Prospective Observational Study of Safety of Early Treatment with Edoxaban in Patients with Ischemic Stroke and Atrial Fibrillation (SATES Study)

 ,
,  , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
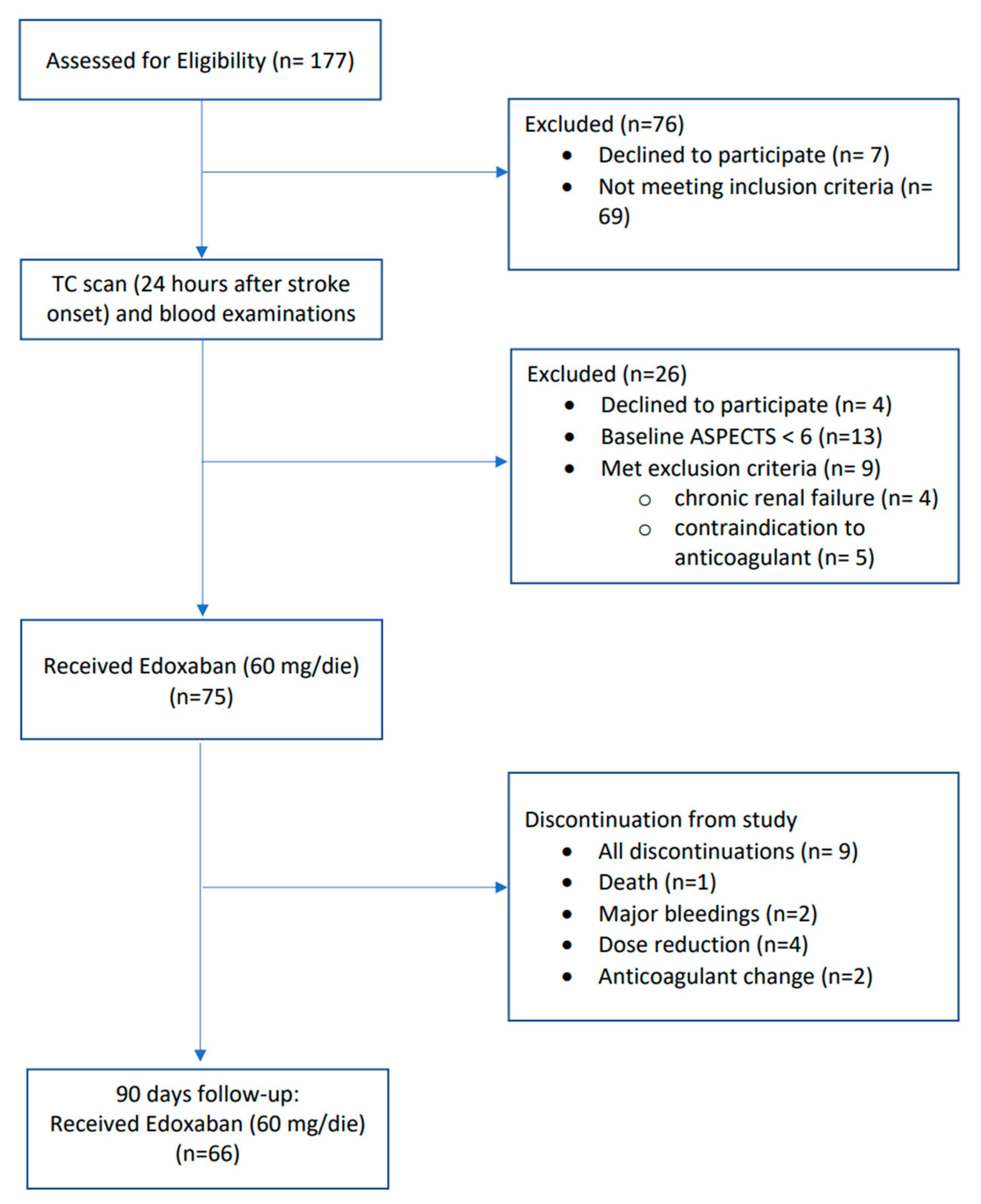
2.1. Study Design and Population
2.2. Clinical Assessment
2.3. CT/MRI Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Odutayo, A.; Wong, C.X.; Hsiao, A.J.; Hopewell, S.; Altman, D.G.; Emdin, C.A. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354, i4482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paciaroni, M.; Agnelli, G.; Falocci, N.; Caso, V.; Becattini, C.; Marcheselli, S.; Rueckert, C.; Pezzini, A.; Poli, L.; Padovani, A.; et al. Early Recurrence and Cerebral Bleeding in Patients with Acute Ischemic Stroke and Atrial Fibrillation: Effect of Anticoagulation and Its Timing: The RAF Study. Stroke 1995, 46, 2175–2182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klijn, C.J.; Paciaroni, M.; Berge, E.; Korompoki, E.; Kõrv, J.; Lal, A.; Putaala, J.; Werring, D.J. Antithrombotic treatment for secondary prevention of stroke and other thromboembolic events in patients with stroke or transient ischemic attack and non-valvular atrial fibrillation: A European Stroke Organisation guideline. Eur. Stroke J. 2019, 4, 198–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arihiro, S.; Todo, K.; Koga, M.; Furui, E.; Kinoshita, N.; Kimura, K.; Yamagami, H.; Terasaki, T.; Yoshimura, S.; Shiokawa, Y.; et al. Three-month risk-benefit profile of anticoagulation after stroke with atrial fibrillation: The SAMURAI-Nonvalvular Atrial Fibrillation (NVAF) study. Int. J. Stroke 2016, 11, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Gioia, L.C.; Kate, M.; Sivakumar, L.; Hussain, D.; Kalashyan, H.; Buck, B.; Bussiere, M.; Jeerakathil, T.; Shuaib, A.; Emery, D.; et al. Early Rivaroxaban Use After Cardioembolic Stroke May Not Result in Hemorrhagic Transformation: A Prospective Magnetic Resonance Imaging Study. Stroke 2016, 47, 1917–1919. [Google Scholar] [CrossRef]
- Seiffge, D.J.; Traenka, C.; Polymeris, A.; Hert, L.; Peters, N.; Lyrer, P.; Engelter, S.T.; Bonati, L.H.; De Marchis, G.M. Early start of DOAC after ischemic stroke: Risk of intracranial hemorrhage and recurrent events. Neurology 2016, 87, 1856–1862. [Google Scholar] [CrossRef]
