
The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence


Abstract
:1. Introduction
1.1. The Link between ADHD and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence
1.2. ADHD and Antisocial Behavior
1.3. Interaction in the Prediction of Antisocial Behavior
1.4. Sense of Coherence
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Analytic Approach
3. Results
3.1. Descriptive Statistics
3.2. Correlations
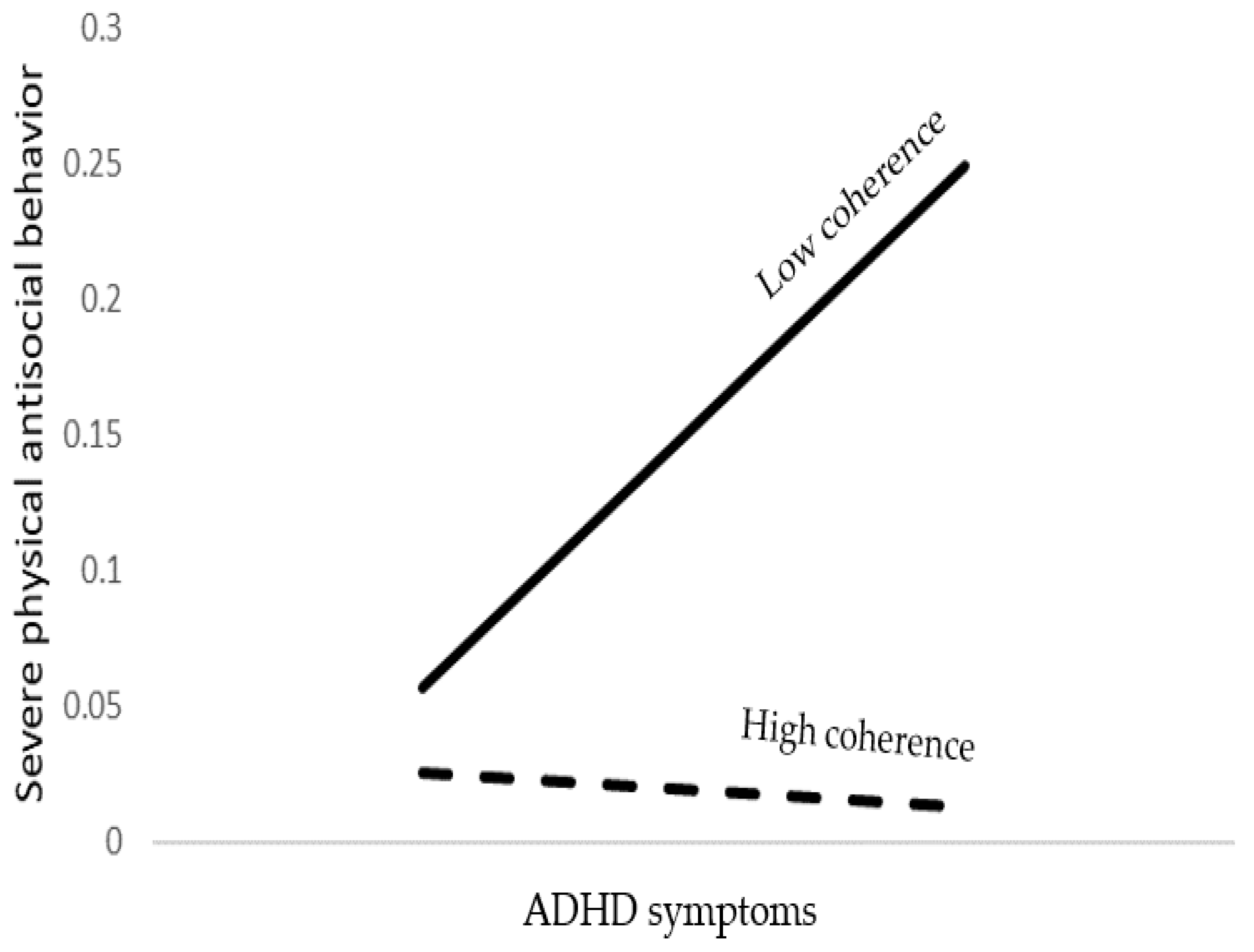
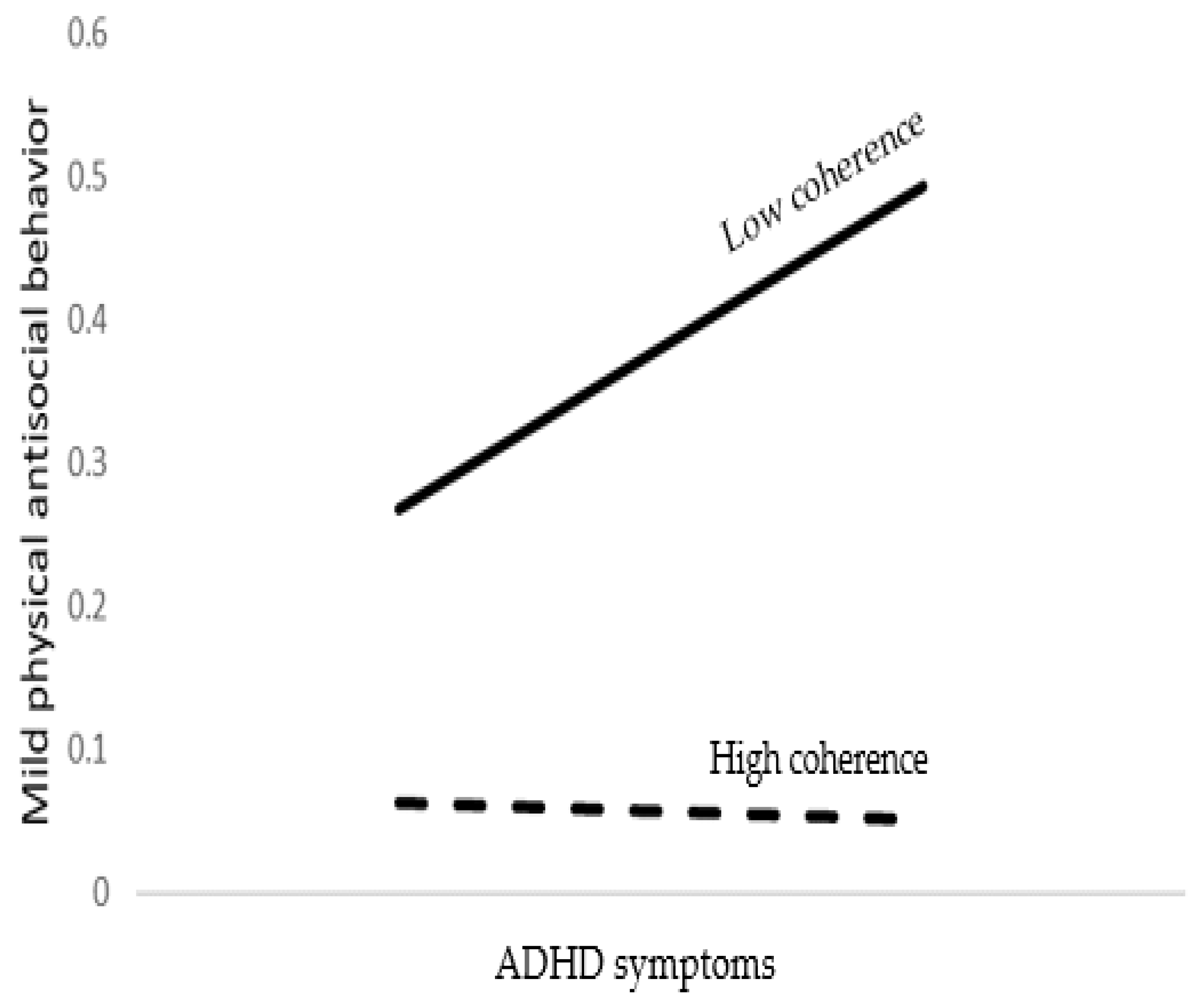
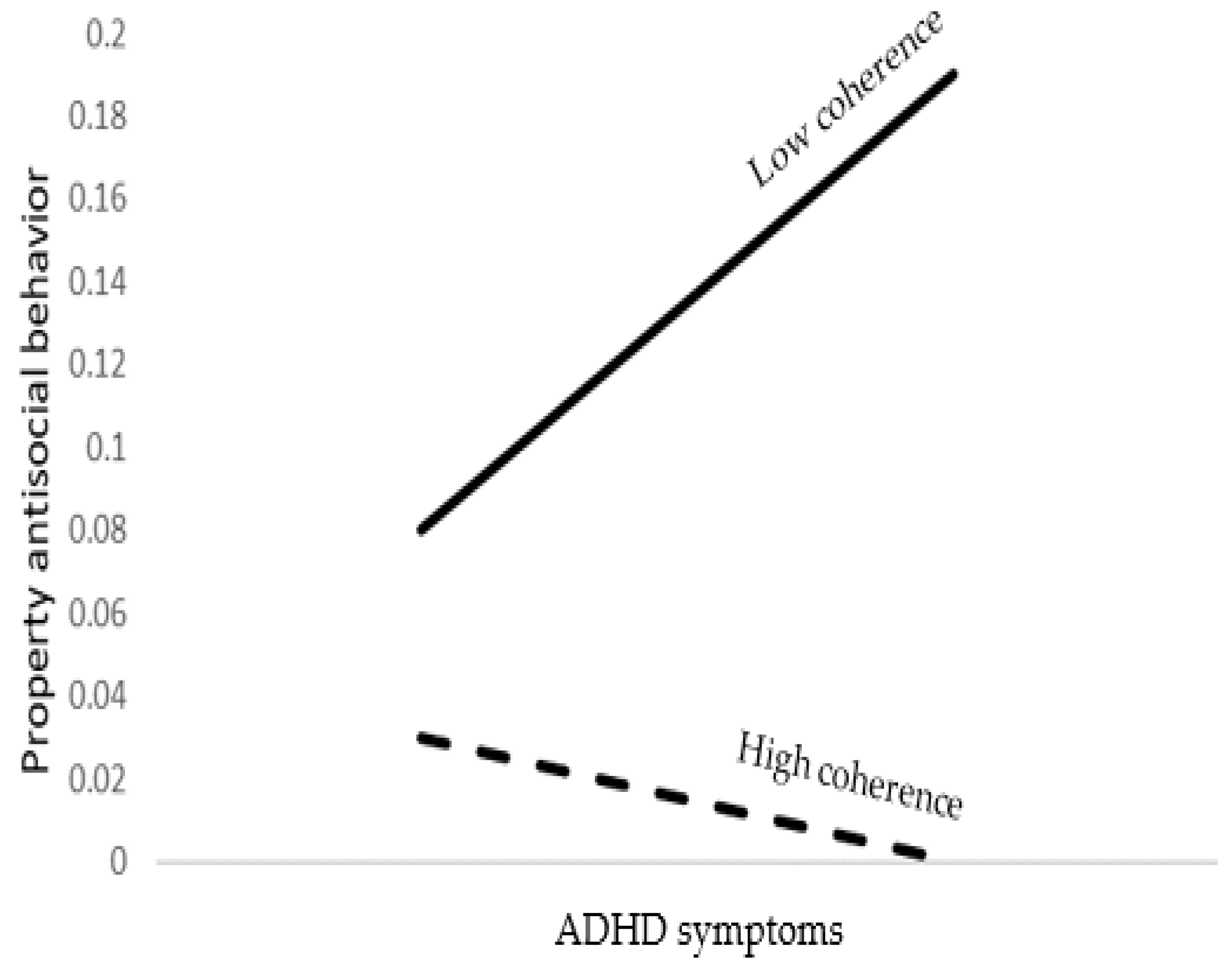
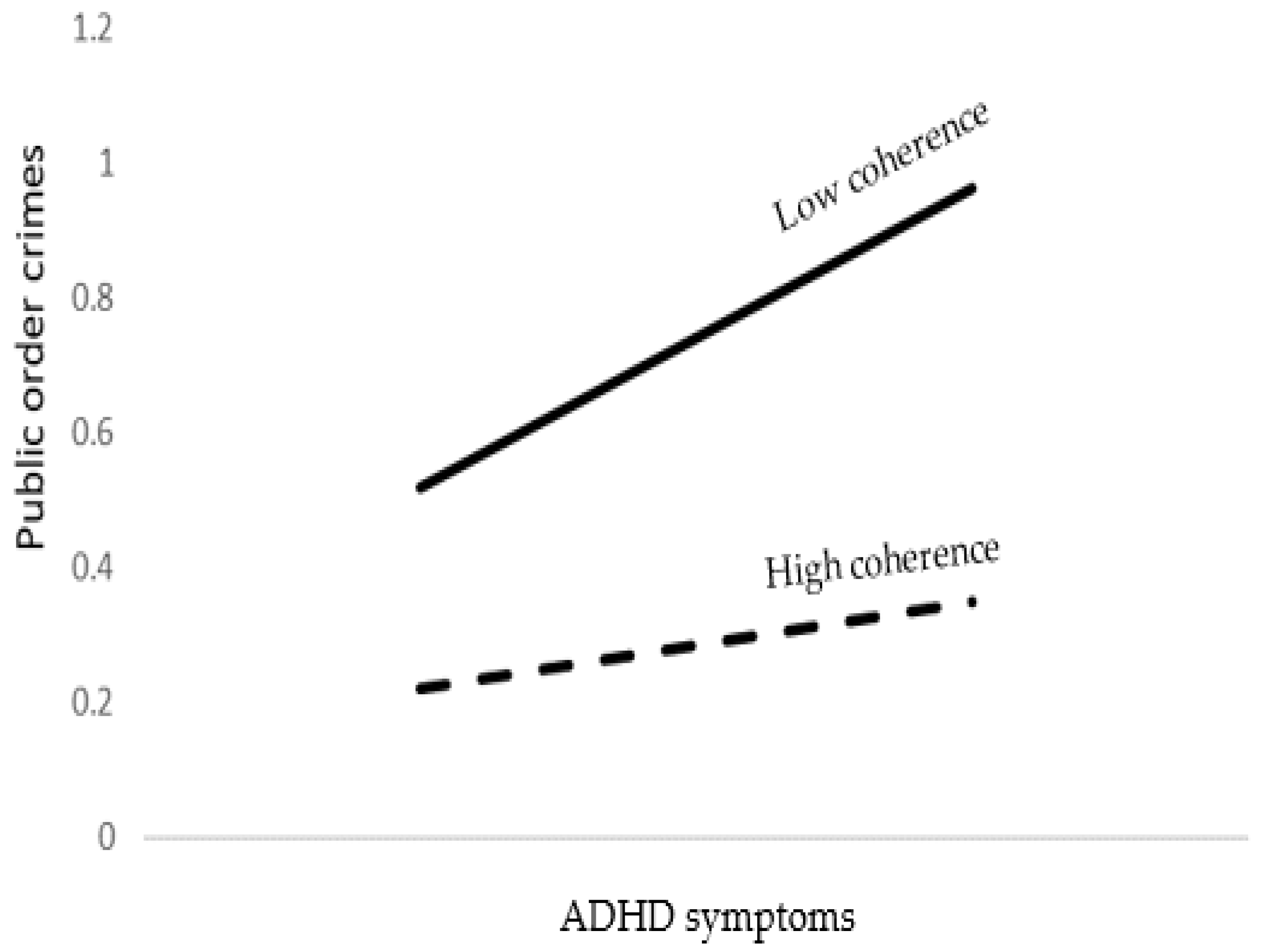
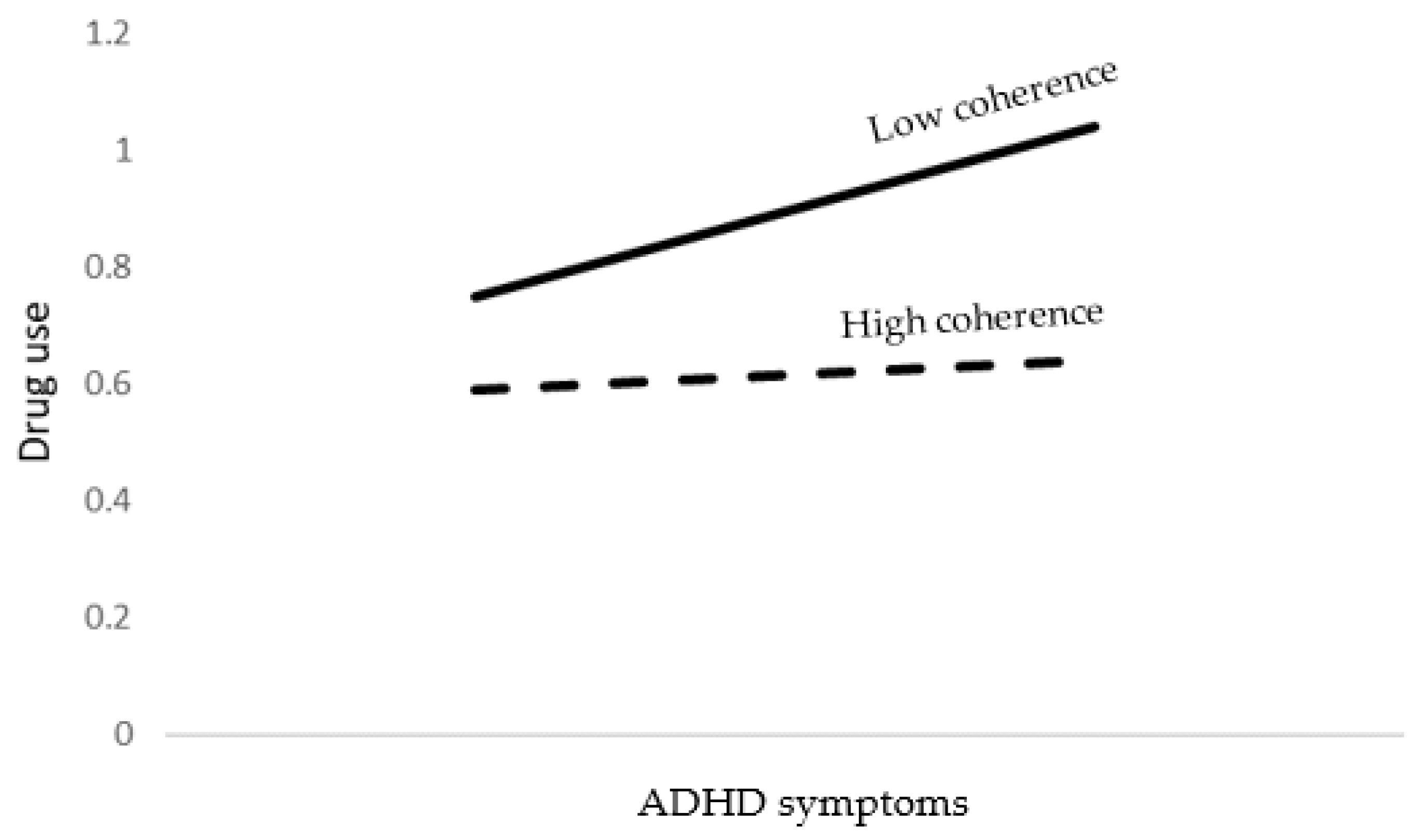
3.3. Moderation Analysis
3.4. Age as a Moderator
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation List
| Amos | Analysis of Moment Structures |
| SOC | Sense Of Coherence |
| ADHD | Attention Deficit Hyperactivity Disorder |
| ICF | International Classification of Functioning, Disability and Health |
| WHO | World Health Organization |
| SWAN | Strengths and Weaknesses of Attention-Deficit/Hyperactivity Symptoms and Normal Behavior |
References
- Faraone, S.V.; Banaschewski, T.; Coghill, D.; Zheng, Y.; Biederman, J.; Bellgrove, M.A.; Newcorn, J.H.; Gignac, M.; Al Saud, N.M.; Manor, I.; et al. The World Federation of ADHD International Consensus Statement: 208 Evidence-based conclusions about the disorder. Neurosci. Biobehav. Rev. 2021, 128, 789–818. [Google Scholar] [CrossRef] [PubMed]
- Cuevas, C.A.; Finkelhor, D.; Shattuck, A.; Turner, H.A.; Hamby, S.L. Children’s exposure to violence and the intersection between delinquency and victimization. In The Societal Burden of Child Abuse; Taylor & Francis Group: London, UK, 2015. [Google Scholar]
- Retz, W.; Ginsberg, Y.; Turner, D.; Barra, S.; Retz-Junginger, P.; Larsson, H.; Asherson, P. Attention-Deficit/Hyperactivity Disorder (ADHD), antisociality and delinquent behavior over the lifespan. Neurosci. Biobehav. Rev. 2020, 120, 236–248. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Cocallis, K. ADHD and offending. J. Neural Transm. 2021, 128, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Baggio, S.; Fructuoso, A.; Guimaraes, M.; Fois, E.; Golay, D.; Heller, P.; Perroud, N.; Aubry, C.; Young, S.; Delessert, D.; et al. Prevalence of Attention Deficit Hyperactivity Disorder in Detention Settings: A Systematic Review and Meta-Analysis. Front. Psychiatry 2018, 9, 331. [Google Scholar] [CrossRef] [Green Version]
- Cherkasova, M.V.; Roy, A.; Molina, B.S.; Scott, G.; Weiss, G.; Barkley, R.A.; Biederman, J.; Uchida, M.; Hinshaw, S.P.; Owens, E.B.; et al. Review: Adult Outcome as Seen through Controlled Prospective Follow-up Studies of Children with Attention-Deficit/Hyperactivity Disorder Followed into Adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2021, 61, 378–391. [Google Scholar] [CrossRef]
