

“My Hand Is Different”: Altered Body Perception in Stroke Survivors with Chronic Pain

 ,
,
Abstract
:1. Introduction
Aims of This Study
2. Materials and Methods
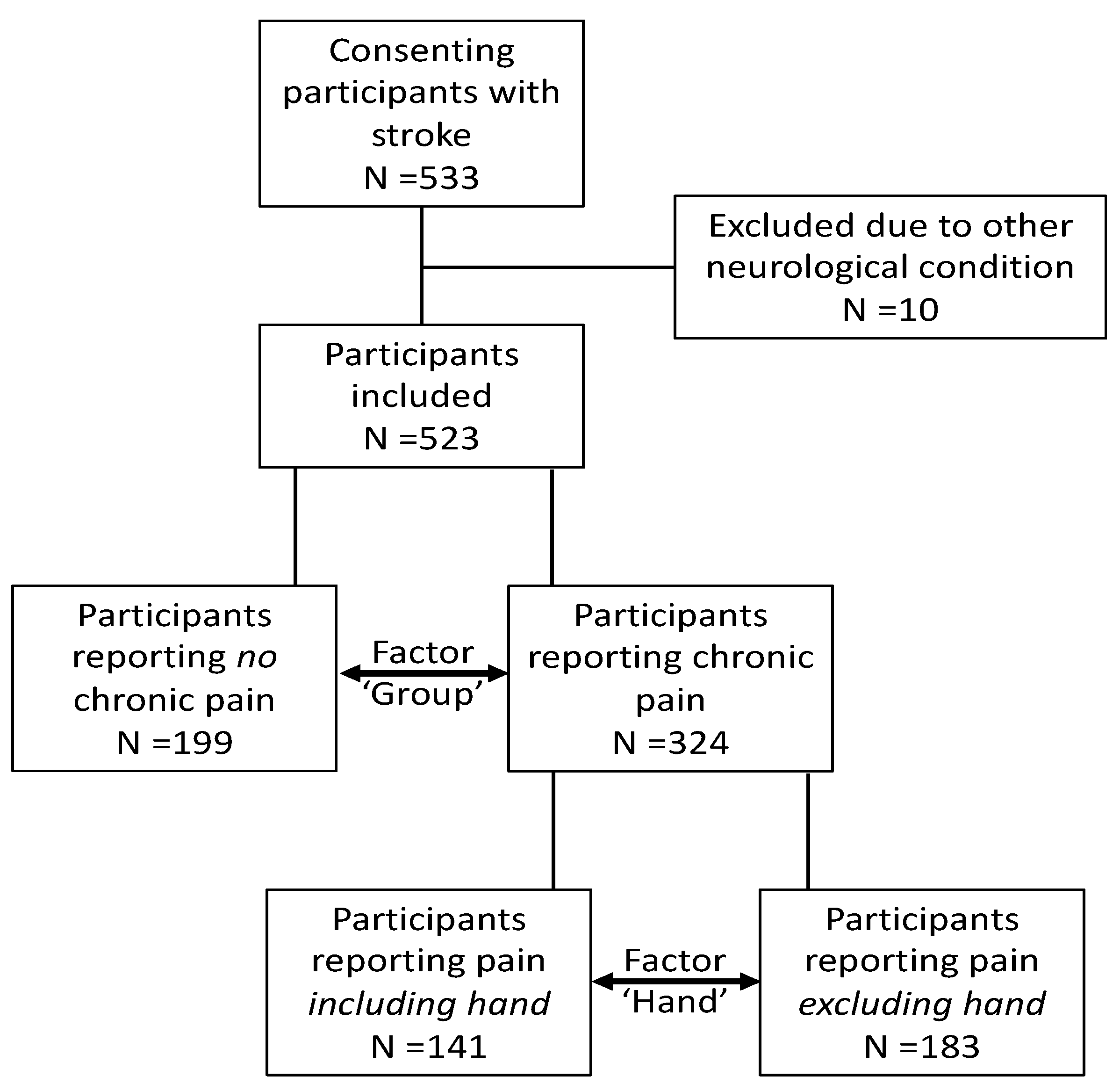
2.1. Study Design and Participants
2.2. Instruments
2.2.1. Numerical Rating Scale for Pain (NRS)
2.2.2. Neuropathic Pain Symptom Inventory (NPSI)
2.2.3. Perceived Hand Size Question
2.3. Data Analysis
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- General Information
- Year of birth (drop down boxes 1910–1998)
- Gender (click male/female/rather not say)
- Country of residence (drop down boxes)
- Have you been diagnosed by a medical practitioner as having had a stroke? (click yes/no)
- If yes:
- (a)
- Was it in the past three months? (click yes/no)
- (b)
- How many strokes have you had (drop down boxes 1–4+)
- (c)
- When did you first have a stroke? (drop down boxes 1930–2018)
- (d)
- When did your most recent stroke happen? (drop down box 1930–2018)
- (e)
- Which best describes your stroke/s:
- (1)
- Bleed (haemorrhage)/Clot (infarct)/Both (bleed and clot)/ Not sure (drop down boxes)
- (2)
- What side/s of your brain were affected by your stroke/s? (click left/right/both/unknown)
- Handedness
- Prior to your stroke, what was your preferred or dominant hand to use? (click left/right)
- Since your stroke, what is your preferred or dominant hand to use? (click left/right)
- Since your stroke, does it feel like your hand is now a different size? (click yes/no)
- (a)
- If yes, does it feel (click bigger/smaller)?
- Pain
- Have you experienced ongoing pain over the past three months that has made you do something for it? (e.g., Take a tablet, change behaviours, see a health professional) (yes/no) If yes please continue
- (a)
- Please score your pain level out of 10 on the chart below, where 0 = no pain, and 10 = worst pain imaginable
![Brainsci 12 01331 i001]()
- (b)
- Where? Tick more than one area if appropriate (body charts with tick boxes)
![Brainsci 12 01331 i002]()


References
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, A.-C.; Lindgren, A.; Hallström, B.; Norrving, B. Prevalence and intensity of pain after stroke: A population based study focusing on patients’ perspectives. J. Neurol. Neurosurg. Psychiatry 2006, 77, 590–595. [Google Scholar] [CrossRef]