- Paciaroni, M.; Angelini, F.; Agnelli, G.; Tsivgoulis, G.; Furie, K.L.; Tadi, P.; Becattini, C.; Falocci, N.; Zedde, M.; Abdul-Rahim, A.H.; et al. Prediction of early recurrent thromboembolic event and major bleeding in patients with acute stroke and atrial fibrillation by a risk stratification schema: The ALESSA score study. Stroke 2017, 48, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.; Ambler, G.; Banerjee, G.; Shakeshaft, C.; Cohen, H.; Yousry, T.A.; Al-Shahi Salman, R.; Lip, G.; Houlden, H.; Brown, M.M.; et al. Early versus late anticoagulation for ischaemic stroke associated with atrial fibrillation: Multicentre cohort study. J. Neurol. Neurosurg. Psychiatry 2019, 90, 320–325. [Google Scholar] [CrossRef] [Green Version]
- Bounameaux, H.; Camm, A.J. Edoxaban: An update on the new oral direct factor Xa inhibitor. Drugs 2014, 74, 1209–1231. [Google Scholar] [CrossRef] [Green Version]
- Goette, A.; Merino, J.L.; Ezekowitz, M.D.; Zamoryakhin, D.; Melino, M.; Jin, J.; Mercuri, M.F.; Grosso, M.A.; Fernandez, V.; Al-Saady, N.; et al. Edoxaban versus enoxaparin-warfarin in patients undergoing cardioversion of atrial fibrillation (ENSURE-AF): A randomised, open-label, phase 3b trial. Lancet 2016, 388, 1995–2003. [Google Scholar] [CrossRef]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef]
- De Marchis, G.M.; Kohler, A.; Renz, N.; Arnold, M.; Mono, M.L.; Jung, S.; Fischer, U.; Karameshev, A.I.; Brekenfeld, C.; Gralla, J.; et al. Posterior versus anterior circulation strokes: Comparison of clinical, radiological and outcome characteristics. J. Neurol. Neurosurg. Psychiatry 2011, 82, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Molina, C.A.; Alvarez-Sabín, J.; Montaner, J.; Abilleira, S.; Arenillas, J.F.; Coscojuela, P.; Romero, F.; Codina, A. Thrombolysis-related hemorrhagic infarction: A marker of early reperfusion, reduced infarct size, and improved outcome in patients with proximal middle cerebral artery occlusion. Stroke 2002, 33, 1551–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trouillas, P.; von Kummer, R. Classification and pathogenesis of cerebral hemorrhages after thrombolysis in ischemic stroke. Stroke 2006, 37, 556–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haeusler, K.G.; Tütüncü, S.; Kunze, C.; Schurig, J.; Malsch, C.; Harder, J.; Wiedmann, S.; Dimitrijeski, B.; Ebinger, M.; Hagemann, G. Oral anticoagulation in patients with atrial fibrillation and acute ischaemic stroke: Design and baseline data of the prospective multicentre Berlin Atrial Fibrillation Registry. Europace 2019, 21, 1621–1632. [Google Scholar] [CrossRef]
- Early Versus Late Initiation of Direct Oral Anticoagulants in Post-Ischaemic Stroke Patients with Atrial Fibrillation (ELAN): An International, Multicentre, randomised-Controlled, Two-Arm, Assessor-Blinded Trial (ELAN). Available online: https://clinicaltrials.gov/ct2/show/NCT03148457 (accessed on 20 June 2020).