- Mohr-Jensen, C.; Steinhausen, H.-C. A meta-analysis and systematic review of the risks associated with childhood attention-deficit hyperactivity disorder on long-term outcome of arrests, convictions, and incarcerations. Clin. Psychol. Rev. 2016, 48, 32–42. [Google Scholar] [CrossRef]
- van der Maas, M.; Kolla, N.J.; Erickson, P.G.; Wickens, C.M.; Mann, R.E.; Vingilis, E. Examining the effect of social bonds on the relationship between ADHD and past arrest in a representative sample of adults. Crim. Behav. Ment. Health 2017, 28, 120–131. [Google Scholar] [CrossRef]
- Breuer, D.; von Wirth, E.; Mandler, J.; Schürmann, S.; Döpfner, M. Predicting delinquent behavior in young adults with a childhood diagnosis of ADHD: Results from the Cologne Adaptive Multimodal Treatment (CAMT) Study. Eur. Child Adolesc. Psychiatry 2020, 31, 553–564. [Google Scholar] [CrossRef]
- García, B.H.; Vázquez, A.L.; Moses, J.O.; Cromer, K.D.; Morrow, A.S.; Villodas, M.T. Risk for substance use among adolescents at-risk for childhood victimization: The moderating role of ADHD. Child Abus. Negl. 2021, 114, 104977. [Google Scholar] [CrossRef]
- Dew, R.E.; Kollins, S.H.; Koenig, H.G. ADHD, Religiosity, and Psychiatric Comorbidity in Adolescence and Adulthood. J. Atten. Disord. 2020, 26, 307–318. [Google Scholar] [CrossRef]
- Giannotta, F.; Rydell, A.M. The prospective links between hyperactive/impulsive, inattentive, and oppositional-defiant behaviors in childhood and antisocial behavior in adolescence: The moderating influence of gender and the parent–child relationship quality. Child Psychiatry Hum. Dev. 2016, 47, 857–870. [Google Scholar] [CrossRef] [PubMed]
- Morse, M. ADHD Symptoms and Alcohol Expectancies: The Moderating Roles of Parenting and School Climate. Ph.D. Thesis, University of South Carolina, Columbia, SC, USA, 2020. [Google Scholar]
- Armeli, S.; Carney, M.A.; Tennen, H.; Affleck, G.; O’Neil, T.P. Stress and alcohol use: A daily process examination of the stressor–vulnerability model. J. Pers. Soc. Psychol. 2000, 78, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Sagar, S. The Role of Protective Factors in Relation to Attentional Abilities in Emerging Adults. Ph.D. Thesis, University of Windsor, Windsor, ON, Canada, 2021. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1987; ISBN 1555420281. [Google Scholar]
- Antonovsky, A. The structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef]
- Haugan, G.; Eriksson, M. Health Promotion in Health Care—Vital Theories and Research; Springer Nature: Cham, Switzerlan, 2021. [Google Scholar]
