
Psychosocial Features of Shift Work Disorder

 ,
, 
Abstract
:1. Introduction
1.1. Diagnosing Shift Work Disorder (SWD): A Complex Task
1.2. Psychosocial Features of SWD
1.3. Objectives of the Current Study
2. Methods
2.1. Study Design
2.2. Setting
2.3. Participants
3. Measures
3.1. Initial Screening
3.2. Sleep and Sleepiness Measures
3.3. Psychosocial Measures
3.3.1. Physiological Activation
3.3.2. Cognitive Activation
3.3.3. Stimulus Control-Behavior
3.3.4. Emotions
3.3.5. Sleep Facilitation
3.4. Procedures
3.5. Participant Assignation
3.6. Statistical Methods
4. Results
4.1. Description of Groups Following the Evaluation
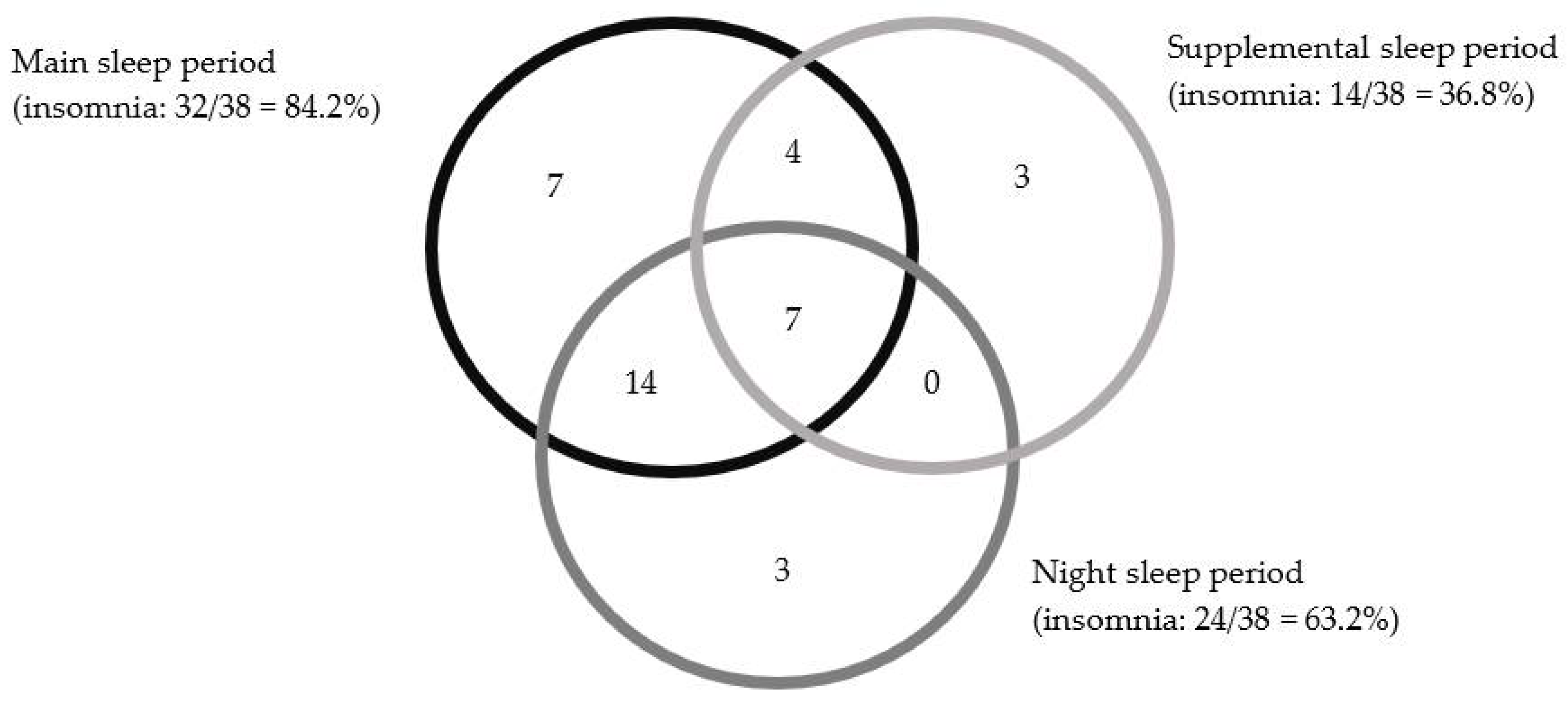
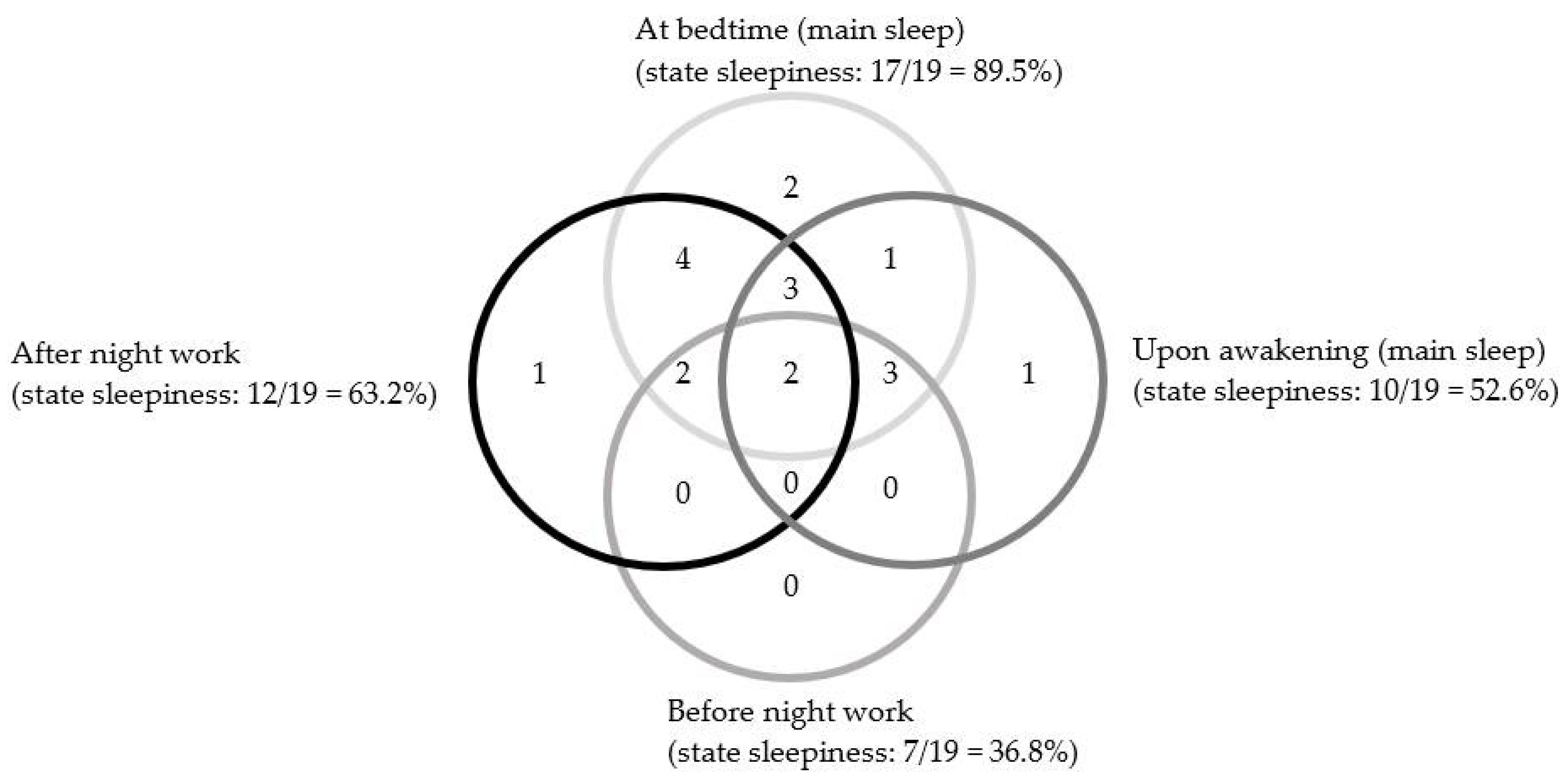
Symptoms of Shift Work Disorder (SWD)
4.2. Sleep and Wake Time Variables
4.3. Naps and Sleepiness
4.4. Differences in Psychosocial Variables
4.4.1. Physiological Activation
4.4.2. Cognitive Activation
4.4.3. Sleep Stimulus Control Behavior
4.4.4. Emotions Variables
4.4.5. Sleep Facilitation Variables
5. Discussion
5.1. Diagnosing SWD
5.2. Psychosocial Features of SWD
5.3. Strengths, Limitations, and Direction for Future Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Williams, C. Work-life balance of shift-workers. In Statistics Canada—Catalogue No. 75-001-X; Statistics Canada: Ottawa, ON, Canada, 2008; pp. 5–16. [Google Scholar]
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders III, 2nd ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2014. [Google Scholar]
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Pallesen, S.; Bjorvatn, B.; Waage, S.; Harris, A.; Sagoe, D. Prevalence of shift work disorder: A systematic review and meta-analysis. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef]
- Bandelow, B.; Michaelis, S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin. Neurosci. 2015, 17, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graa, F.R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef]
- Morin, C.M.; LeBlanc, M.; Daley, M.; Gregoire, J.-P.; Mérette, C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006, 7, 123–130. [Google Scholar] [CrossRef]
- Anbazhagan, S.; Ramesh, N.; Nisha, C.; Joseph, B. Shift work disorder and related health problems among nurses working in a tertiary care hospital, Bangalore, South India. Indian J. Occup. Environ. Med. 2016, 20, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Drake, C.L.; Roehrs, T.; Richardson, G.; Walsh, J.K.; Roth, T. Shift work sleep disorder: Prevalence and consequences beyond that of symptomatic day workers. Sleep 2004, 27, 1453–1462. [Google Scholar] [CrossRef] [PubMed]
- Kalmbach, D.A.; Pillai, V.; Cheng, P.; Arnedt, J.T.; Drake, C.L. Shift work disorder, depression, and anxiety in the transition to rotating shifts: The role of sleep reactivity. Sleep Med. 2015, 16, 1532–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flo, E.; Pallesen, S.; Akerstedt, T.; Mageroy, N.; Moen, B.E.; Gronli, J.; Nordhus, I.H.; Bjorvatn, B. Shift-related sleep problems vary according to work schedule. Occup. Environ. Med. 2013, 70, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Smolensky, M.H.; Roth, T. Consequences of shiftworking on sleep duration, sleepiness, and sleep attacks. Chronobiol. Int. 2010, 27, 575–589. [Google Scholar] [CrossRef] [PubMed]
