
Neurocognitive Impairment in Severe Mental Illness. Comparative study with Spanish Speaking Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
3. Results
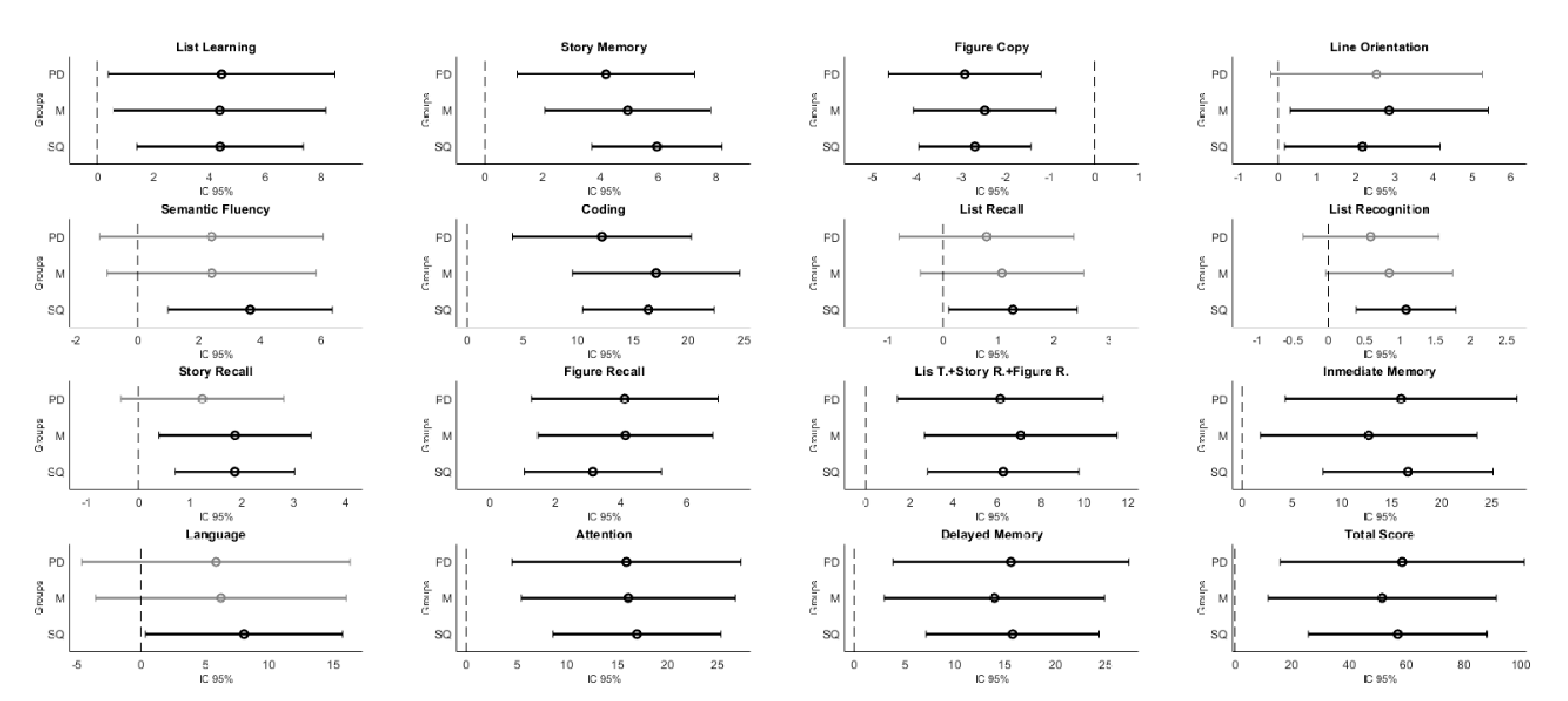
3.1. Between-Group Comparison
3.2. Control vs. Schizophrenia Disorder
3.3. Control vs. Mood Disorder
3.4. Control vs. Personality Disorder
3.5. Comparison among Clinical Groups
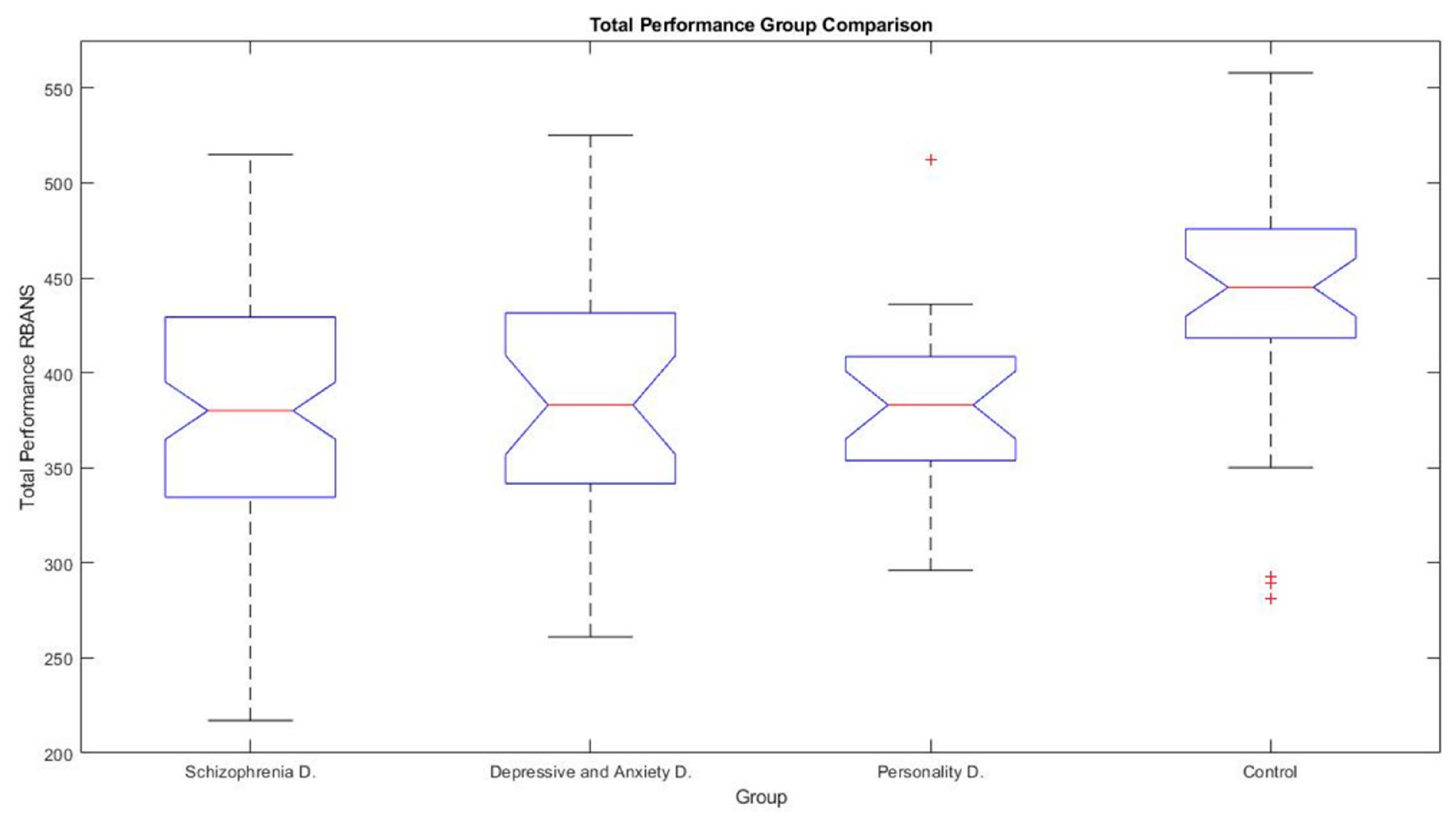
3.6. Global Performance Comparison
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- López, M.; Laviana, M. Rehabilitación, apoyo social y atención comunitaria a personas con trastorno mental grave: Propuestas desde Andalucía. Rev. Asoc. Esp. Neuropsiquiatr. 2007, 27, 187–223. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Report on Disability: Summary 2011, WHO/NMH/VIP/11.01. 2011. Available online: www.refworld.org/docid/50854a322.html (accessed on 23 October 2020).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- De la Torre, G.G.; Suarez-Llorens, A.; Caballero, F.J.; Ramallo, M.A.; Randolph, C.; Lleó, A.; Sala, I.; Sanchez, B. Norms and reliability for the Spanish version of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) Form A. J. Clin. Exp. Neuropsychol. 2014, 36, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Bazanis, E.; Rogers, R.D.; Dowson, J.H.; Taylor, P.; Meux, C.; Staley, C.; Nevinson-Andrews, D.; Taylor, C.; Robbins, T.W.; Sahakian, B.J. Neurocognitive deficits in decision-making and planning of patients with DSM-III-R borderline personality disorder. Psychol. Med. 2002, 32, 1395–1405. [Google Scholar] [CrossRef]
- Kurtz, M. Neurocognitive impairment across the lifespan in schizophrenia: An update. Schizophr. Res. 2005, 74, 15–26. [Google Scholar] [CrossRef]
- Keefe, R.; Harvey, P. Cognitive Impairment in Schizophrenia. In Novel Antischizophrenia Treatments; Geyer, E.M., Gross, G., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 11–37. [Google Scholar]
- Heinrichs, R.; Zakzanis, K. Neurocognitive deficit in schizophrenia: A quantitative review of the evidence. Neuropsychology 1998, 12, 426–445. [Google Scholar] [CrossRef]
- Green, M.; Kern, R.; Braff, D. Neurocognitive deficits and functional outcome in schizophrenia: Are we measuring the “right stuff”? Schizophr. Bull. 2000, 26, 119–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowie, C.; Leung, W.; Reichenberg, A. Predicting schizophrenia patients’ real-world behavior with specific neuropsychological and functional capacity measures. Biol. Psychiatry 2008, 63, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lepage, M.; Bodnar, M.; Bowie, C.R. Neurocognition: Clinical and Functional Outcomes in Schizophrenia. Can. J. Psychiatry 2014, 59, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Puente, A.E.; Ojeda, C.; Zink, D.; Reyes, V.P. Neuropsychological testing of Spanish speakers. In Psychological Testing of Hispanics: Clinical, Cultural, and Intellectual Issues; Geisinger, K.F., Ed.; American Psychological Association: Washington, DC, USA, 2015; pp. 135–152. [Google Scholar] [CrossRef]
