

Vortioxetine Improves Depressive Symptoms and Cognition in Parkinson’s Disease Patients with Major Depression: An Open-Label Prospective Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Analysis
2.2. Data Availability
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Reijnders, J.S.A.M.; Ehrt, U.; Weber, W.E.J.; Aarsland, D.; Leentjens, A.F.G. A systematic review of prevalence studies of depression in Parkinson’s disease. Mov. Disord. 2007, 23, 183–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.C. Mood disorders in Parkinson’s disease. Park. Relat. Disord. 2012, 18 (Suppl. 1), S74–S76. [Google Scholar] [CrossRef]
- Schrag, A. Quality of life and depression in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, S.; Currie, L.J.; Wooten, G.F. Depression is associated with impairment of ADL, not motor function in Parkinson disease. Neurology 2005, 64, 2134–2135. [Google Scholar] [CrossRef] [PubMed]
- Bomasang-Layno, E.; Fadlon, I.; Murray, A.N.; Himelhoch, S. Antidepressive treatments for Parkinson’s disease: A systematic review and meta-analysis. Park. Relat. Disord. 2015, 21, 833–842. [Google Scholar] [CrossRef] [Green Version]
- Seppi, K.; Ray Chaudhuri, K.; Coelho, M.; Fox, S.H.; Katzenschlager, R.; Perez Lloret, S.; Weintraub, D.; Sampaio, C.; the collaborators of the Parkinson’s Disease Update on Non-Motor Symptoms Study Group on behalf of the Movement Disorders Society Evidence-Based Medicine Committee. Update on treatments for nonmotor symptoms of Parkinson’s disease-an evidence-based medicine review. Mov. Disord. 2019, 34, 180–198. [Google Scholar] [CrossRef] [Green Version]
- Bang-Andersen, B.; Ruhland, T.; Jørgensen, M.; Smith, G.; Frederiksen, K.; Jensen, K.G.; Zhong, H.; Nielsen, S.M.; Hogg, S.; Mørk, A.; et al. Discovery of 1-[2-(2,4-Dimethylphenylsulfanyl)phenyl]piperazine (Lu AA21004): A Novel Multimodal Compound for the Treatment of Major Depressive Disorder. J. Med. Chem. 2011, 54, 3206–3221. [Google Scholar] [CrossRef]
- Sanchez, C.; Asin, K.E.; Artigas, F. Vortioxetine, a novel antidepressant with multimodal activity: Review of preclinical and clinical data. Pharmacol. Ther. 2015, 145, 43–57. [Google Scholar] [CrossRef]
- Bobo, W.; Kelliny, M.; Croarkin, P.; Moore, K. Profile of vortioxetine in the treatment of major depressive disorder: An overview of the primary and secondary literature. Ther. Clin. Risk Manag. 2015, 11, 1193–1212. [Google Scholar] [CrossRef] [Green Version]
- Rosenblat, J.D.; Kakar, R.; McIntyre, R.S. The Cognitive Effects of Antidepressants in Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Neuropsychopharmacol. 2015, 19, pyv082. [Google Scholar] [CrossRef]
- Cumbo, E.; Cumbo, S.; Torregrossa, S.; Migliore, D. Treatment Effects of Vortioxetine on Cognitive Functions in Mild Alzheimer’s Disease Patients with Depressive Symptoms: A 12 Month, Open-Label, Observational Study. J. Prev. Alzheimers Dis. 2019, 6, 192–197. [Google Scholar] [CrossRef]