- Sallinen, M.; Kecklund, G. Shift work, sleep, and sleepiness-differences between shift schedules and systems. Scand. J. Work Environ. Health 2010, 36, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P.; Rutherford, C. Moderators of the relationship between long work hours and health. J. Occup. Health Psychol. 2005, 10, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Akerstedt, T. Shift work and disturbed sleep/wakefulness. Occup. Med. 2003, 53, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.; Lee, W.; Choi, W.J.; Ham, S.; Kang, S.K. Association between Working Hours and Self-Rated Health. Int. J. Environ. Res. Public Health 2020, 17, 2736. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Richardson, A.; Poyser, C.; Butterworth, P.; Strazdins, L.; Leach, L.S. Shift work and mental health: A systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 2019. [Google Scholar] [CrossRef]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Goncalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- De Valck, E.; Cluydts, R. Sleepiness as a state-trait phenomenon, comprising both a sleep drive and a wake drive. Med. Hypotheses 2003, 60, 509–512. [Google Scholar] [CrossRef]
- Gumenyuk, V.; Belcher, R.; Drake, C.L.; Roth, T. Differential sleep, sleepiness, and neurophysiology in the insomnia phenotypes of shift work disorder. Sleep 2015, 38, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Vanttola, P.; Harma, M.; Viitasalo, K.; Hublin, C.; Virkkala, J.; Sallinen, M.; Karhula, K.; Puttonen, S. Sleep and alertness in shift work disorder: Findings of a field study. Int. Arch. Occup. Environ. Health 2019, 92, 523–533. [Google Scholar] [CrossRef] [Green Version]
- Gumenyuk, V.; Howard, R.; Roth, T.; Korzyukov, O.; Drake, C.L. Sleep loss, circadian mismatch, and abnormalities in reorienting of attention in night workers with shift work disorder. Sleep 2014, 37, 545–556. [Google Scholar] [CrossRef] [Green Version]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Saksvik-Lehouillier, I.; Hetland, H. A pilot study examining if satisfaction of basic needs can ameliorate negative effects of shift work. Ind. Health 2016, 54, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoddes, E.; Zarcone, V.; Smythe, H.; Phillips, R.; Dement, W.C. Quantification of sleepiness: A new approach. Psychophysiology 1973, 10, 431–436. [Google Scholar] [CrossRef]
- Boivin, D.B.; Boudreau, P. Impacts of shift work on sleep and circadian rhythms. Pathol. Biol. 2014, 62, 292–301. [Google Scholar] [CrossRef]