- Gómez-Benito, J.; Guilera, G.; Pino, Ó.; Rojo, E.; Tabarés-Seisdedos, R.; Safont, G.; Martínez-Arán, A.; Franco, M.; Cuesta, M.J.; Crespo-Facorro, B.; et al. The screen for cognitive impairment in psychiatry: Diagnostic-specific standardization in psychiatric ill patients. BMC Psychiatry 2013, 13, 127. [Google Scholar] [CrossRef] [Green Version]
- Domingo, S.Z.; Bobes, J.; García-Portilla, M.P.; Morralla, C. EPICOG-SCH: A brief battery to screen cognitive impact of schizophrenia in stable outpatients. Schizophr. Res. Cogn. 2017, 8, 7–20. [Google Scholar] [CrossRef]
- Rodriguez-Jimenez, R.; Bagney, A.; Garcia-Navarro, C.; Aparicio, A.I.; Lopez-Anton, R.; Moreno-Ortega, M.; Jiménez-Arriero, M.; Santos, J.; Lobo, A.; Kern, R.; et al. The MATRICS consensus cognitive battery (MCCB): Co-norming and standardization in Spain. Schizophr. Res. 2012, 134, 279–284. [Google Scholar] [CrossRef]
- Muntal-Encinas, S.; Gramunt-Fombuena, N.; Guia, D.B.; Hernanz, L.C.; Barbera, M.A. Spanish translation and adaptation of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) Form A in pilot sample. Neurología 2012, 27, 531–546. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, A.; Livingston, R.; Smernoff, R.; Reese, E.; Hafer, D.; Harris, J. Factor Analysis of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) in a Large Sample of Patients Suspected of Dementia. Appl. Neuropsychol. 2010, 17, 8–17. [Google Scholar] [CrossRef] [PubMed]
- De la Torre, G.G.; Perez, M.J.; Ramallo, M.A.; Randolph, C.; González-Villegas, M.B. Screening of Cognitive Impairment in Schizophrenia: Reliability, Sensitivity, and Specificity of the Repeatable Battery for the Assessment of Neuropsychological Status in a Spanish Sample. Assesment 2015, 23, 221–231. [Google Scholar] [CrossRef]
- Sanz, J.C.; Vargas, M.L.; Marín, J.J. Battery for assessment of neuropsychological status (RBANS) in schizophrenia: A pilot study in the Spanish population. Acta Neuropsychiatr. 2009, 21, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Loughland, C.; Lewin, T.; Carr, V.; Sheedy, J.; Harris, A. RBANS neuropsychological profiles within schizophrenia samples recruited from non-clinical settings. Schizophr. Res. 2007, 89, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Zaytseva, Y.; Fajnerová, I.; Dvořáček, B.; Bourama, E.; Stamou, I.; Šulcová, K.; Motýl, J.; Horáček, J.; Rodriguez, M.; Španiel, F. Theoretical modeling of cognitive dysfunction in schizophrenia by means of errors and corresponding brain networks. Front. Psychol. 