- Baune, B.T.; Sluth, L.B.; Olsen, C.K. The effects of vortioxetine on cognitive performance in working patients with major depressive disorder: A short-term, randomized, double-blind, exploratory study. J. Affect. Disord. 2017, 229, 421–428. [Google Scholar] [CrossRef]
- McIntyre, R.S.; Lophaven, S.; Olsen, C.K. A randomized, double-blind, placebo-controlled study of vortioxetine on cognitive function in depressed adults. Int. J. Neuropsychopharmacol. 2014, 17, 1557–1567. [Google Scholar] [CrossRef]
- Mahableshwarkar, A.R.; Zajecka, J.; Jacobson, W.; Chen, Y.; E Keefe, R.S. A Randomized, Placebo-Controlled, Active-Reference, Double-Blind, Flexible-Dose Study of the Efficacy of Vortioxetine on Cognitive Function in Major Depressive Disorder. Neuropsychopharmacology 2015, 40, 2025–2037. [Google Scholar] [CrossRef] [Green Version]
- Yee, A.; Ng, C.G.; Seng, L.H. Vortioxetine Treatment for Anxiety Disorder: A Meta-Analysis Study. Curr. Drug Targets 2018, 19, 1412–1423. [Google Scholar] [CrossRef]
- Adamo, D.; Pecoraro, G.; Aria, M.; Favia, G.; Mignogna, M.D. Vortioxetine in the Treatment of Mood Disorders Associated with Burning Mouth Syndrome: Results of an Open-Label, Flexible-Dose Pilot Study. Pain Med. 2020, 21, 185–194. [Google Scholar] [CrossRef]
- Cao, B.; Park, C.; Rosenblat, J.D.; Chen, Y.; Iacobucci, M.; Subramaniapillai, M.; Mansur, R.B.; Zuckerman, H.; Lee, Y.; McIntyre, R.S. Changes in sleep predict changes in depressive symptoms in depressed subjects receiving vortioxetine: An open-label clinical trial. J. Psychopharmacol. 2019, 33, 1388–1394. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Schapira, A.H. Non-motor symptoms of Parkinson’s disease: Dopaminergic pathophysiology and treatment. Lancet Neurol. 2009, 8, 464–474. [Google Scholar] [CrossRef]
- Russo, M.; Carrarini, C.; Dono, F.; Ferri, L.; Di Pietro, M.; Onofrj, M. Vortioxetine treatment of depression in Parkinson’s disease [abstract]. In Movement Disorders; 111 RIVER ST, HOBOKEN 07030-5774; Wiley: New York, NJ, USA, 2019; Volume 34, pp. S80–S81. [Google Scholar]
- Miliukhina, I.V. The use of vortioxetine for depression in patients with Parkinson’s disease in the early and advanced stages of the disease. Neurol. Neuropsychiatry Psychosom. 2020, 12, 40–45. [Google Scholar] [CrossRef]
- Barbato, G.; Marano, P.; Passarella, B.; Pilotto, A.; Riboldazzi, G.; Spagnolo, F.; Vanni, P. Vortioxetine for the treatment of depressive episodes associated with Parkinson’s disease: A case series of six patients. J. Psychopathol. 2020, 26, 248–255. [Google Scholar]
- Yoshimura, R.; Ikenouchi, A.; Okamoto, N.; Konishi, Y. Vortioxetine Improved Depressive State In Parkinson’s Disease. Cureus 2021, 13, e15750. [Google Scholar] [CrossRef] [PubMed]