- Booker, L.A.; Sletten, T.L.; Alvaro, P.K.; Barnes, M.; Collins, A.; Chai-Coetzer, C.L.; Naqvi, A.; McMahon, M.; Lockley, S.W.; Rajaratnam, S.M.W.; et al. Exploring the associations between shift work disorder, depression, anxiety and sick leave taken amongst nurses. J. Sleep Res. 2019, e12872. [Google Scholar] [CrossRef] [PubMed]
- Waage, S.; Pallesen, S.; Moen, B.E.; Mageroy, N.; Flo, E.; Di Milia, L.; Bjorvatn, B. Predictors of shift work disorder among nurses: A longitudinal study. Sleep Med. 2014, 15, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Bastille-Denis, E.; Lemyre, A.; Pappathomas, A.; Roy, M.; Vallières, A. Are cognitive variables that maintain insomnia also involved in shift work disorder? Sleep Health 2020, 6, 399–406. [Google Scholar] [CrossRef] [PubMed]
- White, L.; Keith, B. The effect of shift work on the quality and stability of marital relations. J. Marriage Fam. 1990, 52, 453–462. [Google Scholar] [CrossRef]
- Cheng, P.; Drake, C.L. Psychological Impact of Shift Work. Curr. Sleep Med. Rep. 2018, 4, 104–109. [Google Scholar] [CrossRef]
- Espie, C.A. Insomnia: Conceptual issues in the development, persistence, and treatment of sleep disorder in adults. Annu. Rev. Psychol. 2002, 53, 215–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borbely, A.A. A two process model of sleep regulation. Hum. Neurobiol. 1982, 1, 195–204. [Google Scholar]
- Borbely, A.A.; Daan, S.; Wirz-Justice, A.; Deboer, T. The two-process model of sleep regulation: A reappraisal. J. Sleep Res. 2016, 25, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Regen, W.; Teghen, A.; Spiegelhalder, K.; Feige, B.; Nissen, C.; Riemann, D. Sleep changes in the disorder of insomnia: A meta-analysis of polysomnographic studies. Sleep Med. Rev. 2014, 18, 195–213. [Google Scholar] [CrossRef]
- Palagini, L.; Moretto, U.; Dell’Osso, L.; Carney, C. Sleep-related cognitive processes, arousal, and emotion dysregulation in insomnia disorder: The role of insomnia-specific rumination. Sleep Med. 2017, 30, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Vochem, J.; Strobel, C.; Maier, L.; Spiegelhalder, K.; Hertenstein, E.; Riemann, D.; Feige, B. Pre-Sleep Arousal Scale (PSAS) and the Time Monitoring Behavior-10 scale (TMB-10) in good sleepers and patients with insomnia. Sleep Med. 2019, 56, 98–103. [Google Scholar] [CrossRef]
- Lichstein, K.L. Insomnia identity. Behav. Res. Ther. 2017, 97, 230–241. [Google Scholar] [CrossRef]
- Morin, C.M. Insomnia: Psychological Assessment and Management; The Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV Axis I Disorders, Clinical Version (SCID-IV); American Psychiatric Association: Washington, DC, USA, 1997. [Google Scholar]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV); American Psychiatric Association: Arlington, VA, USA, 2015. [Google Scholar]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Barton, J.; Spelten, E.; Totterdell, P.; Smith, L.; Folkard, S.; Costa, G. The Standard Shiftwork Index-A Battery of Questionnaires for Assessing Shiftwork-Related Problems. Work Stress 1995, 9, 4–30. [Google Scholar] [CrossRef]
