
Diffusion Kurtosis Imaging Fiber Tractography of Major White Matter Tracts in Neurosurgery

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Healthy Volunteers
2.2. Patients
2.3. MRI Data Acquisition
- T1-MPRAGE: repetition time (TR), 1900 ms; echo time (TE), 2.26 ms; inversion time (TI), 900 ms; field of view (FoV), 256 mm; matrix, 256 × 256; slice thickness (ST), 1 mm; flip angle, 9°; 176 slices; and parallel imaging (GRAPPA) with factor 2
- DWI: TR, 8500 ms; TE, 101 ms; FoV, 256 mm; matrix, 128 × 128; ST, 2 mm; distance factor, 0%; 60 slices; GRAPPA with factor 2; 30 diffusion encoding gradients; high b-values, 1000 and 2000 s/mm2; axial slices; phase encoding direction anterior >> posterior; resulting voxel size, 2 × 2 × 2 mm3
2.4. Data Preprocessing
2.5. Diffusion Tensor and Kurtosis Estimation
2.6. Whole-Brain Fiber Tractography
2.7. Seed Regions and Selection of White Matter Tracts
2.8. Statistical Analysis
3. Results
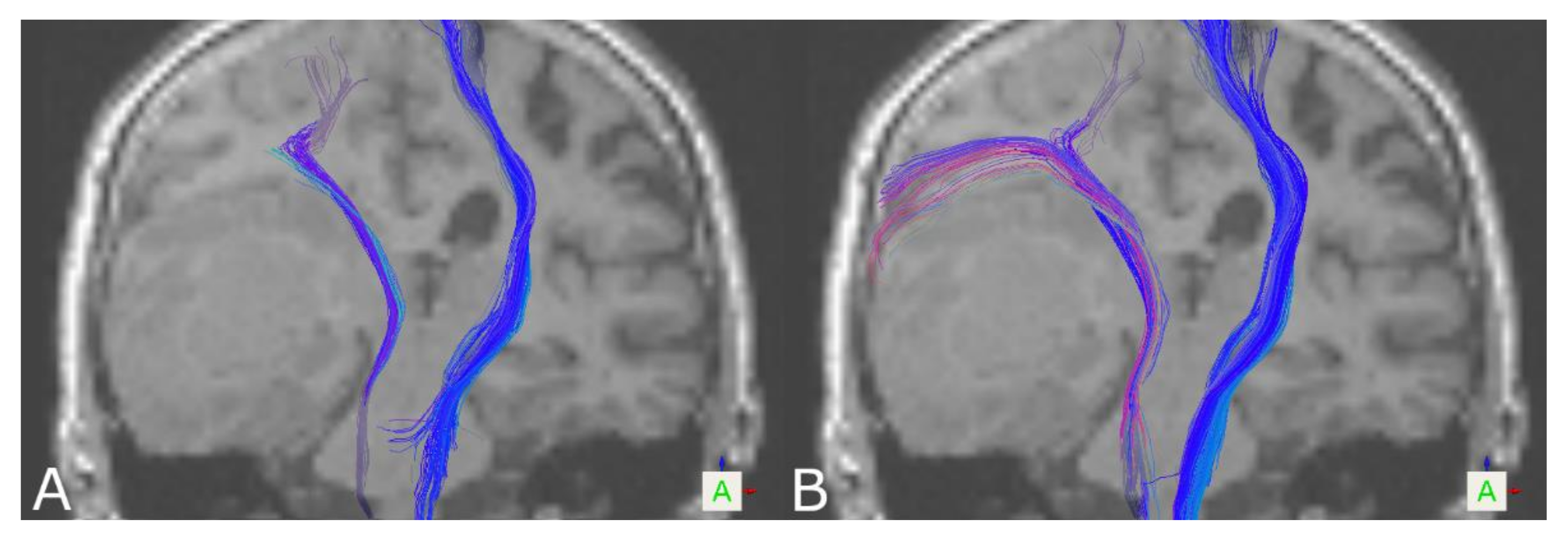
3.1. The Corticospinal Tract
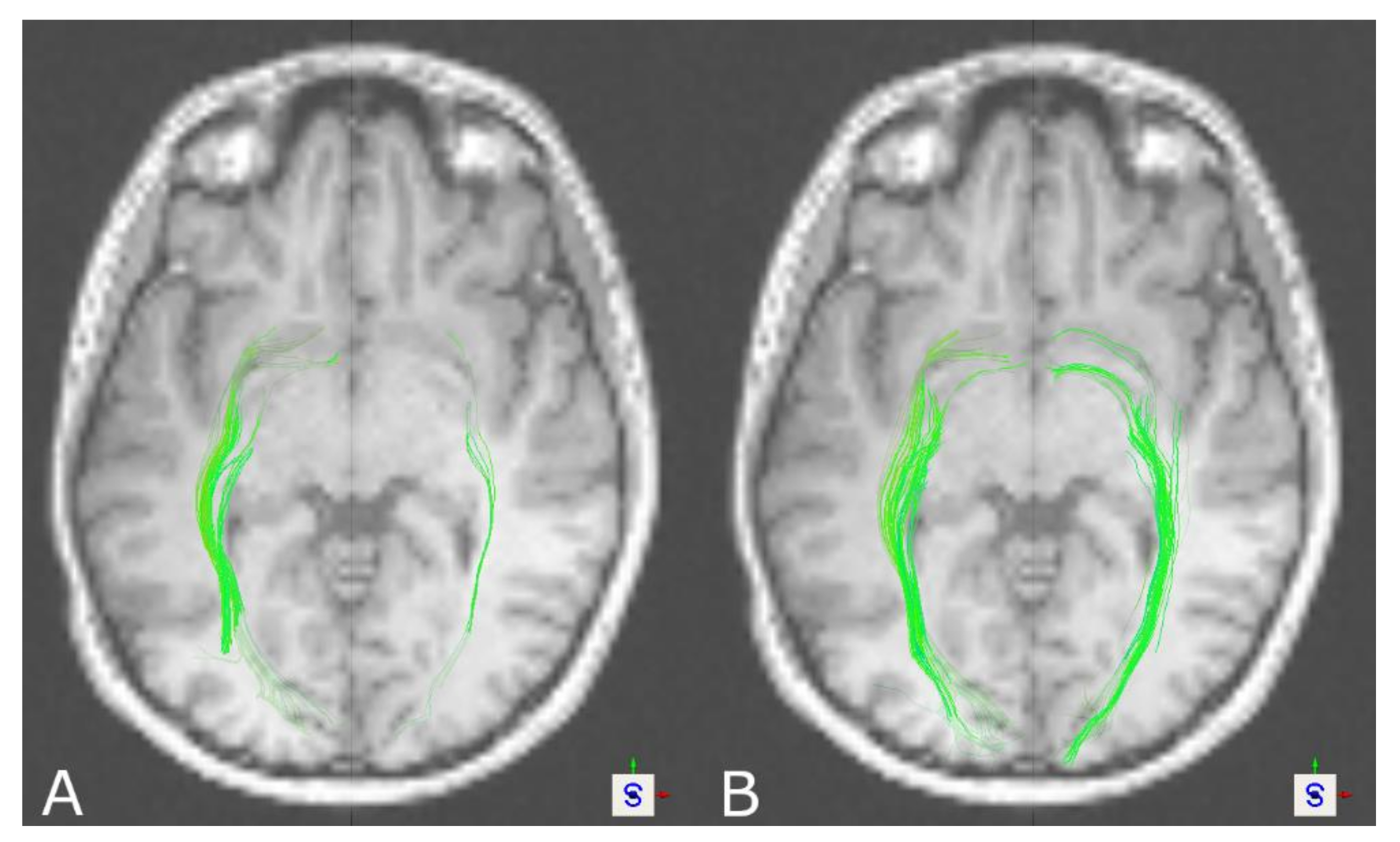
3.2. The Optic Radiation
3.3. The Arcuate Fascicle
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A




References
- Kuhnt, D.; Becker, A.; Ganslandt, O.; Bauer, M.; Buchfelder, M.; Nimsky, C. Correlation of the extent of tumor volume resection and patient survival in surgery of glioblastoma multiforme with high-field intraoperative MRI guidance. Neuro Oncol. 2011, 13, 1339–1348. [Google Scholar] [CrossRef] [Green Version]
- Nimsky, C.; Ganslandt, O.; Buchfelder, M.; Fahlbusch, R. Intraoperative visualization for resection of gliomas: The role of functional neuronavigation and intraoperative 1.5 T MRI. Neurol. Res. 2006, 28, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Nimsky, C.; Ganslandt, O.; Hastreiter, P.; Wang, R.; Benner, T.; Sorensen, A.G.; Fahlbusch, R. Preoperative and intraoperative diffusion tensor imaging-based fiber tracking in glioma surgery. Neurosurgery 2005, 56, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Essayed, W.I.; Zhang, F.; Unadkat, P.; Cosgrove, G.R.; Golby, A.J.; O′Donnell, L.J. White matter tractography for neurosurgical planning: A topography-based review of the current state of the art. Neuroimage Clin. 2017, 15, 659–672. [Google Scholar] [CrossRef] [PubMed]
- Nimsky, C.; Bauer, M.; Carl, B. Merits and Limits of Tractography Techniques for the Uninitiated. Adv. Tech. Stand. Neurosurg. 2016, 43, 37–60. [Google Scholar] [CrossRef]
- Kinoshita, M.; Yamada, K.; Hashimoto, N.; Kato, A.; Izumoto, S.; Baba, T.; Maruno, M.; Nishimura, T.; Yoshimine, T. Fiber-tracking does not accurately estimate size of fiber bundle in pathological condition: Initial neurosurgical experience using neuronavigation and subcortical white matter stimulation. Neuroimage 2005, 25, 424–429. [Google Scholar] [CrossRef]
- Mohammadi, S.; Moller, H.E.; Kugel, H.; Muller, D.K.; Deppe, M. Correcting eddy current and motion effects by affine whole-brain registrations: Evaluation of three-dimensional distortions and comparison with slicewise correction. Magn. Reson. Med. 2010, 64, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Ruthotto, L.; Kugel, H.; Olesch, J.; Fischer, B.; Modersitzki, J.; Burger, M.; Wolters, C.H. Diffeomorphic susceptibility artifact correction of diffusion-weighted magnetic resonance images. Phys. Med. Biol. 2012, 57, 5715–5731. [Google Scholar] [CrossRef] [PubMed]
- Merhof, D.; Soza, G.; Stadlbauer, A.; Greiner, G.; Nimsky, C. Correction of susceptibility artifacts in diffusion tensor data using non-linear registration. Med. Image Anal. 2007, 11, 588–603. [Google Scholar] [CrossRef] [Green Version]
