Autonomic Changes in Juvenile-Onset Huntington’s Disease


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Statistical Analyses
3. Results
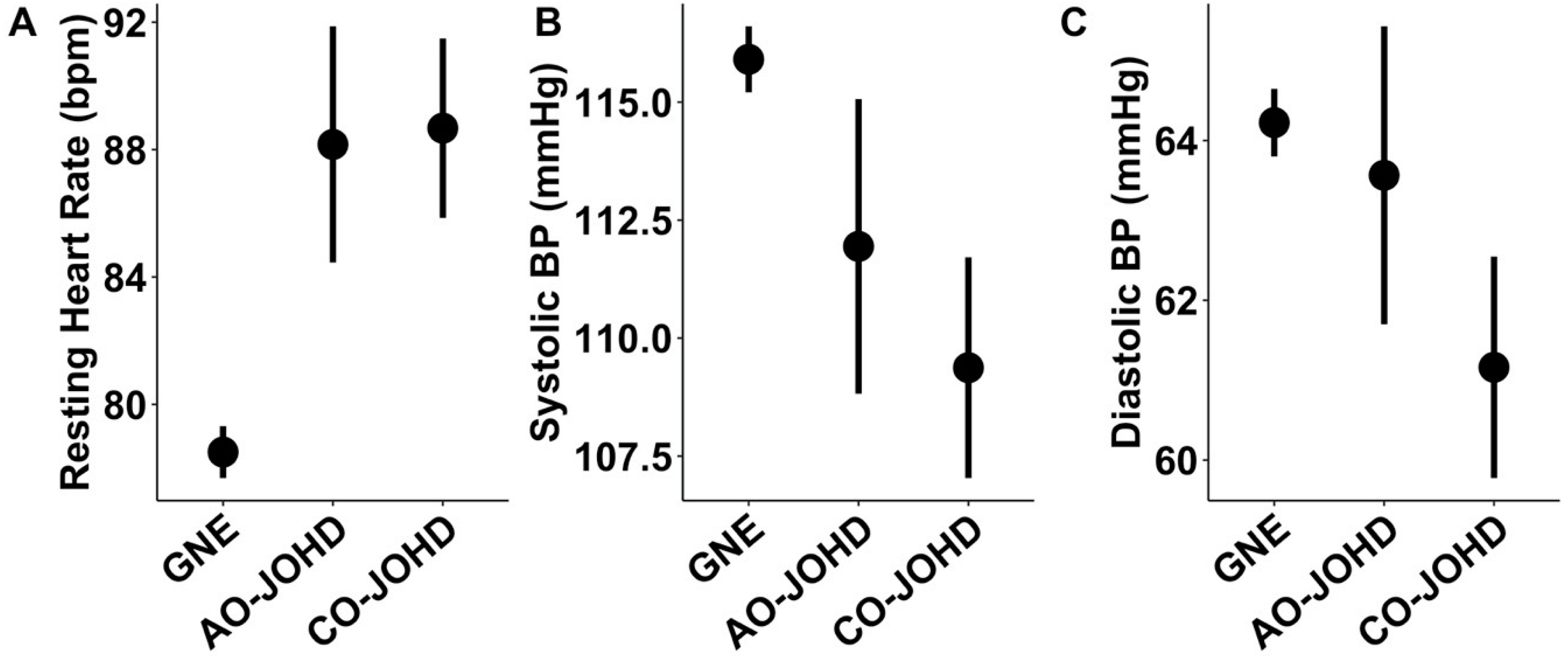
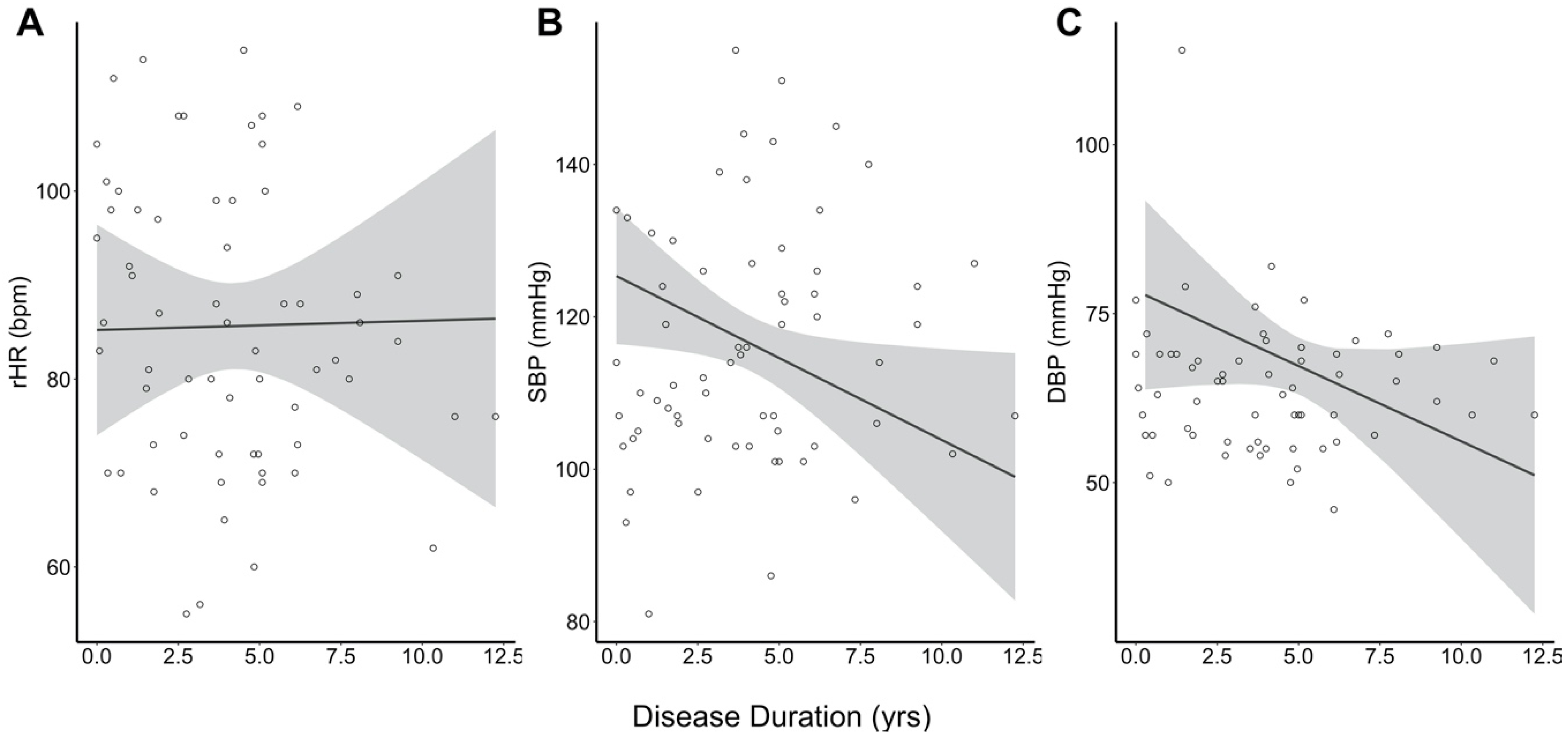
Primary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- MacDonald, M.E.; Ambrose, C.M.; Duyao, M.P.; Myers, R.H.; Lin, C.; Srinidhi, L.; Barnes, G.; Taylor, S.A.; James, M.; Groot, N.; et al. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. The Huntington’s Disease Collaborative Research Group. Cell 1993, 72, 971–983. [Google Scholar] [CrossRef]
- Tabrizi, S.J.; Scahill, R.I.; Owen, G.; Durr, A.; Leavitt, B.R.; Roos, R.A.; Borowsky, B.; Landwehrmeyer, B.; Frost, C.; Johnson, H.; et al. Predictors of phenotypic progression and disease onset in premanifest and early-stage Huntington’s disease in the TRACK-HD study: Analysis of 36-month observational data. Lancet Neurol. 2013, 12, 637–649. [Google Scholar] [CrossRef]
- Paulsen, J.S.; Long, J.D.; Ross, C.A.; Harrington, D.L.; Erwin, C.J.; Williams, J.K.; Westervelt, H.J.; Johnson, H.J.; Aylward, E.H.; Zhang, Y.; et al. Prediction of manifest Huntington’s disease with clinical and imaging measures: A prospective observational study. Lancet Neurol. 2014, 13, 1193–1201. [Google Scholar] [CrossRef] [Green Version]
- Andrich, J.; Schmitz, T.; Saft, C.; Postert, T.; Kraus, P.; Epplen, J.T.; Przuntek, H.; Agelink, M.W. Autonomic nervous system function in Huntington’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 72, 726–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Den Heijer, J.C.; Bollen, W.L.; Reulen, J.P.; van Dijk, J.G.; Kramer, C.G.; Roos, R.A.; Buruma, O.J. Autonomic nervous function in Huntington’s disease. Arch. Neurol. 1988, 45, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Kobal, J.; Meglic, B.; Mesec, A.; Peterlin, B. Early sympathetic hyperactivity in Huntington’s disease. Eur. J. Neurol. 2004, 11, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Kobal, J.; Melik, Z.; Cankar, K.; Bajrovic, F.F.; Meglic, B.; Peterlin, B.; Zaletel, M. Autonomic dysfunction in presymptomatic and early symptomatic Huntington’s disease. Acta Neurol. Scand. 