
Metacognitive Performance on Memory and Visuospatial Tasks in Functional Cognitive Disorder

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Selection
2.2. Assessment Procedure
2.3. Statistical Analysis
2.4. Research Ethics
3. Results
3.1. Participant Characteristics
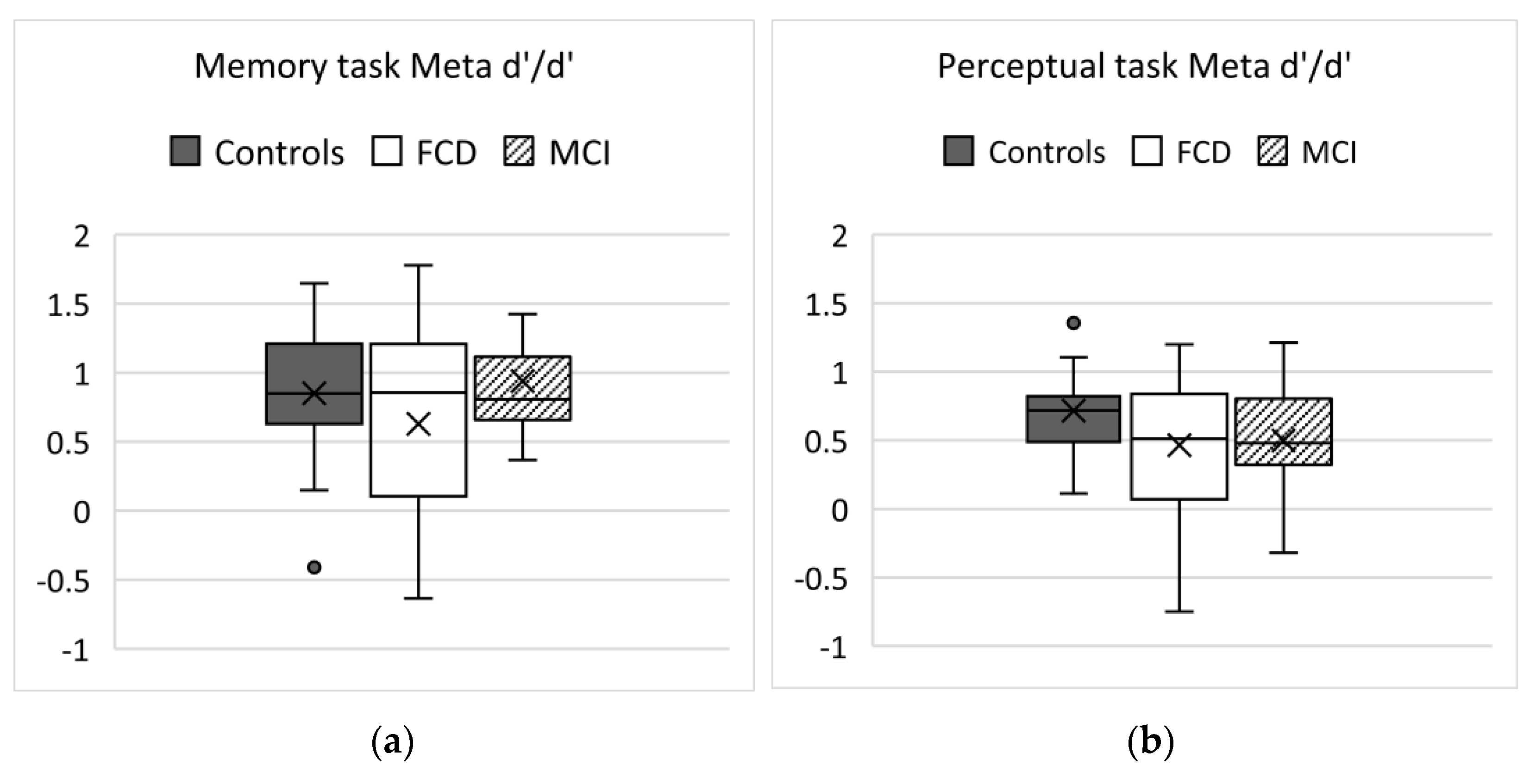
3.2. Memory Task Results
3.3. Perceptual Task Results
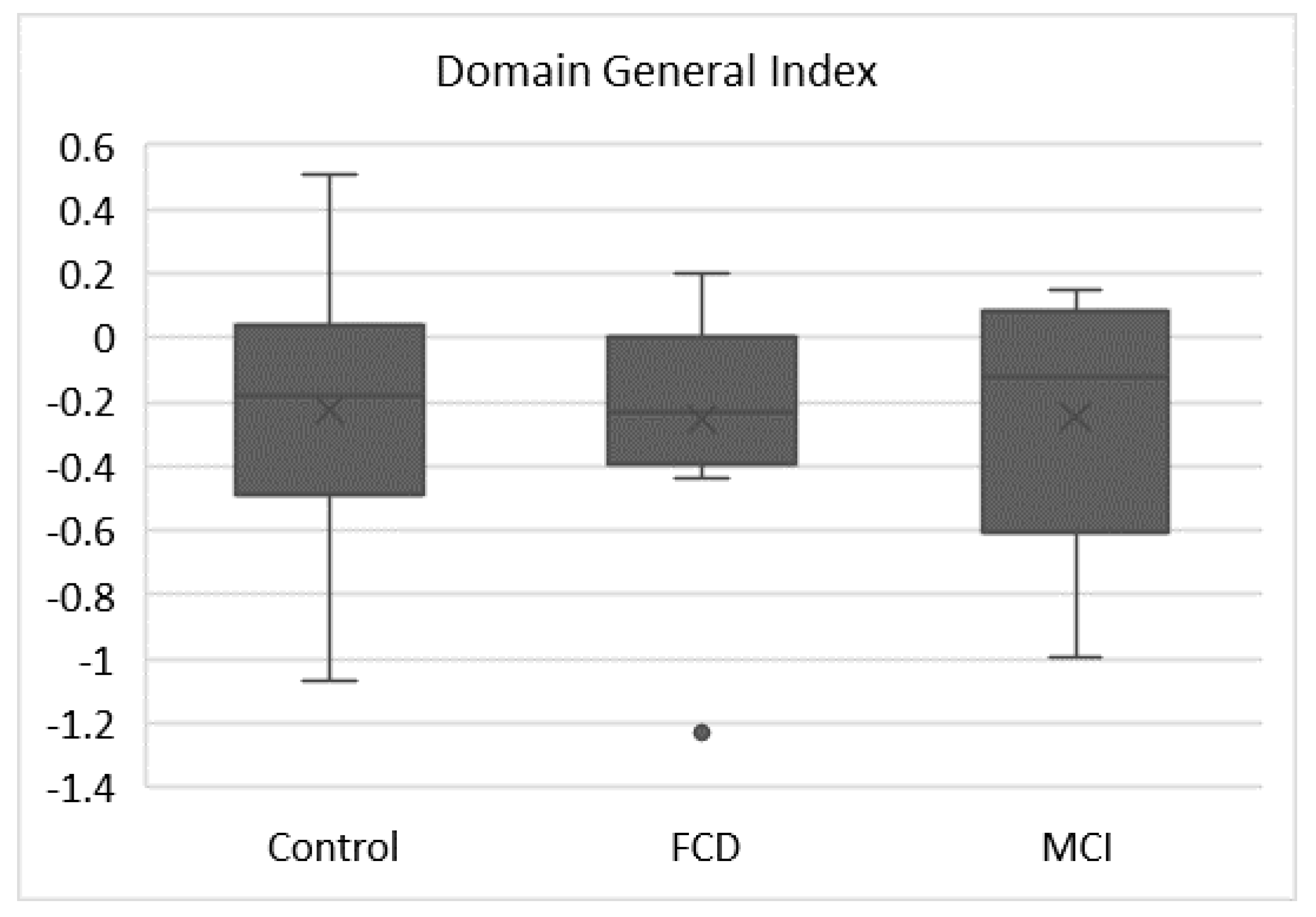
3.4. Domain General Index
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rouault, M.; McWilliams, A.; Allen, M.G.; Fleming, S.M. Human Metacognition across Domains: Insights from Individual Differences and Neuroimaging. Pers. Neurosci. 2018, 1, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Sunderaraman, P.; Cosentino, S. Integrating the Constructs of Anosognosia and Metacognition: A Review of Recent Findings in Dementia. Curr. Neurol. Neurosci. Rep. 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Bastin, C.; Giacomelli, F.; Miévis, F.; Lemaire, C.; Guillaume, B.; Salmon, E. Anosognosia in Mild Cognitive Impairment: Lack of Awareness of Memory Difficulties Characterizes Prodromal Alzheimer’s Disease. Front. Psychiatry 2021, 12, 1–15. [Google Scholar] [CrossRef]
- Pennington, C.; Hayre, A.; Newson, M.; Coulthard, E. Functional Cognitive Disorder: A Common Cause of Subjective Cognitive Symptoms. J. Alzheimer’s Dis. 2015, 48, S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Ball, H.A.; McWhirter, L.; Ballard, C.; Bhome, R.; Blackburn, D.J.; Edwards, M.J.; Fleming, S.M.; Fox, N.C.; Howard, R.; Huntley, J.; et al. Functional cognitive disorder: dementia’s blind spot. Brain 2020, 143, 2895–2903. [Google Scholar] [CrossRef] [PubMed]
- Lehn, A.; Gelauff, J.; Hoeritzauer, A.I.; Ludwig, L.; McWhirter, L.; Williams, S.; Gardiner, P.; Carson, A.; Stone, J. Functional neurological disorders: mechanisms and treatment. J. Neurol. 2016, 263, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Fleming, S.M.; Dolan, R.J. The neural basis of metacognitive ability. In The Cognitive Neuroscience of Metacognition; Springer-Verlag: Berlin/Heidelberg, Germany, 2014; pp. 245–265. [Google Scholar] [CrossRef] [Green Version]