- Hansen, A.; Marcussen, N.; Klit, H.; Andersen, G.; Finnerup, N.; Jensen, T. Pain following stroke: A prospective study. Eur. J. Pain 2012, 16, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Blyth, F.M.; March, L.M.; Brnabic, A.J.M.; Jorm, L.R.; Williamson, M.; Cousins, M.J. Chronic pain in Australia: A prevalence study. Pain 2001, 89, 127–134. [Google Scholar] [CrossRef]
- Johannes, C.B.; Le, T.K.; Zhou, X.; Johnston, J.A.; Dworkin, R.H. The Prevalence of Chronic Pain in United States Adults: Results of an Internet-Based Survey. J. Pain 2010, 11, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Choi-Kwon, S.; Choi, J.M.; Kwon, S.U.; Kang, D.-W.; Kim, J.S. Factors that Affect the Quality of Life at 3 Years Post-Stroke. J. Clin. Neurol. 2006, 2, 34–41. [Google Scholar] [CrossRef]
- Jensen, M.P.; Chodroff, M.J.; Dworkin, R.H. The impact of neuropathic pain on health-related quality of life: Review and implications. Neurology 2007, 68, 1178–1182. [Google Scholar] [CrossRef]
- Harrison, R.A.; Field, T.S. Post Stroke Pain: Identification, Assessment, and Therapy. Cerebrovasc. Dis. 2015, 39, 190–201. [Google Scholar] [CrossRef]
- Klit, H.; Finnerup, N.B.; Overvad, K.; Andersen, G.; Jensen, T.S. Pain Following Stroke: A Population-Based Follow-Up Study. PLoS ONE 2011, 6, e27607. [Google Scholar] [CrossRef]
- Paolucci, S.; Iosa, M.; Barbanti, P.; Bovi, P.; Candeloro, E.; Mancini, A.; Monaco, S.; Pieroni, A.; Truini, A.; Toni, D.; et al. Prevalence and Time Course of Post-Stroke Pain: A Multicenter Prospective Hospital-Based Study. Pain Med. 2015, 17, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Adey-Wakeling, Z.; Arima, H.; Crotty, M.; Leyden, J.; Kleinig, T.; Anderson, C.; Newbury, J. Incidence and Associations of Hemiplegic Shoulder Pain Poststroke: Prospective Population-Based Study. Arch. Phys. Med. Rehabil. 2014, 96, 241–247.e1. [Google Scholar] [CrossRef] [PubMed]
- International Association for the Study of Pain Terminology Working Group. IASP Terminology. 2021. Available online: https://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698&navItemNumber=576 (accessed on 30 September 2021).
