
Effectiveness of Unihemispheric Concurrent Dual-Site Stimulation over M1 and Dorsolateral Prefrontal Cortex Stimulation on Pain Processing: A Triple Blind Cross-Over Control Trial


 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
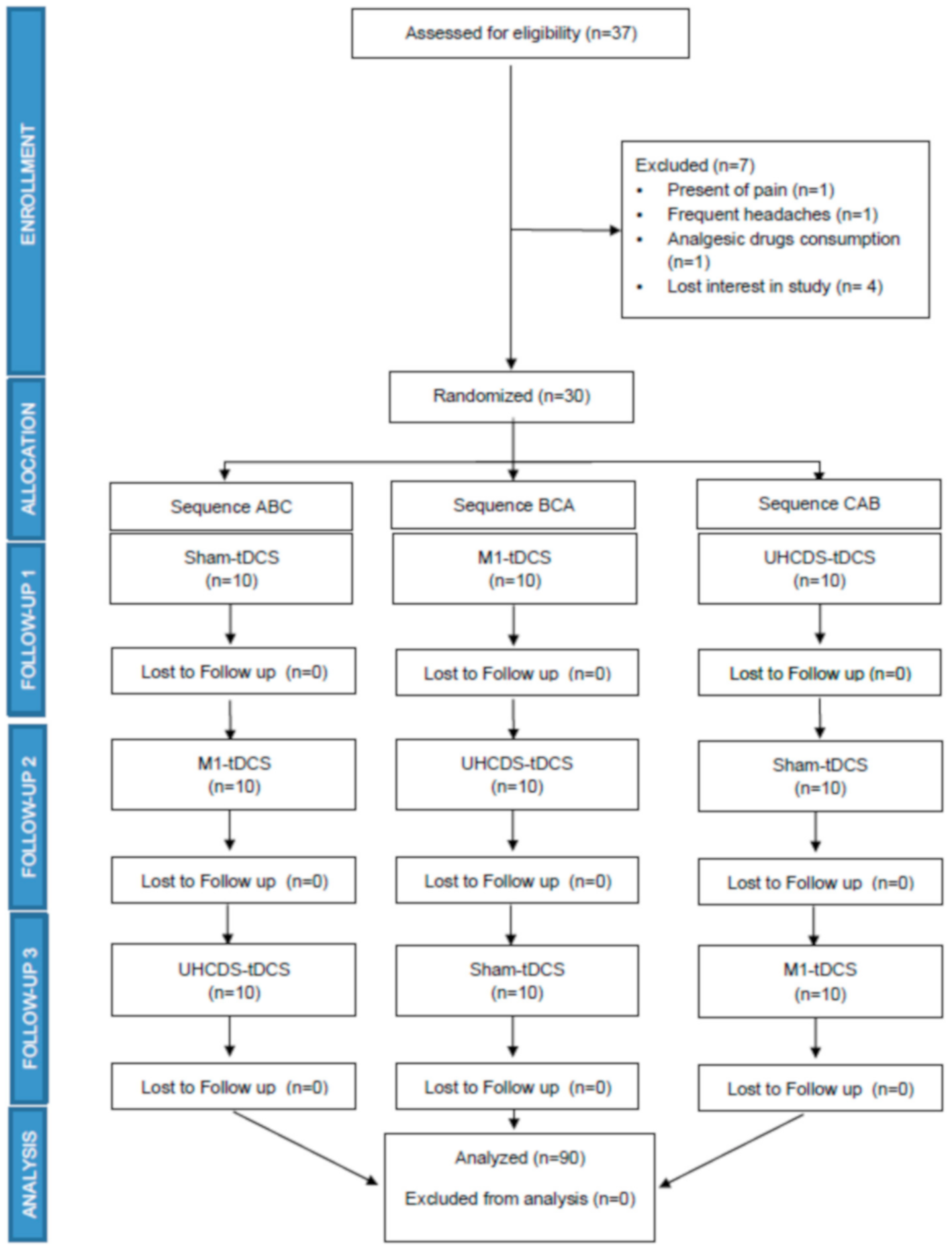
2.1. Study Design and Participants
- Inclusion criteria and recruitment
2.2. Intervention Protocols
- Direct current stimulation intervention
2.3. Outcomes Measurement
- Pressure pain threshold
- Widespread mechanical hyperalgesia
- Temporal summation
- Conditioned pain modulation
Secondary Outcomes
- Pain pressure tolerance
- Neural tension test
- Cold pain intensity
- Maximal isometric grip strength
- State–trait anxiety inventory
- Beck Depression Inventory-II
- Pain Catastrophizing Scale
- Tampa Scale for Kinesiophobia
- Fear of Pain Questionnaire III
- The Pittsburgh Sleep Quality Index
- International Physical Activity Questionnaire Short Form
2.4. Sample Size Calculation
2.5. Data Analyses
3. Results
Demographic and Clinical Characteristics
- Differences in the outcomes by gender
- Pressure pain threshold
- Pressure pain threshold (over finger)
- Pressure pain threshold (trapezius muscle)
- Pressure pain threshold over tibial muscle
- Widespread mechanical hyperalgesia
- Temporal summation
- Conditioned pain modulation
- Pain tolerance
- Neural tension test
- Cold Hyperalgesia
- Maximal isometric grip strength
4. Discussion
- Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Kuo, H.; Datta, A.; Bikson, M.; Paulus, W.; Kuo, M.; Nitsche, M.A. Brain stimulation comparing cortical plasticity induced by conventional and high-definition 4 × 1 ring tDCS: A neurophysiological study. Brain Stimul. 2012, 1–5. [Google Scholar] [CrossRef]
- Da Silva, N.R.J.; Laste, G.; Deitos, A.; Stefani, L.C.; Cambraia-Canto, G.; Torres, I.L.S.; Brunoni, A.R.; Fregni, F.; Caumo, W. Combined neuromodulatory interventions in acute experimental pain: Assessment of melatonin and non-invasive brain stimulation. Front. Behav. Neurosci. 2015, 9, 77. [Google Scholar] [CrossRef] [Green Version]
- Caparelli-Daquer, E.M.; Zimmermann, T.J.; Mooshagian, E.; Parra, L.C.; Rice, J.K.; Datta, A.; Bikson, M.; Wassermann, E.M. A pilot study on effects of 4 × 1 High-Definition tDCS on motor cortex excitability. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2012, 2012, 735–738. [Google Scholar]
- Naegel, S.; Biermann, J.; Theysohn, N.; Kleinschnitz, C.; Diener, H.C.; Katsarava, Z.; Obermann, M.; Holle, D. Polarity-specific modulation of pain processing by transcranial direct current stimulation-A blinded longitudinal fMRI study. J. Headache Pain 2018, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lang, N.; Siebner, H.R.; Ward, N.S.; Lee, L.; Nitsche, M.A.; Paulus, W.; Rothwell, J.C.; Lemon, R.N.; Frackowiak, R.S. How does transcranial DC stimulation of the primary motor cortex alter regional neuronal activity in the human brain? Eur. J. Neurosci. 2005, 22, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Ihle, K.; Rodriguez-Raecke, R.; Luedtke, K.; May, A. TDCS modulates cortical nociceptive processing but has little to no impact on pain perception. Pain 2014, 155, 2080–2087. [Google Scholar] [CrossRef]
