
Developmental Language Disorder: Early Predictors, Age for the Diagnosis, and Diagnostic Tools. A Scoping Review

 ,
, 
 , , ,
, , , 
 ,
,  ,
,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
1.1. Developmental Language Disorder
1.2. Risk Factors and Early Predictors of Poor Language Prognosis
1.3. Effective Tests and Optimal Time to Avoid Diagnostic Bias
1.4. Aims of the Review
2. Methods
2.1. Identifying the Research Question
- Q1.
- Are there early predictors for the identification of DLD?
- Q2.
- What age range is most appropriate for use of screening and diagnostic tools for DLD?
- Q3.
- What tools are effective (in terms of validity, accuracy, and reliability) for the formulation of a diagnosis of DLD in preschool children?
2.2. Source of Data
2.3. Selection Criteria and Data Extraction
2.4. Data synthesis
3. Results
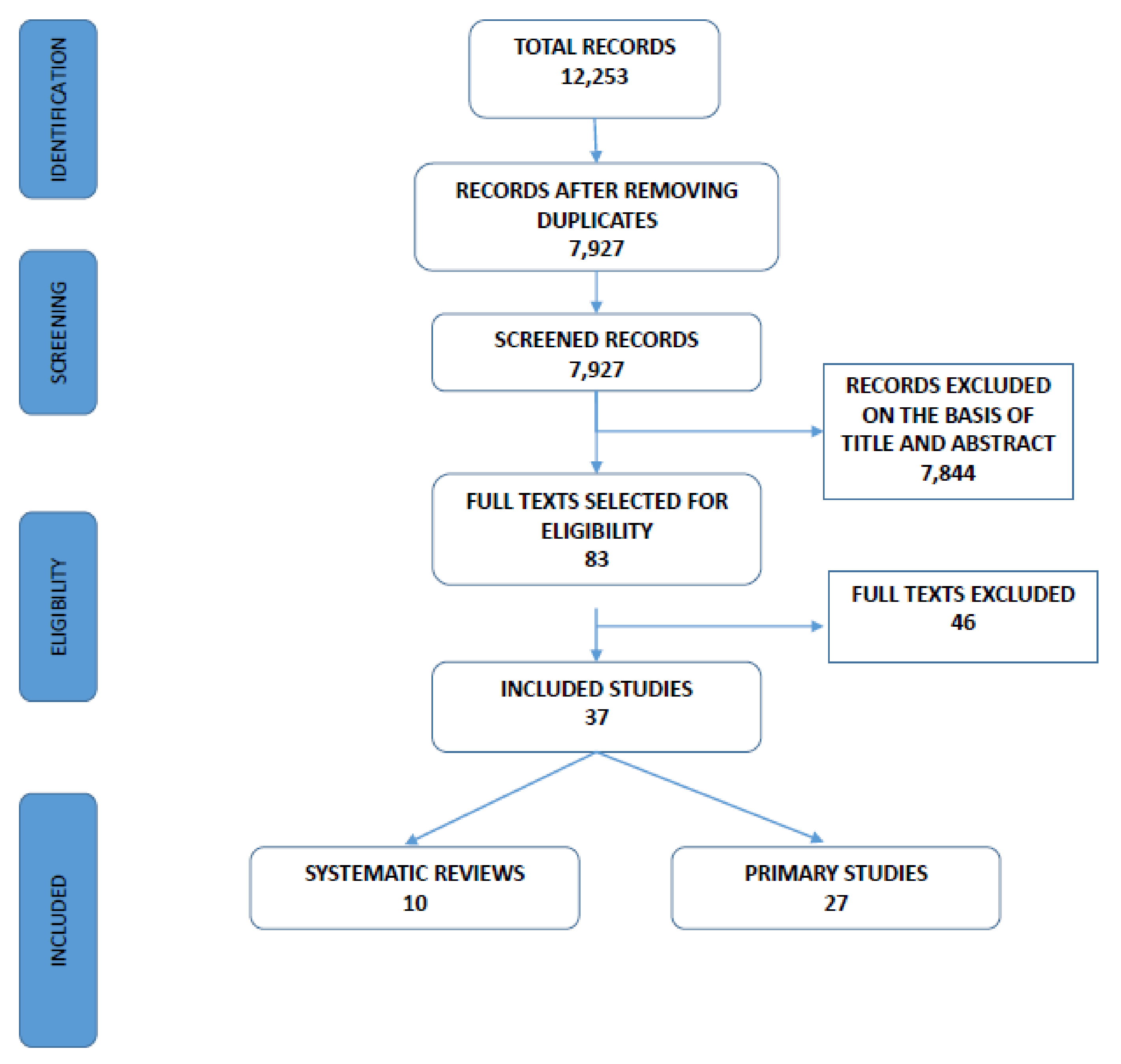
3.1. The Selected Literature
3.1.1. Systematic Reviews
3.1.2. Primary Studies
3.2. Q1: Are There Early Predictors for the Identification of DLD?
3.2.1. Results from the Systematic Reviews
Risk Factors and Early Predictors
Effectiveness of Screening Procedures
3.2.2. Results from the Primary Studies
3.2.3. Q1: Summary
3.3. Q2: What Age Range Is Appropriate for the Use of Screening and Diagnostic Tools for DLD?
3.3.1. Results from the Systematic Reviews
3.3.2. Results from the Primary Studies
3.3.3. Q2: Summary
3.4. Q3: What Tools Are Effective (in Terms of Validity, Accuracy, Reliability) for the Formulation of the Diagnosis of DLD in Preschool Children?
3.4.1. Results from the Systematic Reviews
3.4.2. Results from Primary Studies
3.4.3. Q3: Summary
4. Discussion
4.1. Risk Factors and Early Predictors
4.2. Screening Tools and Early Predictors
4.3. Timely Identification
4.4. Diagnostic Tools
5. Limitations and Future Perspectives
6. Implications for Clinical Practice
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| PubMed Date: 31 December 2020 | |
|---|---|
| Search | Query |
| #15 | #13 AND #14 |
| #14 | systematic[sb] OR meta-analysis[pt] OR meta-analysis as topic[mh] OR meta-analysis[mh] OR meta analy*[tw] OR metanaly*[tw] OR metaanaly*[tw] OR met analy*[tw] OR integrative research[tiab] OR integrative review*[tiab] OR integrative overview*[tiab] OR research integration*[tiab] OR research overview*[tiab] OR collaborative review*[tiab] OR collaborative overview*[tiab] OR systematic review*[tiab] OR technology assessment*[tiab] OR technology overview*[tiab] OR “Technology Assessment, Biomedical”[mh] OR HTA[tiab] OR HTAs[tiab] OR comparative efficacy[tiab] OR comparative effectiveness[tiab] OR outcomes research[tiab] OR indirect comparison*[tiab] OR ((indirect treatment[tiab] OR mixed-treatment[tiab]) AND comparison*[tiab]) OR Embase*[tiab] OR Cinahl*[tiab] OR systematic overview*[tiab] OR methodological overview*[tiab] OR methodologic overview*[tiab] OR methodological review*[tiab] OR methodologic review*[tiab] OR quantitative review*[tiab] OR quantitative overview*[tiab] OR quantitative synthes*[tiab] OR pooled analy*[tiab] OR Cochrane[tiab] OR Medline[tiab] OR Pubmed[tiab] OR Medlars[tiab] OR handsearch*[tiab] OR hand search*[tiab] OR meta-regression*[tiab] OR metaregression*[tiab] OR data synthes*[tiab] OR data extraction[tiab] OR data abstraction*[tiab] OR mantel haenszel[tiab] OR peto[tiab] OR der-simonian[tiab] OR dersimonian[tiab] OR fixed effect*[tiab] |
| #13 | #1 AND #10 AND #11 AND #12 |
| #12 | Child[Mesh] OR Infant[Mesh] OR child*[tiab] OR infant*[tiab] OR baby[tiab] OR babies[tiab] OR toddler*[tiab] OR boy*[tiab] OR girl*[tiab] OR pre-school*[tiab] OR preschool*[tiab] OR kindergarten*[tiab] OR kinder-garten[tiab] OR nursery[tiab] |
| #11 | test*[tiab] OR instrument[tiab] OR judgments[tiab] OR scale[tiab] OR tool*[tiab] OR procedure*[tiab] OR assessment [tiab] OR assessing[tiab] OR vignette*[tiab] OR scenario*[tiab] OR “rating scale”[tiab] OR “rating scales”[tiab] OR “coding manuals”[tiab] OR “coding schemes”[tiab] OR checklist*[tiab] OR interview*[tiab] OR questionnaire*[tiab] |
| #10 | #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 |
| #9 | reliability[tiab] |
| #8 | early identification [tiab] |
| #7 | accuracy[tiab] |
| #6 | “Sensitivity and Specificity”[Mesh] |
| #5 | “Predictive Value of Tests”[Mesh] |
| #4 | “reproducibility of Results” [MESH] |
| #3 | Diagnosis”[Mesh] OR “diagnosis” [Subheading] |
| #2 | diagnosis”[tiab] OR “diagnostic”[tiab] |
| #1 | “Language Disorders”[Mesh] OR “Speech Sound Disorder”[Mesh] OR speech disorder*[tiab] OR speech delay*[tiab] OR speech impair*[tiab] OR language disorder*[tiab] OR language delay*[tiab] OR language impair*[tiab] OR language difficulties[tiab] OR phonological disorder* [tiab] |
Appendix B
| Authors, Year, Reference | Goal of the Review | Study Design (n° of Studies) | Population | Language of Assessment | Language Domain/Task | Test/Assessment Tool |
|---|---|---|---|---|---|---|
| Bettio et al., 2019 [73] Data search: 2013–2017 | Identify: (a) risk factors associated with delays in the development of children’s oral language (b) protective factors that could moderate the effects of risk factors associated with oral language delays | Systematic reviews (n = 2), cohort studies, longitudinal (n = 8), cross-sectional studies (n = 2). | Size of total sample not specified Age = Birth to 8 years | Not specified. Countries where studies were conducted: Finland (1), Ireland (1), Brazil (3), Canada (2), Australia (2), Norway (1), Scotland (1) and USA (1) | Receptive–expressive language (language development in general) | (I) Static risk factors: Male gender, low birth weight, preterm birth, low parental schooling, low socioeconomic status, ≥4 children living in the same household, family history of language delay, father working outside all day, difficult temperament, intracranial hemorrhage, brain injury and persistent otitis media. (II) Dynamic risk factors: Poor quality of communication with the mother, family dynamics, family not reading to the child at home, and problems with the mother’s mental health. |
| Denman et al., 2017 [70] Data search: 1994–2014 | Evaluation of psychometric quality of diagnostic spoken language tests for monolingual English-speaking children | Manuals of tests (n = 12), diagnostic accuracy studies (n = 7) | Size of total sample not specified Age: range 4–12 years | English | Spoken and written language skills including phonemic awareness and pragmatics | Tests assessing language skills across at least two domains of word (semantics), sentence (syntax/morphology) and text (discourse): Assessment of Literacy and Language [ALL]; Comprehensive Assessment of Spoken Language [CASL]; Clinical Evaluation of Language Fundamentals—5th Edition [CELF-5], Clinical Evaluation of Language Fundamentals: Preschool—2nd Edition [CELF:P-2], Diagnostic Evaluation of Language Variance—Norm Referenced [DELV-NR], Illinois Test of Psycholinguistic Abilities—3rd Edition [ITPA-3], Reynell Developmental Language Scales—4th Edition [NRDLS], Oral and Written Language Scales—2nd Edition [OWLS-2], Preschool Language Scales—5th Edition [PLS-5], Test of Early Language Development—3rd Edition [TELD-3], Test of Language Development—Primary: 4th Edition [TOLD-P:4], Woodcock Johnson 4th Edition Oral Language [WJIVOL] |
| Fisher, 2017 [72] Data search: until July 2015 | Analysis of predictors of expressive language outcomes among late talkers | Prospective studies (n = 23), 1 dissertation, 11 personal communications, corresponding to 20 LT samples. | N = 2134 59% boys, 41% girls Age: 18–35 months, with 5 months follow-up assessment | American English, British English, Dutch, Australian English, Finnish, Greek, French, Serbian | Expressive language | Predictors Continuous: expressive vocabulary size, receptive language, phrase speech, socioeconomic status Nominal: gender, family history. |
| Kasper et al., 2011 [68] June–October 2007, updated January and May 2008. | Evaluation of the effectiveness of a screening program, diagnosis and interventions for specific language impairment (SLI). | Screening: Cluster randomized controlled studies (n = 2) | Total sample: N = 10,942 15–24 months with 2 years follow-up period | German | Spontaneous language production (expressive lexicon and morphosyntax) | VTO language screening |
