
Regional Gray Matter Volume Changes in Parkinson’s Disease with Orthostatic Hypotension


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Autonomic Function Tests
2.3. MRI Acquisition and Voxel-Based Morphometry Analysis
2.4. Statistical Analysis
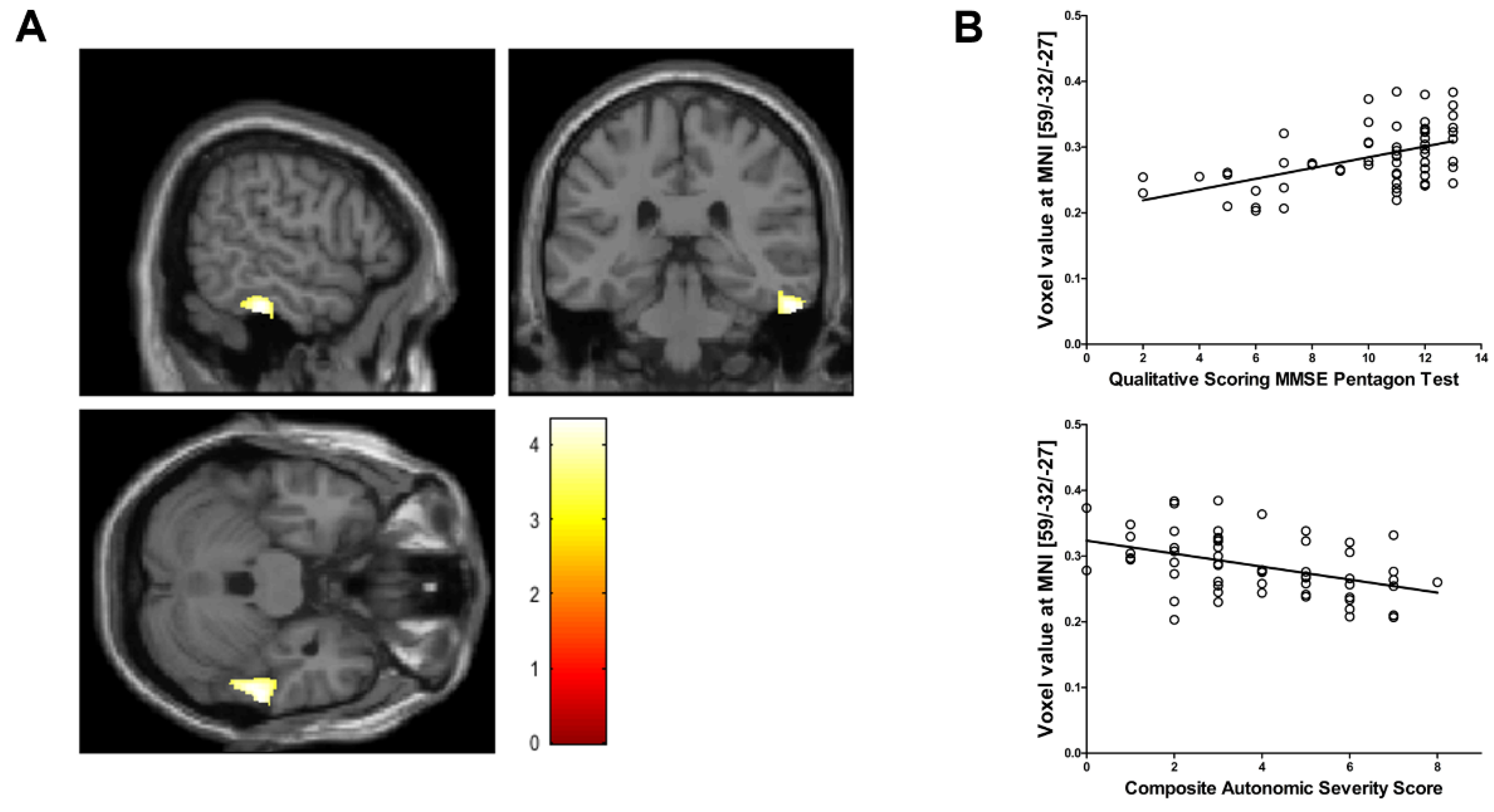
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Merola, A.; Romagnolo, A.; Rosso, M.; Suri, R.; Berndt, Z.; Maule, S.; Lopiano, L.; Espay, A.J. Autonomic dysfunction in Parkinson’s disease: A prospective cohort study. Mov. Disord. 2018, 33, 391–397. [Google Scholar] [CrossRef]
- Velseboer, D.C.; De Haan, R.J.; Wieling, W.; Goldstein, D.S.; De Bie, R.M. Prevalence of orthostatic hypotension in Parkinson’s disease: A systematic review and meta-analysis. Parkinsonism Relat. Disord. 2011, 17, 724–729. [Google Scholar] [CrossRef] [Green Version]
- Low, P.A.; Tomalia, V.A. Orthostatic Hypotension: Mechanisms, Causes, Management. J. Clin. Neurol. 2015, 11, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, K.; Takahashi, H. Neuropathology of autonomic nervous system in Parkinson’s disease. Eur. Neurol. 1997, 38 (Suppl. 2), 2–7. [Google Scholar] [CrossRef]
- Papapetropoulos, S.; Mash, D.C. Insular pathology in Parkinson’s disease patients with orthostatic hypotension. Parkinsonism Relat. Disord. 2007, 13, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Benarroch, E.E. The central autonomic network: Functional organization, dysfunction, and perspective. Mayo. Clin. Proc. 1993, 68, 988–1001. [Google Scholar] [CrossRef]
- McDonald, C.; Newton, J.L.; Burn, D.J. Orthostatic hypotension and cognitive impairment in Parkinson’s disease: Causation or association? Mov. Disord. 2016, 31, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Allcock, L.M.; Kenny, R.A.; Mosimann, U.P.; Tordoff, S.; Wesnes, K.A.; Hildreth, A.J.; Burn, D.J. Orthostatic hypotension in Parkinson’s disease: Association with cognitive decline? Int. J. Geriatr. Psychiatry 2006, 21, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Idiaquez, J.; Benarroch, E.E.; Rosales, H.; Milla, P.; Rios, L. Autonomic and cognitive dysfunction in Parkinson’s disease. Clin. Auton. Res. 2007, 17, 93–98. [Google Scholar] [CrossRef]
- Hohler, A.D.; Zuzuarregui, J.R.; Katz, D.I.; Depiero, T.J.; Hehl, C.L.; Leonard, A.; Allen, V.; Dentino, J.; Gardner, M.; Phenix, H.; et al. Differences in motor and cognitive function in patients with Parkinson’s disease with and without orthostatic hypotension. Int. J. Neurosci. 2012, 122, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Longardner, K.; Bayram, E.; Litvan, I. Orthostatic Hypotension Is Associated With Cognitive Decline in Parkinson Disease. Front. Neurol. 2020, 11, 897. [Google Scholar] [CrossRef]