2018, 9, 1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnsten, A.; Girgis, R.; Gray, D.; Mailman, R. Novel Dopamine Therapeutics for Cognitive Deficits in Schizophrenia. Biol. Psychiatry 2017, 81, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Saykin, A.; Shtasel, D.; Gur, R.; Kester, B.; Mozley, L.; Stafiniak, P.; Gur, R.C. Neuropsychological Deficits in Neuroleptic Naive Patients With First-Episode Schizophrenia. Arch. Gen. Psychiatry 1994, 51, 124–131. [Google Scholar] [CrossRef]
- Braff, D.; Heaton, R.; Kuck, J.; Cullum, M.; Moranville, J.; Grant, I.; Zisook, S. The Generalized Pattern of Neuropsychological Deficits in Outpatients With Chronic Schizophrenia With Heterogeneous Wisconsin Card Sorting Test Results. Arch. Gen. Psychiatry 1991, 48, 891–898. [Google Scholar] [CrossRef]
- Haining, K.; Matrunola, C.; Mitchell, L.; Gajwani, R.; Gross, J.; Gumley, A.; Stephen, M.; Lawrie, S.; Schwannauer, M.; Schultze-Lutter, F.; et al. Neuropsychological deficits in participants at clinical high risk for psychosis recruited from the community: Relationships to functioning and clinical symptoms. Psychol. Med. 2020, 50, 77–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, M. Schizophrenia from a Neurocognitive Perspective: Probing the Impenetrable Darkness; Mass Allyn & Bacon: Boston, MA, USA, 1998. [Google Scholar]
- Murray, R. Neurodevelopmental schizophrenia: The rediscovery of dementia praecox. Br. J. Psychiatry 1994, 165, 6–12. [Google Scholar] [CrossRef]
- Moore, E.; Green, M.; Carr, V. Comorbid personality traits in schizophrenia: Prevalence and clinical characteristics. J. Psychiatr. Res. 2012, 46, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, H.; Patten, S.B. Depression and work impairment. Health Rep. 2007, 18, 9–22. [Google Scholar]
- Zuckerman, H.; Pan, Z.; Park, C.; Brietzke, E.; Musial, N.; Shariq, A.S.; Iacobucci, M.; Yim, S.J.; Lui, L.M.W.; Rong, C.; et al. Recognition and treatment of cognitive dysfunction in major depressive disorder. Front. Psychiatry 2018, 9, 655. [Google Scholar] [CrossRef] [PubMed]
- Lam, R.W.; Kennedy, S.H.; McIntyre, R.S.; Khullar, A. Cognitive dysfunction in major depressive disorder: Effects on psychosocial functioning and implications for treatment. Can. J. Psychiatry 2014, 59, 649–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faust, K.; Nelson, B.D.; Sarapas, C.; Pliskin, N.H. Depression and performance on the repeatable battery for the assessment of neuropsychological status. Appl. Neuropsychol. Adult 2017, 24, 350–356. [Google Scholar] [CrossRef]