- Faraone, S.V.; Biederman, J. Can Attention-Deficit/Hyperactivity Disorder Onset Occur in Adulthood? JAMA Psychiatry 2016, 73, 655–656. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.J.; Martin, J.; Lu, Y.; Brikell, I.; Lundström, S.; Larsson, H.; Lichtenstein, P. Association of Genetic Risk Factors for Psychiatric Disorders and Traits of These Disorders in a Swedish Population Twin Sample. JAMA Psychiatry 2019, 76, 280–289. [Google Scholar] [CrossRef]
- Lasky, A.K.; Weisner, T.S.; Jensen, P.S.; Hinshaw, S.P.; Hechtman, L.; Arnold, L.E.; Murray, D.W.; Swanson, J.M. ADHD in context: Young adults’ reports of the impact of occupational environment on the manifestation of ADHD. Soc. Sci. Med. 2016, 161, 160–168. [Google Scholar] [CrossRef] [Green Version]
- Sedgwick, J.A.; Merwood, A.; Asherson, P. The positive aspects of attention deficit hyperactivity disorder: A qualitative investigation of successful adults with ADHD. ADHD Atten. Deficit Hyperact. Disord. 2018, 11, 241–253. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, M.; Lindström, B. Validity of Antonovsky’s sense of coherence scale: A systematic review. J. Epidemiol. Community Health 2005, 59, 460–466. [Google Scholar] [CrossRef]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and its relation with quality of life: A systematic review. J. Epidemiol. Community Health 2007, 61, 938–944. [Google Scholar] [CrossRef] [Green Version]
- Ristkari, T.; Sourander, A.; Ronning, J.; Helenius, H. Self-reported psychopathology, adaptive functioning and sense of coherence, and psychiatric diagnosis among young men: A population-based study. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 523–531. [Google Scholar] [CrossRef]
- Kishi, K.; Suzuki, J.; Monma, T.; Asanuma, T.; Takeda, F. Psychosocial and criminological factors related to recidivism among Japanese criminals at offender rehabilitation facilities. Cogent Soc. Sci. 2018, 4, 1489458. [Google Scholar] [CrossRef]
- Nilsson, K.W.; Starrin, B.; Simonsson, B.; Leppert, J. Alcohol-related problems among adolescents and the role of a sense of coherence. Int. J. Soc. Welf. 2006, 16, 159–167. [Google Scholar] [CrossRef]
- Mattila, M.-L.; Rautava, P.; Honkinen, P.-L.; Ojanlatva, A.; Jaakkola, S.; Aromaa, M.; Suominen, S.; Helenius, H.; Sillanpää, M. Sense of coherence and health behaviour in adolescence. Acta Paediatr. 2011, 100, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Edbom, T.; Malmberg, K.; Lichtenstein, P.; Granlund, M.; Larsson, J.-O.; Rn, T.E.; Larsson, J. High sense of coherence in adolescence is a protective factor in the longitudinal development of ADHD symptoms. Scand. J. Caring Sci. 2010, 24, 541–547. [Google Scholar] [CrossRef]