- Postuma, R.B.; Gagnon, J.F.; Pelletier, A.; Montplaisir, J. Prodromal autonomic symptoms and signs in Parkinson’s disease and dementia with Lewy bodies. Mov. Disord. 2013, 28, 597–604. [Google Scholar] [CrossRef]
- Goldstein, D.S. Orthostatic hypotension as an early finding in Parkinson’s disease. Clin. Auton. Res. 2006, 16, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Matsui, H.; Udaka, F.; Miyoshi, T.; Hara, N.; Tamura, A.; Oda, M.; Kubori, T.; Nishinaka, K.; Kameyama, M. Three-dimensional stereotactic surface projection study of orthostatic hypotension and brain perfusion image in Parkinson’s disease. Acta. Neurol. Scand. 2005, 112, 36–41. [Google Scholar] [CrossRef]
- Robertson, A.D.; Messner, M.A.; Shirzadi, Z.; Kleiner-Fisman, G.; Lee, J.; Hopyan, J.; Lang, A.E.; Black, S.E.; MacIntosh, B.J.; Masellis, M. Orthostatic hypotension, cerebral hypoperfusion, and visuospatial deficits in Lewy body disorders. Parkinsonism Relat. Disord. 2016, 22, 80–86. [Google Scholar] [CrossRef]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caffarra, P.; Gardini, S.; Dieci, F.; Copelli, S.; Maset, L.; Concari, L.; Farina, E.; Grossi, E. The qualitative scoring MMSE pentagon test (QSPT): A new method for differentiating dementia with Lewy Body from Alzheimer’s disease. Behav. Neurol. 2013, 27, 213–220. [Google Scholar] [CrossRef]
- Freeman, R.; Wieling, W.; Axelrod, F.B.; Benditt, D.G.; Benarroch, E.; Biaggioni, I.; Cheshire, W.P.; Chelimsky, T.; Cortelli, P.; Gibbons, C.H.; et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin. Auton. Res. 2011, 21, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Low, P.A. Composite autonomic scoring scale for laboratory quantification of generalized autonomic failure. Mayo Clin. Proc. 1993, 68, 748–752. [Google Scholar] [CrossRef]
- Kim, J.B.; Kim, H.; Sung, J.H.; Baek, S.H.; Kim, B.J. Heart-Rate-Based Machine-Learning Algorithms for Screening Orthostatic Hypotension. J. Clin. Neurol. 2020, 16, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Seok, H.Y.; Kim, Y.H.; Kim, H.; Kim, B.J. Patterns of Orthostatic Blood Pressure Changes in Patients with Orthostatic Hypotension. J. Clin. Neurol. 2018, 14, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Ashburner, J. A fast diffeomorphic image registration algorithm. Neuroimage 2007, 38, 95–113. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Kim, J.H. Regional gray matter changes in shift workers: A voxel-based morphometry study. Sleep Med. 2017, 30, 185–188. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Miyashita, Y. Inferior temporal cortex: Where visual perception meets memory. Annu. Rev. Neurosci. 1993, 16, 245–263. [Google Scholar] [CrossRef]
- Woloszyn, L.; Sheinberg, D.L. Neural dynamics in inferior temporal cortex during a visual working memory task. J. Neurosci. 2009, 29, 5494–5507. [Google Scholar] [CrossRef] [Green Version]