- Gerhardt, J.; Sollmann, N.; Hiepe, P.; Kirschke, J.S.; Meyer, B.; Krieg, S.M.; Ringel, F. Retrospective distortion correction of diffusion tensor imaging data by semi-elastic image fusion—Evaluation by means of anatomical landmarks. Clin. Neurol. Neurosurg. 2019, 183, 105387. [Google Scholar] [CrossRef]
- Habib, J.; Auer, D.P.; Morgan, P.S. A quantitative analysis of the benefits of cardiac gating in practical diffusion tensor imaging of the brain. Magn. Reson. Med. 2010, 63, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- Bopp, M.H.A.; Yang, J.; Nimsky, C.; Carl, B. The effect of pulsatile motion and cardiac-gating on reconstruction and diffusion tensor properties of the corticospinal tract. Sci. Rep. 2018, 8, 11204. [Google Scholar] [CrossRef] [PubMed]
- Reinges, M.H.; Schoth, F.; Coenen, V.A.; Krings, T. Imaging of postthalamic visual fiber tracts by anisotropic diffusion weighted MRI and diffusion tensor imaging: Principles and applications. Eur. J. Radiol. 2004, 49, 91–104. [Google Scholar] [CrossRef]
- Yang, J.; Carl, B.; Nimsky, C.; Bopp, M.H.A. The impact of position-orientation adaptive smoothing in diffusion weighted imaging-From diffusion metrics to fiber tractography. PLoS ONE 2020, 15, e0233474. [Google Scholar] [CrossRef] [PubMed]
- Bopp, M.H.; Pietruk, P.M.; Nimsky, C.; Carl, B. Fiber tractography of the optic radiations: Impact of diffusion model, voxel shape and orientation. J. Neurosurg. Sci. 2019. [Google Scholar] [CrossRef]
- Fernandez-Miranda, J.C.; Pathak, S.; Engh, J.; Jarbo, K.; Verstynen, T.; Yeh, F.C.; Wang, Y.; Mintz, A.; Boada, F.; Schneider, W.; et al. High-definition fiber tractography of the human brain: Neuroanatomical validation and neurosurgical applications. Neurosurgery 2012, 71, 430–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrens, T.E.; Berg, H.J.; Jbabdi, S.; Rushworth, M.F.; Woolrich, M.W. Probabilistic diffusion tractography with multiple fibre orientations: What can we gain? Neuroimage 2007, 34, 144–155. [Google Scholar] [CrossRef]
- Tuch, D.S.; Reese, T.G.; Wiegell, M.R.; Makris, N.; Belliveau, J.W.; Wedeen, V.J. High angular resolution diffusion imaging reveals intravoxel white matter fiber heterogeneity. Magn. Reson. Med. 2002, 48, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Tuch, D.S. Q-ball imaging. Magn. Reson. Med. 2004, 52, 1358–1372. [Google Scholar] [CrossRef]
- Wedeen, V.J.; Wang, R.P.; Schmahmann, J.D.; Benner, T.; Tseng, W.Y.; Dai, G.; Pandya, D.N.; Hagmann, P.; D’Arceuil, H.; de Crespigny, A.J. Diffusion spectrum magnetic resonance imaging (DSI) tractography of crossing fibers. Neuroimage 2008, 41, 1267–1277. [Google Scholar] [CrossRef]
- Michailovich, O.; Rathi, Y.; Dolui, S. Spatially regularized compressed sensing for high angular resolution diffusion imaging. IEEE Trans. Med. Imaging 2011, 30, 1100–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhnt, D.; Bauer, M.H.; Sommer, J.; Merhof, D.; Nimsky, C. Optic radiation fiber tractography in glioma patients based on high angular resolution diffusion imaging with compressed sensing compared with diffusion tensor imaging—Initial experience. PLoS ONE 2013, 8, e70973. [Google Scholar] [CrossRef]
- Kuhnt, D.; Bauer, M.H.; Egger, J.; Richter, M.; Kapur, T.; Sommer, J.; Merhof, D.; Nimsky, C. Fiber tractography based on diffusion tensor imaging compared with high-angular-resolution diffusion imaging with compressed sensing: Initial experience. Neurosurgery 2013, 72 (Suppl. S1), 165–175. [Google Scholar] [CrossRef] [Green Version]
