
Effects of tDCS on Sound Duration in Patients with Apraxia of Speech in Primary Progressive Aphasia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Clinical Assessment
2.3. Speech Therapy Methods
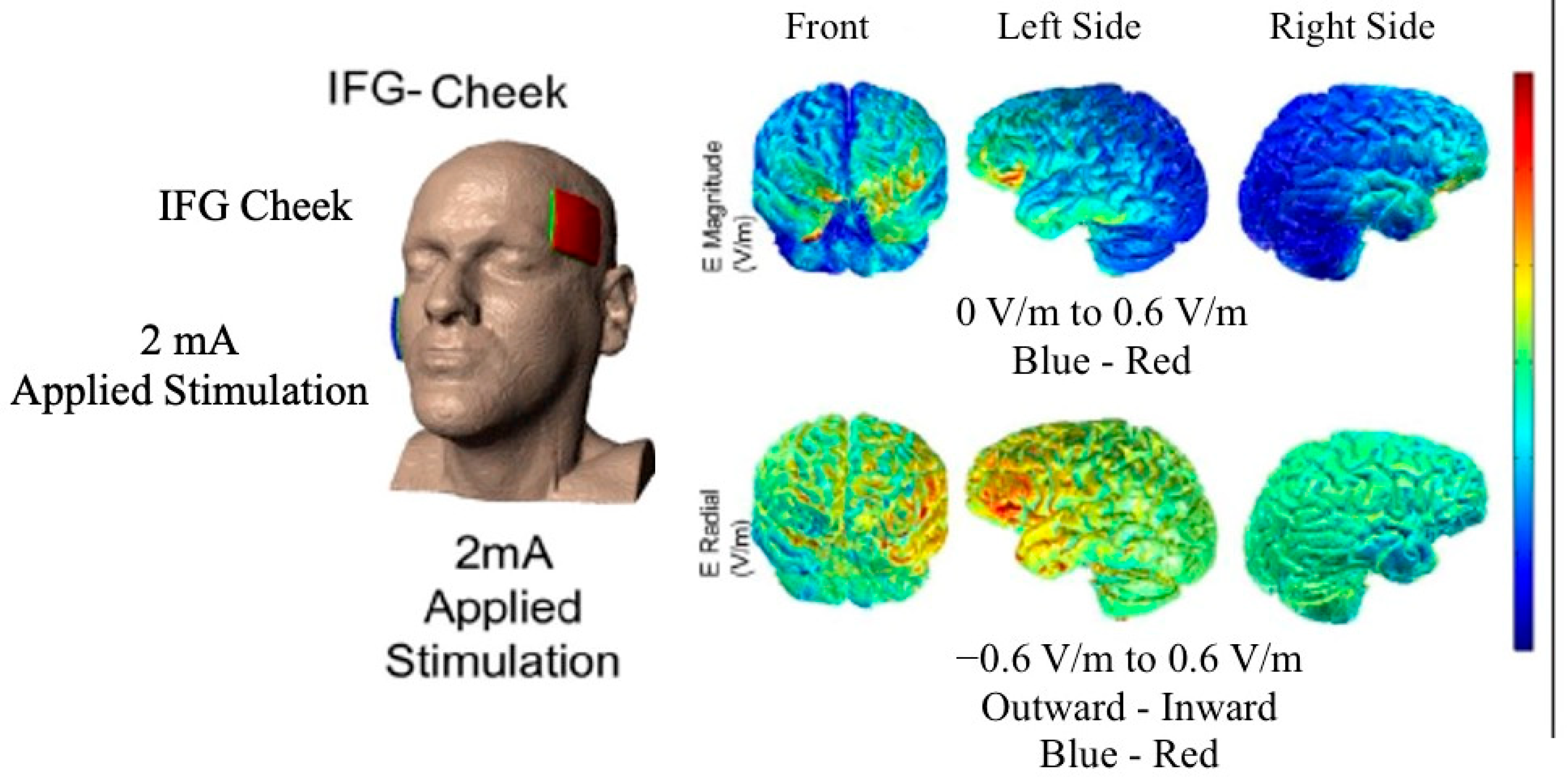
2.4. tDCS Methods
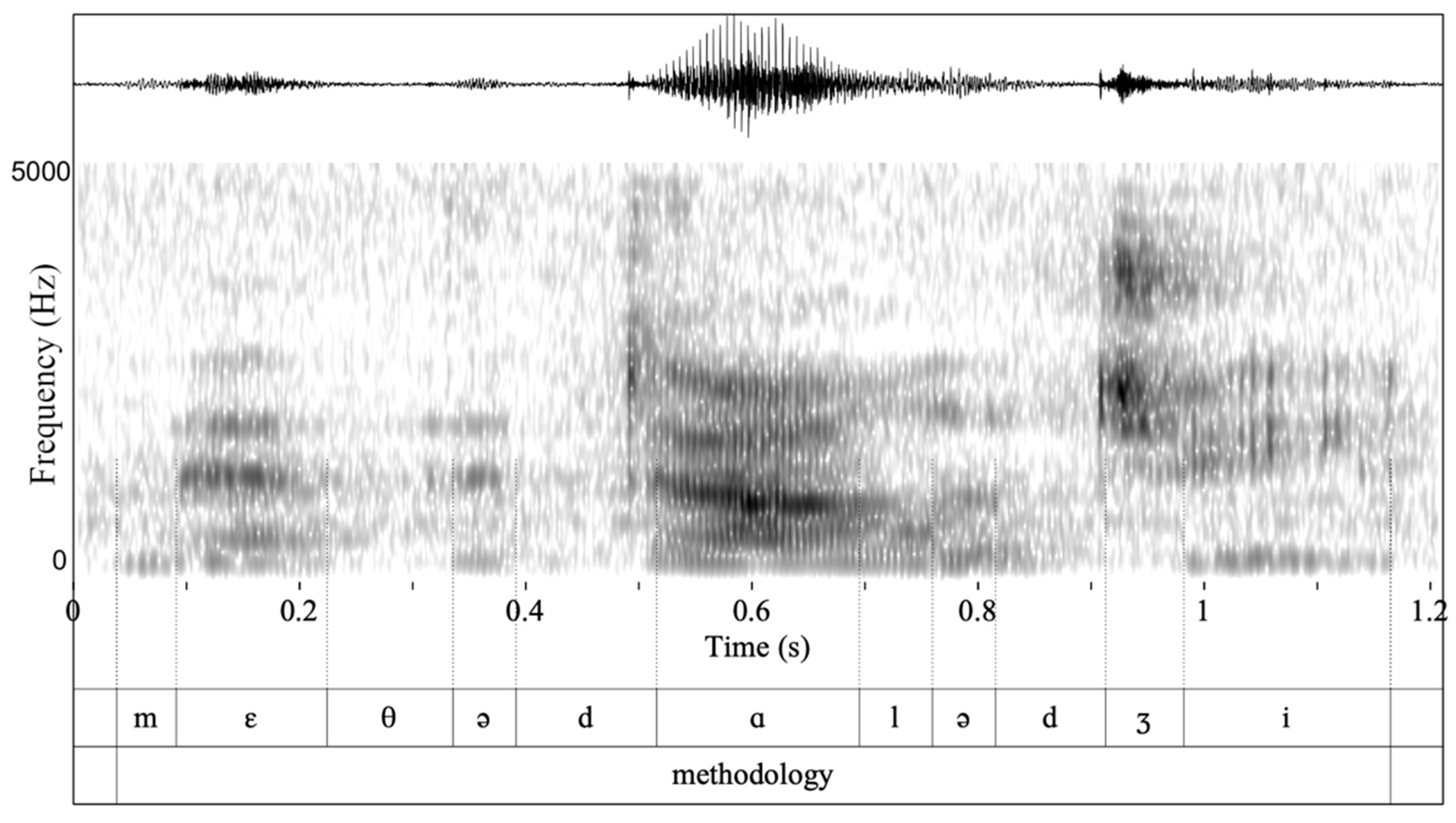
2.5. Acoustic Analysis
2.6. Statistical Analysis
3. Results
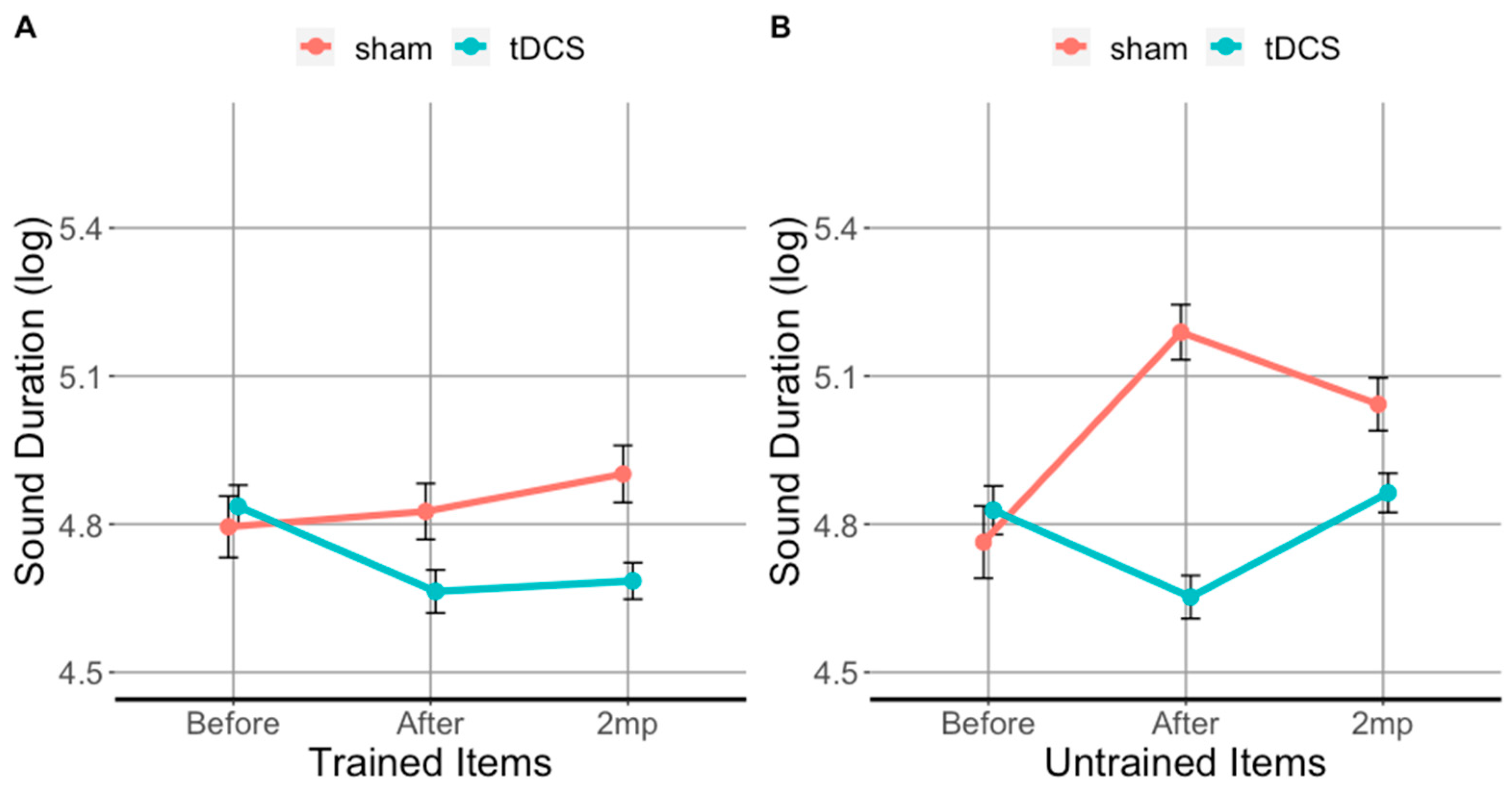
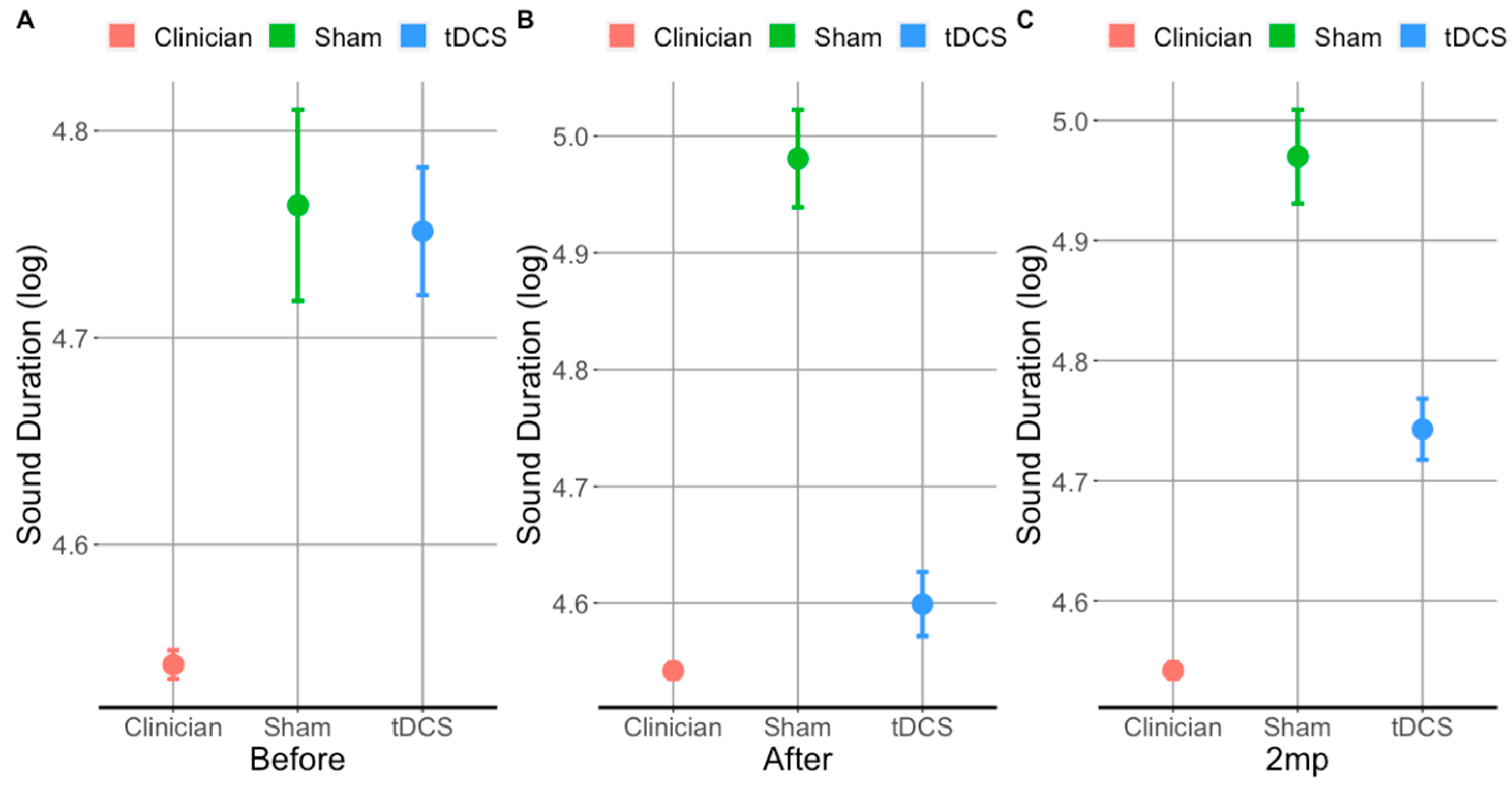
3.1. tDCS Effectiveness on Sound Duration in Trained Items
3.2. tDCS Effectiveness on Sound Duration in Untrained Items
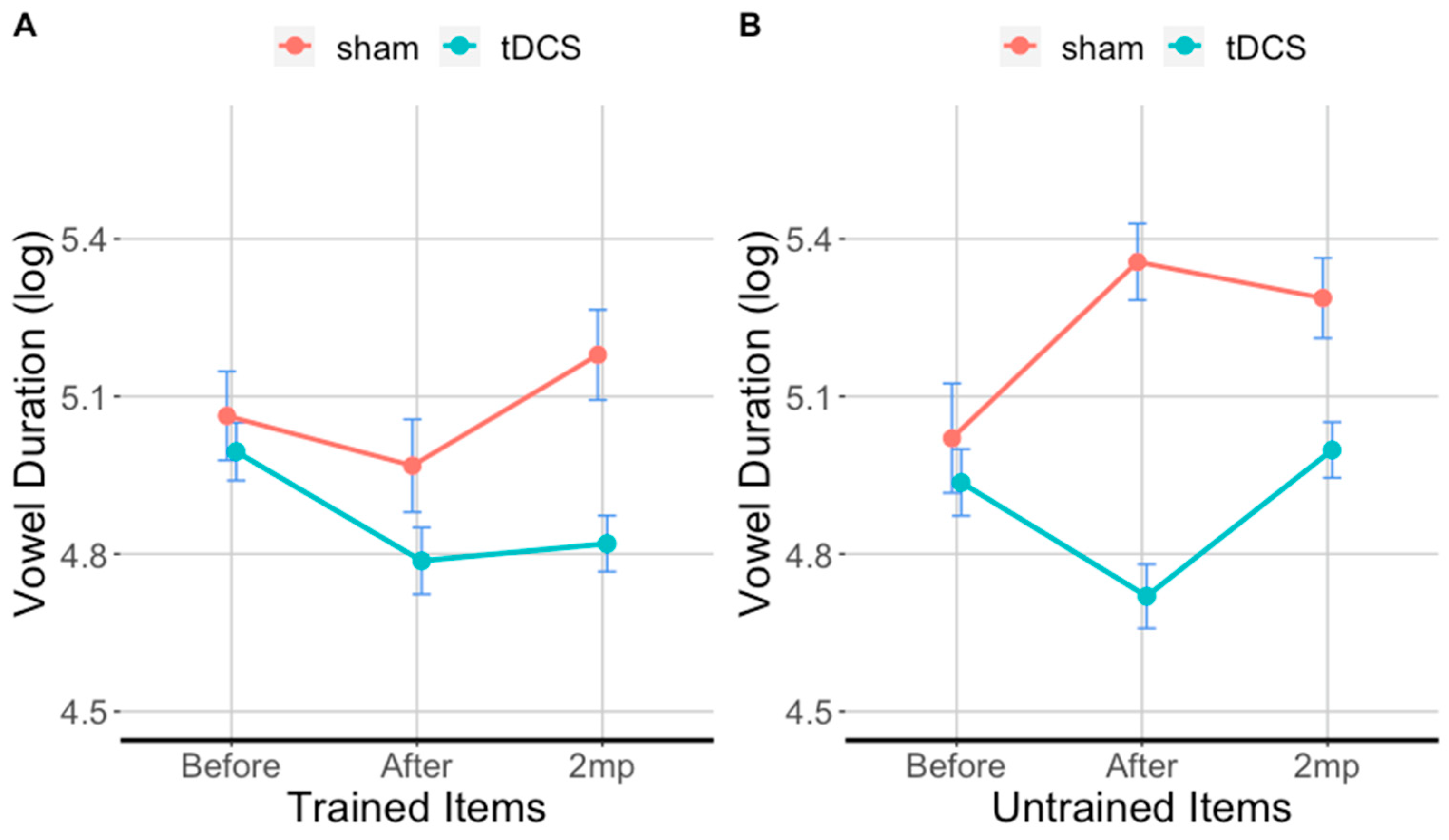
3.3. tDCS Effectiveness on Vowel Duration in Trained Items
3.4. tDCS Effectiveness on Vowel Duration in Untrained Items
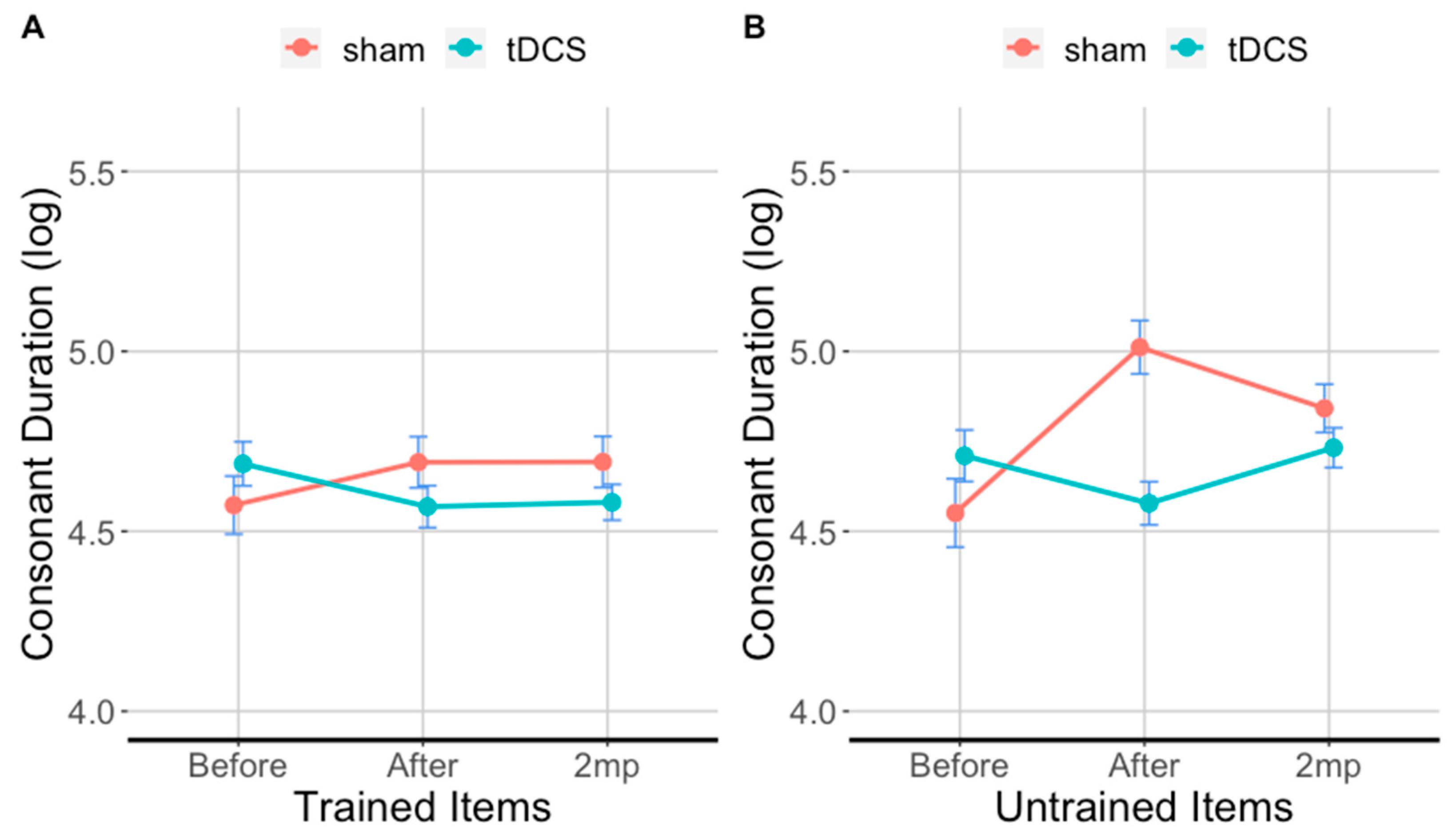
3.5. tDCS Effectiveness on Consonant Duration in Trained Items
3.6. tDCS Effectiveness on Consonant Duration in Untrained Items
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Set Lists | Word Triplets | ||
| SET 1 | intervene | intervention | interventional |
| progress | progression | progressive | |
| reflect | reflection | reflective | |
| stimulate | stimulation | stimulating | |
| stable | stabilize | stabilization | |
| success | successful | successfully | |
| excite | excitable | excitability | |
| improve | improvement | improving | |
| behave | behavioral | behaviorally | |
| perform | performance | performing | |
| SET 2 | enhance | enhancement | enhancing |
| suspend | suspension | suspending | |
| suppress | suppression | suppressive | |
| construct | construction | constructive | |
| accurate | accuracy | inaccurate | |
| therapy | therapeutic | therapeutically | |
| provide | provision | provisional | |
| hypothesis | hypothesize | hypothetical | |
| define | definition | definitive | |
| determine | determination | determining | |
| SET 3 | inform | information | informative |
| suppose | supposition | supposedly | |
| restrict | restriction | restrictive | |
| concentrate | concentration | concentrated | |
| inhibit | inhibition | inhibiting | |
| investigate | investigation | investigator | |
| combine | combination | combinatory | |
| cognition | cognitive | cognitively | |
| method | methodology | methodological | |
| courage | courageous | encouraging | |
Appendix B
References
- Ogar, J.; Willock, S.; Baldo, J.; Wilkins, D.; Ludy, C.; Dronkers, N. Clinical and anatomical correlates of apraxia of speech. Brain Lang. 2006, 97, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Jordan, L.C.; Hillis, A.E. Disorders of speech and language: Aphasia, apraxia and dysarthria. Curr Opin Neurol 2006, 19, 580–585. [Google Scholar] [CrossRef]
- Graff-Radford, J.; Jones, D.T.; Strand, E.A.; Rabinstein, A.A.; Duffy, J.R.; Josephs, K.A. The neuroanatomy of pure apraxia of speech in stroke. Brain Lang. 2014, 129, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Moser, D.; Basilakos, A.; Fillmore, P.; Fridriksson, J. Brain damage associated with apraxia of speech: Evidence from case studies. Neurocase 2016, 22, 346–356. [Google Scholar] [CrossRef]