- Daniel, S.E.; Lees, A.J. Parkinson’s Disease Society Brain Bank, London: Overview and research. J. Neural Transm. Suppl. 1993, 39, 165–172. [Google Scholar] [PubMed]
- DSM-IV-TR. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Naarding, P.; Leentjens, A.F.G.; Van Kooten, F.; Verhey, F.R. Disease-specific properties of the Hamilton Rating Scale for depression in patients with stroke, Alzheimer’s dementia, and Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Burn, D.; Goetz, C.; Aarsland, D.; Brown, R.G.; Broe, G.; Dickson, D.; Duyckaerts, C.; Cummings, J.; Gauthier, S.; et al. Diagnostic procedures for Parkinson’s disease dementia: Recommendations from the movement disorder society task force. Mov. Disord. 2007, 22, 2314–2324. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Fanhn, S.; Elton, R.L. Members of the UPDRS Development Committee. Unified Parkinson’s Disease Rating Scale. In Recent Developments in Parkinson’s Disease; Fahn, S., Marsden, C.D., Calne, D.B., Goldstein, M., Eds.; Macmillan Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–164. [Google Scholar]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.J.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, validity, and clinical correlates of apathy in Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar]
- Pagonabarraga, J.; Kulisevsky, J.; Llebaria, G.; García-Sánchez, C.; Pascual-Sedano, B.; Gironell, A. Parkinson’s disease-cognitive rating scale: A new cognitive scale specific for Parkinson’s disease. Mov. Disord. 2008, 23, 998–1005. [Google Scholar] [CrossRef]
- Krupp, L.B.; Pollina, D.A. Mechanisms and management of fatigue in progressive neurological disorders. Curr. Opin. Neurol. 1996, 9, 456–460. [Google Scholar] [CrossRef]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson’s Disease Questionnaire (PDQ-39): Development and validation of a Parkinson’s disease summary index score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Da Rocha, N.S.; Power, M.J.; Bushnell, D.M.; Fleck, M.P. The EUROHIS-QOL 8-item index: Comparative psychometric properties to its parent WHOQOL-BREF. Value Health 2012, 15, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Schwab, R.S.; England, A.C. Projection Technique for Evaluating Surgery in Parkinson’s Disease. In Proceedings of the Third Symposium on Parkinson’s Disease, Edingurgh, Scotland, 21–22 May 1968; E. And S. Livingstone: Edinburgh, UK, 1969; pp. 152–157. [Google Scholar]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs, Eds.; U.S. Dept. of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs: Rockville, MD, USA, 1976; pp. 218–222. [Google Scholar]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Schade, S.; Mollenhauer, B.; Trenkwalder, C. Levodopa Equivalent Dose Conversion Factors: An Updated Proposal Including Opicapone and Safinamide. Mov. Disord. Clin. Pr. 2020, 7, 343–345. [Google Scholar] [CrossRef]