| Law et al., 1998 [64] Data search: 1966–1997 | Evaluation of screening procedures for speech and language delays. | Cross-sectional studies (n = 45) | 0–7 years | English | Receptive–expressive language Articulation | One screen/multiple populations: Fluharty Preschool Language Screening test, Sentence Repetition Screening Test, Northwestern Syntax Screening test, Revised Denver Developmental Screening Test Expressive/Receptive (DDST), Battelle Developmental Inventory Screening Test, Parent Questionnaire with/without comprehension items, Nurses Developmental Screening, Speech and language Screening Questionnaire; WILSTAAR, SKOLD, ELM, Hackney, LDS, Levett-Muir, Rigby Speech Screen, Stevenson Screen, TPSI, Uppsala Language Screen. |
| Law et al., 2000 [65] Data search: 1967–May 1997 | Evaluation of the feasibility of universal screening for speech and language delay | Cross-sectional studies (n = 45) | Sample size not specified Age: 5–70 months | British and American English | Receptive–expressive language | 1. Single screening applied to more than one population: Fluharty Preschool Language Screening Test and Sentence Repetition Screening Test versus Test of Language Development and Test of Auditory Comprehension of Language. 2. Comparison of more than one screening applied to a single population: Fluharty Preschool Language Screening Test, Northwestern Syntax Screening test, Revised Denver developmental Screening Test Expressive/Receptive, Battelle Developmental Inventory Screening Test, Parent Questionnaire with/without comprehension items, Nurses Developmental Screening, Sentence Repetition Screening Test, Speech and Language Screening Questionnaire |
| Maleki Shahmahmood et al., 2016 [71] Data search: 2000–July 2015 | Evaluation of accuracy of language tests/measures for the diagnosis of Speech and Language Impairment. Evaluation of the possibility to identify universal linguistic markers of DLD. | Cross-sectional studies that compare the performance of two or more diagnostic procedures (n = 23) | Total sample: N = 2784 (range 29–454) Preschool age (from 36 months) | 12 studies on English or American English-speaking children, 11 studies on children speaking other languages: Cantonese (3), Italian (3), French (1), Spanish (1), Slovakian (1), Hebrew (1), Persian (1) | -Receptive–expressive language | Studies in English: non-word repetition, experimental test and digit task, language tasks, CNRep, Spelt-P3, NRT, Bus Story, SPELT-P2, GAPS-test, TMT, PS, FVMS, PPVT-III, PPVT-IV, spontaneous language; reference test: clinical assessment by professionals, other tests |
| Nelson et al., 2006 [67] Data search: 1966–Nov. 2004 | Evaluation of screening and interventions for speech and language delay in primary care setting | Case control, cross-sectional, prospective cohort studies, (n = 38) | KQ2a: N = 13,787; KQ2b and 2c: N = 1627. Total sample N = 15,414 CA < 5 years | American English, German, Dutch, Finnish | -Receptive–expressive language | 0–2 years: Early Language Milestone Scale (2), PEDS (1), DDST-II (1), PLASTER (1), CLAMS (1), LDS (3), DP-II (1), BINS(1); 2–3 years: PLC (1), Structured Screening Test (1), Levett–Muir Language Screening Test (1), Fluharty Preschool Speech and Language Screening Test (2), SKOLD (1), Hackney Early Language Screening Test (2), Early Language Milestone Scale (1); 3–5 years: Fluharty Preschool Speech and Language Screening Test (1), TEEM (1), SRST (1) |
| Sim et al., 2019 [69] Data search: Medline 1946–March 2017, Embase 1947–2017, EBSCO CINAHL 1983–2017, PsycInfo 1914–2017 and ERIC 1959–2017 | Evaluation of the predictive validity of screening tools for language difficulties used in a community preschool setting | Prospective cohort studies (n = 5) | Total sample = 9267 Age: 2–6 years | English (N = 2), German (N = 1), not specified for the remaining studies (probably English as they use English tests) | -Receptive–expressive language -General cognitive development | MB-CDI: UK Short Form (MB-CDI: UKSF) or Toddler form (ELFRA-2); Parent Report of Children’s Abilities (PARCA); Language Development Survey (LDS); Reynell Developmental Language Scales (RDLS); Sprachentwicklungs test (for 2-year-olds) SETK-2; nonverbal subscale of the Munchener Funktionelle Entwicklungsdiagnostik, hearing screen ECHO-SCREEN Plus-T; Productive vocabulary, syntax and morphology; Parent reports; Sure Start Language Measure (SSLM); Strengths and Difficulties Questionnaire (SDQ); Vocabulary; Development and Wellbeing Assessment (DAWBA); Griffiths Mental Development Scale-Extended Revised (GMDS-ER); New Reynell Developmental Language Scales (NRDLS); General Language Screen (GLS); Developmental Profile II (DPII); Receptive and expressive language. |
| Wallace et al., 2015 [66] Data search: Jan. 2004–July 2014 | Evaluation of efficacy of screening and treatment for speech and language delays and disorders (update of Nelson, 2006) | Longitudinal studies (n = 24) (KQ1: 0 studies; KQ2a: 24 studies; KQ2b, KQ2c, KQ2d, KQ3, KQ4: 0 studies). | Total sample: 7823 7–72 months (7–54 screening by parents, 18–72 screening by clinicians) | KQ2a: American English, German, Swedish, Spanish | -Receptive–expressive language -Gestures -Sounds -Object use | KQ2A: Tools compiled by parents: PLS-3 o PLS-4; language observation; ELFRA-2 words and sentences (SETK-2); DP II, EAT, RDLS, BPVS; language inventory RAPT; toddlers Inventory CSBS; clinical assessment on MSEL; MLU, RDLS; parent questionnaires; SLP on language samples; REEL word screening; Tools used by clinicians: Battelle Developmental Inventory Screening test; Brigance Screening; Davis Observation Checklist; Denver test of articulation; Denver screening; Early Profile of verbal concepts PLS-4; Fluharty Preschool Language Screening test; FPSLST Language and Articulation; Northwestern; SKOLD; sentence repetition; structured screening test; Hackney, RDLS; SLP. |
| Authors, Year, Reference | Study Design, Setting | Participants | Age (Months) | Language of Assessment | Language Domain/Task | Test/Assessment Tool |
|---|---|---|---|---|---|---|
| Azab and Ashour, 2015 [91] | Observational, cross-sectional; clinical setting | N = 60 (30 DLD + 30 TD) | 48–70 | Arabic | -Prosody | -Protocol of prosodic assessment; Clinical criteria: -Arabic language test |
| Benavides et al., 2018 [99] | Observational, cross-sectional; clinical setting | N = 770 (184 DLD + 586 TD) 4 y = 73 DLD + 189 TD 5 y = 63 DLD + 245 TD 6 y = 48 DLD + 152 TD | 48–72 | Spanish (Mexico) | -Expressive grammar | Tamiz de Problemas de Lenguaje (Morphology task and sentence repetition task) Clinical criteria: -Subtests of BESA = Bilingual English–-Spanish Assessment. -CELF-4 = Clinical Evaluation of Language Fundamentals -MLU = mean length of utterance |
| Bello et al., 2018 [86] | Observational, longitudinal; clinical setting | N = 35 LT | T0: 29 T1: 34 | Italian | - Receptive and expressive lexicon -Socio-conversational abilities | Clinical criteria: -MacArthur–Bates Infant and Toddler Communication Development Inventories. (Italian version of the MB-CDI Short and Long Form) -Parole in Gioco-PiNG, Test of noun and predicates comprehension and production -Questionnaire of socio-conversational abilities- ASCB |
| Chilosi et al., 2019 [88] | Observational, longitudinal; clinical setting | N = 50 LT | T0:28 T1:36 T2:48 | Italian | -Expressive lexicon -Expressive grammar -Syntactic comprehension | Clinical criteria: -MacArthur–Bates Infant and Toddler Communication Development Inventories. (Italian version of the MB-CDI) -Grid for the Analysis of Spontaneous Speech (GASS). -COVER test of syntactic comprehension |
| Collisson et al., 2015 [93] | Experimental, cross-sectional; clinical setting | N = 54 (16 DLD + 38 TD) | 42–58 | English | -Receptive and expressive lexicon -Expressive grammar | Clinical criteria: -CELF-P2 = Clinical Evaluation of Language Fundamentals -Preschool 2 -PPVT-4 = The Peabody Picture Vocabulary Test—Fourth Edition |
| Conway et al., 2018 [78] | Observational, longitudinal; home setting | N = 197 former LT | T0 24 T1:36 T2:48 | Australian English | -Receptive and expressive lexicon -Receptive and expressive grammar | Maternal speech in mother–infant interaction Clinical criteria: -The Preschool Language Scale (PLS-4) -The Clinical Evaluation of Language Fundamentals Preschool Edition (CELF-P2) |