- Stroke Foundation. Clinical Guidelines for Stroke Management. Melbourne Australia. 2021. Available online: https://informme.org.au/Guidelines/Clinical-Guidelines-for-Stroke-Management (accessed on 30 September 2021).
- Hebert, D.; Lindsay, M.P.; McIntyre, A.; Kirton, A.; Rumney, P.G.; Bagg, S.; Bayley, M.; Dowlatshahi, D.; Dukelow, S.; Garnhum, M.; et al. Canadian stroke best practice recommendations: Stroke rehabilitation practice guidelines, update 2015. Int. J. Stroke 2016, 11, 459–484. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Stroke Rehabilitation in Adults (NICE Guideline 162). 2013. Available online: https://www.nice.org.uk/guidance/cg162 (accessed on 15 July 2021).
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Zorowitz, R.D. Guidelines for adult stroke rehabilitation and recovery: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef]
- Plecash, A.R.; Chebini, A.; Ip, A.; Lai, J.J.; Mattar, A.A.; Randhawa, J.; Field, T.S. Updates in the Treatment of Post-Stroke Pain. Curr. Neurol. Neurosci. Rep. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L. Distorted body image in complex regional pain syndrome. Neurology 2005, 65, 773. [Google Scholar] [CrossRef]
- Lewis, J.S.; Kersten, P.; McCabe, C.S.; McPherson, K.M.; Blake, D.R. Body perception disturbance: A contribution to pain in complex regional pain syndrome (CRPS). Pain 2007, 133, 111–119. [Google Scholar] [CrossRef]
- Martínez, E.; Aira, Z.; Buesa, I.; Aizpurua, I.; Rada, D.; Azkue, J.J. Embodied pain in fibromyalgia: Disturbed somatorepresentations and increased plasticity of the body schema. PLoS ONE 2018, 13, e0194534. [Google Scholar] [CrossRef]
- Moseley, L.G. I can’t find it! Distorted body image and tactile dysfunction in patients with chronic back pain. Pain 2008, 140, 239–243. [Google Scholar] [CrossRef]
- Meier, R.; Iten, P.; Luomajoki, H. Clinical assessments can discriminate altered body perception in patients with unilateral chronic low back pain, but not differences between affected and unaffected side. Musculoskelet. Sci. Pract. 2018, 39, 136–143. [Google Scholar] [CrossRef]
- Moreira, C.; Bassi, A.R.; Brandão, M.P.; Silva, A.G. Do patients with chronic neck pain have distorted body image and tactile dysfunction? Eur. J. Physiother. 2017, 19, 215–221. [Google Scholar] [CrossRef]
- Lotze, M.; Moseley, G.L. Role of distorted body image in pain. Curr. Rheumatol. Rep. 2007, 9, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Sündermann, O.; Flink, I.; Linton, S.J. My body is not working right: A cognitive behavioral model of body image and chronic pain. Pain 2020, 161, 1136–1139. [Google Scholar] [CrossRef] [PubMed]
- Boccia, M.; Raimo, S.; Di Vita, A.; Battisti, A.; Matano, A.; Guariglia, C.; Grossi, D.; Palermo, L. Topological and hodological aspects of body representation in right brain damaged patients. Neuropsychologia 2020, 148, 107637. [Google Scholar] [CrossRef] [PubMed]