- Lamy, M.; Bastille-Denis, E.; Vallières, A. Sleep diaries for shift workers. J. Sleep Res. 2012, 21, 272. [Google Scholar] [CrossRef]
- Carney, C.E.; Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The consensus sleep diary: Standardizing prospective sleep self-monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaminska, M.; Jobin, V.; Mayer, P.; Amyot, R.; Perraton-Brillon, M.; Bellemare, F. The Epworth Sleepiness Scale: Self-administration versus administration by the physician, and validation of a French version. Can. Respir. J. 2010, 17, e27–e34. [Google Scholar] [CrossRef] [Green Version]
- Nicassio, P.M.; Mendlowitz, D.R.; Fussell, J.J.; Petras, L. The phenomenology of the pre-sleep state: The development of the pre-sleep arousal scale. Behav. Res. Ther. 1985, 23, 263–271. [Google Scholar] [CrossRef]
- Morin, C.M.; Vallieres, A.; Ivers, H. Dysfunctional beliefs and attitudes about sleep (DBAS): Validation of a brief version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Harvey, K.J.; Espie, C.A. Development and preliminary validation of the Glasgow Content of Thoughts Inventory (GCTI): A new measure for the assessment of pre-sleep cognitive activity. Br. J. Clin. Psychol. 2004, 43, 409–420. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Inventaire de Dépression de Beck-Deuxième Édition; The Psychological Corporation: Toronto, ON, Canada, 1996. [Google Scholar]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory (STAI); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Sabourin, S.; Valois, P.; Lussier, Y. Development and validation of a brief version of the dyadic adjustment scale with a nonparametric item analysis model. Psychol. Assess. 2005, 17, 15–27. [Google Scholar] [CrossRef]
- Antoine, P.; Christophe, V.; Nandrino, J.L. [Dyadic Adjustment Scale: Clinical interest of a revision and validation of an abbreviated form]. Encephale 2008, 34, 38–46. [Google Scholar] [CrossRef]
- Morin, C.M.; Espie, C.A. Insomnia: A Clinical Guide to Assessment and Treatment; Kluwer Academic/Plenum Publishers: New York, NY, USA, 2003. [Google Scholar]
- Tabachnick, B.; Fidell, L. Using Multivariate Statistics, 4th ed.; HarperCollins College Publishers: New York, NY, USA, 2001. [Google Scholar]
- SAS Institute. SAS/STAT 9.1.3 User’s Guide, Volumes 1 to 7; SAS Institute: Cary, NC, USA, 2005. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbraum Associates, Inc.: Mahwah, NJ, USA, 1988. [Google Scholar]
- Silva-Costa, A.; Griep, R.H.; Rotenberg, L. Disentangling the effects of insomnia and night work on cardiovascular diseases: A study in nursing professionals. Braz. J. Med. Biol. Res. 2015, 48, 120–127. [Google Scholar] [CrossRef] [Green Version]
- Dijk, D.J.; Brunner, D.P.; Beersma, D.G.; Borbely, A.A. Electroencephalogram power density and slow wave sleep as a function of prior waking and circadian phase. Sleep 1990, 13, 430–440. [Google Scholar] [CrossRef]