- Lima, I.M.; Peckham, A.D.; Johnson, S.L. Cognitive deficits in bipolar disorders: Implications for emotion. Clin. Psychol. Rev. 2018, 59, 126–136. [Google Scholar] [CrossRef]
- Dickerson, F.; Boronow, J.; Stallings, C.; Origoni, A.; Cole, S.; Yolken, R. Cognitive functioning in schizophrenia and bipolar disorder: Comparison of performance on the Repeatable Battery for the Assessment of Neuropsychological Status. Psychiatry Res. 2004, 129, 45–53. [Google Scholar] [CrossRef]
- Gogos, A.; Joshua, N.; Rossell, S. Use of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) to investigate group and gender differences in schizophrenia and bipolar disorder. Aust. N. Z. J. Psychiatry 2010, 44, 220–229. [Google Scholar] [CrossRef]
- Baune, B.T.; McAfoose, J.; Leach, G.; Quirk, F.; Mitchell, D. Impact of psychiatric and medical comorbidity on cognitive function in depression. Psychiatry Clin. Neurosci. 2009, 63, 392–400. [Google Scholar] [CrossRef]
- Johnson, L.A.; Mauer, C.; Jahn, D.; Song, M.; Wyshywaniuk, L.; Hall, J.R.; Balldin, V.H.; O’Bryant, S.E. Cognitive differences among depressed and non-depressed MCI participants: A project FRONTIER study. Int. J. Geriatr. Psychiatry 2013, 28, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Saavedra, J.; López, M.; González, S.; Arias, S.; Crawford, P. Cognitive and social functioning correlates of employment among people with severe mental illness. Community Ment. Health J. 2016, 52, 851–858. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Tsatali, M.; Fotiadou, F.; Giaglis, G.; Tsolaki, M. The repeatable battery for the assessment of the neuropsychological status (RBANS): A diagnostic validity study in Greek elderly. Aging Clin. Exp. Res. 2019, 31, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- Olaithe, M.; Weinborn, M.; Lowndes, T.; Ng, A.; Hodgson, E.; Fine, L.; Parker, D.; Pushpanathan, M.; Bayliss, D.; Anderson, M.; et al. Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Normative Data for Older Adults. Arch. Clin. Neuropsychol. 2019, 34, 1356–1366. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.R.; Balldin, V.H.; Gamboa, A.; Edwards, M.L.; Johnson, L.A.; O’Bryant, S.E. Texas Mexican American adult normative studies: Normative data for the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). Dev. Neuropsychol. 2018, 43, 27–35. [Google Scholar] [CrossRef]
- Batty, R.A.; Francis, A.; Thomas, N.; Hopwood, M.; Ponsford, J.; Rossell, S.L. A brief neurocognitive assessment of patients with psychosis following traumatic brain injury (PFTBI): Use of the Repeatable battery for the Assessment of Neuropsychological Status (RBANS). Psychiatry Res. 2016, 237, 27–36. [Google Scholar] [CrossRef]