- Flood, A.; Waddington, G.; Cathcart, S. High-definition transcranial direct current stimulation enhances conditioned pain modulation in healthy volunteers: A randomized trial. J. Pain 2016, 17, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Braulio, G.; Passos, S.C.; Leite, F.; Schwertner, A.; Stefani, L.C.; Palmer, A.C.S.; Torres, I.L.S.; Fregni, F.; Caumo, W. Effects of transcranial direct current stimulation block remifentanil-induced hyperalgesia: A randomized, double-blind clinical trial. Front. Pharmacol. 2018, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Reidler, J.S.; Mendonca, M.E.; Santana, M.B.; Wang, X.; Lenkinski, R.; Motta, A.F.; Marchand, S.; Latif, L.; Fregni, F. Effects of motor cortex modulation and descending inhibitory systems on pain thresholds in healthy subjects. J. Pain 2012, 13, 450–458. [Google Scholar] [CrossRef]
- Borckardt, J.J.; Bikson, M.; Frohman, H.; Reeves, S.T.; Datta, A.; Bansal, V.; Madan, A.; Barth, K.; George, M.S. A pilot study of the tolerability and effects of high-definition transcranial direct current stimulation (HD-tDCS) on pain perception. J. Pain 2012, 13, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Aslaksen, P.M.; Vasylenko, O.; Fagerlund, A.J. The effect of transcranial direct current stimulation on experimentally induced heat pain. Exp. Brain Res. 2014, 232, 1865–1873. [Google Scholar] [CrossRef]
- Antal, A.; Brepohl, N.; Poreisz, C.; Boros, K.; Csifcsak, G.; Paulus, W. Transcranial direct current stimulation over somatosensory cortex decreases experimentally Induced acute pain perception. Clin. J. Pain 2008, 24, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Boggio, P.S.; Zaghi, S.; Lopes, M.; Fregni, F. Modulatory effects of anodal transcranial direct current stimulation on perception and pain thresholds in healthy volunteers. Eur. J. Neurol. 2008, 15, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- Flood, A.; Waddington, G.; Keegan, R.J.; Thompson, K.G.; Cathcart, S. The effects of elevated pain inhibition on endurance exercise performance. PeerJ 2017, 5, e3028. [Google Scholar] [CrossRef] [Green Version]
- Gandiga, P.C.; Hummel, F.C.; Cohen, L.G. Transcranial DC stimulation (tDCS): A tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 2006, 117, 845–850. [Google Scholar] [CrossRef]
- Rêgo, G.G.; Lapenta, O.M.; Marques, L.M.; Costa, T.L.; Leite, J.; Carvalho, S.; Gonçalves, Ó.F.; Brunoni, A.R.; Fregni, F.; Boggio, P.S. Hemispheric dorsolateral prefrontal cortex lateralization in the regulation of empathy for pain. Neurosci. Lett. 2015, 594, 12–16. [Google Scholar] [CrossRef]
- Mariano, T.Y.; van Wout, M.; Garnaat, S.L.; Rasmussen, S.A.; Greenberg, B.D. Transcranial direct current stimulation (tDCS) targeting left dorsolateral prefrontal cortex modulates task-induced acute pain in healthy volunteers. Pain Med. 2016, 17, 737–745. [Google Scholar] [CrossRef] [Green Version]