- Petrov, M.E.; Clark, C.B.; Molzof, H.E.; Johnson, R.L., Jr.; Cropsey, K.L.; Gamble, K.L. Sleep Strategies of Night-Shift Nurses on Days Off: Which Ones are Most Adaptive? Front. Neurol. 2014, 5, 277. [Google Scholar] [CrossRef] [Green Version]
- Papantoniou, K.; Pozo, O.J.; Espinosa, A.; Marcos, J.; Castano-Vinyals, G.; Basagana, X.; Ribas, F.C.; Mirabent, J.; Martin, J.; Carenys, G.; et al. Circadian variation of melatonin, light exposure, and diurnal preference in day and night shift workers of both sexes. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1176–1186. [Google Scholar] [CrossRef] [Green Version]
- Weibel, L.; Follenius, M.; Brandenberger, G. Modifications in biological rhythms in night-shift workers. Presse Med. 1999, 28, 252–258. [Google Scholar]
- Gibbs, M.; Hampton, S.; Morgan, L.; Arendt, J. Adaptation of the circadian rhythm of 6-sulphatoxymelatonin to a shift schedule of seven nights followed by seven days in offshore oil installation workers. Neurosci. Lett. 2002, 325, 91–94. [Google Scholar] [CrossRef]
- Akerstedt, T.; Gillberg, M. Subjective and objective sleepiness in the active individual. Int. J. Neurosci. 1990, 52, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Booker, L.A.; Barnes, M.; Alvaro, P.; Collins, A.; Chai-Coetzer, C.L.; McMahon, M.; Lockley, S.W.; Rajaratnam, S.M.W.; Howard, M.E.; Sletten, T.L. The role of sleep hygiene in the risk of Shift Work Disorder in nurses. Sleep 2020, 43. [Google Scholar] [CrossRef]
- Flo, E.; Pallesen, S.; Mageroy, N.; Moen, B.E.; Gronli, J.; Hilde Nordhus, I.; Bjorvatn, B. Shift work disorder in nurses--assessment, prevalence and related health problems. PLoS ONE 2012, 7, e33981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, A.G. A cognitive model of insomnia. Behav. Res. Ther. 2002, 40, 869–893. [Google Scholar] [CrossRef]
- Demsky, C.A.; Fritz, C.; Hammer, L.B.; Black, A.E. Workplace incivility and employee sleep: The role of rumination and recovery experiences. J. Occup. Health Psychol. 2019, 24, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Zwart, C.A.; Lisman, S.A. Analysis of stimulus control treatment of sleep-onset insomnia. J. Consult. Clin. Psychol. 1979, 47, 113–118. [Google Scholar] [CrossRef]
- Bootzin, R.R. Stimulus control and treatment for insomnia. Proc. Am. Psychol. Assoc. 1972, 7, 395–396. [Google Scholar]
- Jarnefelt, H.; Harma, M.; Sallinen, M.; Virkkala, J.; Paajanen, T.; Martimo, K.P.; Hublin, C. Cognitive behavioural therapy interventions for insomnia among shift workers: RCT in an occupational health setting. Int. Arch. Occup. Environ. Health 2020, 93, 535–550. [Google Scholar] [CrossRef] [Green Version]
- Ministère de la Santé et des Services Sociaux. Emplois Selon la Catégorie Professionnelle 2018. Available online: https://msss.gouv.qc.ca/professionnels/statistiques-donnees-sante-bien-etre/statistiques-de-sante-et-de-bien-etre-selon-le-sexe-volet-national/emplois-selon-la-categorie-professionnelle (accessed on 26 March 2021).