- Jensen, J.H.; Helpern, J.A. MRI quantification of non-Gaussian water diffusion by kurtosis analysis. NMR Biomed. 2010, 23, 698–710. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.H.; Helpern, J.A.; Ramani, A.; Lu, H.; Kaczynski, K. Diffusional kurtosis imaging: The quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn. Reson. Med. 2005, 53, 1432–1440. [Google Scholar] [CrossRef]
- Lazar, M.; Jensen, J.H.; Xuan, L.; Helpern, J.A. Estimation of the orientation distribution function from diffusional kurtosis imaging. Magn. Reson. Med. 2008, 60, 774–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steven, A.J.; Zhuo, J.; Melhem, E.R. Diffusion kurtosis imaging: An emerging technique for evaluating the microstructural environment of the brain. AJR Am. J. Roentgenol. 2014, 202, W26–W33. [Google Scholar] [CrossRef] [PubMed]
- Lazar, M. Mapping brain anatomical connectivity using white matter tractography. NMR Biomed. 2010, 23, 821–835. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.H.; Helpern, J.A.; Tabesh, A. Leading non-Gaussian corrections for diffusion orientation distribution function. NMR Biomed. 2014, 27, 202–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neto Henriques, R.; Correia, M.M.; Nunes, R.G.; Ferreira, H.A. Exploring the 3D geometry of the diffusion kurtosis tensor--impact on the development of robust tractography procedures and novel biomarkers. Neuroimage 2015, 111, 85–99. [Google Scholar] [CrossRef] [Green Version]
- Abdalla, G.; Dixon, L.; Sanverdi, E.; Machado, P.M.; Kwong, J.S.W.; Panovska-Griffiths, J.; Rojas-Garcia, A.; Yoneoka, D.; Veraart, J.; Van Cauter, S.; et al. The diagnostic role of diffusional kurtosis imaging in glioma grading and differentiation of gliomas from other intra-axial brain tumours: A systematic review with critical appraisal and meta-analysis. Neuroradiology 2020, 62, 791–802. [Google Scholar] [CrossRef]
- Van Cauter, S.; De Keyzer, F.; Sima, D.M.; Sava, A.C.; D’Arco, F.; Veraart, J.; Peeters, R.R.; Leemans, A.; Van Gool, S.; Wilms, G.; et al. Integrating diffusion kurtosis imaging, dynamic susceptibility-weighted contrast-enhanced MRI, and short echo time chemical shift imaging for grading gliomas. Neuro Oncol. 2014, 16, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.; Jiang, J.; Zhao, L.; Zhang, J.; Zhang, S.; Yao, Y.; Yang, S.; Shi, J.; Shen, N.; Su, C.; et al. Diffusion kurtosis imaging can efficiently assess the glioma grade and cellular proliferation. Oncotarget 2015, 6, 42380–42393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raja, R.; Sinha, N.; Saini, J.; Mahadevan, A.; Rao, K.N.; Swaminathan, A. Assessment of tissue heterogeneity using diffusion tensor and diffusion kurtosis imaging for grading gliomas. Neuroradiology 2016, 58, 1217–1231. [Google Scholar] [CrossRef]
- Hempel, J.M.; Bisdas, S.; Schittenhelm, J.; Brendle, C.; Bender, B.; Wassmann, H.; Skardelly, M.; Tabatabai, G.; Vega, S.C.; Ernemann, U.; et al. In vivo molecular profiling of human glioma using diffusion kurtosis imaging. J. Neurooncol. 2017, 131, 93–101. [Google Scholar] [CrossRef]
- Tietze, A.; Hansen, M.B.; Ostergaard, L.; Jespersen, S.N.; Sangill, R.; Lund, T.E.; Geneser, M.; Hjelm, M.; Hansen, B. Mean Diffusional Kurtosis in Patients with Glioma: Initial Results with a Fast Imaging Method in a Clinical Setting. AJNR Am. J. Neuroradiol. 2015, 36, 1472–1478. [Google Scholar] [CrossRef] [Green Version]