- Rosenbek, J.C.; Lemme, M.L.; Ahern, M.B.; Harris, E.H.; Wertz, R.T. A treatment for apraxia of speech in adults. J. Speech Hear. Disord. 1973, 38, 462–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogar, J.; Slama, H.; Dronkers, N.; Amici, S.; Gorno-Tempini, M.L. Apraxia of speech: An overview. Neurocase 2005, 11, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Josephs, K.A.; Duffy, J.R. Apraxia of speech and nonfluent aphasia: A new clinical marker for corticobasal degeneration and progressive supranuclear palsy. Curr. Opin. Neurol. 2008, 21, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Laganaro, M.; Croisier, M.; Bagou, O.; Assal, F. Progressive apraxia of speech as a window into the study of speech planning processes. Cortex 2012, 48, 963–971. [Google Scholar] [CrossRef]
- Trupe, L.A.; Varma, D.D.; Gomez, Y.; Race, D.; Leigh, R.; Hillis, A.E.; Gottesman, R.F. Chronic apraxia of speech and Broca’s area. Stroke 2013, 44, 740–744. [Google Scholar] [CrossRef] [Green Version]
- Mesulam, M.M. Primary progressive aphasia—A language-based dementia. N. Engl. J. Med. 2003, 349, 1535–1542. [Google Scholar] [CrossRef]
- Grossman, M. Progressive aphasic syndromes: Clinical and theoretical advances. Curr. Opin. Neurol. 2002, 15, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Grossman, M. Primary progressive aphasia: Clinicopathological correlations. Nat. Rev. Neurol. 2010, 6, 88–97. [Google Scholar] [CrossRef] [Green Version]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, C.K.; Cho, S.; Hsu, C.J.; Wieneke, C.; Rademaker, A.; Weitner, B.B.; Mesulam, M.M.; Weintraub, S. Dissociations Between Fluency And Agrammatism In Primary Progressive Aphasia. Aphasiology 2012, 26, 20–43. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.R. Apraxia of speech in degenerative neurologic disease. Aphasiology 2006, 20, 511–527. [Google Scholar] [CrossRef]
- Duffy, J.R.; Strand, E.A.; Clark, H.; Machulda, M.; Whitwell, J.L.; Josephs, K.A. Primary progressive apraxia of speech: Clinical features and acoustic and neurologic correlates. Am. J. Speech Lang. Pathol. 2015, 24, 88–100. [Google Scholar] [CrossRef]
- Josephs, K.A.; Duffy, J.R.; Strand, E.A.; Whitwell, J.L.; Layton, K.F.; Parisi, J.E.; Hauser, M.F.; Witte, R.J.; Boeve, B.F.; Knopman, D.S.; et al. Clinicopathological and imaging correlates of progressive aphasia and apraxia of speech. Brain 2006, 129, 1385–1398. [Google Scholar] [CrossRef] [Green Version]
- Josephs, K.A.; Whitwell, J.L.; Duffy, J.R.; Vanvoorst, W.A.; Strand, E.A.; Hu, W.T.; Boeve, B.F.; Graff-Radford, N.R.; Parisi, J.E.; Knopman, D.S.; et al. Progressive aphasia secondary to Alzheimer disease vs FTLD pathology. Neurology 2008, 70, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Marangolo, P.; Marinelli, C.V.; Bonifazi, S.; Fiori, V.; Ceravolo, M.G.; Provinciali, L.; Tomaiuolo, F. Electrical stimulation over the left inferior frontal gyrus (IFG) determines long-term effects in the recovery of speech apraxia in three chronic aphasics. Behav. Brain Res. 2011, 225, 498–504. [Google Scholar] [CrossRef]
- Utianski, R.L.; Duffy, J.R.; Clark, H.M.; Strand, E.A.; Botha, H.; Schwarz, C.G.; Machulda, M.M.; Senjem, M.L.; Spychalla, A.J.; Jack, C.R., Jr.; et al. Prosodic and phonetic subtypes of primary progressive apraxia of speech. Brain Lan.g 2018, 184, 54–65. [Google Scholar] [CrossRef]