- Allah-Gholilo, K.; Abolghasemi, A.; Dehghan, H.; Imani, H. The Association of Alexithymia and Sense of Coherence With Life Satisfaction in Attention Deficit Hyperactivity Disorder. Zahedan J. Res. Med. Sci. 2015, 17. [Google Scholar] [CrossRef] [Green Version]
- Elliott, D.S.; Ageton, S.S. Reconciling Race and Class Differences in Self-Reported and Official Estimates of Delinquency. Am. Sociol. Rev. 1980, 45, 95–110. [Google Scholar] [CrossRef]
- Liau, A.K.; Barriga, A.Q.; Gibbs, J.C. Relations between self-serving cognitive distortions and overt vs. Covert antisocial behavior in adolescents. Aggress. Behav. 1998, 24, 335–346. [Google Scholar] [CrossRef]
- Elizur, Y.; Spivak, A.; Ofran, S.; Jacobs, S. A Gender-Moderated Model of Family Relationships and Adolescent Adjustment. J. Clin. Child Adolesc. Psychol. 2007, 36, 430–441. [Google Scholar] [CrossRef]
- Schiff, M.; Benbenishty, R.; Hamburger, R. Adolescents’ Exposure to Negative Life Events and Substance Use: Risk and Protective Factors—Comparison between Adolescents Who Were Born in the Former Soviet Union and Those Who Were Born in Israel; Final report; Israel Anti-Drug Authority: Jerusalem, Pakistan, 2008. [Google Scholar]
- Zohar, A.H.; Konfortes, H. Diagnosing ADHD in Israeli adults: The psychometric properties of the adult ADHD Self Report Scale (ASRS) in Hebrew. Isr. J. Psychiatry Relat. Sci. 2010, 47, 308. [Google Scholar]
- Swanson, J.M.; Schuck, S.; Porter, M.M.; Carlson, C.; Hartman, C.A.; Sergeant, J.A.; Clevenger, W.; Wasdell, M.; McCleary, R.; Lakes, K.; et al. Categorical and Dimensional Definitions and Evaluations of Symptoms of ADHD: History of the SNAP and the SWAN Rating Scales. Int. J. Educ. Psychol. Assess. 2012, 10, 51–70. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Brann, P.; Lethbridge, M.J.; Mildred, H. The young adult Strengths and Difficulties Questionnaire (SDQ) in routine clinical practice. Psychiatry Res. 2018, 264, 340–345. [Google Scholar] [CrossRef]
- Arbuckle, J.L. Ibm Spss Amos 21; Amos Development Corporation: Chicago, IL, USA, 2012. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Mittelmark, M.B.; Bull, T.; Daniel, M.; Urke, H. Specific resistance resources in the salutogenic model of health. In The Handbook of Salutogenesis; Springer: Cham, Switzerlan, 2017. [Google Scholar]
- Feldt, T. The role of sense of coherence in well-being at work: Analysis of main and moderator effects. Work Stress 1997, 11, 134–147. [Google Scholar] [CrossRef]
- World Health Organization. How to Use the ICF: A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF); Exposure draft for comment; WHO: Geneva, Switzerland; Volume 13.