| Eisenberg et al., 2019 [98] | Observational, cross-sectional; setting non specified | N = 62 (31 LT and 31 TD) | 36 | American English | -Expressive lexicon -Expressive grammar | -Fluharty Preschool Speech and Language Screening Test–2ed Clinical criteria: -SPELT-P2 = Structured Photographic Expressive Language Test–Preschool, Second Edition. -MLUm = mean length of utterance in morphemes. -IPSyn = Index of Productive Syntax. -FVMC = finite verb morphology composite. |
| Gudmundsson, 2015 [95] | Observational, cross-sectional; home + clinical setting | N = 1132 (general population) | 15–38 | Icelandic | -Receptive and expressive language | Toddler Language and Motor Questionnaire |
| Hadley et al., 2016 [85] | Observational, longitudinal; clinical setting | N = 45 TD | T0: 21 T1: 24 T2: 27 T3: 30 | American English | -Expressive lexicon -Expressive grammar | -Word and sentences version of MB-CDI (21, 24, 27, 30 months). -Recordings of spontaneous language (21–30 months) obtaining measures of expressive language abilities: total length of complete and interpretable utterance, number of word types, mean length of utterance in morphemes (24 and 30 months), measures of vocabulary as number of different nouns and verbs |
| Haman et al., 2017 [74] | Observational, cross-sectional; school setting | N = 639 TD | 36–82 | Lithuanian, isiXhosa, Finnish, Afrikaans, British English, South African English, German, Luxembourgish, Norwegian, Swedish, Catalan, Italian, Hebrew, Polish, Serbian, Slovak and Turkish | -Expressive lexicon | Cross-linguistic lexical tasks (LITMUS-CLT) |
| Hsu and Iyer, 2016 [75] | Observational, longitudinal; setting not specified | N = 1064 general population | T0: 15 T1: 36 T2: 53 | American English | -Gesture production -Receptive and expressive lexicon | -MacArthur–Bates Communicative Development Inventory (MB-CDI) Clinical criteria: -Reynell Development Language Scales (RDLS, 3 years) -Preschool language scale-3 (PLS-3, 4.5 years) |
| Kademann et al., 2015 [87] | Observational, longitudinal; clinical setting | N = 86 (46 LT + 40 TD) | T0: 24 T1: 36 T2: 54 | German | -Receptive and expressive lexicon -Expressive grammar -Phonology - Narrative production -Metaphonology -Verbal memory -Lexical access -RAN (rapid automatized naming) | Clinical criteria: -SETK-4-5: sentence comprehension (VS), morphological production (plural formation—MR), sentence memory (SG) -Subtest Vocabulary of K-ABC battery |
| Kim et al., 2016 [84] | Observational, longitudinal; clinical setting | N = 206 with delayed language development (79 DLD + 19 TD + other pathologies) | 29.7 (average age) | Korean | -Receptive and expressive lexicon -Receptive and expressive grammar | -Korean version of Ages and Stages Questionnaire (K-ASQ), -MacArthur–Bates Communicative Development Inventories short Korean version (MB- CDI-K) Clinical criteria: -SELSI (Sequenced Language Scale for Infants), -PRES (Preschool Receptive–expressive Language Scale) |
| Klem et al., 2015 [96] | Observational, longitudinal; school setting | 216 TD monolingual children | T0: 51 T1: 63 T2: 75 | Norwegian | -Sentence repetition -Expressive grammar | -Sentence repetition test -‘Grammatic Closure’ from Illinois Test of Psycholinguistic Abilities (ITPA) |
| Lüke et al., 2017 [79] | Experimental, longitudinal; clinical setting | N = 59 TD Recruitment strategy emphasized families in which a sibling or one of the parents had a history of language impairment. | T0: 12 T1: 24 | German | -Gesture comprehension and production -Receptive and expressive lexicon -Receptive and expressive grammar | -Analysis of gestural behavior (pointing) at 1;0 year in a semi-natural setting with their caregivers Clinical criteria: -SETK-2 -FRA-KIS |
| Lüke et al., 2020 [80] | Observational, longitudinal (14 sessions from 1 to 6 years); clinical setting | N = 42 children (TD: N = 32; LD: N = 10 (at 24 months); of children with LD, N = 2 with DLD from age 3. Same recruitment strategy as in [79]. | T0: 1;0; T1: 1;2; T2: 1;4; T3: 1;6; T4: 1;9; T5: 2;0; T6: 2;6; T7: 3;0; T8: 3;6; T9: 4;0; T10: 4;6; T11: 5;0; T12: 5;6; T13: 6;0. | German | -Gesture production and comprehension -Receptive and expressive lexicon -Receptive and expressive grammar -Sentence repetition | -Analysis of gestural behavior (pointing) at 1;0 year in a semi-natural setting with their caregivers -Iconic gesture test to assess comprehension of iconic gestures at 3;0, 4;0 and 5;0 years Clinical criteria: -German version of the MB-CDI (at 24 months) -ELFRA (at 12 months) -FRAKIS and SETK-2 (at 24 and 30 months) -SETK 3-5 and PDSS (at 36 months) -P-ITPA (at 48, 60, 72 months) -TROG-D (at 60, 72 months) and receptive language |
| Marini et al., 2017 [76] | Observational, longitudinal; clinical setting | N = 293 (260 TLD + 33 LT) | T0: 32 T1: 41 | Italian | -Non-word repetition -Expressive lexicon -Phonology/Articulation -Receptive and expressive grammar -Narrative production | -Non-word repetition -Language Development Survey (LDS) -Home Literacy Environment Questionnaire (HLEQ) Clinical criteria: -Batteria per la Valutazione del Linguaggio in Bambini dai 4 ai 12 anni (BVL_4-12) |
| Marini et al., 2020 [94] | Observational, cross-sectional; clinical setting | N = 40 (TD: N = 24; DLD: N = 16) | 64 | Italian | -Phonology/Articulation -Receptive and expressive grammar -Narrative production | Inhibition test (NEPSY-II) Clinical criteria: -Batteria per la Valutazione del Linguaggio in Bambini dai 4 ai 12 anni (BVL_4-12) |
| Morgan et al., 2020 [82] | Observational, longitudinal; clinical/home setting | N = 408 (159 LT + 249 TD) | T0: 18–21 T1: 24 T2: 36 | American English | -Communication and symbolic abilities -Receptive and expressive lexicon | -Communication and Symbolic Behavior Scales (CSBS) -Language Development Survey (LDS) Clinical criteria: -Mullen Scales of Early Learning (MSEL) |
| Nayeb et al., 2019 [89] | Observational, longitudinal; clinical setting | N = 105 (11 DLD + 94 TD) | T0: 30 T1: 36 | Swedish | -Word combination | -Evaluation of word combination in child speech -Comprehension test; Clinical criteria: Reynell Development Language Scales- RDLS-III (Swedish); Evaluation of spontaneous communication |
| Puglisi et al., 2020 [100] | Observational, cross-sectional; school setting | Study 1: 754 TD Study 2: 100 (92 TD e 8 LD) | Study 1: 51–65 Study 2: 60–80 | Brazilian-Portuguese | -Phonology -Expressive lexicon -Expressive grammar | -Screening for Identification of Oral Language Difficulties by Preschool Teachers (SIOLD) (questionnaire on phonology, vocabulary, grammar). Clinical criteria: -Expressive Vocabulary Test- Short -Test for Reception of Grammar Version 2—Short -The Brazilian Children’s Test of Pseudoword Repetition |
| Quam et al., 2020 [90] | Observational, cross-sectional; school setting | N = 52 (26 DLD + 26 TD) | 48–70 | American English | -Sound discrimination -Receptive and Expressive Lexicon | -Computerized sound discrimination task Clinical criterion: -Peabody Picture Vocabulary Test, Fourth Edition (PPVT-4). -Structured Photographic Expressive Language Test—Preschool: 2nd Edition (SPELT-P2) |
| Sahli and Belgin, 2017 [97] | Observational, cross-sectional; clinical setting | N = 1320 (1044 TD; 276 DLD) | 0–95 | Turkish, English | -Auditory Comprehension -Expressive Communication | Clinical criteria: -Preschool language Scale 5 ed. (PLS-5) -Preschool language Scale 4 ed. (PLS-4) |
| Sansavini et al., 2019 [81] | Observational, longitudinal; Clinical setting | N = 110 infants (70 American: -29 TD −41 siblings with no ASD of a child with ASD: 28 no LD, 13 LD; 40 Italian infants: −20 Full Term −20 Extremely preterm: 11 no LD, 9 LD) | T0: 18 T1: 24 T2: 30 T3: 36 | American English Italian | -Gesture production -Expressive lexicon | Analysis of deictic, conventional, and representational gestures during mother–infant play session at 18 months Clinical criteria: -MB-CDI-WS long form (American and Italian versions) at 18, 24, 30, 36 months -Mullen Scales of Early Learning (Receptive and/or Expressive Language subscales, American version) |