- Delgado, A.F.; Fahlstrom, M.; Nilsson, M.; Berntsson, S.G.; Zetterling, M.; Libard, S.; Alafuzoff, I.; van Westen, D.; Latt, J.; Smits, A.; et al. Diffusion Kurtosis Imaging of Gliomas Grades II and III—A Study of Perilesional Tumor Infiltration, Tumor Grades and Subtypes at Clinical Presentation. Radiol. Oncol. 2017, 51, 121–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goryawala, M.Z.; Heros, D.O.; Komotar, R.J.; Sheriff, S.; Saraf-Lavi, E.; Maudsley, A.A. Value of diffusion kurtosis imaging in assessing low-grade gliomas. J. Magn. Reson. Imaging 2018, 48, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Shi, W.; Wang, D.; Xu, Y.; Li, H.; He, J.; Zeng, Q. Evaluation of histopathological changes in the microstructure at the center and periphery of glioma tumors using diffusional kurtosis imaging. Clin. Neurol. Neurosurg. 2016, 151, 120–127. [Google Scholar] [CrossRef]
- Zhang, J.; Jiang, J.; Zhao, L.; Zhang, J.; Shen, N.; Li, S.; Guo, L.; Su, C.; Jiang, R.; Zhu, W. Survival prediction of high-grade glioma patients with diffusion kurtosis imaging. Am. J. Transl. Res. 2019, 11, 3680–3688. [Google Scholar]
- Glenn, G.R.; Helpern, J.A.; Tabesh, A.; Jensen, J.H. Optimization of white matter fiber tractography with diffusional kurtosis imaging. NMR Biomed. 2015, 28, 1245–1256. [Google Scholar] [CrossRef]
- Leote, J.; Nunes, R.G.; Cerqueira, L.; Loucao, R.; Ferreira, H.A. Reconstruction of white matter fibre tracts using diffusion kurtosis tensor imaging at 1.5T: Pre-surgical planning in patients with gliomas. Eur. J. Radiol. Open 2018, 5, 20–23. [Google Scholar] [CrossRef] [Green Version]
- Leote, J.; Nunes, R.; Cerqueira, L.; Ferreira, H.A. Corticospinal MRI tractography in space-occupying brain lesions by diffusion tensor and kurtosis imaging methods. EJNMMI Phys. 2015, 2, A82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loução, R.; Nunes, R.G.; Neto-Henriques, R.; Correia, M.; Ferreira, H. Human brain tractography: A DTI vs DKI comparison analysis. In Proceedings of the IEEE 4th Portuguese Meeting on Bioengineering (ENBENG), Porto, Portugal, 26–28 February 2015. [Google Scholar]
- Leemans, A.; Jones, D.K. The B-matrix must be rotated when correcting for subject motion in DTI data. Magn. Reson. Med. 2009, 61, 1336–1349. [Google Scholar] [CrossRef] [PubMed]
- Tabesh, A.; Jensen, J.H.; Ardekani, B.A.; Helpern, J.A. Estimation of tensors and tensor-derived measures in diffusional kurtosis imaging. Magn. Reson. Med. 2011, 65, 823–836. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Benner, T.; Sorensen, A.; Wedeen, V.J. Diffusion Toolkit: A Software Package for Diffusion Imaging Data Processing and Tractography. In Proceedings of the 15th Annual Meeting of the International Society for Magnetic Resonance in Medicine, Kumamoto, Japan, 18–21 June 2018. [Google Scholar]
- Hattingen, E.; Rathert, J.; Jurcoane, A.; Weidauer, S.; Szelenyi, A.; Ogrezeanu, G.; Seifert, V.; Zanella, F.E.; Gasser, T. A standardised evaluation of pre-surgical imaging of the corticospinal tract: Where to place the seed ROI. Neurosurg. Rev. 2009, 32, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Reich, D.S.; Smith, S.A.; Jones, C.K.; Zackowski, K.M.; van Zijl, P.C.; Calabresi, P.A.; Mori, S. Quantitative characterization of the corticospinal tract at 3T. AJNR Am. J. Neuroradiol. 2006, 27, 2168–2178. [Google Scholar] [PubMed]
- Winston, G.P.; Daga, P.; Stretton, J.; Modat, M.; Symms, M.R.; McEvoy, A.W.; Ourselin, S.; Duncan, J.S. Optic radiation tractography and vision in anterior temporal lobe resection. Ann. Neurol. 2012, 71, 334–341. [Google Scholar] [CrossRef]