- Vaseghi, B.; Zoghi, M.; Jaberzadeh, S. How does anodal transcranial direct current stimulation of the pain neuromatrix affect brain excitability and pain perception? A randomised, double-blind, sham-control study. PLoS ONE 2015, 10, e0118340. [Google Scholar] [CrossRef] [Green Version]
- Ong, W.Y.; Stohler, C.S.; Herr, D.R. Role of the prefrontal cortex in pain processing. Mol. Neurobiol. 2019, 56, 1137–1166. [Google Scholar] [CrossRef] [Green Version]
- Sankarasubramanian, V.; Cunningham, D.A.; Potter-Baker, K.A.; Beall, E.B.; Varnerin, N.M.; Machado, A.G.; Jones, S.E.; Roelle, S.M.; Lowe, M.J.; Plow, E.B. Transcranial direct current stimulation targeting primary motor versus dorsolateral prefrontal cortices: Proof-of-concept study investigating functional connectivity of thalamocortical networks specific to sensory-affective information processing. Brain Connect. 2017, 7, 182–196. [Google Scholar] [CrossRef] [Green Version]
- Vaseghi, B.; Zoghi, M.; Jaberzadeh, S. The effects of anodal-tDCS on corticospinal excitability enhancement and its after-effects: Conventional vs. unihemispheric concurrent dual-site stimulation. Front. Hum. Neurosci. 2015, 9, 533. [Google Scholar] [CrossRef] [Green Version]
- Talimkhani, A.; Abdollahi, I.; Mohseni-Bandpei, M.A.; Ehsani, F.; Khalili, S.; Jaberzadeh, S. Research paper: Differential effects of unihemispheric concurrent dual-site and conventional tDCS on motor learning: A randomized, sham-controlled study. Basic Clin. Neurosci. 2019, 10, 59–71. [Google Scholar] [CrossRef]
- Achacheluee, S.T.; Rahnama, L.; Karimi, N.; Abdollahi, I.; Arslan, S.A.; Jaberzadeh, S. The effect of unihemispheric concurrent dual-site transcranial direct current stimulation of primary motor and dorsolateral prefrontal cortices on motor function in patients with sub-acute stroke. Front. Hum. Neurosci. 2018, 12, 441. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Grimsey, S.; Strutton, P.H. Primary motor cortex transcranial direct current stimulation modulates temporal summation of the nociceptive withdrawal reflex in healthy subjects. Pain Med. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jeric, K.; Hrobjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. Declaración SPIRIT 2013: Definición de los Elementos Estándares del Protocolo de un Ensayo Clínico. Inf. Espec./Spec. Rep. 2015, 38, 506–514. [Google Scholar]
- Ridding, M.C.; Ziemann, U. Determinants of the induction of cortical plasticity by non-invasive brain stimulation in healthy subjects. J. Physiol. 2010, 588, 2291–2304. [Google Scholar] [CrossRef] [PubMed]
- Guerra, A.; López-Alonso, V.; Cheeran, B.; Suppa, A. Solutions for managing variability in non-invasive brain stimulation studies. Neurosci. Lett. 2020, 719, 133332. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Amadera, J.; Berbel, B.; Volz, M.S.; Rizzerio, B.G.; Fregni, F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int. J. Neuropsychopharmacol. 2011, 14, 1133–1145. [Google Scholar] [CrossRef]