| Suttora et al., 2020 [77] | Observational, cross-sectional; clinical setting | N = 61 LT (26 Low-risk preterm; 35 Full Term) | 30 | Italian | -Expressive lexicon -Expressive grammar | -Parental and child speech collected during a video-recorded 10-min parent–child shared book reading session. Measures: Word types, word tokens, MLU Clinical criteria: -MacArthur–Bates Communicative Development Inventories (MB-CDI) Short Form (Italian version) |
| Tomas et al., 2015 [92] | Observational, cross-sectional; clinical setting | N = 30 DLD | 54–71 | Australian English | -Expressive grammar -Non-word repetition | -Question–answer elicitations of the 30 target items, presented along with picture props Clinical criteria: -PLS—Preschool Language Scale -CELF—Clinical Evaluation of Language Function -articulatory screening (non-word repetition) |
| Vehkavuori and Stolt, 2018 [83] | Observational, cross-sectional; home/clinical setting | N = 78 TLD | 24 | Finnish | -Communication and symbolic abilities -Receptive and expressive lexicon | -MacArthur Communicative Development Inventories (FinCDI-SF) -Communication and Symbolic Behavior Scales, Developmental Profile, Infant-Toddler Checklist (FinCSBS) Clinical criteria: -Reynell Developmental Language Scales III (Finnish version) |
References
- Kuhl, P. Brain mechanisms in early language acquisition. Neuron 2010, 67, 713–727. [Google Scholar] [CrossRef] [Green Version]
- Perani, D.; Saccuman, M.C.; Scifo, P.; Anwander, A.; Spada, D.; Baldoli, C.; Poloniato, A.; Lohmann, G.; Friederici, A.D. Neural language networks at birth. Proc. Natl. Acad. Sci. USA 2011, 20, 16056–16061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riva, V.; Cantiani, C.; Dionne, G.; Marini, A.; Mascheretti, S.; Molteni, M.; Marino, C. Working memory mediates the effects of gestational age at birth on expressive language development in children. Neuropsychology 2017, 31, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Caselli, M.C.; Rinaldi, P.; Stefanini, S.; Volterra, V. Early action and gesture ‘‘vocabulary’’ and its relation with word comprehension and production. Child Dev. 2012, 83, 526–542. [Google Scholar] [CrossRef] [PubMed]
- Fenson, L.; Dale, P.S.; Reznick, J.S.; Bates, E.; Thal, D.; Pethick, S. Variability in early communicative development. Monogr. Soc. Res. Child Dev. 1994, 59, 1–173. [Google Scholar] [CrossRef]
- Sansavini, A.; Bello, A.; Guarini, A.; Savini, S.; Stefanini, S.; Caselli, M.C. Early development of gestures, object-related-actions, word comprehension and word production and their relationships in Italian infants: A longitudinal study. Gesture 2010, 10, 52–85. [Google Scholar] [CrossRef]
- Bavin, E.L.; Prior, M.; Reilly, S.; Bretherton, L.; Williams, J.; Eadie, P.; Barrett, Y.; Ukoumunne, O.C. The early language in Victoria study: Predicting vocabulary at age one and two years from gesture and object use. J. Child Lang. 2008, 35, 687–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capirci, O.; Volterra, V. Gesture and speech. The emergence and development of a strong and changing partnership. Gesture 2008, 8, 22–44. [Google Scholar] [CrossRef]
- Zubrick, S.R.; Taylor, C.L.; Rice, M.L.; Slegers, D.W. Late language emergence at 24 months: An epidemiological study of prevalence, predictors, and covariates. J. Speech Lang. Hear. Res. 2007, 50, 1562–1592. [Google Scholar] [CrossRef]
- Guasti, M.T. Language Acquisition: The Growth of Grammar; The MIT Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Domsch, C.; Richels, C.; Saldana, M.; Coleman, C.; Wimberly, C.; Maxwell, L. Narrative skill and syntactic complexity in school-age children with and without late language emergence. Int. J. Lang. Commun. Disord. 2012, 47, 197–207. [Google Scholar] [CrossRef]
- Hawa, V.V.; Spanoudis, G. Toddlers with delayed expressive language: An overview of the characteristics, risk factors and language outcomes. Res. Dev. Disabil. 2014, 35, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Rescorla, L. Late talkers: Do good predictors of outcome exist? Dev. Disabil. Res. Rev. 2011, 17, 141–150. [Google Scholar] [CrossRef]
- Buschmann, A.; Jooss, B.; Rupp, A.; Dockter, S.; Blaschtikowitz, H.; Heggen, I.; Pietz, J. Children with developmental language delay at 24 months of age: Results of a diagnostic workup. Dev. Med. Child Neurol. 2008, 50, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Desmarais, C.; Sylvestre, A.; Meyer, F.; Bairati, I.; Rouleau, N. Systematic review of the literature on characteristics of late-talking toddlers. Int. J. Lang. Commun. Disord. 2008, 43, 361–389. [Google Scholar] [CrossRef] [PubMed]
- Leonard, L.B. Is expressive language disorder an accurate diagnostic category? Am. J. Speech Lang. Pathol. 2009, 18, 115–123. [Google Scholar] [CrossRef] [Green Version]
- Rescorla, L. Language and reading outcomes to age 9 in late-talking toddlers. J. Speech Lang. Hear. Res. 2002, 45, 360–371. [Google Scholar] [CrossRef]
- Rescorla, L. Age 17 language and reading outcomes in late-talking toddlers: Support for a dimensional perspective on language delay. J. Speech Lang. Hear. Res. 2009, 52, 16–30. [Google Scholar] [CrossRef]
- Snowling, M.J.; Duff, F.J.; Nash, H.M.; Hulme, C. Language profiles and literacy outcomes of children with resolving, emerging, or persisting language impairments. J. Child Psychol. Psychiatry 2016, 57, 1360–1369. [Google Scholar] [CrossRef]
- Zambrana, I.M.; Pons, F.; Eadie, P.; Ystrom, E. Trajectories of language delay from age 3 to 5: Persistence, recovery and late onset. Int. J. Lang. Commun. Disord. 2014, 49, 304–316. [Google Scholar] [CrossRef]
- APA–American Psychiatric Association. DSM-5 Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Bishop, D.M.V.; Snowling, M.G.; Thompson, P.A.; Greenhalgh, T. The Catalise-2 Consortium. Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J. Child Psychol. Psychiatry Allied Discip. 2017, 58, 1068–1080. [Google Scholar] [CrossRef]
- Lum, J.A.G.; Conti-Ramsden, G.; Page, D.; Ullman, M.T. Working, declarative and procedural memory in specific language impairment. Cortex 2012, 48, 1138–1154. [Google Scholar] [CrossRef] [PubMed]
- Finlay, J.C.S.; McPhillips, M. Comorbid motor deficits in a clinical sample of children with specific language impairment. Res. Dev. Disabil. 2013, 34, 2533–2542. [Google Scholar] [CrossRef]
- Duinmeijer, I.; De Jong, J.; Scheper, A. Narrative abilities, memory and attention in children with a Specific Language Impairment. Int. J. Lang. Commun. Disord. 2012, 47, 542–555. [Google Scholar] [CrossRef] [PubMed]
- Pauls, L.J.; Archibald, L.M.D. Executive functions in children with specific language impairment: A meta-analysis. J. Speech Lang. Hear. Res. 2016, 59, 1074–1086. [Google Scholar] [CrossRef] [PubMed]
- Kapa, L.L.; Plante, E. Executive function in SLI: Recent advances and future directions. Curr. Dev. Disord. Rep. 2015, 2, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Marini, A.; Gentili, C.; Molteni, M.; Fabbro, F. Differential verbal working memory effects on linguistic production in children with Specific Language Impairment. Res. Dev. Disabil. 2014, 35, 3534–3542. [Google Scholar] [CrossRef]
- Reilly, S.; Bishop, D.V.M.; Tomblin, B. Terminological debate over language impairment in children: Response forward movement and sticking points. Int. J. Lang. Commun. Disord. 2014, 49, 452–462. [Google Scholar] [CrossRef]
- Reilly, S.; Tomblin, B.; Law, J.; Mc Kean, C.; Mensah, F.K.; Morgan, A.; Goldfeld, S.; Nicholson, J.M.; Wake, M. Specific Language Impairment: A convenient label for whom? Int. J. Lang. Commun. Disord. 2014, 49, 416–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomblin, J.B.; Zhang, X.; Buckwalter, P.; O’Brien, M. The stability of Primary Language Disorder: Four years after kindergarten diagnosis. J. Speech Lang. Hear. Res. 2003, 46, 1283–1296. [Google Scholar] [CrossRef]
- Communication & Language Acquisition Studies in Typical & Atypical Populations–CLASTA; Federazione Logopedisti Italiani–FLI (Eds.) Consensus Conference sul Disturbo Primario del Linguaggio; CLASTA: Roma, Italy, 2019; pp. 1–58. Available online: https://www.disturboprimariolinguaggio.it/wp-content/uploads/2019/11/Documento-Finale-Consensus-Conference-2.pdf (accessed on 6 April 2021).