- Muntal-Encinas, S.; Doval, E.; Badenes, D.; Casas-Hernanz, L.; Cerulla, N.; Calzado, N.; Aguilar, M. New data from the Spanish-language version of the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), form A. Neurología 2020, 35, 303–310. [Google Scholar] [CrossRef]
- Harvey, P.; Fortuny, L.; Vester-Blockland, E.; De Smedt, G. Cross-national cognitive assessment in schizophrenia clinical trials: A feasibility study. Schizophr. Res. 2003, 59, 243–251. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochber, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Kraus, M.; Keefe, R. Cognition as an outcome measure in schizophrenia. Br. J. Psychiatry 2007, 191, s46–s51. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D. Cortical circuit dysfunction and cognitive deficits in schizophrenia–implications for preemptive interventions. Eur. J. Neurosci. 2012, 35, 1871–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinzen, W.; Ximenes, J.R. The linguistics of schizophrenia: Thought disturbance as language pathology across symptoms. Front. Psychol. 2015, 6, 971. [Google Scholar] [CrossRef] [Green Version]
- Murphy, E.; Benítez-Burraco, A. Bridging the gap between genes and language deficits in schizophrenia: An oscillopathic approach. Front. Hum. Neurosci. 2016, 10, 422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcclure, G.; Hawes, D.J.; Dadds, M.R. Borderline personality disorder and neuropsychological measures of executive function: A systematic review. Personal. Ment. Health 2016, 10, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, T.; Becerra, R.; Coombes, J. Executive functioning deficits among adults with Bipolar Disorder (types I and II): A systematic review and meta-analysis. J. Affect. Disord. 2017, 218, 407–427. [Google Scholar] [CrossRef] [PubMed]
- Rock, P.L.; Roiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029. [Google Scholar] [CrossRef] [Green Version]
- Bredemeier, K.; Warren, S.L.; Berenbaum, H.; Miller, G.A.; Heller, W. Executive function deficits associated with current and past major depressive symptoms. J. Affect. Disord. 2016, 204, 226–233. [Google Scholar] [CrossRef] [Green Version]
- DeBattista, C. Executive dysfunction in major depressive disorder. Expert Rev. Neurother. 2005, 5, 79–83. [Google Scholar] [CrossRef]
- Schug, R.A.; Raine, A. Comparative meta-analyses of neuropsychological functioning in antisocial schizophrenic persons. Clin. Psychol. Rev. 2009, 29, 230–242. [Google Scholar] [CrossRef]