- Querstret, D.; Cropley, M. Exploring the relationship between work-related rumination, sleep quality, and work-related fatigue. J. Occup. Health Psychol. 2012, 17, 341–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarnefelt, H.; Lagerstedt, R.; Kajaste, S.; Sallinen, M.; Savolainen, A.; Hublin, C. Cognitive behavioral therapy for shift workers with chronic insomnia. Sleep Med. 2012, 13, 1238–1246. [Google Scholar] [CrossRef]
- Lee, K.A.; Gay, C.L.; Alsten, C.R. Home-based behavioral sleep training for shift workers: A pilot study. Behav. Sleep Med. 2014, 12, 455–468. [Google Scholar] [CrossRef]
- Claveau, S.; Lemyre, A.; Bastien, C.H.; Vallières, A. Efficacité d’interventions comportementales pour le sommeil des travailleurs de nuit. Exploration préliminaire. Médecine du Sommeil 2017, 14, 174–185. [Google Scholar] [CrossRef]
- Vallières, A.; Roy, M.; Bastille-Denis, E.; Claveau, S.; Simon, T. Exploring a behavioral therapy for Insomnia in shift workers. J. Sleep Disord. Ther. 2015, 4. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Sociodemographic | All (N = 119) | Night Workers | Day Workers | Night Workers | Day Workers | ||
|---|---|---|---|---|---|---|---|
| GS (n = 36) | SWD (n = 43) | GS (n = 20) | Insomnia (n = 20) | GS vs. SWD p-Value a | GS vs. Insomnia p-Value a | ||
| Age in years (M, SD) | 37.8 (12.1) | 39.4 (14.6) | 35.4 (10.4) | 36.4 (12.5) | 41.5 (9.1) | 0.1815 | 0.1484 |
| Gender (% male) | 22.7% | 19.4% | 25.6% | 30.0% | 15.0% | 0.5172 | 0.4506 |
| Years working under this schedule (M, SD) | 5.7 (6.8) | 7.9 (7.2) | 4.1 (4.7) | 6.8 (10.6) | 4.3 (4.0) | 0.0096 | 0.3599 |
| Nationality (% Canadian) | 99.2% | 97.2% | 100.0% | 100.0% | 100.0% | 0.4557 | - |
| Single, separated/divorced (%) | 37.8% | 47.2% | 30.2% | 40% | 35% | 0.1212 | 0.6485 |
| Schooling in years (M, SD) | 15.2 (2.5) | 14.9 (2.1) | 15.5 (2.4) | 15.5 (1.6) | 14.4 (3.7) | 0.2597 | 0.2035 |
| Full time employment (%) | 76.5% | 83.3% | 69.8% | 75.0% | 80.0% | 0.1600 | 1.0000 |
| Annual income (% participants) | 0.3223 | 0.8330 | |||||
| <35,000$ | 19.3% | 16.7% | 11.6% | 25% | 35% | ||
| 35,000 and 50,000$ | 39.5% | 41.7% | 37.2% | 45% | 35% | ||
| >50,000$ | 36.1% | 36.1% | 51.2% | 20.0% | 20.0% | ||
| Refuse to answer | 2.5% | 5.6% | 0.0% | 0.0% | 5.0% | ||
| Residence (% participants) | 0.0796 | 0.2619 | |||||
| Alone | 18.0% | 30.6% | 11.6% | 20.0% | 5.0% | ||
| With partner | 32% | 36.1% | 32.6% | 25.0% | 25.0% | ||
| With partner + children or family | 42.0% | 25.0% | 48.8% | 35.0% | 65.0% | ||
| Other | 6.7% | 8.3% | 7.0% | 10.0% | 0.0% | ||
| Recruitment (15 min) | Visit 1 | Observation (Two Weeks) | Visit 2 (One Hour) | Group Assignation (One Hour) | ||
|---|---|---|---|---|---|---|
| Evaluation (Three Hours) | Observation (45 min) | |||||
| Tools used |
|
|
|
|
|
|
| Objective | To determine participant eligibility | To make the diagnosis | To assess variables that might be related to SWD. | To obtain sleep variables and sleepiness measures. The sleep diary data were used to confirm if insomnia criteria were met. | Enhance compliance to study procedures | To assign participants to the good sleeper group or insomnia/SWD group. |
| Night Workers | Day Workers | Night Workers | Day Workers | |||||