- Rinaldi, S.; Caselli, M.C.; Cofelice, V.; D’Amico, S.; De Cagno, A.G.; Della Corte, G.; Di Martino, M.V.; Di Costanzo, B.; Levorato, M.C.; Penge, R.; et al. Efficacy of the Treatment of Developmental Language Disorder: A Systematic Review. Brain Sci. 2021, 11, 407. [Google Scholar] [CrossRef]
- Arosio, F.; Pagliarini, E.; Perugini, M.; Barbieri, L.; Guasti, M.T. Morphosyntax and logical abilities in Italian poor readers: The problem of SLI misidentification. First Lang. 2016, 36, 295–315. [Google Scholar] [CrossRef]
- Arosio, F.; Foppolo, F.; Pagliarini, E.; Perugini, M.; Guasti, M.T. Semantic and Pragmatic abilities can be spared in Italian children with SLI. Lang. Learn. Dev. 2017, 13, 418–429. [Google Scholar] [CrossRef]
- Leonard, L.B. Children with Specific Language Impairment; MIT Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Rapin, I. Language heterogeneity and regression in the autism spectrum disorders—Overlaps with other childhood language regression syndromes. Clin. Neurosci. Res. 2006, 6, 209–218. [Google Scholar] [CrossRef]
- Cantiani, C.; Lorusso, M.L.; Perego, P.; Molteni, M.; Guasti, M.T. Developmental dyslexia with and without language impairment: ERPs reveal qualitative differences in morphosyntactic processing. Dev. Neuropsychol. 2015, 40, 291–312. [Google Scholar] [CrossRef] [PubMed]
- Chilosi, A.M.; Brizzolara, D.; Lami, L.; Pizzoli, C.; Gasperini, F.; Pecini, C.; Cipriani, P.; Zoccolotti, P. Reading and spelling disabilities in children with and without a history of early language delay: A neuropsychological and linguistic study. Child Neuropsychol. 2009, 15, 582–604. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; St Clair, M.C.; Pickles, A.; Durkin, K. Developmental trajectories of verbal and nonverbal skills in individuals with a history of Specific Language Impairment: From childhood to adolescence. J. Speech Lang. Hear. Res. 2012, 55, 1716–1735. [Google Scholar] [CrossRef]
- Durkin, K.; Mok, P.L.H.; Conti-Ramsden, G. Severity of Specific Language Impairment predicts delayed development in number skills. Front. Psychol. 2013, 4, 581. [Google Scholar] [CrossRef] [Green Version]
- Catts, H.W.; Fey, M.E.; Tomblin, J.B.; Zhang, X. A longitudinal investigation of reading out-comes in children with language impairments. J. Speech Lang. Hear. Res. 2002, 45, 1142–1157. [Google Scholar] [CrossRef] [Green Version]
- Tomblin, J.B.; Zhang, X.; Buckwalter, P.; Catts, H. The association of reading disability, behavioral disorders, and language impairment among second-grade children. J. Child Psychol. Psychiatry 2000, 41, 473–482. [Google Scholar] [CrossRef]
- Clegg, J.; Hollis, C.; Mawhood, L.; Rutter, M. Developmental language disorders--a follow-up in later adult life. Cognitive, language and psychosocial outcomes. J. Child Psychol. Psychiatry 2005, 46, 128–149. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Mok, P.L.; Pickles, A.; Durkin, K. Adolescents with a history of Specific Language Impairment (SLI): Strengths and difficulties in social, emotional and behavioral functioning. Res. Dev. Disabil. 2013, 34, 4161–4169. [Google Scholar] [CrossRef] [PubMed]
- Snowling, M.J.; Bishop, D.V.M.; Stothard, S.E.; Chipchase, B.; Kaplan, C. Psychosocial outcomes at 15 years of children with a preschool history of speech-language impairment. J. Child Psychol. Psychiatry 2006, 47, 759–765. [Google Scholar] [CrossRef] [PubMed]
- St Clair, M.; Pickles, A.; Durkin, K.; Conti-Ramsden, G. A longitudinal study of behavioral, emotional and social difficulties in individuals with a history of Specific Language Impairment (SLI). J. Commun. Disord. 2011, 44, 186–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stothard, S.E.; Snowling, M.J.; Bishop, D.V.M.; Chipchase, B.B.; Kaplan, C.A. Language-impaired preschoolers: A follow-up into adolescence. J. Speech Lang. Hear. Res. 1998, 41, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Tomblin, J.B. Validating diagnostic standards for Specific Language Impairment using adolescent outcomes. In Understanding Developmental Language Disorders: From Theory to Practice; Norbury, C.F., Tomblin, J.B., Bishop, D.V.M., Eds.; Psychology Press: New York, NY, USA, 2008; pp. 93–114. [Google Scholar]
- Spaulding, T.J.; Plante, E.; Farinella, K.A. Eligibility criteria for language impairment: Is the low end of normal always appropriate? Lang. Speech Hear. Serv. Sch. 2006, 37, 61–72. [Google Scholar] [CrossRef]
- Sansavini, A.; Guarini, A.; Justice, L.M.; Savini, S.; Broccoli, S.; Alessandroni, R.; Faldella, G. Does preterm birth increase a child’s risk for language impairment? Early Hum. Dev. 2010, 86, 765–772. [Google Scholar] [CrossRef]
- Marini, A.; Tavano, A.; Fabbro, F. Assessment of linguistic abilities in Italian children with Specific Language Impairment. Neuropsychologia 2008, 46, 2816–2823. [Google Scholar] [CrossRef] [PubMed]
- Aram, D.M.; Morris, R.; Hall, N.E. Clinical and research congruence in identifying children with Specific Language Impairment. J. Speech Hear. Res. 1993, 36, 580–591. [Google Scholar] [CrossRef]
- Bishop, D.M.V. Is Specific Language Impairment a valid diagnostic category? Genetic and psycholinguistic evidence. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1994, 346, 105–111. [Google Scholar] [CrossRef]
- Cole, K.N.; Schwartz, I.S.; Notari, A.R.; Dale, P.S.; Mills, P.E. Examination of the stability of two methods of defining Specific Language Impairment. Appl. Psycholinguist. 1995, 16, 103–123. [Google Scholar] [CrossRef]
- Lahey, M. Who shall be called language disordered? Some reflections and one perspective. J. Speech Hear. Disord. 1990, 55, 612–620. [Google Scholar] [CrossRef]
- Tallal, P.; Curtiss, S.; Kaplan, R. The San Diego longitudinal study: Evaluating the outcomes of preschool impairment in language development. In International Perspectives on Communication Disorders; Gerber, S.E., Mencher, G.T., Eds.; Gallaudet University Press: Washington, DC, USA, 1988; pp. 86–126. [Google Scholar]
- Whitehurst, G.J.; Fischel, J.E. Practitioner review: Early developmental language delay: What, if anything, should the clinician do about it? J. Child Psychol. Psychiatry 1994, 35, 613–648. [Google Scholar] [CrossRef] [PubMed]
- Candiani, G.; Colombo, C.; Daghini, R.; Magrini, N.; Mosconi, P.; Nonino, F.; Satolli, R. Manuale Metodologico: Come Organizzare una Conferenza di Consenso (Engl. Transl: Methodological Manual: How to Organize a Consensus Conference); Istituto Superiore di Sanità, Sistema Nazionale Linee Guida (SNLG): Roma, Italy, 2013; Available online: https://www.psy.it/wp-content/uploads/2018/02/Manuale-Metodologico-Consensus.pdf (accessed on 6 April 2021).