- Duffy, J.R.; Hanley, H.; Utianski, R.; Clark, H.; Strand, E.; Josephs, K.A.; Whitwell, J.L. Temporal acoustic measures distinguish primary progressive apraxia of speech from primary progressive aphasia. Brain Lang. 2017, 168, 84–94. [Google Scholar] [CrossRef]
- Themistocleous, C.; Ficek, B.; Webster, K.; den Ouden, D.-B.; Hillis, A.E.; Tsapkini, K. Automatic Subtyping of Individuals with Primary Progressive Aphasia. J. Alzheimer’s Dis. 2021, 79, 1185–1194. [Google Scholar] [CrossRef]
- Ballard, K.J.; Azizi, L.; Duffy, J.R.; McNeil, M.R.; Halaki, M.; O’Dwyer, N.; Layfield, C.; Scholl, D.I.; Vogel, A.P.; Robin, D.A. A predictive model for diagnosing stroke-related apraxia of speech. Neuropsychologia 2016, 81, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Basilakos, A. Towards Improving the Evaluation of Speech Production Deficits in Chronic Stroke; University of South Carolina: Los Angeles, CA, USA, 2016. [Google Scholar]
- Collins, M.; Rosenbek, J.C.; Wertz, R.T. Spectrographic analysis of vowel and word duration in apraxia of speech. J. Speech Hear. Res. 1983, 26, 224–230. [Google Scholar] [CrossRef]
- Kent, R.D.; Rosenbek, J.C. Acoustic patterns of apraxia of speech. J. Speech Hear. Res. 1983, 26, 231–249. [Google Scholar] [CrossRef]
- Hardcastle, W.J. Electropalatographic study of articulation disorders in verbal dyspraxia. In Phonetic Approaches to Speech Production in Aphasia and Related Disorders; Ryalls, J.H., Ed.; College-Hill Press: Boston, MA, USA, 1987; pp. 113–136. [Google Scholar]
- Itoh, M. Articulatory movements in apraxia of speech. In Apraxia of Speech: Physiology, Acoustics, Linguistics, Management; Ryalls, J.H., Ed.; College Hill: Boston, MA, USA, 1984; pp. 135–165. [Google Scholar]
- Itoh, M.; Sasanuma, S.; Tatsumi, I.F.; Murakami, S.; Fukusako, Y.; Suzuki, T. Voice onset time characteristics in apraxia of speech. Brain Lang. 1982, 17, 193–210. [Google Scholar] [CrossRef]
- Cunningham, K.T.; Haley, K.L.; Jacks, A. Speech sound distortions in aphasia and apraxia of speech: Reliability and diagnostic significance. Aphasiology 2016, 30, 396–413. [Google Scholar] [CrossRef]
- Varley, R.A.; Whiteside, S.P. Voicing in severe apraxia of speech: Perceptual and acoustic analysis of a single case. J. Neurolinguistics 1998, 11, 259–273. [Google Scholar] [CrossRef]
- Mauszycki, S.C.; Dromey, C.; Wambaugh, J.L. Variability in apraxia of speech: A perceptual, acoustic, and kinematic analysis of stop consonants. J. Med. Speech-Lang. Pathol. 2007, 15, 223–242. [Google Scholar]
- Haley, K.L. Temporal and spectral properties of voiceless fricatives in aphasia and apraxia of speech. Aphasiology 2002, 16, 595–607. [Google Scholar] [CrossRef]
- Haley, K.L.; Jacks, A. Word-level prosodic measures and the differential diagnosis of apraxia of speech. Clin. Linguist. Phon. 2019, 33, 479–495. [Google Scholar] [CrossRef]