- Davis, L.M. A Study of the Factors Associated with Academic and Vocational Success in Five Women with co-Occurring ADHD and LD; Alliant International University: Alhambra, CA, USA, 2014. [Google Scholar]
- Dvorsky, M.R.; Langberg, J.M. A Review of Factors that Promote Resilience in Youth with ADHD and ADHD Symptoms. Clin. Child Fam. Psychol. Rev. 2016, 19, 368–391. [Google Scholar] [CrossRef] [PubMed]
- Climie, E.A.; Mastoras, S.M. ADHD in schools: Adopting a strengths-based perspective. Can. Psychol. Can. 2015, 56, 295–300. [Google Scholar] [CrossRef]
- Jia, R.M.; Mikami, A.Y.; Normand, S. Social Resilience in Children with ADHD: Parent and Teacher Factors. J. Child Fam. Stud. 2021, 30, 839–854. [Google Scholar] [CrossRef]
- Lee, S.S.; Sibley, M.H.; Epstein, J.N. Attention-deficit/hyperactivity disorder across development: Predictors, resilience, and future directions. J. Abnorm. Psychol. 2016, 125, 151–153. [Google Scholar] [CrossRef]
- Lesch, K.-P. ‘Shine bright like a diamond!’: Is research on high-functioning ADHD at last entering the mainstream? J. Child Psychol. Psychiatry 2017, 59, 191–192. [Google Scholar] [CrossRef] [Green Version]
- Schoenfelder, E.N.; Kollins, S. Topical Review: ADHD and Health-Risk Behaviors: Toward Prevention and Health Promotion. J. Pediatr. Psychol. 2015, 41, 735–740. [Google Scholar] [CrossRef] [Green Version]
- Gudjonsson, G.H.; Gonzalez, R.A.; Young, S. The Risk of Making False Confessions: The Role of Developmental Disorders, Conduct Disorder, Psychiatric Symptoms, and Compliance. J. Atten. Disord. 2019, 25, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Brikell, I.; Kuja-Halkola, R.; Larsson, H. Heritability of attention-deficit hyperactivity disorder in adults. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2015, 168, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.W.; Wu, R.; Helms, K. Performance of the Adult ADHD Self-Report Scale-v1.1 in Adults with Major Depressive Disorder. Behav. Sci. 2018, 8, 37. [Google Scholar] [CrossRef]
- van de Glind, G.; Brink, W.V.D.; Koeter, M.W.; Carpentier, P.-J.; Oortmerssen, K.V.E.-V.; Kaye, S.; Skutle, A.; Bu, E.-T.H.; Franck, J.; Konstenius, M.; et al. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend. 2013, 132, 587–596. [Google Scholar] [CrossRef] [Green Version]
- Cheung, L.; Gunby, P. Crime and mobility during the COVID-19 lockdown: A preliminary empirical exploration. N. Z. Econ. Pap. 2021, 56, 106–113. [Google Scholar] [CrossRef]