- Aleman, A.; Agrawal, N.; Morgan, K.D.; David, A.S. Insight in psychosis and neuropsychological function: Meta-analysis. Br. J. Psychiatry 2006, 189, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Li, H.; Stone, W.S.; Woodberry, K.A.; Seidman, L.J.; Tang, Y.; Guo, Q.; Zhuo, K.; Qian, Z.; Cui, H.; et al. Neuropsychological impairment in prodromal, first-episode, and chronic psychosis: Assessing RBANS performance. PLoS ONE 2015, 10, e0125784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, L.C.; Bailie, J.M.; Kinney, D.I.; Nitch, S.R. Is the repeatable battery for the assessment of neuropsychological status factor structure appropriate for inpatient psychiatry? An exploratory and higher-order analysis. Arch. Clin. Neuropsychol. 2012, 27, 756–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, J.M.; Queern, C.; Iannone, V.N.; Buchanan, R.W. Repeatable battery for the assessment of neuropsychological status as a screening test in schizophrenia, I: Sensitivity, reliability, and validity. Am. J. Psychiatry 1999, 156, 1944–1950. [Google Scholar] [PubMed]
- Seres, I.; Unoka, Z.; Bódi, N.; Aspán, N.; Kéri, S. The neuropsychology of borderline personality disorder: Relationship with clinical dimensions and comparison with other personality disorders. J. Personal. Disord. 2009, 23, 555–562. [Google Scholar] [CrossRef]
- Randolph, C. Repeatable Battery for the Assessment of Neuropsychological Status (RBANS); The Psychological Corporation: San Antonio, TX, USA, 1998. [Google Scholar]



{kind=link}
{kind=link}
| MEAN ± STD | ANCOVA | Post hoc p-Values | Effect Size | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Healthy Controls | Schizophrenia Disorder | Mood Disorders | BL Personality Disorder | ANCOVAF | p-Value | Controls vs. Schizophrenia | Controls vs. Mood | Controls vs. Personality | Eta-Squared (η2) | |
| n | 35 | 97 | 29 | 23 | ||||||
| Age | 38.63 ± 17.98 | 40 ± 7.45 | 42.48 ± 8.83 | 37.22 ± 7.44 | ||||||
| Gender (M-F) | 11/24 | 69/28 | 16/13 | 16/7 | ||||||
| Level of education | 3.66 ± 0.53 | 3.42 ± 0.95 | 3.59 ± 0.98 | 3.52 ± 1.08 | ||||||
| Total performance | 440 ± 66.65 | 383.04 ± 58 | 388.52 ± 64.32 | 381.52 ± 46.14 | 8.31 | <0.001 * | <0.001 * | 0.002 * | 0.002* | 0.108 |
| List Learning | 28.8 ± 6.89 | 24.40 ± 5.52 | 24.41 ± 5.29 | 24.35 ± 4.44 | 4.84 | 0.004 * | 0.002 * | 0.016 * | 0.024 * | 0.063 |
| Story Memory | 17.37 ± 3.93 | 11.4 ± 4.5 | 12.41 ± 4.52 | 13.17 ± 3.58 | 16.6 | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.196 |
| Figure Copy | 16.26 ± 3.8 | 18.95 ± 2 | 18.72 ± 2.07 | 19.17 ± 1.40 | 11.82 | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.156 |
| Line Orientation | 17.46 ± 3.49 | 15.28 ± 3.81 | 14.59 ± 4.26 | 14.91 ± 3.67 | 5.96 | 0.001 * | <0.001 * | 0.002 * | 0.01 * | 0.060 |
| Picture Naming | 9.63 ± 1 | 9.75 ± 0.9 | 9.62 ± 0.78 | 9.87 ± 0.34 | 0.27 | 0.85 | 0.99 | 0.99 | 0.92 | 0.007 |
| Semantic Fluency | 18.94 ± 6.58 | 15.26 ± 4.63 | 16.52 ± 5.41 | 16.53 ± 3.93 | 3.74 | 0.02 * | 0.005* | 0.28 | 0.47 | 0.064 |
| Digit Span | 8.2 ± 1.65 | 7.86 ± 2.07 | 7.52 ± 1.79 | 7.74 ± 2.99 | 1.16 | 0.37 | 0.41 | 0.33 | 0.9 | 0.009 |