- Hillis, A.E.; Work, M.; Barker, P.B.; Jacobs, M.A.; Breese, E.L.; Maurer, K. Re-examining the brain regions crucial for orchestrating speech articulation. Brain 2004, 127, 1479–1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogar, J.M.; Dronkers, N.F.; Brambati, S.M.; Miller, B.L.; Gorno-Tempini, M.L. Progressive nonfluent aphasia and its characteristic motor speech deficits. Alzheimer Dis. Assoc. Disord. 2007, 21, S23–S30. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.P.; Benson, D.F.; Stuss, D.T. Frontal lobes and language. Brain Lang. 1989, 37, 656–691. [Google Scholar] [CrossRef]
- Dronkers, N.F. A new brain region for coordinating speech articulation. Nature 1996, 384, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Saur, D.; Kreher, B.W.; Schnell, S.; Kummerer, D.; Kellmeyer, P.; Vry, M.S.; Weiller, C. Ventral and dorsal pathways for language. Proc. Natl. Acad. Sci.USA 2008, 105, 18035. [Google Scholar] [CrossRef] [Green Version]
- Hickok, G.; Poeppel, D. The cortical organization of speech processing. Nat. Rev. Neurosci. 2007, 8, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Peach, R.K.; Tonkovich, J.D. Phonemic characteristics of apraxia of speech resulting from subcortical hemorrhage. J. Commun. Disord. 2004, 37, 77–90. [Google Scholar] [CrossRef]
- Henry, M.L.; Meese, M.V.; Truong, S.; Babiak, M.C.; Miller, B.L.; Gorno-Tempini, M.L. Treatment for apraxia of speech in nonfluent variant primary progressive aphasia. Behav. Neurol. 2013, 26, 77–88. [Google Scholar] [CrossRef]
- Harris, A.D.; Wang, Z.; Ficek, B.; Webster, K.; Edden, R.A.E.; Tsapkini, K. Reductions in GABA following a tDCS-language intervention for primary progressive aphasia. Neurobiol. Aging 2019, 79, 75–82. [Google Scholar] [CrossRef]
- Antonenko, D.; Schubert, F.; Bohm, F.; Ittermann, B.; Aydin, S.; Hayek, D.; Grittner, U.; Fl√∂el, A. tDCS-Induced Modulation of GABA Levels and Resting-State Functional Connectivity in Older Adults. J. Neurosci. Off. J. Soc. Neurosci. 2017, 37, 4065–4073. [Google Scholar] [CrossRef]
- Stagg, C.J.; Nitsche, M.A. Physiological basis of transcranial direct current stimulation. Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2011, 17, 37–53. [Google Scholar] [CrossRef]
- Ficek, B.N.; Wang, Z.; Zhao, Y.; Webster, K.T.; Desmond, J.E.; Hillis, A.E.; Frangakis, C.; Faria, A.V.; Caffo, B.; Tsapkini, K. The effect of tDCS on functional connectivity in primary progressive aphasia. Neuroimage Clin. 2018. [Google Scholar] [CrossRef]
- Chesters, J.; Watkins, K.E.; Möttönen, R. Investigating the feasibility of using transcranial direct current stimulation to enhance fluency in people who stutter. Brain Lang. 2017, 164, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Chesters, J.; Mottonen, R.; Watkins, K.E. Transcranial direct current stimulation over left inferior frontal cortex improves speech fluency in adults who stutter. Brain 2018, 141, 1161–1171. [Google Scholar] [CrossRef]
- Buchwald, A.; Calhoun, H.; Rimikis, S.; Lowe, M.S.; Wellner, R.; Edwards, D.J. Using tDCS to facilitate motor learning in speech production: The role of timing. Cortex 2019, 111, 274–285. [Google Scholar] [CrossRef]
- Tsapkini, K.; Frangakis, C.; Davis, C.; Gomez, Y.; Chakravarty, T.; Hillis, A. Spelling rehabilitation using transcranial direct current (tDCS) in primary progressive aphasia (PPA). Front. Psychol. 2014, 5, 1. [Google Scholar]