- Jensen, J.F.; Egerod, I.; Bestle, M.; Christensen, D.F.; Elklit, A.; Hansen, R.L.; Knudsen, H.; Grode, L.; Overgaard, D. A recovery program to improve quality of life, sense of coherence and psychological health in ICU survivors: A multicenter randomized controlled trial, the RAPIT study. Intensiv. Care Med. 2016, 42, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Mayer, C.-H.; Boness, C. Interventions to promoting sense of coherence and transcultural competences in educational contexts. Int. Rev. Psychiatry 2011, 23, 516–524. [Google Scholar] [CrossRef]
- Odajima, Y.; Kawaharada, M.; Wada, N. Development and validation of an educational program to enhance sense of coherence in patients with diabetes mellitus type 2. Nagoya J. Med. Sci. 2017, 79, 363–374. [Google Scholar] [CrossRef]
- Tan, K.K.; Chan, S.W.-C.; Wang, W.; Vehviläinen-Julkunen, K. A salutogenic program to enhance sense of coherence and quality of life for older people in the community: A feasibility randomized controlled trial and process evaluation. Patient Educ. Couns. 2016, 99, 108–116. [Google Scholar] [CrossRef]
- Uzdil, N.; Ceyhan, Ö.; Şimşek, N. The effect of salutogenesis-based care on the sense of coherence in peritoneal dialysis patients. J. Clin. Nurs. 2021, 31, 184–195. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Median | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|
| Religiosity | 3165 | 3.00 | 2.76 | 1.44 | 0.00 | 4.00 |
| Emotional symptoms | 2804 | 1.40 | 1.56 | 0.48 | 1.00 | 3.00 |
| ADHD symptoms | 3179 | 1.28 | 1.37 | 0.72 | 0.00 | 4.00 |
| Coherence | 2963 | 4.92 | 4.78 | 1.16 | 1.00 | 7.00 |
| Severe physical antisocial behavior | 3079 | 0.00 | 0.11 | 0.35 | 0.00 | 4.00 |
| Mild physical antisocial behavior | 3079 | 0.00 | 0.24 | 0.52 | 0.00 | 4.00 |
| Verbal antisocial behavior | 3079 | 0.75 | 1.01 | 0.93 | 0.00 | 4.00 |
| Property crimes | 3079 | 0.00 | 0.09 | 0.33 | 0.00 | 4.00 |
| Public order crimes | 3070 | 0.33 | 0.51 | 0.76 | 0.00 | 4.00 |
| Drug use | 2834 | 0.40 | 0.77 | 1.13 | 0.00 | 7.00 |
| ADHD | Severe Physical Antisocial Behavior | Mild Physical Antisocial Behavior | Verbal Antisocial Behavior | Property Crimes | Public Order Crimes | Drug Use | Coherence | |
|---|---|---|---|---|---|---|---|---|
| ADHD symptoms | 1.000 | |||||||
| Severe physical antisocial behavior | 0.175 ** | 1.000 | ||||||
| Mild physical antisocial behavior | 0.207 ** | 0.542 ** | 1.000 | |||||
| Verbal antisocial behavior | 0.234 ** | 0.403 ** | 0.520 ** | 1.000 | ||||
| Property crimes | 0.176 ** | 0.459 ** | 0.418 ** | 0.365 ** | 1.000 | |||
| Public order crimes | 0.246 ** | 0.335 ** | 0.382 ** | 0.464 ** | 0.346 ** | 1.000 | ||
| Drug use | 0.117 ** | 0.130 ** | 0.143 ** | 0.203 ** | 0.186 ** | 0.254 ** | 1.000 | |
| Coherence | −0.424 ** | −0.195 ** | −0.283 ** | −0.363 ** | −0.259 ** | −0.288 ** | −0.086 ** | 1.000 |