- Loo, C.K.; Sachdev, P.; Martin, D.; Pigot, M.; Alonzo, A.; Malhi, G.S.; Lagopoulos, J.; Mitchell, P. A double-blind, sham-controlled trial of transcranial direct current stimulation for the treatment of depression. Int. J. Neuropsychopharmacol. 2010. [Google Scholar] [CrossRef] [PubMed]
- Pixa, N.H.; Berger, A.; Steinberg, F.; Doppelmayr, M. Parietal, but not motor cortex, HD-atDCS deteriorates learning transfer of a complex bimanual coordination task. J. Cogn. Enhanc. 2019. [Google Scholar] [CrossRef]
- Chesterton, L.S.; Barlas, P.; Foster, N.E.; Baxter, G.D.; Wright, C.C. Gender differences in pressure pain threshold in healthy humans. Pain 2003, 101, 259–266. [Google Scholar] [CrossRef]
- Amer-Cuenca, J.J.; Pecos-Martín, D.; Martínez-Merinero, P.; Lluch Girbés, E.; Nijs, J.; Meeus, M.; Ferrer Peña, R.; Fernández-Carnero, J. How much is needed? Comparison of the effectiveness of different pain education dosages in patients with fibromyalgia. Pain Med. 2020, 21, 782–793. [Google Scholar] [CrossRef]
- Coronado, R.A.; George, S.Z. The central sensitization inventory and pain sensitivity questionnaire: An exploration of construct validity and associations with widespread pain sensitivity among individuals with shoulder pain. Musculoskelet. Sci. Pract. 2018, 36, 61–67. [Google Scholar] [CrossRef]
- Fischer, A.A. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain 1987, 30, 115–126. [Google Scholar] [CrossRef]
- Nussbaum, E.L.; Downes, L. Reliability of clinical pressure-pain algometric measurements obtained on consecutive days. Phys. Ther. 1998, 78, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Rolke, R.; Baron, R.; Maier, C.; Tölle, T.R.; Treede, R.-D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Bötefür, I.C.; et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Cathcart, S.; Winefield, A.H.; Rolan, P.; Lushington, K. Reliability of temporal summation and diffuse noxious inhibitory control. Pain Res. Manag. 2009, 14, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Nie, H.; Arendt-Nielsen, L.; Andersen, H.; Graven-Nielsen, T. Temporal summation of pain evoked by mechanical stimulation in deep and superficial tissue. J. Pain 2005, 6, 348–355. [Google Scholar] [CrossRef]
- Flood, A.; Waddington, G.; Cathcart, S. Examining the relationship between endogenous pain modulation capacity and endurance exercise performance. Res. Sport. Med. 2017, 25, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Vaegter, H.B.; Handberg, G.; Graven-Nielsen, T. Similarities between exercise-induced hypoalgesia and conditioned pain modulation in humans. Pain 2014, 155, 158–167. [Google Scholar] [CrossRef]
- Butler, D.S.; David, S.; Matheson, J. The Sensitive Nervous System; Noigroup Publications: Adelaide, Australia, 2000; ISBN 9780975091029. [Google Scholar]