- Optimal Timing of Anticoagulation after Acute Ischaemic Stroke: A randomised Controlled Trial (OPTIMAS). Available online: https://clinicaltrials.gov/ct2/show/NCT03759938 (accessed on 20 June 2020).
- Timing of Oral Anticoagulant Therapy in Acute Ischemic Stroke with Atrial Fibrillation. Available online: https://clinicaltrials.gov/ct2/show/NCT02961348 (accessed on 6 June 2020).
- Optimal Delay Time to Initiate Anticoagulation after Ischemic Stroke in Atrial Fibrillation (START). Available online: https://clinicaltrials.gov/ct2/show/NCT03021928 (accessed on 6 June 2020).
- Lixiana Acute Stroke Evaluation Registry (LASER). Available online: https://clinicaltrials.gov/ct2/show/NCT03494530 (accessed on 19 October 2020).
- Apixaban for Early Prevention of Recurrent Embolic Stroke and Hemorrhagic Transformation (AREST). Available online: https://clinicaltrials.gov/ct2/show/NTC02283294 (accessed on 19 October 2020).
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [Green Version]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef]
- National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1587. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Fieschi, C.; von Kummer, R.; Davalos, A.; Meier, D.; Larrue, V.; Bluhmki, E.; Davis, S.; Donnan, G.; et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998, 352, 1245–1251. [Google Scholar] [CrossRef]
- Paciaroni, M.; Agnelli, G.; Falocci, N.; Tsivgoulis, G.; Vadikolias, K.; Liantinioti, C.; Chondrogianni, M.; Bovi, P.; Carletti, M.; Cappellari, M.; et al. Early Recurrence and Major Bleeding in Patients With Acute Ischemic Stroke and Atrial Fibrillation Treated With Non-Vitamin-K Oral Anticoagulants (RAF-NOACs) Study. J. Am. Heart Assoc. 2017, 6, e007034. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Demographic Features and Risk Factors | n (%) |
|---|---|
| Age, median (y, IQR) | 78.3 (13.5) |
| Gender, female, n (%) | 48 (64) |
| Risk factors | |
| Hypertension, n (%) | 55 (73.3) |
| Diabetes mellitus, n (%) | 15 (20) |
| Hyperlipidemia, n (%) | 17 (22.7) |
| Cigarette smoking, n (%) | 13 (17.3) |
| Previous stroke/TIA, n (%) | 14 (18.6) |
| Previous vascular disease, n (%) | 14 (18.6) |
| Antiplatelet therapy prior to stroke, n (%) | 20 (26.7) |
| CHA2DS2VASc score, median (IQR) | 5 (2) |
| HASBLED score, median (IQR) | 3 (0) |
| Atrial fibrillation | |
| Paroxysmal, n (%) | 27 (36) |
| Persistent, n (%) | 2 (2.7) |
| Permanent, n (%) | 11 (14.7) |
| Unknown, n (%) | 35 (46.7) |
| OCSP 1 classification | |
| PACI 2, n (%) | 56 (74.7) |
| POCI 3, n (%) | 15 (20) |
| LACI 4, n (%) | 4 (5.3) |
| TACI 5, n (%) | 0 (0) |
| Clinical assessment and procedures | |
| Wake-up stroke, n (%) | 14 (18.9) |
| NIHSS 6 at stroke onset, median (IQR) | 6 (8) |