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.127 | 0.062 | 0.009 | 6.79 | <0.001 | 0.041 | 0.083 |
| Coherence | −0.190 | −0.057 | 0.007 | −8.51 | <0.001 | −0.077 | −0.043 |
| ADHD symptoms × Coherence | −0.172 | −0.061 | 0.006 | −10.18 | <0.001 | −0.089 | −0.034 |
| Age | −0.159 | −0.143 | 0.015 | −9.48 | <0.001 | −0.191 | −0.102 |
| Gender | −0.094 | −0.066 | 0.012 | −5.58 | <0.001 | −0.089 | −0.039 |
| Religiosity | −0.006 | −0.002 | 0.004 | −0.37 | 0.711 | −0.010 | 0.007 |
| Emotional symptoms | −0.105 | −0.076 | 0.016 | −4.87 | <0.001 | −0.122 | −0.041 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.299 | 0.133 | 0.011 | 12.76 | <0.001 | 0.113 | 0.154 |
| High coherence | −0.045 | −0.009 | 0.012 | −0.68 | 0.491 | −0.033 | 0.016 |
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.102 | 0.074 | 0.013 | 5.57 | <0.001 | 0.049 | 0.103 |
| Coherence | −0.311 | −0.138 | 0.010 | −14.28 | <0.001 | −0.171 | −0.117 |
| ADHD symptoms × Coherence | −0.135 | −0.070 | 0.009 | −8.17 | <0.001 | −0.098 | −0.044 |
| Age | −0.186 | −0.247 | 0.022 | −11.34 | <0.001 | −0.311 | −0.183 |
| Gender | −0.099 | −0.103 | 0.017 | −6.00 | <0.001 | −0.139 | −0.073 |
| Religiosity | 0.056 | 0.020 | 0.006 | 3.35 | <0.001 | 0.011 | 0.038 |
| Emotional symptoms | −0.109 | −0.116 | 0.022 | −5.19 | <0.001 | −0.171 | −0.069 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.237 | 0.156 | 0.015 | 10.35 | <0.001 | 0.126 | 0.185 |
| High coherence | −0.033 | −0.008 | 0.018 | −0.46 | 0.643 | −0.044 | 0.027 |
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.098 | 0.128 | 0.023 | 5.46 | <0.001 | 0.088 | 0.168 |
| Coherence | −0.371 | −0.297 | 0.017 | −17.31 | <0.001 | −0.334 | −0.264 |
| ADHD symptoms × Coherence | −0.059 | −0.055 | 0.015 | −3.65 | <0.001 | −0.088 | −0.029 |
| Age | −0.159 | −0.380 | 0.038 | −9.89 | <0.001 | −0.468 | −0.278 |
| Gender | −0.113 | −0.211 | 0.030 | −6.97 | <0.001 | −0.285 | −0.156 |
| Religiosity | −0.051 | −0.033 | 0.011 | −3.11 | 0.002 | −0.053 | −0.014 |
| Emotional symptoms | −0.108 | −0.207 | 0.040 | −5.23 | <0.001 | −0.296 | −0.127 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.157 | 0.19 | 0.027 | 7.23 | <0.001 | 0.140 | 0.245 |
| High coherence | 0.039 | 0.63 | 0.032 | 1.97 | 0.048 | 0.001 | 0.126 |
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.063 | 0.029 | 0.009 | 3.29 | 0.001 | 0.001 | 0.046 |
| Coherence | −0.190 | −0.053 | 0.006 | −8.34 | <0.001 | −0.069 | −0.040 |
| ADHD symptoms × Coherence | −0.135 | −0.044 | 0.006 | −7.78 | <0.001 | −0.079 | −0.022 |
| Age | −0.109 | −0.091 | 0.014 | −6.34 | <0.001 | −0.134 | −0.049 |
| Gender | −0.112 | −0.073 | 0.011 | −6.50 | <0.001 | −0.104 | −0.049 |