- De Houwer, A. Bilingual First Language Acquisition; Multilingual Matter: Toronto, ON, Canada, 2009. [Google Scholar]
- Paradis, J.; Genesee, F.; Crago, M.B. Dual Language Development and Disorders. A Handbook on Bilingualism and Second Language Learning, 2nd ed.; Paul H. Brookes: Baltimore, MD, USA, 2011. [Google Scholar]
- Marini, A.; Sperindé, P.; Ruta, I.; Savegnago, C.; Avanzini, F. Linguistic skills in bilingual children with Developmental Language Disorders: A pilot study. Front. Psychol. 2019, 10, 493. [Google Scholar] [CrossRef] [PubMed]
- Harrison, L.J.; McLeod, S. Risk and protective factors associated with speech and language impairment in a nationally representative sample of 4- and 5-year-old children. J. Speech Lang. Hear. Res. 2010, 53, 508–529. [Google Scholar] [CrossRef]
- Law, J.; Boyle, J.; Harris, F.; Harkness, A.; Nye, C. Screening for speech and language delay: A systematic review of the literature. Health Technol. Assess. 1998, 2, 1–184. [Google Scholar] [CrossRef] [Green Version]
- Law, J.; Boyle, J.; Harris, F.; Harkness, A.; Nye, C. Prevalence and natural history of primary speech and language delay: Findings from a systematic review of the literature. Int. J. Lang. Commun. Disord. 2000, 35, 165–188. [Google Scholar] [CrossRef] [PubMed]
- Wallace, I.F.; Berkman, N.D.; Watson, L.R.; Coyne-Beasley, T.; Wood, C.T.; Cullen, K.; Lohr, K.N. Screening for Speech and Language Delay in Children 5 Years Old and Younger: A Systematic Review. Pediatrics 2015, 136, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Nelson, H.D.; Nygren, P.; Walker, M.; Panoscha, R. Screening for Speech and Language Delay in Preschool Children: Systematic Evidence Review for the US Preventive Services Task Force. Pediatrics 2006, 117, 298–319. [Google Scholar] [CrossRef] [Green Version]
- Kasper, J.; Kreis, J.; Scheibler, F.; Möller, D.; Skipka, G.; Lange, S.; von dem Knesebeck, O. Population-Based Screening of Children for Specific Speech and Language Impairment in Germany: A Systematic Review. Folia Phoniatr. Logop. 2011, 63, 247–263. [Google Scholar] [CrossRef]
- Sim, F.; Thompson, L.; Marryat, L.; Ramparsad, N.; Wilson, P. Predictive validity of preschool screening tools for language and behavioural difficulties: A PRISMA systematic review. PLoS ONE 2019, 14, e0211409. [Google Scholar] [CrossRef]
- Denman, D.; Speyer, R.; Munro, N.; Pearce, W.M.; Chen, Y.-W.; Cordier, R. Psychometric properties of language assessments for children aged 4–12 years: A systematic review. Front. Psychol. 2017, 8, 1515. [Google Scholar] [CrossRef] [PubMed]
- Maleki Shahmahmood, T.; Jalaie, S.H.; Soleymani, Z.; Haresabadi, F.; Nemati, P. A systematic review on diagnostic procedures for specific language impairment: The sensitivity and specificity issues. J. Res. Med. Sci. 2016, 21–67. [Google Scholar] [CrossRef]
- Fisher, E.L. A systematic review and meta-analysis of predictors of expressive-language outcomes among late talkers. J. Speech Lang. Hear. Res. 2017, 60, 2935–2948. [Google Scholar] [CrossRef] [PubMed]
- Bettio, C.D.B.; Bazon, M.R.; Schmidt, A. Risk and protective factors for language development delay. Psicol. Estud. 2019, 24, e41889. [Google Scholar] [CrossRef]
- Haman, E.; Luniewska, M.; Hansen, P.; Simonsen, H.G.; Chiat, S.; Bjekic, J.; Blažienė, A.; Chyl, K.; Dabašinskienė, I.; De Abreu, P.E.; et al. Noun and verb knowledge in monolingual preschool children across 17 languages: Data from cross-linguistic lexical tasks (LITMUS-CLT). Clin. Linguist. Phon. 2017, 31, 818–843. [Google Scholar] [CrossRef] [Green Version]
- Hsu, H.C.; Iyer, S.N. Early gesture, early vocabulary, and risk of language impairment in preschoolers. Res. Dev. Disabil. 2016, 57, 201–210. [Google Scholar] [CrossRef]
- Marini, A.; Ruffino, M.; Sali, M.E.; Molteni, M. The role of phonological working memory and environmental factors in lexical development in Italian-speaking late talkers: A one year follow up study. J. Speech Lang. Hear. Res. 2017, 60, 3462–3473. [Google Scholar] [CrossRef]
- Suttora, C.; Guarini, A.; Zuccarini, M.; Aceti, A.; Corvaglia, L.; Sansavini, A. Speech and language skills of low-risk preterm and full-term late-talkers: The role of child factors and parent input. Int. J. Environ. Res. Public Health 2020, 17, 7684. [Google Scholar] [CrossRef]
- Conway, L.J.; Levickis, P.A.; Smith, J.; Mensah, F.; Wake, M.; Reilly, R. Maternal communicative behaviours and interaction quality as predictors of language development: Findings from a community-based study of slow-to-talk toddlers. Int. J. Lang. Commun. Disord. 2018, 53, 339–354. [Google Scholar] [CrossRef] [Green Version]
- Lüke, C.; Grimminger, A.; Rohlfing, K.J.; Liszkowski, U.; Ritterfeld, U. In infants’ hands: Identification of preverbal infants at risk for Primary Language Delay. Child Dev. 2017, 88, 484–492. [Google Scholar] [CrossRef]
- Lüke, C.; Ritterfeld, U.; Grimminger, A.; Rohlfing, K.J.; Liszkowski, U. Integrated communication system: Gesture and language acquisition in typically developing children and children with LD and DLD. Front. Psychol. 2020, 11, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sansavini, A.; Guarini, A.; Zuccarini, M.; Lee, J.Z.; Faldella, G.; Iverson, J.M. Low rates of pointing in 18-month-olds at risk for autism spectrum disorder and extremely preterm infants: A common index of language delay? Front. Psychol. 2019, 10, 2131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, L.; Delehantyb, A.; Dillonc, J.C.; Schatschneiderd, C.; Wetherby, A.M. Measures of early social communication and vocabulary production to predict language outcomes at two and three years in late-talking toddlers. Early Child. Res. Q. 2020, 51, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Vehkavuori, S.-M.; Stolt, S. Screening language skills at 2;0. Infant Behav. Dev. 2018, 50, 174–179. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Kim, J.Y.; Lee, S.Y.; Jeon, H.R. The Comparison of M-B CDI-K Short Form and K-ASQ as Screening Test for Language Development. Ann. Rehabil. Med. 2016, 40, 1108–1113. [Google Scholar] [CrossRef] [Green Version]
- Hadley, P.A.; Rispoli, M.; Hsu, N. Toddlers’ Verb Lexicon Diversity and Grammatical Outcomes. Lang. Speech Hear. Serv. Sch. 2016, 47, 44–58. [Google Scholar] [CrossRef]
- Bello, A.; Onofrio, D.; Remi, L.; Caselli, M.C. Prediction and persistence of late talking: A study of Italian toddlers at 29 and 34 months. Res. Dev. Disabil. 2018, 75, 40–48. [Google Scholar] [CrossRef]
- Kademann, S.; Sachse, S.; von Suchodoletz, W. Spätsprecher im Kindergartenalter. Mon. Kinderheilkd 2015, 5, 463–470. [Google Scholar] [CrossRef]
- Chilosi, A.M.; Pfanner, L.; Pecini, C.; Salvadorini, R.; Casalini, C.; Brizzolara, D.; Cipriani, P. Which linguistic measures distinguish transient from persistent language problems in Late Talkers from 2 to 4 years? A study on Italian speaking children. Res. Dev. Disabil. 2019, 89, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Nayeb, L.; Lagerberg, D.; Westerlund, M.; Sarkadi, A.; Lucas, S.; Eriksson, M. Modifying a language screening tool for three-year-old children identified severe language disorders six months earlier. Acta Paediatr. 2019, 108, 1642–1648. [Google Scholar] [CrossRef]