| NIHSS after revascularization, median (IQR) | 5 (5.5) |
| NIHSS after discharge, median (IQR) | 2 (5) |
| GCS 7 at stroke onset, median (IQR) | 15 (1) |
| Thrombolysis, n (%) | 28 (37.3) |
| Thrombectomy, n (%) | 17 (22.7) |
| Neuroradiological Features | |
|---|---|
| ASPECT 1 at Emergency Department CT scan, median (IQR) | 10 (1) |
| HT 2 at Emergency Department CT scan, n (%) | 2 (2.7) |
| HT subtypes, (n) | HI-1 3 (1), HI-2 4 (1), PH-1 5 (0), PH-2 6 (0) |
| ASPECT after 24 h from the stroke onset, median (IQR) | 8 (1) |
| HT on brain MRI, 5 days after stroke onset, n (%) | 16 (21.3) |
| HT subtypes, (n) | HI-1 (9), HI-2 (5), PH-1 (2), PH-2 (0) |
| Clinical Evaluation at 3 Months Follow-Up | |
|---|---|
| Intracranial bleedings, n (%) | 0 (0) |
| Major bleedings, n (%) | 2 (2.7) |
| Minor bleedings, n (%) | 11 (14.7) |
| Blood transfusion, n (%) | 0 (0) |
| Hospitalization, n (%) | 4 (5.4) |
| Deaths, n (%) | 1 (1.3) |
| mRS 1, median (IQR) | 1 (2) |
| Adherence to treatment, n (%) | 69 (92) |
| Stroke recurrence, n (%) | 0 (0) |
| Myocardial infarction, n (%) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frisullo, G.; Profice, P.; Brunetti, V.; Scala, I.; Bellavia, S.; Broccolini, A.; Caliandro, P.; Di Iorio, R.; Morosetti, R.; Pilato, F.; et al. Prospective Observational Study of Safety of Early Treatment with Edoxaban in Patients with Ischemic Stroke and Atrial Fibrillation (SATES Study). Brain Sci. 2021, 11, 30. https://doi.org/10.3390/brainsci11010030
Frisullo G, Profice P, Brunetti V, Scala I, Bellavia S, Broccolini A, Caliandro P, Di Iorio R, Morosetti R, Pilato F, et al. Prospective Observational Study of Safety of Early Treatment with Edoxaban in Patients with Ischemic Stroke and Atrial Fibrillation (SATES Study). Brain Sciences. 2021; 11(1):30. https://doi.org/10.3390/brainsci11010030
Chicago/Turabian StyleFrisullo, Giovanni, Paolo Profice, Valerio Brunetti, Irene Scala, Simone Bellavia, Aldobrando Broccolini, Pietro Caliandro, Riccardo Di Iorio, Roberta Morosetti, Fabio Pilato, and et al. 2021. "Prospective Observational Study of Safety of Early Treatment with Edoxaban in Patients with Ischemic Stroke and Atrial Fibrillation (SATES Study)" Brain Sciences 11, no. 1: 30. https://doi.org/10.3390/brainsci11010030
APA StyleFrisullo, G., Profice, P., Brunetti, V., Scala, I., Bellavia, S., Broccolini, A., Caliandro, P., Di Iorio, R., Morosetti, R., Pilato, F., Laborante, R., & Della Marca, G. (2021). Prospective Observational Study of Safety of Early Treatment with Edoxaban in Patients with Ischemic Stroke and Atrial Fibrillation (SATES Study). Brain Sciences, 11(1), 30. https://doi.org/10.3390/brainsci11010030