- Schmid, A.B.; Brunner, F.; Luomajoki, H.; Held, U.; Bachmann, L.M.; Künzer, S.; Coppieters, M.W. Reliability of clinical tests to evaluate nerve function and mechanosensitivity of the upper limb peripheral nervous system. BMC Musculoskelet. Disord. 2009, 10, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coppieters, M.; Stappaerts, K.; Janssens, K.; Jull, G. Reliability of detecting “onset of pain” and “submaximal pain” during neural provocation testing of the upper quadrant. Physiother. Res. Int. 2002, 7, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, S.; Sterling, M. An investigation of the use of a numeric pain rating scale with ice application to the neck to determine cold hyperalgesia. Man. Ther. 2013, 18, 172–174. [Google Scholar] [CrossRef] [PubMed]
- Sterling, M.; Jull, G.; Vicenzino, B.; Kenardy, J. Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery. Pain 2003, 104, 509–517. [Google Scholar] [CrossRef]
- Hamilton, G.F.; McDonald, C.; Chenier, T.C. Measurement of grip strength: Validity and reliability of the sphygmomanometer and Jamar grip dynamometer. J. Orthop. Sports Phys. Ther. 1992, 16, 215–219. [Google Scholar] [CrossRef]
- Fan, J.; Voisin, J.; Milot, M.H.; Higgins, J.; Boudrias, M.H. Transcranial direct current stimulation over multiple days enhances motor performance of a grip task. Ann. Phys. Rehabil. Med. 2017, 60, 329–333. [Google Scholar] [CrossRef]
- Hendy, A.M.; Kidgell, D.J. Anodal-tDCS applied during unilateral strength training increases strength and corticospinal excitability in the untrained homologous muscle. Exp. Brain Res. 2014, 232, 3243–3252. [Google Scholar] [CrossRef]
- Frazer, A.K.; Williams, J.; Spittle, M.; Kidgell, D.J. Cross-education of muscular strength is facilitated by homeostatic plasticity. Eur. J. Appl. Physiol. 2017, 117, 665–677. [Google Scholar] [CrossRef]
- Hendy, A.M.; Teo, W.P.; Kidgell, D.J. Anodal transcranial direct current stimulation prolongs the cross-education of strength and corticomotor plasticity. Med. Sci. Sports Exerc. 2015, 47, 1788–1797. [Google Scholar] [CrossRef]
- Spielberger, C. Development of the spanish edition of the state-trait anxiety inventory. Interam. J. Psychol. 1971, 5, 145–158. [Google Scholar]
- Wiebe, J.S.; Penley, J.A. A psychometric comparison of the Beck Depression Inventory-II in English and Spanish. Psychol. Assess. 2005, 17, 481–485. [Google Scholar] [CrossRef]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validación de la versión española de la escala de la catastrofización ante el dolor (Pain Catastrophizing Scale) en la fibromialgia. Med. Clin. (Barc.) 2008, 131, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pérez, L.; López-Martínez, A.E.; Ruiz-Párraga, G.T. Psychometric properties of the spanish version of the tampa scale for kinesiophobia (TSK). J. Pain 2011, 12, 425–435. [Google Scholar] [CrossRef]