- Yogarajah, M.; Focke, N.K.; Bonelli, S.; Cercignani, M.; Acheson, J.; Parker, G.J.; Alexander, D.C.; McEvoy, A.W.; Symms, M.R.; Koepp, M.J.; et al. Defining Meyer’s loop-temporal lobe resections, visual field deficits and diffusion tensor tractography. Brain 2009, 132, 1656–1668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.; Rigolo, L.; O’Donnell, L.J.; Norton, I.; Shriver, S.; Golby, A.J. Visual pathway study using in vivo diffusion tensor imaging tractography to complement classic anatomy. Neurosurgery 2012, 70, 145–156; discussion 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.J.; Riley, J.D.; Juranek, J.; Cramer, S.C. Vulnerability of the frontal-temporal connections in temporal lobe epilepsy. Epilepsy Res. 2008, 82, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Vernooij, M.W.; Smits, M.; Wielopolski, P.A.; Houston, G.C.; Krestin, G.P.; van der Lugt, A. Fiber density asymmetry of the arcuate fasciculus in relation to functional hemispheric language lateralization in both right- and left-handed healthy subjects: A combined fMRI and DTI study. Neuroimage 2007, 35, 1064–1076. [Google Scholar] [CrossRef] [PubMed]
- Eickhoff, S.B.; Paus, T.; Caspers, S.; Grosbras, M.H.; Evans, A.C.; Zilles, K.; Amunts, K. Assignment of functional activations to probabilistic cytoarchitectonic areas revisited. Neuroimage 2007, 36, 511–521. [Google Scholar] [CrossRef]
- Eickhoff, S.B.; Heim, S.; Zilles, K.; Amunts, K. Testing anatomically specified hypotheses in functional imaging using cytoarchitectonic maps. Neuroimage 2006, 32, 570–582. [Google Scholar] [CrossRef]
- Eickhoff, S.B.; Stephan, K.E.; Mohlberg, H.; Grefkes, C.; Fink, G.R.; Amunts, K.; Zilles, K. A new SPM toolbox for combining probabilistic cytoarchitectonic maps and functional imaging data. Neuroimage 2005, 25, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Woolrich, M.W.; Jbabdi, S.; Patenaude, B.; Chappell, M.; Makni, S.; Behrens, T.; Beckmann, C.; Jenkinson, M.; Smith, S.M. Bayesian analysis of neuroimaging data in FSL. Neuroimage 2009, 45, S173–S186. [Google Scholar] [CrossRef]
- Jenkinson, M.; Beckmann, C.F.; Behrens, T.E.; Woolrich, M.W.; Smith, S.M. Fsl. Neuroimage 2012, 62, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004, 23 (Suppl. S1), S208–S219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catani, M.; Thiebaut de Schotten, M. A diffusion tensor imaging tractography atlas for virtual in vivo dissections. Cortex 2008, 44, 1105–1132. [Google Scholar] [CrossRef]
- Dini, L.I.; Vedolin, L.M.; Bertholdo, D.; Grando, R.D.; Mazzola, A.; Dini, S.A.; Isolan, G.R.; da Costa, J.C.; Campero, A. Reproducibility of quantitative fiber tracking measurements in diffusion tensor imaging of frontal lobe tracts: A protocol based on the fiber dissection technique. Surg. Neurol. Int. 2013, 4, 51. [Google Scholar] [CrossRef] [PubMed]
- Wassermann, D.; Makris, N.; Rathi, Y.; Shenton, M.; Kikinis, R.; Kubicki, M.; Westin, C.F. The white matter query language: A novel approach for describing human white matter anatomy. Brain Struct. Funct. 2016, 221, 4705–4721. [Google Scholar] [CrossRef]
- Martino, J.; De Witt Hamer, P.C.; Vergani, F.; Brogna, C.; de Lucas, E.M.; Vazquez-Barquero, A.; Garcia-Porrero, J.A.; Duffau, H. Cortex-sparing fiber dissection: An improved method for the study of white matter anatomy in the human brain. J. Anat. 2011, 219, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Sydnor, V.J.; Rivas-Grajales, A.M.; Lyall, A.E.; Zhang, F.; Bouix, S.; Karmacharya, S.; Shenton, M.E.; Westin, C.F.; Makris, N.; Wassermann, D.; et al. A comparison of three fiber tract delineation methods and their impact on white matter analysis. Neuroimage 2018, 178, 318–331. [Google Scholar] [CrossRef]
- Zhang, H.; Awate, S.P.; Das, S.R.; Woo, J.H.; Melhem, E.R.; Gee, J.C.; Yushkevich, P.A. A tract-specific framework for white matter morphometry combining macroscopic and microscopic tract features. Med. Image Anal. 2010, 14, 666–673. [Google Scholar] [CrossRef]