- Aarsland, D.; Påhlhagen, S.; Ballard, C.G.; Ehrt, U.; Svenningsson, P. Depression in Parkinson disease--epidemiology, mechanisms and management. Nat. Rev. Neurol. 2011, 8, 35–47. [Google Scholar] [CrossRef]
- Schrag, A.; Jahanshahi, M.; Quinn, N. What contributes to quality of life in patients with Parkinson’s disease? J. Neurol. Neurosurg. Psychiatry 2000, 69, 308–312. [Google Scholar] [CrossRef] [Green Version]
- Santos García, D.; de Deus Fonticoba, T.; Cores, C.; Muñoz, G.; Paz González, J.M.; Martínez Miró, C.; Suárez, E.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. COPPADIS Study Group. Predictors of clinically significant quality of life impairment in Parkinson’s disease. NPJ Park. Dis. 2021, 7, 118. [Google Scholar] [CrossRef]
- Santos-García, D.; de Deus Fonticoba, T.; Cores Bartolomé, C.; Íñiguez Alvarado, M.C.; Feal Panceiras, M.J.; Suárez Castro, E.; Canfield, H.; Martínez Miró, C.; Jesús, S.; Aguilar, M.; et al. Predictors of the change in burden, strain, mood, and quality of life among caregivers of Parkinson’s disease patients. Int. J. Geriatr. Psychiatry 2022, 37. [Google Scholar] [CrossRef]
- Kano, O.; Ikeda, K.; Cridebring, D.; Takazawa, T.; Yoshii, Y.; Iwasaki, Y. Neurobiology of depression and anxiety in Parkinson’s disease. Parkinsons Dis. 2011, 2011, 143547. [Google Scholar] [CrossRef] [Green Version]
- Barone, P.; Poewe, W.; Albrecht, S.; Debieuvre, C.; Massey, D.; Rascol, O.; Tolosa, E.; Weintraub, D. Pramipexole for the treatment of depressive symptoms in patients with Parkinson’s disease: A randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2010, 9, 573–580. [Google Scholar] [CrossRef]
- Menza, M.; Dobkin, R.D.; Marin, H.; Mark, M.H.; Gara, M.; Buyske, S.; Bienfait, K.; Dicke, A. A controlled trial of antidepressants in patients with Parkinson disease and depression. Neurology 2009, 72, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Tolosa, E.; Gaig, C.; Santamaría, J.; Compta, Y. Diagnosis and the premotor phase of Parkinson’s disease. Neurology 2009, 72 (Suppl. 7), 12–20. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, A.; English, C.D.; Rey, J.A. Vortioxetine (brintellix): A new serotonergic antidepressant. P T J. Formul. Manag. 2015, 40, 36–40. [Google Scholar]
- Pae, C.-U.; Wang, S.-M.; Han, C.; Lee, S.-J.; Patkar, A.A.; Masand, P.S.; Serretti, A. Vortioxetine: A meta-analysis of 12 short-term, randomized, placebo-controlled clinical trials for the treatment of major depressive disorder. J. Psychiatry Neurosci. 2015, 40, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Thase, M.E.; Mahableshwarkar, A.R.; Dragheim, M.; Loft, H.; Vieta, E. A meta-analysis of randomized, placebo-controlled trials of vortioxetine for the treatment of major depressive disorder in adults. Eur. Neuropsychopharmacol. 2016, 26, 979–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koesters, M.; Ostuzzi, G.; Guaiana, G.; Breilmann, J.; Barbui, C. Vortioxetine for depression in adults. Cochrane Database Syst. Rev. 2017, 7, CD011520. [Google Scholar] [CrossRef] [PubMed]