- Solé, E.; Castarlenas, E.; Sánchez-Rodríguez, E.; Galán, S.; de la Vega, R.; Jensen, M.P.; Miró, J. The reliability and validity of the Spanish version of the Fear of Pain Questionnaire. J. Health Psychol. 2019, 24, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef]
- Mantilla Toloza, S.C.; Gómez-Conesa, A. El cuestionario internacional de actividad física. Un instrumento adecuado en el seguimiento de la actividad física poblacional. Rev. Iberoam. Fisioter. Kinesiol. 2007, 10, 48–52. [Google Scholar] [CrossRef]
- Hughes, S.; Ali, M.; Sharma, P.; Insan, N.; Strutton, P.H. Frequency-dependent top-down modulation of temporal summation by anodal transcranial direct-current stimulation of the primary motor cortex in healthy adults. Eur. J. Pain 2018, 22, 1494–1501. [Google Scholar] [CrossRef]
- Dasilva, A.F.; Mendonca, M.E.; Zaghi, S.; Lopes, M.; Dossantos, M.F.; Spierings, E.L.; Bajwa, Z.; Datta, A.; Bikson, M.; Fregni, F. TDCS-induced analgesia and electrical fields in pain-related neural networks in chronic migraine. Headache 2012, 52, 1283–1295. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Sluka, K.A.; Nie, H.L. Experimental muscle pain impairs descending inhibition. Pain 2008, 140, 465–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yarnitsky, D.; Bouhassira, D.; Drewes, A.M.; Fillingim, R.B.; Granot, M.; Hansson, P.; Landau, R.; Marchand, S.; Matre, D.; Nilsen, K.B.; et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur. J. Pain 2015, 19, 805–806. [Google Scholar] [CrossRef]
- Quiton, R.L.; Greenspan, J.D. Sex differences in endogenous pain modulation by distracting and painful conditioning stimulation. Pain 2007, 132, S134. [Google Scholar] [CrossRef] [Green Version]
- Imai, Y.; Petersen, K.K.; Mørch, C.D.; Arendt Nielsen, L. Comparing test–retest reliability and magnitude of conditioned pain modulation using different combinations of test and conditioning stimuli. Somatosens. Mot. Res. 2016, 33, 169–177. [Google Scholar] [CrossRef]
- Bachmann, C.G.; Muschinsky, S.; Nitsche, M.A.; Rolke, R.; Magerl, W.; Treede, R.D.; Paulus, W.; Happe, S. Transcranial direct current stimulation of the motor cortex induces distinct changes in thermal and mechanical sensory percepts. Clin. Neurophysiol. 2010, 121, 2083–2089. [Google Scholar] [CrossRef]
- Grundmann, L.; Rolke, R.; Nitsche, M.A.; Pavlakovic, G.; Happe, S.; Treede, R.D.; Paulus, W.; Bachmann, C.G. Effects of transcranial direct current stimulation of the primary sensory cortex on somatosensory perception. Brain Stimul. 2011, 4, 253–260. [Google Scholar] [CrossRef]
- Lattari, E.; Oliveira, B.R.R.; Monteiro Júnior, R.S.; Marques Neto, S.R.; Oliveira, A.J.; Maranhão Neto, G.A.; Machado, S.; Budde, H. Acute effects of single dose transcranial direct current stimulation on muscle strength: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0209513. [Google Scholar] [CrossRef] [Green Version]
- Machado, S.; Jansen, P.; Almeida, V.; Veldema, J. Is tDCS an adjunct ergogenic resource for improving muscular strength and endurance performance? A systematic review. Front. Psychol. 2019, 10, 1127. [Google Scholar] [CrossRef]