- Di Vita, A.; Boccia, M.; Palermo, L.C. To move or not to move, that is the question! Body schema and non-action orientated body representaions: An fMRI meta-analytic study. Neurosci. Biobehav. Rev. 2016, 68, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Brugger, P. Interdependence of movement and anatomy persists when amputees learn a physiologically impossible movement of their phantom limb. Proc. Natl. Acad. Sci. USA 2009, 106, 18798–18802. [Google Scholar] [CrossRef] [PubMed]
- Price, B. Assessing altered body image. J. Psychiatr. Ment. Health Nurs. 1995, 2, 169–175. [Google Scholar] [CrossRef]
- Nijs, J.; Lahousse, A.; Kapreli, E.; Bilika, P.; Saraçoğlu, I.; Malfliet, A.; Coppieters, I.; De Baets, L.; Leysen, L.; Roose, E.; et al. Nociplastic Pain Criteria or Recognition of Central Sensitization? Pain Phenotyping in the Past, Present and Future. J. Clin. Med. 2021, 10, 3203. [Google Scholar] [CrossRef]
- Lewis, J.; Schweinhardt, P. Perceptions of the painful body: The relationship between body perception disturbance, pain and tactile discrimination in complex regional pain syndrome. Eur. J. Pain 2012, 16, 1320–1330. [Google Scholar] [CrossRef]
- Boesch, E.; Bellan, V.; Moseley, G.L.; Stanton, T.R. The effect of bodily illusions on clinical pain: A systematic review and meta-analysis. Pain 2016, 157, 516–529. [Google Scholar] [CrossRef]
- McCabe, C.S.; Haigh, R.C.; Blake, D.R. Mirror visual feedback for the treatment of complex regional pain syndrome (type 1). Curr. Pain Headache Rep. 2008, 12, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Chmalzl, L.; Ragnoö, C.; Ehrsson, H.H. An Alternative to Traditional Mirror Therapy: Illusory touch can reduce phantom pain when illusory movement does not. Clin. J. Pain 2013, 29, e10–e18. [Google Scholar] [CrossRef] [PubMed]
- Kotiuk, V.; Burianov, O.; Kostrub, O.; Khimion, L.; Zasadnyuk, I. The impact of mirror therapy on body schema perception in patients with complex regional pain syndrome after distal radius fractures. Br. J. Pain 2018, 13, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Raimo, S.; Boccia, M.; Di Vita, A.; Iona, T.; Cropano, M.; Ammendolia, A.; Colao, R.; Angelillo, V.; Maiorino, A.; Guariglia, C.; et al. Body Representation Alterations in Patients with Unilateral Brain Damage. J. Int. Neuropsychol. Soc. 2021, 28, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Llorens, R.; Borrego, A.; Palomo, P.; Cebolla, A.; Noé, E.; I Badia, S.B.; Baños, R. Body schema plasticity after stroke: Subjective and neurophysiological correlates of the rubber hand illusion. Neuropsychologia 2017, 96, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Veerbeek, J.M.; Kwakkel, G.; van Wegen, E.E.; Ket, J.C.; Heymans, M.W. Early prediction of outcome of activities of daily living after stroke: A systematic review. Stroke 2011, 42, 1482–1488. [Google Scholar] [CrossRef]
- Carey, L.M. Somatosensory Loss after Stroke. Crit. Rev. Phys. Rehabil. Med. 1995, 7, 51–91. [Google Scholar] [CrossRef]