- Fleming, S.M.; Lau, H.C. How to measure metacognition. Front. Hum. Neurosci. 2014, 8, 443. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.; Blackburn, D.; Reuber, M. Patients’ accounts of memory lapses in interactions between neurologists and patients with functional memory disorders. Sociol. Heal. Illn. 2019, 41, 249–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pareés, I.; Saifee, T.; Kassavetis, P.; Kojovic, M.; Rubio-Agusti, I.; Rothwell, J.; Bhatia, K.; Edwards, M.J. Believing is perceiving: mismatch between self-report and actigraphy in psychogenic tremor. Brain 2011, 135, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, J.; Carson, A. Functional Neurologic Symptoms: Assessment and Management. Neurol. Clin. 2011, 29, 1–18. [Google Scholar] [CrossRef]
- Starkstein, S.E. Anosognosia in Alzheimer’s disease: Diagnosis, frequency, mechanism and clinical correlates. Cortex 2014, 61, 64–73. [Google Scholar] [CrossRef]
- Vannini, P.; Hanseeuw, B.; Munro, C.E.; Amariglio, R.E.; Marshall, G.A.; Rentz, D.M.; Pascual-Leone, A.; Johnson, K.A.; Sperling, R.A. Anosognosia for memory deficits in mild cognitive impairment: Insight into the neural mechanism using functional and molecular imaging. NeuroImage Clin. 2017, 15, 408–414. [Google Scholar] [CrossRef]
- Pennington, C.; Ball, H.; Swirski, M. Functional Cognitive Disorder: Diagnostic Challenges and Future Directions. Diagnostics 2019, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- Ball, H.A.; Swirski, M.; Newson, M.; Coulthard, E.J.; Pennington, C.M. Differentiating functional cognitive disorder from early neurodegeneration: A clinic-based study. Brain Sci. 2021, 11, 800. [Google Scholar] [CrossRef] [PubMed]
- Fleming, S.M.; Ryu, J.; Golfinos, J.G.; Blackmon, K.E. Domain-specific impairment in metacognitive accuracy following anterior prefrontal lesions. Brain 2014, 137, 2811–2822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maniscalco, B.; Lau, H. A signal detection theoretic approach for estimating metacognitive sensitivity from confidence ratings. Conscious. Cogn. 2012, 21, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Griem, J.; Stone, J.; Carson, A.; Kopelman, M. Psychologic/Functional Forms of Memory Disorder, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2016. [Google Scholar] [CrossRef]