2010, 121, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Kobal, J.; Melik, Z.; Cankar, K.; Strucl, M. Cognitive and autonomic dysfunction in presymptomatic and early Huntington’s disease. J. Neurol. 2014, 261, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Mielcarek, M.; Inuabasi, L.; Bondulich, M.K.; Muller, T.; Osborne, G.F.; Franklin, S.A.; Smith, D.L.; Neueder, A.; Rosinski, J.; Rattray, I.; et al. Dysfunction of the CNS-heart axis in mouse models of Huntington’s disease. PLoS Genet. 2014, 10, e1004550. [Google Scholar] [CrossRef]
- Critchley, B.J.; Isalan, M.; Mielcarek, M. Neuro-Cardio Mechanisms in Huntington’s Disease and Other Neurodegenerative Disorders. Front. Physiol. 2018, 9, 559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moser, A.D.; Epping, E.; Espe-Pfeifer, P.; Martin, E.; Zhorne, L.; Mathews, K.; Nance, M.; Hudgell, D.; Quarrell, O.; Nopoulos, P. A survey-based study identifies common but unrecognized symptoms in a large series of juvenile Huntington’s disease. Neurodegener Dis. Manag. 2017, 7, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tereshchenko, A.; McHugh, M.; Lee, J.K.; Gonzalez-Alegre, P.; Crane, K.; Dawson, J.; Nopoulos, P. Abnormal Weight and Body Mass Index in Children with Juvenile Huntington’s Disease. J. Huntingt. Dis. 2015, 4, 231–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tereshchenko, A.; Magnotta, V.; Epping, E.; Mathews, K.; Espe-Pfeifer, P.; Martin, E.; Dawson, J.; Duan, W.; Nopoulos, P. Brain structure in juvenile-onset Huntington disease. Neurology 2019, 92, e1939–e1947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Plas, E.; Langbehn, D.R.; Conrad, A.L.; Koscik, T.R.; Tereshchenko, A.; Epping, E.A.; Magnotta, V.A.; Nopoulos, P.C. Abnormal brain development in child and adolescent carriers of mutant huntingtin. Neurology 2019, 93, e1021–e1030. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.B.; Bates, G.P.; Steffan, J.; Saft, C.; Tabrizi, S.J. Treating the whole body in Huntington’s disease. Lancet Neurol. 2015, 14, 1135–1142. [Google Scholar] [CrossRef]