- Kessner, S.S.; Schlemm, E.; Cheng, B.; Bingel, U.; Fiehler, J.; Gerloff, C.; Thomalla, G. Somatosensory Deficits After Ischemic Stroke. Stroke 2019, 50, 1116–1123. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Fermanian, J.; Alchaar, H.; Gautron, M.; Masquelier, E.; Rostaing, S.; Lanteri-Minet, M.; Collin, E.; Grisart, J.; et al. Development and validation of the Neuropathic Pain Symptom Inventory. Pain 2004, 108, 248–257. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Bernhardt, J.; Hayward, K.; Kwakkel, G.; Ward, N.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Neurorehabilit. Neural Repair 2017, 31, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematic review of the pain scales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Nishigami, T.; Ohishi, K.; Nishikawa, K.; Wand, B.M.; Stanton, T.R.; Yamashita, H.; Mibu, A.; Tokunaga, M.; Yoshimoto, T.; et al. “But it feels swollen!”: The frequency and clinical characteristics of people with knee osteoarthritis who report subjective knee swelling in the absence of objective swelling. Pain Rep. 2021, 6, e971. [Google Scholar] [CrossRef] [PubMed]
- Förderreuther, S.; Sailer, U.; Straube, A. Impaired self-perception of the hand in complex regional pain syndrome (CRPS). Pain 2004, 110, 756–761. [Google Scholar] [CrossRef]
- Galer, B.S.; Jensen, M. Neglect-Like Symptoms in Complex Regional Pain Syndrome: Results of a Self-Administered Survey. J. Pain Symptom Manag. 1999, 18, 213–217. [Google Scholar] [CrossRef]
- Vallar, G.; Calzolari, E. Unilateral spatial neglect after posterior parietal damage. Handb. Clin. Neurol. 2018, 151, 287–312. [Google Scholar] [CrossRef]
- Longo, M.R.; Azañón, E.; Haggard, P. More than skin deep: Body representation beyond primary somatosensory cortex. Neuropsychologia 2010, 48, 655–668. [Google Scholar] [CrossRef]
- Linkenauger, S.A.; Geuss, M.N.; Stefanucci, J.K.; Leyrer, M.; Richardson, B.H.; Proffitt, D.R.; Bülthoff, H.; Mohler, B.J. Evidence for Hand-Size Constancy: The Dominant Hand as a Natural Perceptual Metric. Psychol. Sci. 2014, 25, 2086–2094. [Google Scholar] [CrossRef]
- Wallwork, S.; Bellan, V.; Catley, M.J.; Moseley, L. Neural representations and the cortical body matrix: Implications for sports medicine and future directions. Br. J. Sports Med. 2015, 50, 990–996. [Google Scholar] [CrossRef]
- Tsang, A.; Von Korff, M.; Lee, S.; Alonso, J.; Karam, E.; Angermeyer, M.C.; Borges, G.L.G.; Bromet, E.J.; de Girolamo, G.; de Graaf, R.; et al. Common Chronic Pain Conditions in Developed and Developing Countries: Gender and Age Differences and Comorbidity With Depression-Anxiety Disorders. J. Pain 2008, 9, 883–891. [Google Scholar] [CrossRef]
- Kennedy, J.; Roll, J.M.; Schraudner, T.; Murphy, S.; McPherson, S. Prevalence of Persistent Pain in the U.S. Adult Population: New Data From the 2010 National Health Interview Survey. J. Pain 2014, 15, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Samulowitz, A.; Gremyr, I.; Eriksson, E.; Hensing, G. “Brave Men” and “Emotional Women”: A Theory-Guided Literature Review on Gender Bias in Health Care and Gendered Norms towards Patients with Chronic Pain. Pain Res. Manag. 2018, 2018, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Goodin, P.; Lamp, G.; Vidyasagar, R.; McArdle, D.; Seitz, R.J.; Carey, L.M. Altered functional connectivity differs in stroke survivors with impaired touch sensation following left and right hemisphere lesions. NeuroImage Clin. 2018, 18, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Schwoebel, J.; Coslett, H.B. Evidence for Multiple, Distinct Representations of the Human Body. J. Cogn. Neurosci. 