- Tsapkini, K.; Frangakis, C.; Gomez, Y.; Davis, C.; Hillis, A.E. Augmentation of spelling therapy with transcranial direct current stimulation in primary progressive aphasia: Preliminary results and challenges. Aphasiology 2014, 28, 1112–1130. [Google Scholar] [CrossRef] [Green Version]
- de Aguiar, V.; Zhao, Y.; Ficek, B.N.; Webster, K.; Rofes, A.; Wendt, H.; Frangakis, C.; Caffo, B.; Hillis, A.E.; Rapp, B.; et al. Cognitive and language performance predicts effects of spelling intervention and tDCS in Primary Progressive Aphasia. Cortex 2020, 124, 66–84. [Google Scholar] [CrossRef]
- Tsapkini, K.; Webster, K.T.; Ficek, B.N.; Desmond, J.E.; Onyike, C.U.; Rapp, B.; Frangakis, C.E.; Hillis, A.E. Electrical brain stimulation in different variants of primary progressive aphasia: A randomized clinical trial. Alzheimers Dement. 2018, 4, 461–472. [Google Scholar] [CrossRef]
- Roncero, C.; Kniefel, H.; Service, E.; Thiel, A.; Probst, S.; Chertkow, H. Inferior parietal transcranial direct current stimulation with training improves cognition in anomic Alzheimer’s disease and frontotemporal dementia. Alzheimers Dement. 2017, 3, 247–253. [Google Scholar] [CrossRef] [PubMed]
- McConathey, E.M.; White, N.C.; Gervits, F.; Ash, S.; Coslett, H.B.; Grossman, M.; Hamilton, R.H. Baseline Performance Predicts tDCS-Mediated Improvements in Language Symptoms in Primary Progressive Aphasia. Front. Hum. Neurosci. 2017, 11, 347. [Google Scholar] [CrossRef]
- Byrd, D.; Saltzman, E. The elastic phrase: Modeling the dynamics of boundary-adjacent lengthening. J. Phon. 2003, 31, 149–180. [Google Scholar] [CrossRef]
- Themistocleous, C. Edge-Tone Effects and Prosodic Domain Effects on Final Lengthening. Linguist. Var. 2014, 14, 129–160. [Google Scholar] [CrossRef] [Green Version]
- Howard, D.; Patterson, K. The Pyramid and Palm Trees Test: A Test of Semantic Access from Words and Pictures; Thames Valley Test Company: Bury St. Edmunds, UK, 1992. [Google Scholar]
- Kaplan, E.; Goodglass, H.; Weintraub, S. Boston Naming Test; Pro-Ed: Austin, TX, USA, 2001. [Google Scholar]
- Love, T.; Oster, E. On the categorization of aphasic typologies: The SOAP (a test of syntactic complexity). J. Psycholinguist Res. 2002, 31, 503–529. [Google Scholar] [CrossRef]
- Spreen, O.; Benton, A.L. Neurosensory Center Comprehensive Examination for Aphasia: Manual of Directions, Revised Edition; Department of Psychology, University of Victoria: Vicotria, BC, Canada, 1977. [Google Scholar]
- Knopman, D.S.; Kramer, J.H.; Boeve, B.F.; Caselli, R.J.; Graff-Radford, N.R.; Mendez, M.F.; Miller, B.L.; Mercaldo, N. Development of methodology for conducting clinical trials in frontotemporal lobar degeneration. Brain 2008, 131, 2957–2968. [Google Scholar] [CrossRef] [Green Version]
- Dabul, B. ABA-2: Apraxia Battery for Adults: Examiner’s Manual; Pro-Ed: Austin, TX, USA, 2000. [Google Scholar]
- Unal, G.; Ficek, B.; Webster, K.; Shahabuddin, S.; Truong, D.; Hampstead, B.; Bikson, M.; Tsapkini, K. Impact of brain atrophy on tDCS and HD-tDCS current flow: A modeling study in three variants of primary progressive aphasia. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 1781–1789. [Google Scholar] [CrossRef]