- Katona, C.; Hansen, T.; Olsen, C.K. A randomized, doubleblind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Int. Clin. Psychopharmacol. 2012, 27, 215–223. [Google Scholar] [CrossRef]
- Henigsberg, N.; Mahableshwarkar, A.R.; Jacobsen, P.; Chen, Y.; Thase, M.E. A randomized, double-blind, placebo-controlled 8-week trial of the efficacy and tolerability of multiple doses of Lu AA21004 in adults with major depressive disorder. J. Clin. Psychiatry 2012, 73, 953–959. [Google Scholar] [CrossRef]
- Jain, R.; Mahableshwarkar, A.R.; Jacobsen, P.L.; Chen, Y.; Thase, M.E. A randomized, double-blind, placebo-controlled 6-wk trial of the efficacy and tolerability of 5 mg vortioxetine in adults with major depressive disorder. Int. J. Neuropsychopharmacol. 2012, 16, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Mahableshwarkar, A.R.; Jacobsen, P.L.; Chen, Y. A randomized, double-blind trial of 2.5 mg and 5 mg vortioxetine (LuAA21004) versus placebo for 8 weeks in adults with major depressive disorder. Curr. Med. Res. Opin. 2013, 29, 217–226. [Google Scholar] [CrossRef]
- Baldwin, D.S.; Hansen, T.; Florea, I. Vortioxetine (Lu AA21004) in the long-term open-label treatment of major depressive disorder. Curr. Med. Res. Opin. 2012, 28, 1717–1724. [Google Scholar] [CrossRef]
- Frampton, J.E. Vortioxetine: A Review in Cognitive Dysfunction in Depression. Drugs 2016, 76, 1675–1682. [Google Scholar] [CrossRef]
- Harrison, J.E.; Lophaven, S.; Olsen, C.K. Which Cognitive Domains are Improved by Treatment with Vortioxetine? Int. J. Neuropsychopharmacol. 2016, 19, pyw054. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Baik, S.Y.; Kim, Y.W.; Lee, S. Improved cognitive function in patients with major depressive disorder after treatment with vortioxetine: A EEG study. Neuropsychopharmacol. Rep. 2021, 42, 21–31. [Google Scholar] [CrossRef]
- Jeong, H.W.; Yoon, K.H.; Lee, C.H.; Moon, Y.S.; Kim, D.H. Vortioxetine Treatment for Depression in Alzheimer’s Disease: A Randomized, Double-blind, Placebo-controlled Study. Clin. Psychopharmacol. Neurosci. 2022, 20, 311–319. [Google Scholar] [CrossRef]
- Bennabi, D.; Haffen, E.; Van Waes, V. Vortioxetine for Cognitive Enhancement in Major Depression: From Animal Models to Clinical Research. Front. Psychiatry 2019, 10, 771. [Google Scholar] [CrossRef] [Green Version]
- Kehagia, A.A.; Barker, R.A.; Robbins, T.W. Cognitive impairment in Parkinson’s disease: The dual syndrome hypothesis. Neurodegener. Dis. 2012, 11, 79–92. [Google Scholar] [CrossRef] [Green Version]