| Coding | 47.83 ± 14.47 | 31.45 ± 10.12 | 30.76 ± 11.81 | 35.65 ± 9.76 | 15.94 | <0.001 * | <0.001 * | <0.001 * | 0.003 * | 0.168 |
| List Recall | 6.49 ± 1.01 | 5.22 ± 2.5 | 5.41 ± 2.20 | 5.70 ± 2.22 | 2.18 | 0.11 | 0.06 | 0.29 | 0.68 | 0.04 |
| List Recognition | 19.86 ± 0.35 | 18.76 ± 1.6 | 19.00 ± 1.36 | 19.26 ± 0.92 | 5.04 | 0.003 * | <0.001 * | 0.066 | 0.38 | 0.075 |
| Story Recall | 7.63 ± 0.64 | 5.76 ± 2.38 | 5.76 ± 2.61 | 6.39 ± 2.31 | 6.56 | <0.001 * | <0.001 * | 0.003 * | 0.09 | 0.094 |
| Figure Recall | 15.91 ± 3.37 | 12.75 ± 3.87 | 11.76 ± 4.35 | 11.78 ± 4.66 | 8.23 | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.119 |
| List T. + Story R. + Figure R. | 30.03 ± 4.17 | 23.73 ± 6.8 | 22.93 ± 7.05 | 23.87 ± 7.91 | 8.88 | <0.001 * | <0.001 * | <0.001 * | 0.003 * | 0.125 |
| Inmediate Memory | 90.40 ± 18.49 | 73.78 ± 15.84 | 77.72 ± 17.31 | 74.48 ± 11.82 | 8.66 | <0.001 * | <0.001 * | 0.01 * | 0.002 * | 0.112 |
| Visuospatial | 88.77 ± 18.49 | 89.18 ± 17.23 | 86.24 ± 17.49 | 83.57 ± 17.94 | 0.58 | 0.66 | 0.99 | 0.9 | 0.71 | 0.011 |
| Language | 91.54 ± 18.91 | 83.52 ± 13.02 | 85.31 ± 15.65 | 85.70 ± 11.56 | 3.54 | 0.02 * | 0.06 | 0.2 | 0.31 | 0.062 |
| Attention | 76.83 ± 17.54 | 59.87 ± 15.08 | 60.72 ± 14.46 | 60.91 ± 18.03 | 9.53 | <0.001 * | <0.001 * | <0.001 * | 0.004 * | 0.109 |
| Delayed Memory | 92.46 ± 6.14 | 76.7 ± 18.03 | 78.52 ± 18.89 | 76.87 ± 16.01 | 7.54 | <0.001 * | <0.001 * | 0.004 * | 0.003 * | 0.111 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De la Torre, G.G.; Doval, S.; López-Sanz, D.; García-Sedeño, M.; Ramallo, M.A.; Bernal, M.; González-Torre, S. Neurocognitive Impairment in Severe Mental Illness. Comparative study with Spanish Speaking Patients. Brain Sci. 2021, 11, 389. https://doi.org/10.3390/brainsci11030389
De la Torre GG, Doval S, López-Sanz D, García-Sedeño M, Ramallo MA, Bernal M, González-Torre S. Neurocognitive Impairment in Severe Mental Illness. Comparative study with Spanish Speaking Patients. Brain Sciences. 2021; 11(3):389. https://doi.org/10.3390/brainsci11030389
Chicago/Turabian StyleDe la Torre, Gabriel G., Sandra Doval, David López-Sanz, Manuel García-Sedeño, Miguel A. Ramallo, Macarena Bernal, and Sara González-Torre. 2021. "Neurocognitive Impairment in Severe Mental Illness. Comparative study with Spanish Speaking Patients" Brain Sciences 11, no. 3: 389. https://doi.org/10.3390/brainsci11030389
APA StyleDe la Torre, G. G., Doval, S., López-Sanz, D., García-Sedeño, M., Ramallo, M. A., Bernal, M., & González-Torre, S. (2021). Neurocognitive Impairment in Severe Mental Illness. Comparative study with Spanish Speaking Patients. Brain Sciences, 11(3), 389. https://doi.org/10.3390/brainsci11030389