- Nimsky, C. Fiber tracking—We should move beyond diffusion tensor imaging. World Neurosurg. 2014, 82, 35–36. [Google Scholar] [CrossRef] [PubMed]
- Farquharson, S.; Tournier, J.D.; Calamante, F.; Fabinyi, G.; Schneider-Kolsky, M.; Jackson, G.D.; Connelly, A. White matter fiber tractography: Why we need to move beyond DTI. J. Neurosurg. 2013, 118, 1367–1377. [Google Scholar] [CrossRef] [Green Version]
- Neher, P.F.; Descoteaux, M.; Houde, J.C.; Stieltjes, B.; Maier-Hein, K.H. Strengths and weaknesses of state of the art fiber tractography pipelines—A comprehensive in-vivo and phantom evaluation study using Tractometer. Med. Image Anal. 2015, 26, 287–305. [Google Scholar] [CrossRef]
- Wilkins, B.; Lee, N.; Gajawelli, N.; Law, M.; Lepore, N. Fiber estimation and tractography in diffusion MRI: Development of simulated brain images and comparison of multi-fiber analysis methods at clinical b-values. Neuroimage 2015, 109, 341–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cote, M.A.; Girard, G.; Bore, A.; Garyfallidis, E.; Houde, J.C.; Descoteaux, M. Tractometer: Towards validation of tractography pipelines. Med. Image Anal. 2013, 17, 844–857. [Google Scholar] [CrossRef]
- Fillard, P.; Descoteaux, M.; Goh, A.; Gouttard, S.; Jeurissen, B.; Malcolm, J.; Ramirez-Manzanares, A.; Reisert, M.; Sakaie, K.; Tensaouti, F.; et al. Quantitative evaluation of 10 tractography algorithms on a realistic diffusion MR phantom. Neuroimage 2011, 56, 220–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tournier, J.D.; Mori, S.; Leemans, A. Diffusion tensor imaging and beyond. Magn. Reson. Med. 2011, 65, 1532–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrale, M.; Collura, G.; Brai, M.; Toschi, N.; Midiri, F.; La Tona, G.; Lo Casto, A.; Gagliardo, C. Physics, Techniques and Review of Neuroradiological Applications of Diffusion Kurtosis Imaging (DKI). Clin. Neuroradiol. 2016, 26, 391–403. [Google Scholar] [CrossRef]
- Glenn, G.R.; Kuo, L.W.; Chao, Y.P.; Lee, C.Y.; Helpern, J.A.; Jensen, J.H. Mapping the Orientation of White Matter Fiber Bundles: A Comparative Study of Diffusion Tensor Imaging, Diffusional Kurtosis Imaging, and Diffusion Spectrum Imaging. AJNR Am. J. Neuroradiol. 2016, 37, 1216–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.C.; Phal, P.M.; Desmond, P.M.; Nichols, A.D.; Kokkinos, C.; Danesh-Meyer, H.V.; Kaye, A.H.; Moffat, B.A. Probabilistic MRI tractography of the optic radiation using constrained spherical deconvolution: A feasibility study. PLoS ONE 2015, 10, e0118948. [Google Scholar] [CrossRef] [PubMed]
- Dayan, M.; Kreutzer, S.; Clark, C.A. Tractography of the optic radiation: A repeatability and reproducibility study. NMR Biomed. 2015, 28, 423–431. [Google Scholar] [CrossRef]
- Yamamoto, T.; Yamada, K.; Nishimura, T.; Kinoshita, S. Tractography to depict three layers of visual field trajectories to the calcarine gyri. Am. J. Ophthalmol. 2005, 140, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Sherbondy, A.J.; Dougherty, R.F.; Napel, S.; Wandell, B.A. Identifying the human optic radiation using diffusion imaging and fiber tractography. J. Vis. 2008, 8, 12.1–12.11. [Google Scholar] [CrossRef]
- Sincoff, E.H.; Tan, Y.; Abdulrauf, S.I. White matter fiber dissection of the optic radiations of the temporal lobe and implications for surgical approaches to the temporal horn. J. Neurosurg. 2004, 101, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.; Miki, Y.; Urayama, S.; Fushimi, Y.; Okada, T.; Hanakawa, T.; Fukuyama, H.; Togashi, K. Diffusion tensor fiber tractography of the optic radiation: Analysis with 6-, 12-, 40-, and 81-directional motion-probing gradients, a preliminary study. AJNR Am. J. Neuroradiol. 2007, 28, 92–96. [Google Scholar]