- Skorvanek, M.; Gdovinova, Z.; Rosenberger, J.; Ghorbani Saeedian, R.; Nagyova, I.; Groothoff, J.W.; Van Dijk, J.P. The associations between fatigue, apathy, and depression in Parkinson’s disease. Acta Neurol. Scand. 2015, 131, 80–87. [Google Scholar] [CrossRef]
- Christensen, M.C.; Florea, I.; Lindsten, A.; Baldwin, D.S. Efficacy of vortioxetine on the physical symptoms of major depressive disorder. J. Psychopharmacol. 2018, 32, 1086–1097. [Google Scholar] [CrossRef] [Green Version]
- Florea, I.; Danchenko, N.; Brignone, M.; Loft, H.; Rive, B.; Abetz-Webb, L. The effect of vortioxetine on health-related quality of life in patients with major depressive disorder. Clin. Ther. 2015, 37, 2309–2323.e6. [Google Scholar] [CrossRef] [Green Version]
- Ekhart, C.; van Hunsel, F.; van Puijenbroek, E.; Chandler, R.; Meldau, E.-L.; Taavola, H.; Norén, G.N. Post-Marketing Safety Profile of Vortioxetine Using a Cluster Analysis and a Disproportionality Analysis of Global Adverse Event Reports. Drug Saf. 2022, 45, 145–153. [Google Scholar] [CrossRef]
- Baldwin, D.S.; Chrones, L.; Florea, I.; Nielsen, R.; Nomikos, G.G.; Palo, W.; Reines, E. The safety and tolerability of vortioxetine: Analysis of data from randomized placebo-controlled trials and open-label extension studies. J. Psychopharmacol. 2016, 30, 242–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemutlu Samur, D.; Akçay, G.; Yıldırım, S.; Özkan, A.; Çeker, T.; Derin, N.; Tanrıöver, G.; Aslan, M.; Ağar, A.; Özbey, G. Vortioxetine ameliorates motor and cognitive impairments in the rotenone-induced Parkinson’s disease via targeting TLR-2 mediated neuroinflammation. Neuropharmacology 2022, 208, 108977. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age | 66.23 ± 10.27 (48–83) | Family cases of depression (%) | 33.3 |
| Gender (males) (%) | 73.3 | Family cases of PD (%) | 26.7 |
| Race (%) | |||
| Caucasian | 100 | Time from symptoms onset | 4.16 ± 3.11 (0.33–11) |
| Other | 0 | ||
| Motor fluctuations (%) | 60 | ||
| Civil status (%): | Dyskinesia (%) | 23.3 | |
| Married | 53.3 | ||
| Widowed | 23.3 | Treatment for PD (%): | |
| Single | 10 | Levodopa | 96.7 |
| Divorced | 10 | MAO-B inhibitor | 76.7 |
| Other | 3.4 | COMT inhibitor | 23.3 |
| Dopamine agonist | 60 | ||
| Living style (%) | Amantadine | 6.7 | |
| With the partner | 56.7 | ||
| Alone | 20 | L-dopa daily dose (mg) | 505.71 ± 392.56 (0–1910) |
| With a son/daughter | 20 | LEDD (mg) | 765.25 ± 477.63 (100–2150) |
| Other | 3.3 | ||
| Other treatments (%): | |||
| Habitat (%): | Amitriptiline | 6.6 | |
| Rural (<5000) | 10 | Trazodone | 10 |
| Semiurban (5000–20,000) | 26.7 | Mirtazapine | 3.3 |
| Urban (>20,000) | 63.3 | Benzodiazepine | 43.3 |
| Antipsychotic | 3.3 | ||
| Comorbidities (%): | Analgesic | 20 | |
| Arterial hypertension | 40 | ||
| Diabetes mellitus | 6.7 | Number of anti-PD drugs | 2.86 ± 1.3 (1–6) |
| Dyslipemia | 36.7 | Number of non-PD drugs | 2.82 ± 2.8 (0–9) |