- Quam, C.; Cardinal, H.; Gallegos, C.; Bodner, T. Sound discrimination and explicit mapping of sounds to meanings in preschoolers with and without developmental language disorder. Int. J. Speech Lang. Pathol. 2020, 23, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Azab, S.N.; Ashour, H. Studying some elicited verbal prosodic patterns in Egyptian specific language impaired children. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Tomas, E.; Demuth, K.; Smith-Lock, K.M.; Petocz, P. Phonological and morphophonological effects on grammatical development in children with Specific Language Impairment. Int. J. Lang. Commun. Disord. 2015, 50, 516–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collisson, B.A.; Grela, B.; Spaulding, T.; Rueckl, J.G.; Magnuson, J.S. Individual differences in the shape bias in preschool children with specific language impairment and typical language development: Theoretical and clinical implications. Dev. Sci. 2015, 18, 373–388. [Google Scholar] [CrossRef]
- Marini, A.; Piccolo, B.; Taverna, L.; Berginc, M.; Ozbič, M. The complex relation between executive functions and language in preschoolers with Developmental Language Disorders. Int. J. Environ. Res. Public Health 2020, 17, 1772. [Google Scholar] [CrossRef] [Green Version]
- Gudmundsson, E. The Toddler Language and Motor Questionnaire: A mother-report measure of language and motor development. Res. Dev. Disabil. 2015, 45–46, 21–31. [Google Scholar] [CrossRef]
- Klem, M.; Melby-Lervåg, M.; Hagtvet, B.; Lyster, S.-A.H.; Gustafsson, J.-E.; Hulme, C. Sentence repetition is a measure of children’s language skills rather than working memory limitations. Dev. Sci. 2015, 18, 146–154. [Google Scholar] [CrossRef] [Green Version]
- Sahli, A.S.; Belgin, E. Adaptation, validity, and reliability of the Preschool Language Scale Fifth Edition (PLSe5) in the Turkish context: The Turkish Preschool Language Scalee5 (TPLSe5). Int. J. Pediatr. Otorhinolaryngol. 2017, 98, 143–149. [Google Scholar] [CrossRef]
- Eisenberg, S.; Victorino, K.; Murray, S. Concurrent validity of the Fluharty preschool speech and language screening test–second edition at age 3: Comparison with four diagnostic measures. Lang. Speech Hear. Ser. 2019, 50, 673–682. [Google Scholar] [CrossRef]
- Benavides, A.A.; Kapantzoglou, M.; Murata, C. Two Grammatical Tasks for Screening Language Abilities in Spanish-Speaking Children. Am. J. Speech-Lang. Pathol. 2018, 27, 690–705. [Google Scholar] [CrossRef]
- Puglisi, M.L.; Blasi, H.F.; Snowling, M.J. Screening for the identification of oral language difficulties in Brazilian preschoolers: A validation study. Lang. Speech Hear. Ser. 2020, 51, 852–865. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.G.; Jorgensen, S.K.; Blondeau, R. Investigating the validity of the Clinical Linguistic Auditory Milestone Scale. Int. J. Pediatr. Otorhinolaringol. 1995, 31, 63–75. [Google Scholar] [CrossRef]
- Coplan, J.; Gleason, J.R.; Ryan, R.; Burke, M.G.; Williams, M.L. Validation of an Early Language Milestone Scale in a high-risk population. Pediatrics 1982, 70, 677–683. [Google Scholar] [PubMed]
- Walker, D.; Guggenheim, S.; Downs, M.; Northern, J.L. Early Language Milestone Scale and language screening of young children. Pediatrics 1989, 83, 284–288. [Google Scholar] [CrossRef]
- Dixon, J.; Kot, A.; Law, J. Early language screening in City and Hackney: Work in progress. Child Care Health Dev. 1988, 14, 213–229. [Google Scholar] [CrossRef]
- Law, J. Early language screening in City and Hackney: The concurrent validity of a measure designed for use with 21/2-year-olds. Child Care Health Dev. 1994, 20, 295–308. [Google Scholar] [CrossRef]
- Rescorla, L. The Language Development Survey: A screening tool for delayed language in toddlers. J. Speech Hear. Disord. 1989, 54, 587–599. [Google Scholar] [CrossRef]
- Klee, T.; Carson, D.K.; Gavin, W.J.; Hall, L.; Kent, A.; Reece, S. Concurrent and predictive validity of an early language screening program. J. Speech Lang. Hear. Res. 1998, 41, 627–641. [Google Scholar] [CrossRef] [PubMed]
- Klee, T.; Pearce, K.; Carson, D.K. Improving the positive predictive valu.e of screening for developmental language disorder. J. Speech Lang. Hear. Res. 2000, 43, 821–833. [Google Scholar] [CrossRef]
- Rescorla, L.; Alley, A. Validation of the language development survey (LDS): A parent report tool for identifying language delay in toddlers. J. Speech Lang. Hear. Res. 2001, 44, 434–445. [Google Scholar] [CrossRef]
- Levett, L.; Muir, J. Which three year olds need speech therapy? Uses of the Levett-Muir language screening test. Health Visit. 1983, 56, 454–456. [Google Scholar] [PubMed]
- Rigby, M.J.; Chesham, I. A trial speech screening test for school entrants. Br. Med. J. 1981, 282, 449–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bliss, L.S.; Allen, D.V. Screening Kit of Language Development: A preschool language screening instrument. J. Commun. Disord. 1984, 17, 133–141. [Google Scholar] [CrossRef]
- Fenson, L.; Marchman, V.; Thal, D.; Dale, P.; Reznick, J.; Bates, E. MacArthur-Bates Communicative Developmental Inventories, 2nd ed.; Brookes: Baltimore, MD, USA, 2007. [Google Scholar]
- Wetherby, A.M.; Goldstein, H.; Clearly, J.; Allen, L.; Kublin, K. Early identification of children with communication disorders: Concurrent and predictive validity of the CSBS Developmental Profile. Infant Young Child. 2003, 6, 161–174. [Google Scholar] [CrossRef]
- Sachse, S.; Von Suchodoletz, W. Early identification of language delay by direct language assessment or parent report? J. Dev. Behav. Pediatr. 2008, 29, 34–41. [Google Scholar] [CrossRef] [Green Version]
- Grimm, H. Sprachentwicklungstest Für Zweijährige Kinder (SETK-2); [Language development test for two-year-old children]; Hogrefe: Göttingen, Germany, 2000. [Google Scholar]
- Dale, P.S.; Price, T.S.; Bishop, D.V.M.; Plomin, R. Outcomes of early language delay: I. Predicting persistent and transient language difficulties at 3 and 4 years. J. Speech Lang. Hear. Res. 2003, 46, 544–560. [Google Scholar] [CrossRef]
- Muris, P.; Meesters, C.; van den Berg, F. The Strengths and Difficulties Questionnaire (SDQ). Eur. Child Adolesc. Psychiatry 2003, 12, 1–8. [Google Scholar] [CrossRef]
- Frankenburg, W.K.; Dodds, J.B. The Denver Developmental Screening Test. J. Pediatr. 1967, 71, 181–191. [Google Scholar] [CrossRef]
- Cadman, D.; Chambers, L.W.; Walter, S.D.; Feldman, W.; Smith, K.; Ferguson, R. The usefulness of the Denver Developmental Screening Test to predict kindergarten problems in a general community population. Am. J. Public Health 1984, 74, 1093–1097. [Google Scholar] [CrossRef] [Green Version]
- Stott, C.M.; Merricks, M.J.; Bolton, P.F.; Goodyer, I.M. Screening for speech and language disorders: The reliability, validity and accuracy of the General Language Screen. Int. J. Lang. Commun. Disord. 2002, 37, 133–151. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.; Kersley, H.; Law, J. The Sure Start Language Measure Standardisation Study, July 2004–March 2005. DFES Publication. 2005. Available online: https://lemosandcrane.co.uk/resources/Roy%20-%20Sure%20Start%20Language%20Measure.pdf (accessed on 6 April 2021).