- Colombari, E.; Sato, M.A.; Cravo, S.L.; Bergamaschi, C.T.; Campos, R.R., Jr.; Lopes, O.U. Role of the medulla oblongata in hypertension. Hypertension 2001, 38, 549–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rub, U.; Hentschel, M.; Stratmann, K.; Brunt, E.; Heinsen, H.; Seidel, K.; Bouzrou, M.; Auburger, G.; Paulson, H.; Vonsattel, J.P.; et al. Huntington’s disease (HD): Degeneration of select nuclei, widespread occurrence of neuronal nuclear and axonal inclusions in the brainstem. Brain Pathol. 2014, 24, 247–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| JOHD Group | Controls | p-Value | |
|---|---|---|---|
| N (Visits) | 27 (64) | 259 (395) | NA |
| Female, % (n) | 55.6 (15) | 53.5 (138) | 0.998 |
| Age (years), Mean ± SD | 15.89 ± 6.06 | 12.34 ± 3.76 | <0.001 |
| CAG Repeats, Mean ± SD | 72.19 ± 14.18 | 20.29 ± 3.91 | <0.001 |
| Parental SES, % (n) | 0.356 | ||
| 1 | 0.0 (0) | 0.8 (2) | |
| 2 | 48.0 (12) | 58.0 (149) | |
| 3 | 40.0 (10) | 37.4 (96) | |
| 4 | 8.0 (2) | 3.1 (8) | |
| 5 | 4.0 (1) | 0.8 (2) | |
| Missing | N = 2 | N = 2 | |
| BP Increasing Meds, % (n) | 11.1 (3) | 2.7 (7) | 0.087 |
| BP Decreasing Meds, % (n) | 14.8 (4) | 1.2 (3) | <0.001 |
| Disease Duration (years), | 3.38 ± 3.04 | NA | NA |
| Mean ± SD |
| JOHD Group | Controls | p-Value | |
|---|---|---|---|
| rHR, Mean ± SE | 88.56 ± 2.36 | 78.50 ± 0.83 | <0.0001 |
| SBP, Mean ± SE | 109.96 ± 1.99 | 115.99 ± 0.71 | 0.0053 |
| DBP, Mean ± SE | 61.88 ± 1.17 | 64.25 ± 0.42 | 0.060 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schultz, J.L.; Nopoulos, P.C. Autonomic Changes in Juvenile-Onset Huntington’s Disease. Brain Sci. 2020, 10, 589. https://doi.org/10.3390/brainsci10090589
Schultz JL, Nopoulos PC. Autonomic Changes in Juvenile-Onset Huntington’s Disease. Brain Sciences. 2020; 10(9):589. https://doi.org/10.3390/brainsci10090589
Chicago/Turabian StyleSchultz, Jordan L., and Peg C. Nopoulos. 2020. "Autonomic Changes in Juvenile-Onset Huntington’s Disease" Brain Sciences 10, no. 9: 589. https://doi.org/10.3390/brainsci10090589
APA StyleSchultz, J. L., & Nopoulos, P. C. (2020). Autonomic Changes in Juvenile-Onset Huntington’s Disease. Brain Sciences, 10(9), 589. https://doi.org/10.3390/brainsci10090589