- Abdelmoula, A.; Baudry, S.; Duchateau, J. Anodal transcranial direct current stimulation enhances time to task failure of a submaximal contraction of elbow flexors without changing corticospinal excitability. Neuroscience 2016, 322, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Kan, B.; Dundas, J.E.; Nosaka, K. Effect of transcranial direct current stimulation on elbow flexor maximal voluntary isometric strength and endurance. Appl. Physiol. Nutr. Metab. 2013, 38, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Cogiamanian, F.; Marceglia, S.; Ardolino, G.; Barbieri, S.; Priori, A. Improved isometric force endurance after transcranial direct current stimulation over the human motor cortical areas. Eur. J. Neurosci. 2007, 26, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Hazime, F.A.; da Cunha, R.A.; Soliaman, R.R.; Romancini, A.C.B.; de Pochini, A.C.; Ejnisman, B.; Baptista, A.F. Anodal transcranial direct current stimulation (tDCS) increases isometric strength of shoulder rotators muscles in handball players. Int. J. Sports Phys. Ther. 2017, 12, 402–407. [Google Scholar]
- Vargas, V.Z.; Baptista, A.F.; Pereira, G.O.C.; Pochini, A.C.; Ejnisman, B.; Santos, M.B.; João, S.M.A.; Hazime, F.A. Modulation of isometric quadriceps strength in soccer players with transcranial direct current stimulation: A crossover study. J. Strength Cond. Res. 2018, 32, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Hanakawa, T.; Honda, M.; Watanabe, K. Enhancement of pinch force in the lower leg by anodal transcranial direct current stimulation. Exp. Brain Res. 2009, 196, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Vaseghi, B.; Zoghi, M.; Jaberzadeh, S. Unihemispheric concurrent dual-site cathodal transcranial direct current stimulation: The effects on corticospinal excitability. Eur. J. Neurosci. 2016, 43, 1161–1172. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | |
|---|---|
| Age: mean (range) | 21.92 (18–29) |
| Sex | |
| Number of men (%) | 51 (56.7) |
| Number of women (%) | 39 (43.3) |
| Height (m) | 1.70 ± 0.08 |
| Weight (kg) | 66.16 ± 10.27 |
| Body mass index (kg/m2): mean | 22.68 ± 1.90 |
| Smoking | |
| Number of cigarettes | 1.83 ± 7.72 |
| Pressure pain threshold (kg/cm2) | |
| PPT_Finger | 7.12 ± 2.16 |
| PPT_Trapezius | 2.53 ± 2.27 |
| PPT_Tibial muscle | 7.49 ± 2.92 |
| Mechanical hyperalgesia (kg/cm2) | 19.15 ± 6.46 |
| Tolerance threshold (kg/cm2) | 12.41 ± 1.68 |
| Hand grip strength (kg) | 35.66 ± 15.48 |
| Cold hyperalgesia 1 | 35.15 ± 19.06 |
| CPM (Δkg/cm2) | 1.87 ± 1.31 |
| Temporal summation 1 | 9.64 ± 13.59 |
| ULNT1 (degrees) | 135.57 ± 34.91 |
| STAI-S (0–60) | 10.70 ± 9.35 |
| STAI -T (0–69) | 22.97 ± 9.85 |
| BDI-II (0–63) | 4.13 ± 6.24 |
| PCS (0–52) | 6.63 ± 6.49 |
| TSK (11–44) | 17.20 ± 5.46 |
| PSQI (0–21) | 3.72 ± 2.34 |
| FPQIII (30–150) | 57.83 ± 16.23 |
| IPAQ-SF (METS) | 3835.43 ± 2332.67 |
| Placebo | M1-tDCS | UHCDS-tDCS | p-Values | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Time | Group | |