- Tamietto, M.; Corazzini, L.L.; Castelli, L.; Geminiani, G. Domain-Specific Anosognosia in Alzheimer’s Disease and Vascular Dementia. Brain Impair. 2004, 5, 187–197. [Google Scholar] [CrossRef]
- Snowden, J.; Gibbons, Z.; Blackshaw, A.; Doubleday, E.; Thompson, J.; Craufurd, D.; Foster, J.; Happé, F.; Neary, D. Social cognition in frontotemporal dementia and Huntington’s disease. Neuropsychologia 2003, 41, 688–701. [Google Scholar] [CrossRef]
- Fleming, S.; Dolan, R. The neural basis of metacognitive ability. Philos. Trans. R. Soc. B Biol. Sci. 2012, 367, 1338–1349. [Google Scholar] [CrossRef]
- Chudoba, L.A.; Schmitter-Edgecombe, M. Insight into memory and functional abilities in individuals with amnestic mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2020, 42, 822–833. [Google Scholar] [CrossRef]
- Vannini, P.; Amariglio, R.; Hanseeuw, B.; Johnson, K.A.; McLaren, D.G.; Chhatwal, J.; Pascual-Leone, A.; Rentz, D.; Sperling, R.A. Memory self-awareness in the preclinical and prodromal stages of Alzheimer’s disease. Neuropsychologia 2017, 99, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, M.J.; Fotopoulou, A.; Pareés, I. Neurobiology of functional (psychogenic) movement disorders. Curr. Opin. Neurol. 2013, 26, 442–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, S.H.; Plant, G.T. How to interpret visual fields. Pr. Neurol. 2015, 15, 374–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, D.; Drew, P.; Elsey, C.; Blackburn, D.; Wakefield, S.; Harkness, K.; Reuber, M. Conversational assessment in memory clinic encounters: interactional profiling for differentiating dementia from functional memory disorders. Aging Ment. Health 2015, 20, 500–509. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| FCD | nMCI | HC | FCD vs. HC p Value | FCD vs. nMCI p Value | nMCI vs. HC p Value | |
|---|---|---|---|---|---|---|
| Female:Male | 9:11 | 8:6 | 16:7 | 0.043 | ||
| Age (years) | 57.2 | 70.6 | 60.7 | 0.882 | 0.003 | 0.048 |