- Udow, S.J.; Robertson, A.D.; MacIntosh, B.J.; Espay, A.J.; Rowe, J.B.; Lang, A.E.; Masellis, M. ‘Under pressure’: Is there a link between orthostatic hypotension and cognitive impairment in alpha-synucleinopathies? J. Neurol. Neurosurg. Psychiatry 2016, 87, 1311–1321. [Google Scholar] [CrossRef] [Green Version]
- Wood, S.J.; Ramsdell, C.D.; Mullen, T.J.; Oman, C.M.; Harm, D.L.; Paloski, W.H. Transient cardio-respiratory responses to visually induced tilt illusions. Brain Res. Bull. 2000, 53, 25–31. [Google Scholar] [CrossRef]
- Yoon, B.W.; Morillo, C.A.; Cechetto, D.F.; Hachinski, V. Cerebral hemispheric lateralization in cardiac autonomic control. Arch. Neurol. 1997, 54, 741–744. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Suh, S.I.; Seo, W.K.; Koh, S.B.; Kim, J.H. Right insular atrophy in neurocardiogenic syncope: A volumetric MRI study. AJNR Am. J. Neuroradiol. 2014, 35, 113–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| PD with OH (n = 25) | PD without OH (n = 35) | p Value | |
|---|---|---|---|
| Age, years | 75.8 ± 7.7 | 74.6 ± 4.0 | 0.489 |
| Male, n (%) a | 15 (60.0) | 17 (48.6) | 0.382 |
| Hypertension, n (%) a | 13 (52.0) | 18 (51.4) | 0.965 |
| H&Y stage | 2.3 ± 0.6 | 2.3 ± 0.6 | 0.676 |
| UPDRS part III | 27.8 ± 10.9 | 23.6 ± 9.3 | 0.108 |
| CASS | 5.1 ± 1.8 | 3.0 ± 1.7 | <0.001 |
| MMSE | 25.6 ± 2.9 | 24.6 ± 3.9 | 0.238 |
| QSPT | 8.96 ± 3.1 | 10.8 ± 2.5 | 0.012 |
| MoCA | 19.9 ± 4.9 | 19.6 ± 6.1 | 0.805 |
| Variables | β | p Value |
|---|---|---|
| Age | ‒0.001 | 0.164 |
| Male sex | ‒0.002 | 0.872 |
| H&Y | ‒0.008 | 0.421 |
| UPDRS part III | ‒0.002 | 0.003 |
| CASS | ‒0.010 | 0.001 |
| MMSE | 0.001 | 0.768 |
| QSPT | 0.008 | <0.001 |
| MoCA | 0.001 | 0.294 |
| Variables | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Age | NS | NS | NS |
| Male sex | NS | NS | NS |
| UPDRS part III | ‒0.357 ** | ‒0.285 * | NS |
| CASS | ‒0.374 ** | ‒0.284 * | |
| QSPT | 0.367 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.B.; Kim, H.; Lee, C.-N.; Park, K.-W.; Kim, B.-J. Regional Gray Matter Volume Changes in Parkinson’s Disease with Orthostatic Hypotension. Brain Sci. 2021, 11, 294. https://doi.org/10.3390/brainsci11030294
Kim JB, Kim H, Lee C-N, Park K-W, Kim B-J. Regional Gray Matter Volume Changes in Parkinson’s Disease with Orthostatic Hypotension. Brain Sciences. 2021; 11(3):294. https://doi.org/10.3390/brainsci11030294
Chicago/Turabian StyleKim, Jung Bin, Hayom Kim, Chan-Nyung Lee, Kun-Woo Park, and Byung-Jo Kim. 2021. "Regional Gray Matter Volume Changes in Parkinson’s Disease with Orthostatic Hypotension" Brain Sciences 11, no. 3: 294. https://doi.org/10.3390/brainsci11030294
APA StyleKim, J. B., Kim, H., Lee, C. -N., Park, K. -W., & Kim, B. -J. (2021). Regional Gray Matter Volume Changes in Parkinson’s Disease with Orthostatic Hypotension. Brain Sciences, 11(3), 294. https://doi.org/10.3390/brainsci11030294