2005, 17, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Polito, C.; Bolognesi, E.; D’Argenio, A.; Ginestroni, A.; Mascalchi, M.; Pellicanò, G.; Mazzoni, L.; Rotella, F.; Faravelli, C.; et al. Looking at my body. Similarities and differences between anorexia nervosa patients and controls in body image visual processing. Eur. Psychiatry 2013, 28, 427–435. [Google Scholar] [CrossRef]
- Attall, N.; Bouhassira, D.; Baron, R.; Dostrovsky, J.; Dworkin, R.H.; Finnerup, N.; Gourlay, G.; Haanpaa, M.; Raja, S.; Rice, A.S.; et al. Assessing symptom profiles in neuropathic pain clinical trials: Can it improve outcome? Eur. J. Pain 2011, 15, 441–443. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Jensen, T.S. Mechanisms of Disease: Mechanism-based classification of neuropathic pain—A critical analysis. Nat. Clin. Pract. Cardiovasc. Med. 2006, 2, 107–115. [Google Scholar] [CrossRef]
- Bouhassira, D.; Wilhelm, S.; Schacht, A.; Perrot, S.; Kosek, E.; Cruccu, G.; Freynhagen, R.; Tesfaye, S.; Lledó, A.; Choy, E.; et al. Neuropathic pain phenotyping as a predictor of treatment response in painful diabetic neuropathy: Data from the randomized, double-blind, COMBO-DN study. Pain 2014, 155, 2171–2179. [Google Scholar] [CrossRef]
- Lewis, J.S.M.; McCabe, C.S. Body perception disturbance in CRPS. Pract. Pain Manag. 2010, 10, 60–66. [Google Scholar]
- Nishigami, T.; Mibu, A.; Tanaka, K.; Yamashita, Y.; Yamada, E.; Wand, B.M.; Catley, M.J.; Stanton, T.; Moseley, L. Development and psychometric properties of knee-specific body-perception questionnaire in people with knee osteoarthritis: The Fremantle Knee Awareness Questionnaire. PLoS ONE 2017, 12, e0179225. [Google Scholar] [CrossRef]
- Stanton, T.; Lin, C.-W.C.; Bray, H.; Smeets, R.; Taylor, D.; Law, R.Y.W.; Moseley, L. Tactile acuity is disrupted in osteoarthritis but is unrelated to disruptions in motor imagery performance. Rheumatology 2013, 52, 1509–1519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braus, D.F.; Krauss, J.K. The shoulder-hand syndrome after stroke: A prospective clinical trial. Ann. Neurol. 1994, 36, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Roosink, M.; Renzenbrink, G.J.; Buitenweg, J.R.; Van Dongen, R.T.; Geurts, A.C.; Ijzerman, M. Persistent Shoulder Pain in the First 6 Months After Stroke: Results of a Prospective Cohort Study. Arch. Phys. Med. Rehabil. 2011, 92, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Kalita, J.; Misra, U.; Kumar, A.; Bhoi, S.K. Long-term Prednisolone in Post-stroke Complex Regional Pain Syndrome. Pain Physician 2016, 19, 565–574. [Google Scholar] [CrossRef]
- Wand, B.M.; Catley, M.J.; Rabey, M.I.; O’Sullivan, P.; O’Connell, N.E.; Smith, A.J. Disrupted Self-Perception in People With Chronic Low Back Pain. Further Evaluation of the Fremantle Back Awareness Questionnaire. J. Pain 2016, 17, 1001–1012. [Google Scholar] [CrossRef]
- Porges, S.W. Body Perception Questionnaire. Laboratory of Developmental Assessment. Univ. Maryland 1993, 10, 2009. [Google Scholar]