- de Aguiar, V.; Zhao, Y.; Faria, A.; Ficek, B.; Webster, K.T.; Wendt, H.; Wang, Z.; Hillis, A.E.; Onyike, C.U.; Frangakis, C.; et al. Brain volumes as predictors of tDCS effects in primary progressive aphasia. Brain Lang. 2020, 200, 104707. [Google Scholar] [CrossRef]
- Senn, S. Cross-Over Trials in Clinical Research, 2nd ed.; John Wiley & Sons, Ltd.: New York, NY, USA, 2002. [Google Scholar]
- Purcell, J.J.; Turkeltaub, P.E.; Eden, G.F.; Rapp, B. Examining the central and peripheral processes of written word production through meta-analysis. Front. Psychol. 2011, 2, 239. [Google Scholar] [CrossRef] [Green Version]
- Price, C.J. A review and synthesis of the first 20years of PET and fMRI studies of heard speech, spoken language and reading. NeuroImage 2012, 62, 816–847. [Google Scholar] [CrossRef] [Green Version]
- Homan, R.W.; Herman, J.; Purdy, P. Cerebral location of international 10-20 system electrode placement. Electroencephalogr. Clin. Neurophysiol. 1987, 66, 376–382. [Google Scholar] [CrossRef]
- Gandiga, P.C.; Hummel, F.C.; Cohen, L.G. Transcranial DC stimulation (tDCS): A tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol 2006, 117, 845–850. [Google Scholar] [CrossRef]
- Peterson, G.E.; Lehiste, I. Duration of Syllable Nuclei in English. J. Acoust. Soc. Am. 1960, 32, 693–703. [Google Scholar] [CrossRef]
- Themistocleous, C. The Nature of Phonetic Gradience across a Dialect Continuum: Evidence from Modern Greek Vowels. Phonetica 2017, 74, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Themistocleous, C. Dialect classification using vowel acoustic parameters. Speech Commun. 2017, 92, 13–22. [Google Scholar] [CrossRef]
- Themistocleous, C.; Savva, A.; Aristodemou, A. Effects of stress on fricatives: Evidence from Standard Modern Greek. In Proceedings of the Interspeech 2016, San Francisco, CA, USA, 8–12 September 2016; pp. 1–4. [Google Scholar]
- Themistocleous, C. Dialect Classification From a Single Sonorant Sound Using Deep Neural Networks. Front. Commun. 2019, 4, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Themistocleous, C. The bursts of stops can convey dialectal information. J. Acoust. Soc. Am. 2016, 140, EL334–EL339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boersma, P.; Weenink, D. Praat: Doing Phonetics by Computer (Version 6.0.37); University of Amsterdam: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Baayen, R.H. Analyzing Linguistic Data: A Practical Introduction to Statistics Using R; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- Schielzeth, H.; Dingemanse, N.J.; Nakagawa, S.; Westneat, D.F.; Allegue, H.; Teplitsky, C.; Réale, D.; Dochtermann, N.A.; Garamszegi, L.Z.; Araya-Ajoy, Y.G. Robustness of linear mixed-effects models to violations of distributional assumptions. Methods Ecol. Evol. 2020, 11, 1141–1152. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Bruun Brockhoff, P.; Haubo Bojesen Christensen, R. lmerTest: Tests in Linear Mixed Effects Models; R Foundation for Statistical Computing: Vienna, Austria, 2016. [Google Scholar]