- Mandelstam, S.A. Challenges of the anatomy and diffusion tensor tractography of the Meyer loop. AJNR Am. J. Neuroradiol. 2012, 33, 1204–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catani, M.; Jones, D.K.; Donato, R.; Ffytche, D.H. Occipito-temporal connections in the human brain. Brain 2003, 126, 2093–2107. [Google Scholar] [CrossRef] [PubMed]
- Yap, Q.J.; Teh, I.; Fusar-Poli, P.; Sum, M.Y.; Kuswanto, C.; Sim, K. Tracking cerebral white matter changes across the lifespan: Insights from diffusion tensor imaging studies. J. Neural Transm. 2013, 120, 1369–1395. [Google Scholar] [CrossRef] [PubMed]
- Barrio-Arranz, G.; de Luis-Garcia, R.; Tristan-Vega, A.; Martin-Fernandez, M.; Aja-Fernandez, S. Impact of MR Acquisition Parameters on DTI Scalar Indexes: A Tractography Based Approach. PLoS ONE 2015, 10, e0137905. [Google Scholar] [CrossRef]
- Borkowski, K.; Krzyzak, A.T. Analysis and correction of errors in DTI-based tractography due to diffusion gradient inhomogeneity. J. Magn. Reson. 2018, 296, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Krzyzak, A.T.; Olejniczak, Z. Improving the accuracy of PGSE DTI experiments using the spatial distribution of b matrix. Magn. Reson. Imaging 2015, 33, 286–295. [Google Scholar] [CrossRef]
- Mazur, W.; Urbanczyk-Zawadzka, M.; Banys, R.; Obuchowicz, R.; Trystula, M.; Krzyzak, A.T. Diffusion as a Natural Contrast in MR Imaging of Peripheral Artery Disease (PAD) Tissue Changes. A Case Study of the Clinical Application of DTI for a Patient with Chronic Calf Muscles Ischemia. Diagnostics 2021, 11, 92. [Google Scholar] [CrossRef]
- Andrews, E.; Eierud, C.; Banks, D.; Harshbarger, T.; Michael, A.; Rammell, C. Effects of Lifelong Musicianship on White Matter Integrity and Cognitive Brain Reserve. Brain Sci. 2021, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Qin, W.; Yu, C.S.; Zhang, F.; Du, X.Y.; Jiang, H.; Yan, Y.X.; Li, K.C. Effects of echo time on diffusion quantification of brain white matter at 1.5 T and 3.0 T. Magn. Reson. Med. 2009, 61, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Helmer, K.G.; Chou, M.C.; Preciado, R.I.; Gimi, B.; Rollins, N.K.; Song, A.; Turner, J.; Mori, S. Multi-site Study of Diffusion Metric Variability: Characterizing the Effects of Site, Vendor, Field Strength, and Echo Time using the Histogram Distance. Proc. SPIE Int. Soc. Opt. Eng. 2016, 9788. [Google Scholar] [CrossRef] [Green Version]
- Schilling, K.G.; Nath, V.; Hansen, C.; Parvathaneni, P.; Blaber, J.; Gao, Y.; Neher, P.; Aydogan, D.B.; Shi, Y.; Ocampo-Pineda, M.; et al. Limits to anatomical accuracy of diffusion tractography using modern approaches. Neuroimage 2019, 185, 1–11. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diffusion Tensor Imaging (DTI) | Diffusion Kurtosis Imaging (DKI) | DTI vs. DKI | ||||
|---|---|---|---|---|---|---|
| Left CST | Right CST | Left CST | Right CST | Left CST | Right CST | |
| Tract volume (cm3) | ||||||
| Mean ± SD | 13.34 ± 5.49 | 14.78 ± 5.36 | 18.57 ± 5.82 | 19.86 ± 5.47 | p < 0.001 * | p < 0.001 * |
| Range (min; max) | (3.89; 22.64) | (6.67; 25.61) | (8.70; 28.70) | (13.34; 29.88) | ||
| Tract density (fibers/voxel) | ||||||
| Mean ± SD | 6.74 ± 1.90 | 6.63 ± 1.99 | 8.49 ± 2.30 | 8.34 ± 2.51 | p < 0.001 * | p = 0.002 + |
| Range (min; max) | (1.85; 10.67) | (3.69; 9.52) | (3.70; 13.03) | (3.94; 13.92) | ||
| DTI | DKI | DTI vs. DKI | ||||
|---|---|---|---|---|---|---|
| Left CST | Right CST | Left CST | Right CST | Left CST | Right CST | |
| Tract volume (cm3) | ||||||