- Cabrera, A.; Kolacz, J.; Pailhez, G.; Bulbena-Cabre, A.; Bulbena, A.; Porges, S.W. Assessing body awareness and autonomic reactivity: Factor structure and psychometric properties of the Body Perception Questionnaire-Short Form (BPQ-SF). Int. J. Methods Psychiatr. Res. 2017, 27, e1596. [Google Scholar] [CrossRef]
- Galer, B.S.; Jensen, M.P. Development and preliminary validation of a pain measure specific to neuropathic pain: The Neuropathic Pain Scale. Neurology 1997, 48, 332–338. [Google Scholar] [CrossRef]
- Haanpää, M.; Attal, N.; Backonja, M.; Baron, R.; Bennett, M.; Bouhassira, D.; Cruccu, G.; Hansson, P.; Haythornthwaite, J.A.; Iannetti, G.D.; et al. NeuPSIG guidelines on neuropathic pain assessment. Pain 2011, 152, 14–27. [Google Scholar] [CrossRef]
- Choi-Kwon, S.; Choi, S.H.; Suh, M.; Choi, S.; Cho, K.-H.; Nah, H.-W.; Song, H.; Kim, J.S. Musculoskeletal and central pain at 1 year post-stroke: Associated factors and impact on quality of life. Acta Neurol. Scand. 2016, 135, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Klit, H.; Finnerup, N.B.; Jensen, T.S. Central post-stroke pain: Clinical characteristics, pathophysiology, and management. Lancet Neurol. 2009, 8, 857–868. [Google Scholar] [CrossRef]
- Ratnasabapathy, Y.; Broad, J.; Baskett, J.; Pledger, M.; Marshall, J.; Bonita, R. Shoulder pain in people with a stroke: A population-based study. Clin. Rehabil. 2003, 17, 304–311. [Google Scholar] [CrossRef]
- Lindgren, I.; Jönsson, A.-C.; Norrving, B.; Lindgren, A. Shoulder pain after stroke: A prospective population-based study. Stroke 2007, 38, 343–348. [Google Scholar] [CrossRef]
- Menger, F.; Morris, J.; Salis, C. The impact of aphasia on Internet and technology use. Disabil. Rehabil. 2019, 42, 2986–2996. [Google Scholar] [CrossRef]
- de Vries, N.J.; Sloot, P.H.; Achterberg, W.P. Pain and pain assessment in stroke patients with aphasia: A systematic review. Aphasiology 2016, 31, 703–719. [Google Scholar] [CrossRef]
- Lee, H.; Lamb, S.E.; Bagg, M.K.; Toomey, E.; Cashin, A.G.; Moseley, G.L. Reproducible and replicable pain research: A critical review. Pain 2018, 159, 1683–1689. [Google Scholar] [CrossRef]
- Moseley, G.L.; Butler, D.S. The Explain Pain Handbook: Protectometer; Noigroup Publications: Adelaide, Australia, 2015. [Google Scholar]
- Osumi, M.; Imai, R.; Ueta, K.; Nobusako, S.; Morioka, S. Negative Body Image Associated with Changes in the Visual Body Appearance Increases Pain Perception. PLoS ONE 2014, 9, e107376. [Google Scholar] [CrossRef]
- Haslam, B.S.; Butler, D.S.; Carey, L.M. Novel insights into stroke pain beliefs and perceptions. Top. Stroke Rehabil. 2019, 27, 344–353. [Google Scholar] [CrossRef]
- Kitzmüller, G.; Häggström, T.; Asplund, K. Living an unfamiliar body: The significance of the long-term influence of bodily changes on the perception of self after stroke. Med. Health Care Philos. 2012, 16, 19–29. [Google Scholar] [CrossRef]
- Matamala-Gomez, M.; Malighetti, C.; Cipresso, P.; Pedroli, E.; Realdon, O.; Mantovani, F.; Riva, G. Changing Body Representation Through Full Body Ownership Illusions Might Foster Motor Rehabilitation Outcome in Patients with Stroke. Front. Psychol. 2020, 11, 1962. [Google Scholar] [CrossRef]