| Years of Education | 13.9 | 14.4 | 15.1 | 0.48 * | ||
| MoCA | 23.7 | 23.6 | 27.7 | 0.003 | 1.00 | 0.001 |
| Study Time | % Correct (Mean) | % Correct (SD) | Confidence 1 (Mean) | Confidence (SD) | Meta-d’/d’ | Meta-d’/d’ (SD) | |
|---|---|---|---|---|---|---|---|
| FCD | 30 s | 60.00 | 9.43 | 2.84 | 0.82 | 0.63 | 0.68 |
| 60 s | 66.10 | 8.96 | 3.23 | 0.78 | |||
| 90 s | 64.95 | 13.60 | 3.57 | 0.93 | |||
| Mean | 63.65 | 7.75 | 3.19 | 0.74 | |||
| nMCI | 30 s | 62.14 | 7.98 | 3.37 | 0.60 | 0.94 | 0.47 |
| 60 s | 62.86 | 8.25 | 3.63 | 0.50 | |||
| 90 s | 66.86 | 10.58 | 3.77 | 0.64 | |||
| Mean | 63.96 | 9.04 | 3.59 | 0.59 | |||
| HC | 30 s | 66.87 | 8.98 | 3.41 | 0.75 | 0.85 | 0.46 |
| 60 s | 71.83 | 8.16 | 3.70 | 0.73 | |||
| 90 s | 74.96 | 11.00 | 4.01 | 0.60 | |||
| Mean | 71.22 | 7.19 | 3.71 | 0.61 |
| % Correct (Mean) | % Correct (SD) | Confidence (Mean) | Confidence (SD) | Meta-d’/d’ | Meta-d’/d’ (SD) | |
|---|---|---|---|---|---|---|
| FCD | 63.97 | 5.55 | 3.71 | 0.51 | 0.50 | 0.51 |
| nMCI | 64.50 | 2.10 | 3.43 | 0.60 | 0.51 | 0.40 |
| HC | 65.86 | 1.85 | 3.88 | 0.69 | 0.72 | 0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pennington, C.; Ball, H.; Swirski, M.; Newson, M.; Coulthard, E. Metacognitive Performance on Memory and Visuospatial Tasks in Functional Cognitive Disorder. Brain Sci. 2021, 11, 1368. https://doi.org/10.3390/brainsci11101368
Pennington C, Ball H, Swirski M, Newson M, Coulthard E. Metacognitive Performance on Memory and Visuospatial Tasks in Functional Cognitive Disorder. Brain Sciences. 2021; 11(10):1368. https://doi.org/10.3390/brainsci11101368
Chicago/Turabian StylePennington, Catherine, Harriet Ball, Marta Swirski, Margaret Newson, and Elizabeth Coulthard. 2021. "Metacognitive Performance on Memory and Visuospatial Tasks in Functional Cognitive Disorder" Brain Sciences 11, no. 10: 1368. https://doi.org/10.3390/brainsci11101368
APA StylePennington, C., Ball, H., Swirski, M., Newson, M., & Coulthard, E. (2021). Metacognitive Performance on Memory and Visuospatial Tasks in Functional Cognitive Disorder. Brain Sciences, 11(10), 1368. https://doi.org/10.3390/brainsci11101368