| Mean ± SD | 11.08 ± 4.58 | 10.74 ± 5.10 | 18.50 ± 6.17 | 18.44 ± 6.53 | p < 0.001 * | p < 0.001 * |
| Range (min; max) | (2.87; 17.25) | (3.53; 21.99) | (4.04; 26.27) | (6.62; 34.17) | ||
| Tract density (fibers/voxel) | ||||||
| Mean ± SD | 3.99 ± 1.57 | 4.34 ± 1.64 | 7.81 ± 2.58 | 8.23 ± 2.40 | p < 0.001 * | p < 0.001 * |
| Range (min; max) | (1.62; 6.70) | (1.25; 7.57) | (3.71; 11.88) | (4.59; 11.84) | ||
| DTI | DKI | DTI vs. DKI | ||||
|---|---|---|---|---|---|---|
| Left OR | Right OR | Left OR | Right OR | Left OR | Right OR | |
| Tract volume (cm3) | ||||||
| Mean ± SD | 5.74 ± 3.10 | 3.69 ± 2.40 | 7.64 ± 2.78 | 5.02 ± 2.33 | p < 0.001 * | p = 0.005 * |
| Range (min; max) | (1.11; 12.02) | (1.10; 10.78) | (3.28 to 14.18) | (0.74 to 10.40) | ||
| Tract density (fibers/voxel) | ||||||
| Mean ± SD | 2.84 ± 1.16 | 2.31 ± 0.80 | 3.48 ± 1.11 | 2.98 ± 1.19 | p = 0.005 + | p = 0.02499 * |
| Range (min; max) | (1.00; 5.68) | (1.00; 4.26) | (1.09; 5.90) | (1.00; 5.64) | ||
| DTI | DKI | DTI vs. DKI | ||||
|---|---|---|---|---|---|---|
| Left OR | Right OR | Left OR | Right OR | Left OR | Right OR | |
| Tract volume (cm3) | ||||||
| Mean ± SD | 4.07 ± 3.16 | 4.45 ± 3.23 | 5.43 ± 3.81 | 4.81 ± 2.61 | p = 0.021 * | p = 0.389 * |
| Range (min; max) | (0.38; 12.29) | (0.99; 14.10) | (0.35; 16.62) | (2.54; 13.42) | ||
| Tract density (fibers/voxel) | ||||||
| Mean ± SD | 2.77 ± 1.43 | 2.17 ± 1.18 | 2.91 ± 1.13 | 2.57 ± 1.12 | p = 0.638 * | p = 0.183 * |
| Range (min; max) | (1.00; 5.46) | (0.25; 4.00) | (1.25; 4.63) | (1.12; 4.73) | ||
| DTI | DKI | DTI vs. DKI | ||||
|---|---|---|---|---|---|---|
| Left AF | Right AF | Left AF | Right AF | Left AF | Right AF | |
| Tract volume (cm3) | ||||||
| Mean ± SD | 4.04 ± 1.74 | 3.31 ± 1.23 | 3.21 ± 1.73 | 2.61 ± 1.26 | p = 0.101 * | p = 0.044 + |
| Range (min; max) | (1.50; 7.38) | (1.12; 5.46) | (0.80; 6.43) | (0.42; 5.18) | ||
| Tract density (fibers/voxel) | ||||||
| Mean ± SD | 4.90 ± 2.35 | 4.56 ± 2.68 | 3.84 ± 2.05 | 3.61 ± 1.85 | p = 0.163 * | p = 0.205 * |
| Range (min; max) | (2.25; 10.56) | (0.29; 11.43) | (1.14; 9.67) | (1.05; 6.71) | ||
| DTI | DKI | DTI vs. DKI | ||||
|---|---|---|---|---|---|---|
| Left AF | Right AF | Left AF | Right AF | Left AF | Right AF | |
| Tract volume (cm3) | ||||||
| Mean ± SD | 5.02 ± 2.66 | 4.64 ± 1.97 | 3.66 ± 1.60 | 2.97 ± 1.09 | p = 0.023 * | p = 0.010 * |
| Range (min; max) | (0.58; 8.98) | (2.40; 8.75) | (0.00; 5.55) | (1.58; 5.45) | ||
| Tract density (fibers/voxel) | ||||||
| Mean ± SD | 6.53 ± 4.37 | 4.81 ± 1.91 | 3.57 ± 1.84 | 4.65 ± 2.72 | p = 0.010 * | p = 0.823 * |
| Range (min; max) | (0.60; 15.09) | (1.08; 7.78) | (0.00; 6.55) | (1.06; 9.70) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bopp, M.H.A.; Emde, J.; Carl, B.; Nimsky, C.; Saß, B. Diffusion Kurtosis Imaging Fiber Tractography of Major White Matter Tracts in Neurosurgery. Brain Sci. 2021, 11, 381. https://doi.org/10.3390/brainsci11030381
Bopp MHA, Emde J, Carl B, Nimsky C, Saß B. Diffusion Kurtosis Imaging Fiber Tractography of Major White Matter Tracts in Neurosurgery. Brain Sciences. 2021; 11(3):381. https://doi.org/10.3390/brainsci11030381
Chicago/Turabian StyleBopp, Miriam H. A., Julia Emde, Barbara Carl, Christopher Nimsky, and Benjamin Saß. 2021. "Diffusion Kurtosis Imaging Fiber Tractography of Major White Matter Tracts in Neurosurgery" Brain Sciences 11, no. 3: 381. https://doi.org/10.3390/brainsci11030381
APA StyleBopp, M. H. A., Emde, J., Carl, B., Nimsky, C., & Saß, B. (2021). Diffusion Kurtosis Imaging Fiber Tractography of Major White Matter Tracts in Neurosurgery. Brain Sciences, 11(3), 381. https://doi.org/10.3390/brainsci11030381