019c | United Kingdom | RCT crossover | 13 | 30.8 | 0 (0) | No medication influencing GABA+ levels. Methylphenidate (n = 1), sertraline (n = 1) | 0 (0) | CBD | 600 mg | Placebo | Single administration |
| Authors | Year | Outcome (Measures) | Results | Side Effects (%) | Drop Out/Treatment Discontinuation, n (%) |
|---|---|---|---|---|---|
| Aran et al. [62] | 2019 |
|
| Any adverse event (51%), Sleep disturbances (14%), Restlessness (9%), Nervousness (9%), Loss of appetite (9%), Gastrointestinal symptoms (7%), Unexplained laugh (7%), Mood changes (5%), Fatigue (5%), Nocturnal enuresis (3.5%), Gain of appetite (3.5%), Weight loss (3.5%), Weight gain (3.5%), Dry mouth (3.5%), Tremor (3.5%), Sleepiness (2%), Anxiety (2%), Confusion (2%), Cough (2%), Psychotic event (2%) | 1 (1.6%) |
| Barchel et al. [57] | 2019 |
|
| Somnolence (22.6%), Appetite decrease (11.3%), Appetite increase (7.5%), Insomnia (3.7%), Sense abnormality response (to temperature) (3.7%), Eyes blinking (3.7%), Diarrhea (3.7%), Hair loss (1.8%), Nausea (1.8%), Confusion (1.8%), Acne (1.8%), Palpitations (1.8%), Urinary (1.8%), Incontinence (1.8%), Eye redness (1.8%), Constipation (1.8%) | 5 (9.4%) |
| Fleury-Teixeira et al. [63] | 2019 |
|
| Sleepiness, moderate irritability (n = 3); diarrhea, increased appetite, conjunctival hyperemia, and increased body temperature (n = 1). All these side effects were mild and/or transient. Nocturia (n = 2), which in one case appeared concomitantly to an improvement in sleep quality. | 3 out of 18 (16.7%) |
| Kuester et al. [58] | 2017 |
| CGI-I And APSI: 66.7% of patients had significant improvement. Most cases improved at least one of ASD core symptoms. Sensory difficulties, food acceptance, feeding and sleep disorders, and/or seizures were improved in most cases. | Two patients had more agitation and one had more irritability, effects that were solved by changing the strain. | None |
| Kurz and Blaas [55] | 2010 |
| Significant improvement in all subscales | None reported. | None |
| McVige et al. [64] | 2020 |
|
| Three patients reported mild adverse events (unspecified). | None |
| Schleider et al. [56] | 2019 |
|
| Restlessness (6.6%), sleepiness (3.2%), psychoactive effect (3.2%), increased appetite (3.2%), digestion problems (3.2%), dry mouth (2.2%), lack of appetite (2.2%). | 23 (12.2%) |
| Pretzsch et al. [59] | 2019a | MRS, effects of Glx and GABA+ | CBD increased subcortical, but decreased cortical, Glx. CBD decreased GABA+ in ASD. | None reported | None |
| Pretzsch et al. [60] | 2019b | MRS, effects of Glx and GABA+ | CBDV significantly increased Glx in the basal ganglia. In the ASD group, the ‘shift’ in Glx correlated negatively with baseline Glx concentration, CBDV had no significant impact on Glx in the DMPFC, or on GABA+. | None reported | None |
| Pretzsch et al. [61] | 2019c | fMRI, measure of fractional amplitude of low-frequency fluctuations’ (fALFF) and, functional connectivity (FC) | CBD significantly increased fALFF in the cerebellar vermis and the right fusiform gyrus in the ASD group. CBD also significantly altered vermal FC with several of its subcortical (striatal) and cortical targets but did not affect fusiform FC with other regions. | None reported | None |
| Study Characteristics | Participants Characteristics | Treatment Characteristics | Outcomes | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Registration Number | Principal Investigator | Affiliation | Country | Study Design | N of Participants with ASD | Age Range | Active Treatment | Control Treatment | Duration | Outcome Measures |
| NCT03202303 | Eric Hollander | Montefiore Medical Center | United States | RCT | 100 | 5–18 | 10 mg/kg/day CBDV | 10 mg/kg/day placebo | 12 weeks | ABC-I; RBS-R; ABC-SW; PedsQL; Vineland 3; CGI-I |
| NCT03849456 | Gregory N Barnes | University of Louiseville | United States | Open label | 30 | 4–18 | CBDV at a dose of 2.5 mg/kg/day and titrate to a target dose of 10 mg/kg/day or 800 mg/day during the first 4 week. If intolerance during titration, participant may be maintained on a dose below 10 mg/kg/day. Maximum dose: 20 mg/kg/day or 1600 mg/day. | None | 52 weeks | TEAEs; CCC-2; Vineland 3; NIH; RBS-R; CSHQ; ABC, CGI-I |
| NCT03900923 | Francisco Castellanos, Orrin Devinsky | New York Langone Health | United States | Open label | 30 | 7–17 | Cohorts of size 3 receiving doses of 3, 6, or 9 mg/kg/day of CBD, depending on the treatment response of participants in prior cohorts. | None | 6 weeks | CGI-I; BOSCC; RBS-R; SRS-2; ABC-SW; ABC-I; CCC-2; SCARED; SDSC; Vineland 3; CGI-S; AFEQ; ASC-ASD-P; ASC-ASD-C; OSUS; OSUI; BIS |
| NCT02956226 | Adi Aran, Varda Gross | Shaare Zedek Medical Center | Israel | RCT | 150 | 5–21 | Oral cannabinoids mix (CBD:THC in a 20:1 ratio) at 1 mg/kg CBD per day, up titrated until intolerance or to a maximum dose of 10 mg/kg CBD per day, divided to 3 daily doses. | Oral olive oil and flavors that mimic in texture and flavor the cannabinoids’ solution. | 3 months | HSQ-ASD; CGI-I; SRS-2; APSI; LAEP |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusar-Poli, L.; Cavone, V.; Tinacci, S.; Concas, I.; Petralia, A.; Signorelli, M.S.; Díaz-Caneja, C.M.; Aguglia, E. Cannabinoids for People with ASD: A Systematic Review of Published and Ongoing Studies. Brain Sci. 2020, 10, 572. https://doi.org/10.3390/brainsci10090572
Fusar-Poli L, Cavone V, Tinacci S, Concas I, Petralia A, Signorelli MS, Díaz-Caneja CM, Aguglia E. Cannabinoids for People with ASD: A Systematic Review of Published and Ongoing Studies. Brain Sciences. 2020; 10(9):572. https://doi.org/10.3390/brainsci10090572
Chicago/Turabian StyleFusar-Poli, Laura, Vito Cavone, Silvia Tinacci, Ilaria Concas, Antonino Petralia, Maria Salvina Signorelli, Covadonga M. Díaz-Caneja, and Eugenio Aguglia. 2020. "Cannabinoids for People with ASD: A Systematic Review of Published and Ongoing Studies" Brain Sciences 10, no. 9: 572. https://doi.org/10.3390/brainsci10090572
APA StyleFusar-Poli, L., Cavone, V., Tinacci, S., Concas, I., Petralia, A., Signorelli, M. S., Díaz-Caneja, C. M., & Aguglia, E. (2020). Cannabinoids for People with ASD: A Systematic Review of Published and Ongoing Studies. Brain Sciences, 10(9), 572. https://doi.org/10.3390/brainsci10090572