| PPT | ||||||||
| Finger | 7.04 ± 2.15 | 7.16 ± 2.07 | 7.01 ± 1.95 | 7.03 ± 1.68 | 7.32 ± 2.41 | 7.42 ± 2.44 | 0.58 | 0.95 |
| Trapezius | 4.65 ± 2.52 | 4.86 ± 2.69 | 4.34 ± 1.67 | 4.53 ± 1.78 | 4.61 ± 2.57 | 4.79 ± 2.43 | <0.05 * | 0.99 |
| Tibial muscle | 7.73 ± 3.02 | 8.30 ± 3.17 | 7.10 ± 2.43 | 8.04 ± 2.98 | 7.63 ± 3.30 | 7.96 ± 2.96 | <0.05 * | 0.25 |
| Mechanical hyperalgesia | 19.44 ± 6.74 | 20.32 ± 7.21 | 18.45 ± 5.26 | 19.61 ± 5.67 | 19.57 ± 7.37 | 20.18 ± 7.03 | <0.05 * | 0.76 |
| Tolerance threshold | 12.44 ± 1.59 | 12.67 ± 1.51 | 12.42 ± 1.84 | 12.54 ± 1.75 | 12.37 ± 1.65 | 12.21 ± 1.69 | 0.58 | 0.38 |
| Hand grip strength | 36.29 ± 15.51 | 36.39 ± 15.23 | 33.95 ± 17.79 | 34.85 ± 18.32 | 36.71 ± 13.20 | 37.56 ± 13.67 | <0.05 * | 0.44 |
| Cold hyperalgesia | 35.75 ± 21.54 | 31.86 ± 21.25 | 36.67 ± 18.13 | 31.06 ± 19.09 | 33.02 ± 17.68 | 32.11 ± 18.59 | <0.05 * | 0.17 |
| CPM | 1.62 ± 1.32 | 2.28 ± 1.58 | 2.26 ± 1.38 | 2.20 ± 1.71 | 1.75 ± 1.18 | 2.05 ± 1.09 | 0.06 | 0.18 |
| Temporal Summation | 8.37 ± 10.32 | 10.40 ± 13.28 | 12.00 ± 16.78 | 9.41 ± 13.35 | 9.23 ± 13.05 | 10.03 ± 12.92 | 0.95 | 0.35 |
| ULNT1 | 137.07 ± 33.71 | 143.93 ± 30.75 | 133.63 ± 34.31 | 143.97 ± 34.1 | 136.00 ± 37.68 | 141.24 ± 32.94 | <0.05 * | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gurdiel-Álvarez, F.; González-Zamorano, Y.; Lerma Lara, S.; Gómez-Soriano, J.; Taylor, J.; Romero, J.P.; Gómez Jiménez, M.; Fernández-Carnero, J. Effectiveness of Unihemispheric Concurrent Dual-Site Stimulation over M1 and Dorsolateral Prefrontal Cortex Stimulation on Pain Processing: A Triple Blind Cross-Over Control Trial. Brain Sci. 2021, 11, 188. https://doi.org/10.3390/brainsci11020188
Gurdiel-Álvarez F, González-Zamorano Y, Lerma Lara S, Gómez-Soriano J, Taylor J, Romero JP, Gómez Jiménez M, Fernández-Carnero J. Effectiveness of Unihemispheric Concurrent Dual-Site Stimulation over M1 and Dorsolateral Prefrontal Cortex Stimulation on Pain Processing: A Triple Blind Cross-Over Control Trial. Brain Sciences. 2021; 11(2):188. https://doi.org/10.3390/brainsci11020188
Chicago/Turabian StyleGurdiel-Álvarez, Francisco, Yeray González-Zamorano, Sergio Lerma Lara, Julio Gómez-Soriano, Julian Taylor, Juan Pablo Romero, María Gómez Jiménez, and Josué Fernández-Carnero. 2021. "Effectiveness of Unihemispheric Concurrent Dual-Site Stimulation over M1 and Dorsolateral Prefrontal Cortex Stimulation on Pain Processing: A Triple Blind Cross-Over Control Trial" Brain Sciences 11, no. 2: 188. https://doi.org/10.3390/brainsci11020188
APA StyleGurdiel-Álvarez, F., González-Zamorano, Y., Lerma Lara, S., Gómez-Soriano, J., Taylor, J., Romero, J. P., Gómez Jiménez, M., & Fernández-Carnero, J. (2021). Effectiveness of Unihemispheric Concurrent Dual-Site Stimulation over M1 and Dorsolateral Prefrontal Cortex Stimulation on Pain Processing: A Triple Blind Cross-Over Control Trial. Brain Sciences, 11(2), 188. https://doi.org/10.3390/brainsci11020188