- Russell, L. emmeans: Estimated Marginal Means, aka Least-Squares Means; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Margulies, D.S.; Petrides, M. Distinct parietal and temporal connectivity profiles of ventrolateral frontal areas involved in language production. J. Neurosci 2013, 33, 16846–16852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Wu, D.; Cheng, Y.; Song, W.; Yuan, Y.; Zhang, X.; Zhang, D.; Zhang, T.; Wang, Z.; Tang, J.; et al. Effects of Transcranial Direct Current Stimulation on Apraxia of Speech and Cortical Activation in Patients With Stroke: A Randomized Sham-Controlled Study. Am. J. Speech-Lang. Pathol. 2019, 28, 1625–1637. [Google Scholar] [CrossRef]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [Green Version]
- Marangolo, P.; Fiori, V.; Cipollari, S.; Campana, S.; Razzano, C.; Paola, M.D.; Koch, G.; Caltagirone, C. Bihemispheric stimulation over left and right inferior frontal region enhances recovery from apraxia of speech in chronic aphasia. Eur. J. Neurosci. 2013, 38, 3370–3377. [Google Scholar] [CrossRef] [Green Version]
- Lehiste, I. Suprasegmentals; MIT Press: Cambridge, MA, USA, 1970. [Google Scholar]
- Ohala, J. The application of phonological universals in speech pathology. Speech Lang. 1980, 3, 75–97. [Google Scholar]
- Stevens, K.N. Acoustic Phonetics; MIT Press: Cambridge, MA, USA, 1998. [Google Scholar]
- Fant, G. Acoustic Theory of Speech Production. Slav. East. Eur. J. 1960, 5, 285. [Google Scholar] [CrossRef]
- Themistocleous, C. Seeking an Anchorage. Stability and Variability in Tonal Alignment of Rising Prenuclear Pitch Accents in Cypriot Greek. Lang. Speech 2016, 59, 433–461. [Google Scholar] [CrossRef]
- Pierrehumbert, J. Phonology and Phonetics of English Intonation; Massachusetts Institute of Technology: Boston, MA, USA, 1980. [Google Scholar]
- Cruttenden, A. Gimson’s Pronunciation of English, 7th ed.; Hodder Education: London, UK, 2008. [Google Scholar]
- Levelt, W.J.M. Speaking: From Intention to Articulation; MIT Press: Cambridge, MA, USA, 1993. [Google Scholar]
- Kelso, J.A.; Tuller, B. Toward a theory of apractic syndromes. Brain Lang. 1981, 12, 224–245. [Google Scholar] [CrossRef]
- Whiteside, S.P.; Varley, R.A. A reconceptualisation of apraxia of speech: A synthesis of evidence. Cortex 1998, 34, 221–231. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sham | tDCS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Participant | ABN | DAN | JJI | Mean | BIN | DRY | GSH | JBN | CDY | Mean | p |
| Education | 16 | 16 | 16 | 16 (0) | 16 | 16 | 20 | 20 | 16 | 18 (2.30) | 0.2 |
| Gender | F | F | M | - | M | F | M | M | F | - | |
| Condition onset (years) | 4 | 2.5 | 1.5 | 2.7 (1.3) | 3 | 3.5 | 6 | 2 | 4 | 3.7 (1.48) | 0.2 |
| Age at start of Therapy | 54 | 71 | 78 | 67.67 (5.27) | 65 | 53 | 68 | 65 | 74 | 65 (7.64) | 0.5 |
| FTD-CDR Language Severity | 2 | 1 | 2 | 1.67(0.58) | 1 | 0.5 | 2 | 0.5 | 1 | 1(0.6) | 0.2 |
| FTD-CDR Total Severity | 4 | 4.5 | 5.5 | 4.67 (0.54) | 2 | 0.5 | 2.5 | 1 | 1.5 | 1.5 (0.79) | 0.03 * |
| F.A.S. | 6 | 11 | 4 | 7 (3.51) | 21 | 34 | 21 | 31 | 15 | 24.4 (7.86) | 0.02 * |