|---|---|---|---|---|---|---|---|---|
| GS (n = 36) | SWD (n = 43) | GS (n = 20) | Insomnia (n = 20) | ANCOVA | GS vs. SWD | GS vs. Insomnia | ||
| Sleep | LsMean (SD) | LsMean (SD) | LsMean (SD) | LsMean (SD) | F (pglobal) | F (pinteraction) | ES (p-Value) | ES (p-Value) |
| Main sleep (in minutes) | ||||||||
| Main-TST | 369.9 (63.1) | 339.1 (61.6) | 418.8 (59.1) | 383.4 (62.3) | 9.13 (<0.0001) | 0.04 (0.842) | −0.56 (0.003) | |
| Main-TWT | 43.0 (39.7) | 68.7 (38.8) | 41.8 (37.2) | 130.1 (39.2) | 16.92 (<0.0001) | 18.48 (<0.0001) | 0.70 (0.003) | 2.38 (<0.0001) |
| Main-SOL | 17.2 (13.1) | 19.2 (12.8) | 13.2 (12.3) | 38.9 (12.9) | 11.20 (<0.0001) | 24.50 (<0.0001) | 0.16 (0.485) | 2.10 (<0.0001) |
| Night sleep (in minutes) | ||||||||
| Night-TST | 443.5 (78.5) | 421.1 (76.8) | 420.5 (73.6) | 375.8 (77.6) | 3.20 (0.01) | 0.60 (0.44) | −0.42 (0.026) | |
| Night-TWT | 51.7 (51.0) | 90.1 (49.8) | 43.2 (47.8) | 133.6 (50.4) | 11.00 (<0.0001) | 7.70 (0.006) | 0.81 (0.001) | 1.90 (<.0001) |
| Night-SOL | 20.2 (18.5) | 21.5 (18.1) | 13.8 (17.3) | 40.2 (18.3) | 5.40 (<0.0001) | 13.70 (<0.0001) | 0.08 (0.731) | 1.53 (<.0001) |
| Night Workers | Day Workers | Night Workers | Day Workers | |||||
|---|---|---|---|---|---|---|---|---|
| GS (n = 36) | SWD (n = 43) | GS (n = 20) | Insomnia (n = 20) | ANCOVA or Linear Model | GS vs. SWD | GS vs. Insomnia | ||
| Naps and Sleepiness | LsMean (SD) or % | LsMean (SD) or % | LsMean (SD) or % | LsMean (SD) or % | F or χ2 (pglobal) | F or χ2 (pinteraction) | ES (p-Value) | ES (p-Value) |
| Naps | ||||||||
| Average per day | 1.27 (0.30) | 1.29 (0.33) | 0.98 (0.30) | 0.99 (0.30) | 5.81 (<0.0001) | 0.00 (0.9781) | −1.08 (<0.0001) | |
| Nap-TST | 108.59 (56.5) | 89.31 (55.00) | 91.92 (52.40) | 49.31 (54.40) | 4.74 (0.0007) | 0.85 (0.3603) | −0.55 (0.0254) | |
| Nap-TWT | 23.52 (23.80) | 36.25 (23.10) | 18.33 (22.00) | 35.45 (22.90) | 3.56 (0.0055) | 0.17 (0.6823) | −0.14 (0.5721) | |
| Average per 14 days | 1.45 (3.60) | 2.82 (3.50) | 0.36 (3.40) | 0.51 (3.50) | 1.92 (0.0989) | 0.54 (0.4632) | −0.51 (<0.0042) | |
| Nap-TST on 14 days | 895.54 (502.4) | 720.48 (489) | 154.34 (465.9) | 43.34 (484.2) | 18.12 (<0.0001) | 0.08 (0.7772) | −1.55 (<0.0001) | |
| Nap-TWT on 14 days | 160.2 (157.7) | 253.51 (153.5) | 31.74 (146.3) | 88.52 (152) | 6.93 (<0.0001) | 0.27 (0.6074) | −1.02 (0.0001) | |
| Sleepiness | ||||||||
| ESS | 8.2 (4.6) | 8.7 (4.4) | 7.8 (4.3) | 9.2 (4.5) | 1.36 (0.251) | 0.3 (0.619) | 0.21 (0.262) | |
| SSS | 2.8 (0.72) | 3.1 (0.72) | 2.7 (0.72) | 3.2 (0.72) | 3.96 (0.005) | 0.4 (0.539) | 0.60 (0.001) | |
| Excessive (% yes) | 14.3% | 32.5% | 15.0% | 30.0% | 11.3 (0.104) | 0.0 (0.970) | 0.91 (0.490) | |
| Night Workers | Day Workers | Ancova (or Chi-Square a) | Night Workers | Day Workers | ||||
|---|---|---|---|---|---|---|---|---|
| Psychosocial Variables | GS (n = 36) | SWD (n = 43) | GS (n = 20) | Insomnia (n = 20) | GS vs. SWD | GS vs. Insomnia | ||
| LsMean (SD) | LsMean (SD) | LsMean (SD) | LsMean (SD) | F (pglobal) | F or χ2 (pinteraction) | ES (p-Value) | ES (p-Value) | |
| Physiological activation and lifestyle habit | ||||||||
| Physiological activation (PSAS-somatic) | 11.18 (3.7) | 12.03 (3.6) | 9.65 (3.5) | 13.47 (3.6) | 3.50 (0.006) | 4.80 (0.031) | 0.25 (0.278) | 1.11 (0.001) |