- Tambone, R.; Giachero, A.; Calati, M.; Molo, M.T.; Burin, D.; Pyasik, M.; Cabria, F.; Pia, L. Using Body Ownership to Modulate the Motor System in Stroke Patients. Psychol. Sci. 2021, 32, 655–667. [Google Scholar] [CrossRef]


{kind=link}
| No Pain N = 199 | Pain N = 324 | p Value | |
|---|---|---|---|
| Age, years (mean, SD) | 59(14) | 58 (13) | 0.486 a |
| Gender, female | 43% (86/199) | 56% (182/324) | 0.004 b |
Reported hemisphere of lesion
| 44% (88/199) 34% (67/199) 5% (9/199) 18% (35/199) | 46% (150/324) 35% (114/324) 7% (24/324) 11% (36/324) | 0.644 b 0.723 b 0.188 b |
| Duration post-stroke, years (mean, SD) | 7.88 (6.77) | 7.14 (6.20) | 0.215 a |
| Altered perceived hand size (yes) | 15% (30/199) | 34% (110/324) | 0.001 b |
Reported nature of size change
| 37% (11/30) 63% (19/30) - | 35% (39/110) 58% (64/110) 6% (7/110) | 0.902 b 0.611 b |
| Pain (Excl Hand) N = 183 | Pain (Incl Hand) N = 141 | p Value | |
|---|---|---|---|
Hemisphere of lesion
| 48% (87/183) 33% (60/183) 7% (13/183) 13% (23/183) | 45% (63/141) 38% (54/141) 8% (11/141) 9% (13/141) | 0.609 b 0.303 b 0.812 b |
| Altered perceived hand size (yes) | 28% (51/183) | 42% (59/141) | 0.009 b |
Reported nature of size change
| 10% (19/183) 16% (29/183) | 14% (20/141) 25% (35/141) | 0.297 b 0.044 b |
| Pain Scale (Mean, SD) | Other Pain | Hand Pain | p Value |
|---|---|---|---|
| Numerical Rating Scale | 5.97 (1.92) | 6.11 (1.81) | 0.514 a |
Neuropathic Pain Symptom Inventory *
| 27.8 (21.6) 3.10 (3.23) 2.76 (2.81) 1.87 (2.97) 3.65 (3.42) 2.87 (2.95) 2.29 (3.15) 3.45 (3.59) 2.43 (2.53) 1.86 (2.89) 3.49 (3.42) 1.93 (33.18) 3.09 (3.05) 3.36 (3.35) 2.83 (3.14) | 42.4 (22.1) 4.37 (3.16) 4.01 (2.97) 3.53 (3.22) 4.48 (3.33) 3.43 (2.97) 3.28 (3.26) 3.59 (3.42) 3.98 (2.86) 3.76 (3.27) 4.22 (3.44) 3.96 (3.39) 5.58 (3.18) 5.39 (3.33) 5.78 (3.25) | <0.001 a <0.001 a <0.001 a <0.001 a 0.029 a 0.089 a 0.006 a 0.741 a <0.001 a <0.001 a 0.056 a <0.001 a <0.001 a <0.001 a <0.001 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haslam, B.S.; Butler, D.S.; Moseley, G.L.; Kim, A.S.; Carey, L.M. “My Hand Is Different”: Altered Body Perception in Stroke Survivors with Chronic Pain. Brain Sci. 2022, 12, 1331. https://doi.org/10.3390/brainsci12101331
Haslam BS, Butler DS, Moseley GL, Kim AS, Carey LM. “My Hand Is Different”: Altered Body Perception in Stroke Survivors with Chronic Pain. Brain Sciences. 2022; 12(10):1331. https://doi.org/10.3390/brainsci12101331
Chicago/Turabian StyleHaslam, Brendon S., David S. Butler, G. Lorimer Moseley, Anthony S. Kim, and Leeanne M. Carey. 2022. "“My Hand Is Different”: Altered Body Perception in Stroke Survivors with Chronic Pain" Brain Sciences 12, no. 10: 1331. https://doi.org/10.3390/brainsci12101331
APA StyleHaslam, B. S., Butler, D. S., Moseley, G. L., Kim, A. S., & Carey, L. M. (2022). “My Hand Is Different”: Altered Body Perception in Stroke Survivors with Chronic Pain. Brain Sciences, 12(10), 1331. https://doi.org/10.3390/brainsci12101331