| Hiperuricemia | 3.3 | Total number of drugs | 5.68 ± 2.96 (1–13) |
| Cardiomyopathy | 3.3 | Number of pills for PD | 4.87 ± 2.26 (1–9.5) |
| Cardiac arrhythmia | 3.3 | Number of pills for other cause | 2.62 ± 2.49 (0–8.5) |
| Smoking | 6.7 | Total number of pills | 7.5 ± 2.68 (3–13.75) |
| Alcohol consumption | 0 |
| VB | V12w | Cohen’s d | ∆VB–V12w | p | |
|---|---|---|---|---|---|
| MOTOR ASSESSMENT | |||||
| H&Y-ON | 2 (1.75–2) | N.A. | N. A | N.A. | N.A. |
| UPDRS-III-ON | 23.1 ± 9.85 (9–51) | 21.63 ± 8.28 (7–39) | −0.21 | −6.90% | 0.483 |
| UPDRS−IV | 2.53 ± 2.04 | N.A. | N.A. | N.A. | N.A. |
| NON MOTOR ASSESSMENT | |||||
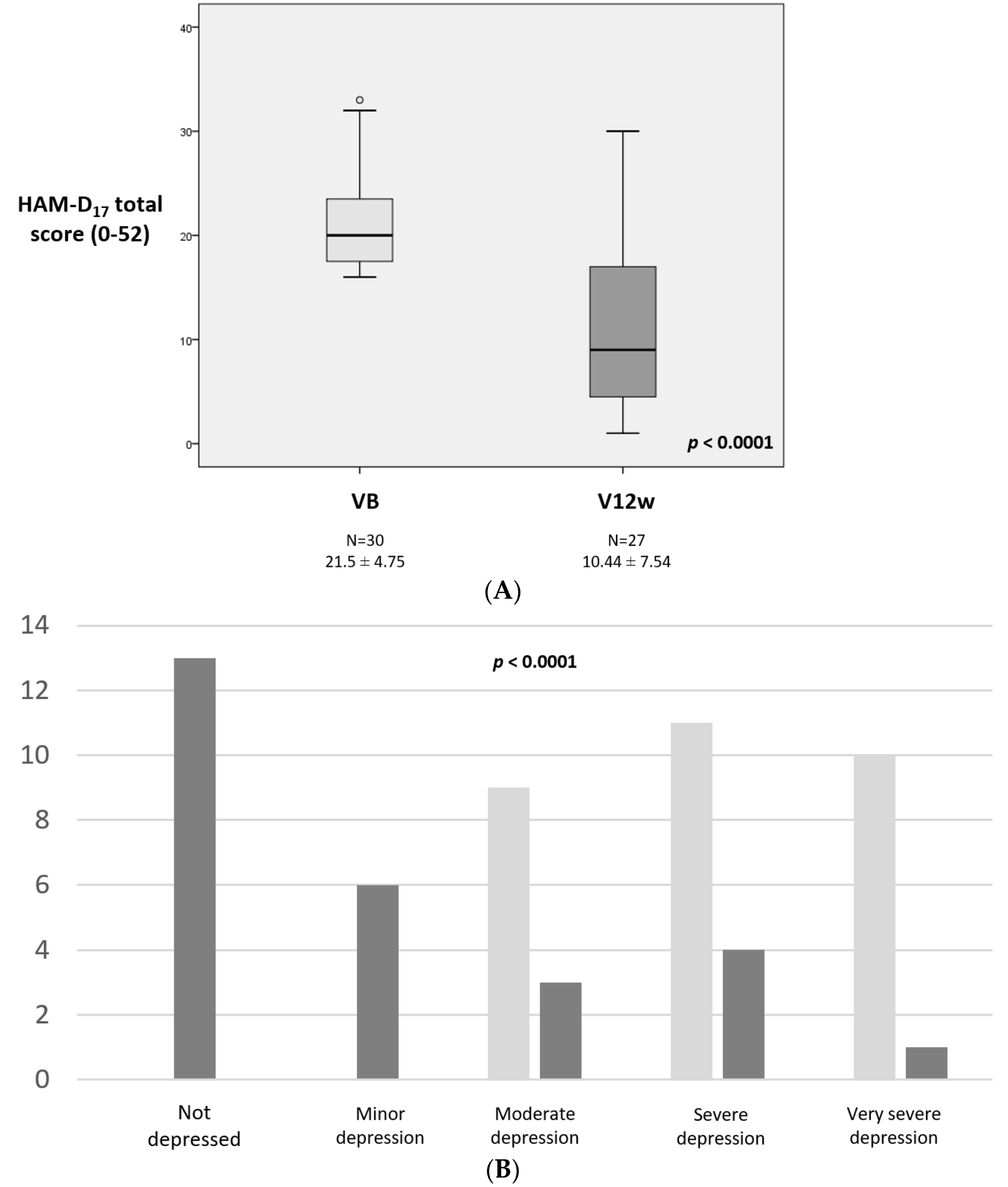
| HAM-D17 | 21.5 ± 4.75 (16–33) | 10.44 ± 7.54 (1–30) | −2.5 | −52.70% | <0.0001 |
| AS | 17.6 ± 6.54 (1–31) | 11.29 ± 7.18 (1–26) | −1.3 | −35.10% | <0.0001 |
| PD-CRS | 80.66 ± 19.14 (29–116) | 86.81 ± 20.45 (38–127) | 0.8 | 7.94% | 0.007 |
| PD-CRS FS sub-score | 54.17 ± 18.19 | 59 ± 18.96 | 0.39 | 8.90% | 0.104 |
| Immediate verbal memory | 7.3 ± 2.03 (4–12) | 7.85 ± 2.14 (4–12) | 0.46 | 7.50% | 0.091 |
| Sustained attention | 7.37 ± 3.21 (0–10) | 8.33 ± 2.07 (2–10) | 0.49 | 13% | 0.094 |
| Working memory | 5.9 ± 2.67 (0–9) | 6.19 ± 2.2 (0–19) | 0.08 | 4.90% | 0.946 |
| Clock drawing | 8.57 ± 2.3 (1–10) | 9 ± 1.54 (5–10) | 0.16 | 5% | 0.711 |
| Delayed verbal memory | 4.4 ± 2.67 (0–11) | 4.96 ± 2.54 (0–10) | 0.54 | 12.70% | 0.047 |
| Alternating verbal fluency | 9.67 ± 4.22 (2–17) | 10.7 ± 4.71 (2–20) | 0.48 | 10.60% | 0.114 |
| Action verbal fluency | 12.53 ± 4.68 (5–24) | 13.07 ± 5.61 (6–27) | 0.25 | 4.30% | 0.654 |
| PD-CRS PC sub-score | 26.5 ± 8.94 | 27.81 ± 7.06 | 0.44 | 4.90% | 0.098 |
| Confrontation naming | 15.57 ± 4.98 (7–24) | 17.48 ± 3.78 (8–26) | 0.46 | 12.30% | 0.067 |
| Clock copy | 9.2 ± 2.14 (1–10) | 9.37 ± 1.36 (4–10) | 0.22 | 1.80% | 0.566 |
| FSS | 38.7 ± 18.49 (9–76) | 29.04 ± 16.3 (9–60) | −0.77 | −27.90% | 0.014 |
| QOL AND AUTONOMY | |||||
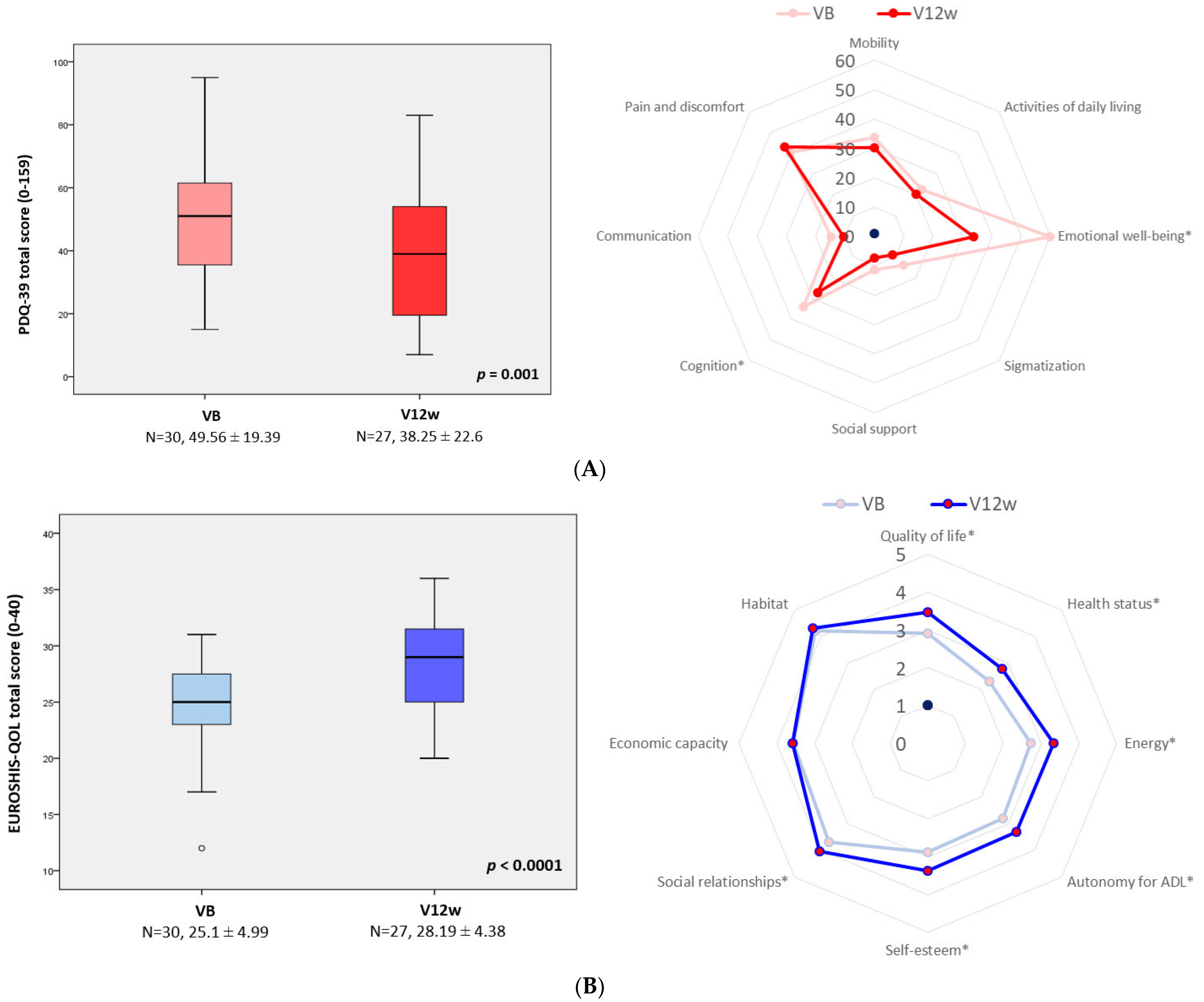
| PDQ-39 | 49.56 ± 19.39 (15–95) | 38.25 ± 22.6 (7–83) | −0.78 | −23.80% | 0.001 |
| Mobility | 33.83 ± 22 (0–35) | 30.37 ± 24.27 (0–35) | −0.26 | −10.20% | 0.109 |
| Activities of daily living | 22.64 ± 18.94 (0–18) | 20.22 ± 18.37 (0–16) | −0.23 | −10.70% | 0.273 |
| Emotional well-being | 59.72 ± 24.05 (1–24) | 33.95 ± 24.23 (0–21) | −1.28 | −43.20% | <0.0001 |
| Stigmatization | 13.96 ± 18.18 (0–10) | 8.8 ± 13 (0–6) | −0.46 | −36.90% | 0.092 |
| Social support | 11.39 ± 18.88 (0–8) | 7.41 ± 13.73 (0–6) | −0.38 | −35.20% | 0.143 |
| Cognition | 34.17 ± 26.19 (0–15) | 27.31 ± 22.14 (0–13) | −0.6 | −20.10% | 0.033 |
| Communication | 14.72 ± 16.47 (0–6) | 10.49 ± 15.77 (0–6) | −0.48 | −28.70% | 0.069 |
| Pain and discomfort | 40.56 ± 21.52 (0–10) | 43.21 ± 26.85 (0–12) | 0.2 | 6.50% | 0.583 |
| EUROHIS-QOL8 | 25.1 ± 4.99 (12–38) | 28.19 ± 4.38 (20–36) | 1.35 | 12.30% | <0.0001 |