| Smoker (% yes) | 22.22% | 6.98% | 10% | 20% | - | 0.21 (0.645) | RR = 1.04 (0.785) | |
| Cigarettes (qty per week) | 11.16 (33) | 6.58 (32.2) | 4.85 (31) | 17.7 (32.7) | 0.6 (0.702) | 2.03 (0.157) | 0.05 (0.795) | |
| Alcoholic beverages (qty per week) | 2.41 (3.6) | 3.18 (3.6) | 3.02 (3.4) | 3.79 (3.6) | 1.14 (0.344) | 0.00 (0.997) | 0.23 (0.22) | |
| Caffeine beverages (qty per week) | 11.89 (9) | 8.36 (8.8) | 7.8 (8.5) | 11.67 (9) | 2.21 (0.058) | 4.88 (0.029) | −0.42 (0.071) | 0.46 (0.151) |
| Cognitive activation | ||||||||
| Cognitive activation (PSAS-cognitive) | 14.61 (5.3) | 18.08 (5.2) | 14.25 (4.9) | 20.57 (5.2) | 6.10 (<0.0001) | 2.1 (0.15) | 0.90 (<0.0001) | |
| Beliefs (DBAS-16) | 3.85 (1.3) | 4.68 (1.3) | 3.53 (1.2) | 5.91 (1.3) | 12.82 (<0.0001) | 10.68 (0.001) | 0.70 (0.002) | 1.99 (<0.0001) |
| Intrusive thoughts (GCTI) | 40.45 (10.1) | 47.56 (10.1) | 37.89 (9.7) | 52.14 (10.1) | 5.96 (<0.0001) | 3.11 (0.081) | 0.99 (<0.0001) | |
| Stimulus control behavior in bed | ||||||||
| TV, phone, electronic tablets (% yes) | 72.22% | 76.74% | 85% | 75% | - | 0.23 (0.635) | RR = 1.00 (0.985) | |
| Reading (% yes) | 30.56% | 48.84% | 55% | 65% | - | 0.03 (0.873) | RR = 0.91 (0.503) | |
| Emotions | ||||||||
| Depression (BDI-II) | 3.8 (6.5) | 7.98 (6.4) | 3.53 (6.1) | 11.77 (6.5) | 7.85 (<0.0001) | 2.82 (0.096) | 0.92 (<0.0001) | |
| Anxiety STATE | 26.69 (9.6) | 32.53 (9.4) | 28.6 (9.0) | 34.37 (9.6) | 3.63 (0.004) | 0 (0.985) | 0.66 (0.001) | |
| Anxiety TRAIT | 30.84 (8.2) | 36.38 (8.1) | 32.38 (7.7) | 41.84 (8.2) | 7.07 (<0.0001) | 1.6 (0.209) | 0.90 (<0.0001) | |
| Sleep facilitation | ||||||||
| Work satisfaction | 28.25 (4.9) | 26.17 (4.8) | 29.20 (4.6) | 26.25 (4.8) | 2.51 (0.046) | 0.23 (0.629) | −0.53 (0.005) | |
| Work schedule satisfaction | 17.40 (4.0) | 16.90 (4.0) | 20.51 (3.8) | 22.59 (3.9) | 8.81 (<0.0001) | 2.50 (0.117) | 1.16 (<0.0001) | |
| Domestic and Social situation | 72.59 (17.4) | 69.29 (16.2) | 66.48 (15.7) | 68.41 (17.1) | 0.39 (0.811) | 0.25 (0.624) | −0.05 (0.889) | |
| Marital distress (DAS) | 75.12 (11.8) | 72.23 (12.0) | 70.61 (11.5) | 69.86 (12.3) | 1.44 (0.22) | 0.16 (0.693) | −0.19 (0.372) | |
| Distance from home to work (km) | 13.15 (16.8) | 19.20 (16.4) | 11.05 (16.2) | 15.42 (17.1) | 1.26 (0.291) | 0.33 (0.566) | 0.34 (0.131) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallières, A.; Mérette, C.; Pappathomas, A.; Roy, M.; Bastien, C.H. Psychosocial Features of Shift Work Disorder. Brain Sci. 2021, 11, 928. https://doi.org/10.3390/brainsci11070928
Vallières A, Mérette C, Pappathomas A, Roy M, Bastien CH. Psychosocial Features of Shift Work Disorder. Brain Sciences. 2021; 11(7):928. https://doi.org/10.3390/brainsci11070928
Chicago/Turabian StyleVallières, Annie, Chantal Mérette, Alric Pappathomas, Monica Roy, and Célyne H. Bastien. 2021. "Psychosocial Features of Shift Work Disorder" Brain Sciences 11, no. 7: 928. https://doi.org/10.3390/brainsci11070928
APA StyleVallières, A., Mérette, C., Pappathomas, A., Roy, M., & Bastien, C. H. (2021). Psychosocial Features of Shift Work Disorder. Brain Sciences, 11(7), 928. https://doi.org/10.3390/brainsci11070928