- Wetherby, A.M.; Prizant, B.M. Communication and Symbolic Behavior Scales—Normed Edition; Paul H. Brookes: Baltimore, MD, USA, 2003. [Google Scholar]
- Mullen, E.M. Mullen Scales of Early Learning; American Guidance Service: Circle Pines, MN, USA, 1995. [Google Scholar]
- Laakso, M.-L.; Eklund, K.; Poikkeus, A.-M. Esikko: Lapsen Esikielellisen Kommunikaation ja Kielen Ensikartoitus; NMI Niilo Mäki Instituutti: Jyväskylä, Finland, 2011. [Google Scholar]
- Kortesmaa, M.; Heimonen, K.; Merikoski, H.; Warma, M.-L.; Varpela, V. Reynellin Kielellisen Kehityksen Testi—Käsikirja; Psykologien Kustannus Oy: Helsinki, Finland, 2001. [Google Scholar]
- Chung, H.J.; Eun, B.L.; Kim, H.S.; Kim, J.K.; Shin, S.M.; Lee, J.H. The validity of Korean Ages and Stages Questionnaires (K-ASQ) in Korean infants and children. J. Korean Child Neurol. Soc. 2014, 22, 1–11. [Google Scholar] [CrossRef]
- Caselli, M.C.; Bello, A.; Rinaldi, P.; Stefanini, S.; Pasqualetti, P. Il Primo Vocabolario del Bambino: Gesti, Parole e Frasi. Forme Lunghe e Forme Brevi del Questionario e Valori di Riferimento per la Fascia 8–36 Mesi; Franco Angeli: Milano, Italy, 2015. [Google Scholar]
- Rescorla, L.; Frigerio, A.; Sali, M.E.; Spataro, P.; Longobardi, E. Typical and delayed lexical development in Italian. J. Speech Lang. Hear. Res. 2014, 57, 1792–1803. [Google Scholar] [CrossRef]
- Squires, J.; Potter, L.; Bricker, D. Ages and Stages Questionnaire User’s Guide; Brookes: Baltimore, MD, USA, 1999. [Google Scholar]
- Sturner, R.A.; Heller, J.H.; Funk, S.G.; Layton, T.L. The Fluharty Preschool Speech and Language Screening Test: A population-based validation study using sample independent decision rules. J. Speech Hear. Res. 1993, 36, 738–745. [Google Scholar] [CrossRef]
- Fluharty, N. Fluharty Preschool Speech and Language Screening Test–Second Edition (Fluharty-2); Pro-Ed: Austin, TX, USA, 2001. [Google Scholar]
- Reynell, J.; Gruber, C. Reynell Developmental Language Scales; Western Publishing: Los Angeles, CA, USA, 1985. [Google Scholar]
- Edwards, S.; Letts, C.; Sinka, I. The New Reynell Developmental Language Scales; GL-Assessment: London, UK, 2011. [Google Scholar]
- Steinlen, A.K.; Neils, K.; Piske, T.; Trumpp, C. SETK 3-5: A developmental language test on German for 3-to-5-year old children. In Bilingual Preschools, Volume 1: Learning and Development; Kersten, K., Rohde, A., Schelletter, C., Steinlen, A.K., Eds.; Wissenschaftlicher Verlag Trier: Trier, Germany, 2010; Volume 1, pp. 119–135. [Google Scholar]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Lombardino, L.J.; Leiberman, R.; Brown, J.C. Assessment of Literacy and Language; Pearson Psychcorp: San Antonio, TX, USA, 2005. [Google Scholar]
- Carrow-Woolfolk, E. Comprehensive Assessment of Spoken Language; American Guidance Service: Circle Pines, MN, USA, 1999. [Google Scholar]
- Semel, E.; Wiig, E.H.; Secord, W.A. Clinical Evaluation of Language Fundamentals-Preschool, 2nd ed.; Pearson Psychcorp: San Antonio, TX, USA, 2004. [Google Scholar]
- Wiig, E.H.; Semel, E.; Secord, W.A. Clinical Evaluation of Language Fundamentals, 5th ed.; Pearson Psychcorp: Bloomington, MN, USA, 2013. [Google Scholar]
- Seymour, H.N.; Roeper, T.W.; de Villiers, J.; de Villiers, P.A.; Pearson, B.Z. Diagnostic Evaluation of Language Variation; Pearson Psychcorp.: Minneapolis, MN, USA, 2005. [Google Scholar]
- Hammill, D.D.; Mather, R.; Roberts, R. Illinois Test of Psycholinguistic Abilities, 3rd ed.; Pro-Ed: Austin, TX, USA, 2001. [Google Scholar]
- Carrow-Woolfolk, E. Oral and Written Language Scales, 2nd ed.; Pearson Psychcorp.: Minneapolis, MN, USA, 2011. [Google Scholar]
- Zimmerman, I.L.; Steiner, V.G.; Pond, R.E. Preschool Language Scales, 5th ed.; (PLS-5); Pearson: San Antonio, TX, USA, 2011. [Google Scholar]
- Hresko, W.P.; Reid, D.K.; Hammill, D.D. Test of Early Language Development, 3rd ed.; Pro-Ed: Austin, TX, USA, 1999. [Google Scholar]
- Hammill, D.D.; Newcomer, P.L. Test of Language Development—Primary, 4th ed.; Pro-Ed.: Austin, TX, USA, 2008. [Google Scholar]
- Shrank, F.A.; Mather, N.; McGrew, K.S. Woodcock-Johnson IV Tests of Oral Language; Riverside: Rolling Meadows, IL, USA, 2014. [Google Scholar]
- Vance, R.; Plante, E. Selection of preschool language tests: A data-based approach. Lang. Speech Hear. Serv. Sch. 1994, 25, 15–24. [Google Scholar] [CrossRef]
- Pankratz, M.E.; Plante, E.; Vance, R.; Insalaco, D.M. The diagnostic and predictive validity of the Renfrew Bus Story. Lang. Speech Hear. Serv. Sch. 2007, 38, 390–399. [Google Scholar] [CrossRef]
- Gardner, H.; Froud, K.; McClelland, A.; van der Lely, H.K. Development of the Grammar and Phonology Screening (GAPS) test to assess key markers of specific language and literacy difficulties in young children. Int. J. Lang. Commun. Disord. 2006, 41, 513–540. [Google Scholar] [CrossRef] [Green Version]
- Nash, H.; Leavett, R.; Childs, H. Evaluating the GAPS test as a screener for language impairment in young children. Int. J. Lang. Commun. Disord. 2011, 46, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Greenslade, K.J.; Plante, E.; Vance, R. The diagnostic accuracy and construct validity of the structured photographic expressive language test—Preschool: Second edition. Lang. Speech Hear. Serv. Sch. 2009, 40, 150–160. [Google Scholar] [CrossRef]
- Perona, K.; Plante, E.; Vance, R. Diagnostic accuracy of the structured photographic expressive language test: Third edition (SPELT–3). Lang. Speech Hear. Serv. Sch. 2005, 36, 103–115. [Google Scholar] [CrossRef] [Green Version]
- Dunn, L.M.; Dunn, L.M. Peabody Picture Vocabulary Test-III; American Guidance Service: Circle Pines, MN, USA, 1997. [Google Scholar]
- Dunn, L.M.; Dunn, D.M. Peabody Picture Vocabulary Test—4; NCS Pearson: Minneapolis, MN, USA, 2007. [Google Scholar]
- Conti-Ramsden, G.; Hesketh, A. Risk markers for SLI: A study of young language-learning children. Int. J. Lang. Commum. Disord. 2003, 38, 251–263. [Google Scholar] [CrossRef]
- Archibald, L.M.; Joanisse, M.F. On the sensitivity and specificity of non-word repetition and sentence recall to language and memory impairments in children. J. Speech Lang. Hear. Res. 2009, 52, 899–914. [Google Scholar] [CrossRef] [Green Version]
- Dollaghan, C.; Campbell, T.F. Nonword repetition and child language impairment. J. Speech Lang. Hear. Res. 1998, 41, 1136–1146. [Google Scholar] [CrossRef] [PubMed]
- To, T.; Guttmann, A.; Dick, P.T.; Rosenfield, J.D.; Parkin, P.C.; Tassoudji, M.; Harris, J.K. Risk markers for poor developmental attainment in young children: Results from a longitudinal national survey. Arch. Pediatr. Adolesc. Med. 2004, 158, 643–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonard, L.B.; Kueser, J.B. Five overarching factors central to grammatical learning and treatment in children with developmental language disorder. Int. J. Lang. Commun. Disord. 2019, 54, 347–361. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sansavini, A.; Favilla, M.E.; Guasti, M.T.; Marini, A.; Millepiedi, S.; Di Martino, M.V.; Vecchi, S.; Battajon, N.; Bertolo, L.; Capirci, O.; et al. Developmental Language Disorder: Early Predictors, Age for the Diagnosis, and Diagnostic Tools. A Scoping Review. Brain Sci. 2021, 11, 654. https://doi.org/10.3390/brainsci11050654
Sansavini A, Favilla ME, Guasti MT, Marini A, Millepiedi S, Di Martino MV, Vecchi S, Battajon N, Bertolo L, Capirci O, et al. Developmental Language Disorder: Early Predictors, Age for the Diagnosis, and Diagnostic Tools. A Scoping Review. Brain Sciences. 2021; 11(5):654. https://doi.org/10.3390/brainsci11050654
Chicago/Turabian StyleSansavini, Alessandra, Maria Elena Favilla, Maria Teresa Guasti, Andrea Marini, Stefania Millepiedi, Maria Valeria Di Martino, Simona Vecchi, Nadia Battajon, Laura Bertolo, Olga Capirci, and et al. 2021. "Developmental Language Disorder: Early Predictors, Age for the Diagnosis, and Diagnostic Tools. A Scoping Review" Brain Sciences 11, no. 5: 654. https://doi.org/10.3390/brainsci11050654
APA StyleSansavini, A., Favilla, M. E., Guasti, M. T., Marini, A., Millepiedi, S., Di Martino, M. V., Vecchi, S., Battajon, N., Bertolo, L., Capirci, O., Carretti, B., Colatei, M. P., Frioni, C., Marotta, L., Massa, S., Michelazzo, L., Pecini, C., Piazzalunga, S., Pieretti, M., ... Lorusso, M. L. (2021). Developmental Language Disorder: Early Predictors, Age for the Diagnosis, and Diagnostic Tools. A Scoping Review. Brain Sciences, 11(5), 654. https://doi.org/10.3390/brainsci11050654