| Religiosity | −0.081 | −0.018 | 0.004 | −4.62 | <0.001 | −0.027 | −0.009 |
| Emotional symptoms | −0.065 | −0.043 | 0.015 | −2.94 | 0.003 | −0.073 | −0.016 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.198 | 0.080 | 0.010 | 8.08 | <0.001 | 0.061 | 0.099 |
| High coherence | −0.072 | −0.023 | 0.012 | −1.91 | 0.055 | −0.046 | 0.001 |
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.166 | 0.176 | 0.019 | 9.09 | <0.001 | 0.135 | 0.212 |
| Coherence | −0.279 | −0.182 | 0.014 | −12.84 | <0.001 | −0.213 | −0.145 |
| ADHD symptoms × Coherence | −0.099 | −0.075 | 0.013 | −5.99 | <0.001 | −0.104 | −0.046 |
| Age | −0.164 | −0.319 | 0.032 | −10.05 | <0.001 | −0.404 | −0.251 |
| Gender | −0.072 | −0.110 | 0.025 | −4.41 | <0.001 | −0.159 | −0.064 |
| Religiosity | −0.096 | −0.051 | 0.009 | −5.75 | <0.001 | −0.070 | −0.033 |
| Emotional symptoms | −0.154 | −0.241 | 0.033 | −7.36 | <0.001 | −0.304 | −0.174 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.265 | 0.264 | 0.022 | 11.99 | <0.001 | 0.221 | 0.307 |
| High coherence | 0.067 | 0.088 | 0.026 | 3.33 | <0.001 | 0.036 | 0.139 |
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.075 | 0.119 | 0.029 | 4.09 | <0.001 | 0.070 | 0.188 |
| Coherence | −0.122 | −0.118 | 0.021 | −5.55 | <0.001 | −0.165 | −0.074 |
| ADHD symptoms × Coherence | −0.062 | −0.071 | 0.019 | −3.73 | <0.001 | −0.118 | −0.023 |
| Age | 0.092 | 0.267 | 0.048 | 5.59 | <0.001 | 0.166 | 0.386 |
| Gender | −0.323 | −0.732 | 0.038 | −19.43 | <0.001 | −0.814 | −0.656 |
| Religiosity | −0.235 | −0.185 | 0.013 | −13.96 | <0.001 | −0.216 | −0.156 |
| Emotional symptoms | −0.067 | −0.156 | 0.049 | −3.17 | 0.002 | −0.261 | −0.060 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.137 | 0.201 | 0.033 | 6.08 | <0.001 | 0.137 | 0.266 |
| High coherence | 0.013 | 0.036 | 0.040 | 0.92 | 0.355 | −0.041 | 0.115 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dayan, H.; Khoury-Kassabri, M.; Pollak, Y. The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence. Brain Sci. 2022, 12, 1336. https://doi.org/10.3390/brainsci12101336
Dayan H, Khoury-Kassabri M, Pollak Y. The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence. Brain Sciences. 2022; 12(10):1336. https://doi.org/10.3390/brainsci12101336
Chicago/Turabian StyleDayan, Haym, Mona Khoury-Kassabri, and Yehuda Pollak. 2022. "The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence" Brain Sciences 12, no. 10: 1336. https://doi.org/10.3390/brainsci12101336
APA StyleDayan, H., Khoury-Kassabri, M., & Pollak, Y. (2022). The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence. Brain Sciences, 12(10), 1336. https://doi.org/10.3390/brainsci12101336