| Fruits, Animals, Vegetables | 38 | 11 | 10 | 19.67 (5.32) | 33 | 54 | 33 | 42 | 28 | 38 (10.27) | 0.2 |
| Digit Span Forward | 3.5 | 4 | 3.5 | 3.67 (0.25) | 4.5 | 5.5 | 3.5 | 6 | 7 | 5.3 (1.35) | 0.09 |
| Digit Span Backward | 2 | 3.5 | 2.5 | 2.67 (0.54) | 4.5 | 5 | 3.5 | 3 | 5.5 | 4.3 (1.04) | 0.07 |
| Pyramids and Palm Trees | 15 | 15 | 15 | 15 (0) | 15 | 15 | 15 | 15 | 15 | 15 (0) | 1 |
| BNT (30) | 28 | 28 | 15 | 23.67 (6.62) | 29 | 30 | 24 | 30 | 23 | 27 (3.4) | 0.3 |
| SOAP Total (40) | 30 | 33 | 27 | 30 (4.24) | 35 | 37 | 35 | 33 | 37 | 35 (1.7) | 0.03 * |
| Estimate | SE | df | t | p | ||
|---|---|---|---|---|---|---|
| A. Trained Items | Intercept | 4.7955 | 0.1657 | 6.1702 | 28.95 | <0.0001 |
| tDCS vs. sham After | −0.3194 | 0.0493 | 4900.5593 | −6.48 | <0.0001 | |
| tDCS vs. sham at 2 m post | −0.2559 | 0.0468 | 4899.0188 | −5.47 | <0.0001 | |
| B. Untrained Items | Intercept | 4.7427 | 0.1838 | 6.12 | 25.81 | 0009 |
| tDCS vs. sham After | −0.59 | 0.0539 | 4118.06 | −11.02 | <0.0001 | |
| tDCS vs. sham at 2 m post | −0.26 | 0.0495 | 4113.87 | −5.19 | <0.0001 |
| Estimate | SE | df | t | p | ||
|---|---|---|---|---|---|---|
| A. Trained Items | Intercept | 5.0919 | 0.1728 | 6.3419 | 29.47 | <0.0001 |
| tDCS in the After timepoint | −0.2434 | 0.0687 | 2043.0476 | −3.54 | 0004 | |
| tDCS in the 2 mp timepoint | −0.2820 | 0.0657 | 2041.6251 | −4.29 | <0.0001 | |
| B. Untrained Items | Intercept | 5.0122 | 0.1740 | 6.3172 | 28.81 | <0.0001 |
| tDCS in the After timepoint | −0.6013 | 0.0738 | 1802.2565 | −8.15 | <0.0001 | |
| tDCS in the 2 mp timepoint | −0.2455 | 0.0670 | 1797.7502 | −3.66 | 0002 |
| Estimate | SE | df | t | p | ||
|---|---|---|---|---|---|---|
| A. Trained Items | Intercept | 4.5697 | 0.1647 | 6.2897 | 27.75 | <0.0001 |
| tDCS in the After timepoint | −0.3307 | 0.0647 | 2804.4270 | −5.11 | <0.0001 | |
| tDCS in the 2 mp timepoint | −0.2239 | 0.0613 | 2803.4093 | −3.65 | 0.00027 | |
| B. Untrained Items | Intercept | 4.5255 | 0.1897 | 6.1737 | 23.85 | <0.0001 |
| tDCS in the After timepoint | −0.5427 | 0.0726 | 2259.5804 | −7.48 | <0.0001 | |
| tDCS in the 2 mp timepoint | −0.2540 | 0.0668 | 2255.8899 | −3.80 | 0.00015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Themistocleous, C.; Webster, K.; Tsapkini, K. Effects of tDCS on Sound Duration in Patients with Apraxia of Speech in Primary Progressive Aphasia. Brain Sci. 2021, 11, 335. https://doi.org/10.3390/brainsci11030335
Themistocleous C, Webster K, Tsapkini K. Effects of tDCS on Sound Duration in Patients with Apraxia of Speech in Primary Progressive Aphasia. Brain Sciences. 2021; 11(3):335. https://doi.org/10.3390/brainsci11030335
Chicago/Turabian StyleThemistocleous, Charalambos, Kimberly Webster, and Kyrana Tsapkini. 2021. "Effects of tDCS on Sound Duration in Patients with Apraxia of Speech in Primary Progressive Aphasia" Brain Sciences 11, no. 3: 335. https://doi.org/10.3390/brainsci11030335
APA StyleThemistocleous, C., Webster, K., & Tsapkini, K. (2021). Effects of tDCS on Sound Duration in Patients with Apraxia of Speech in Primary Progressive Aphasia. Brain Sciences, 11(3), 335. https://doi.org/10.3390/brainsci11030335