| Quality of life | 2.93 ± 0.94 (1–4) | 3.48 ± 0.7 (2–4) | 0.9 | 18.70% | 0.004 |
| Health status | 2.3 ± 0.87 (1–4) | 2.78 ± 0.93 (1–4) | 0.71 | 20.80% | 0.02 |
| Energy | 2.73 ± 0.98 (1–5) | 3.33 ± 0.92 (1–5) | 0.96 | 21.90% | 0.002 |
| Autonomy for ADL | 2.8 ± 1.03 (1–5) | 3.3 ± 0.95 (2–5) | 1.01 | 17.80% | 0.002 |
| Self-esteem | 2.87 ± 1.04 (1–5) | 3.37 ± 1 (1–5) | 0.86 | 17.40% | 0.004 |
| Social relationships | 3.7 ± 0.75 (1–5) | 4.04 ± 0.51 (3–5) | 0.61 | 9.10% | 0.025 |
| Economic capacity | 3.57 ± 0.72 (2–5) | 3.59 ± 0.84 (1–5) | 0.24 | 0.50% | 0.356 |
| Habitat | 4.2 ± 0.61 (3–5) | 4.3 ± 0.61 (3–5) | 0.51 | 2.30% | 0.059 |
| ADLS | 82.66 ± 11.72 (50–100) | 84.81 ± 11.22 (50–100) | 0.32 | 2.60% | 0.227 |
| Functional dependency (%) | 23.3 | 14.8 | N.A. | N.A. | 0.687 |
| ∆V12W–VB | HAM-D17 | p |
|---|---|---|
| AS | 0.465 | 0.015 |
| PD-CRS | −0.087 | 0.667 |
| PC-CRS FS sub-score | −0.221 | 0.268 |
| PD-CRS PC sub-score | 0.01 | 0.961 |
| FSS | 0.497 | 0.008 |
| PDQ39 | 0.406 | 0.036 |
| EUROHIS-QOL8 | −0.235 | 0.238 |
| ADLS | 0.103 | 0.609 |
| N | |
|---|---|
| Total AEs, N | 11 |
| Nausea | 5 |
| Dizziness | 2 |
| Vomiting | 1 |
| Headache | 1 |
| Helicobacter pylori infection | 1 |
| COVID-19 disease | 1 |
| Patients with at least one AE, N (%) | 10 (33.3) |
| At least possibly related AEs, N | 8 |
| Definitely related | 2 |
| Probably related | 4 |
| Possibly related | 2 |
| Unrelated | 3 |
| Patients with at least possibly * related to vortioxetine AEs, N (%) | 7 (23.3) |
| Severity, N | |
| Mild | 9 |
| Moderate | 1 |
| Severe | 1 |
| Total SAEs, N | 1 |
| Vomiting | |
| Patients with al least one SAE, N (%) | 1 (3.3) |
| At least possibly * related to vortioxetine SAEs, N | 1 |
| Patients with at least possibly related to vortioxetine SAEs, N (%) | 1 (3.3) |
| Patients with at least one AE leading to discontinuation, N (%) | 1 (3.3) |
| Patients with at least one possibly * related to vortioxetine AE leading to discontinuation N (%) | 1 (3.3) |
| Action taken with the AE, N | |
| Drug withdraw | 1 |
| Dose reduction | 1 |
| None | 9 |
| Deaths, N (%) | 0 (0%) |
| Outcome of the EA, N | |
| Fully recovered | 9 |
| Improvement (not fully recovered) | 1 |
| Unknown | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos García, D.; Alonso Losada, M.G.; Cimas Hernando, I.; Cabo López, I.; Yáñez Baña, R.; Alonso Redondo, R.; Paz González, J.M.; Cores Bartolomé, C.; Feal Painceiras, M.J.; Íñiguez Alvarado, M.C.; et al. Vortioxetine Improves Depressive Symptoms and Cognition in Parkinson’s Disease Patients with Major Depression: An Open-Label Prospective Study. Brain Sci. 2022, 12, 1466. https://doi.org/10.3390/brainsci12111466
Santos García D, Alonso Losada MG, Cimas Hernando I, Cabo López I, Yáñez Baña R, Alonso Redondo R, Paz González JM, Cores Bartolomé C, Feal Painceiras MJ, Íñiguez Alvarado MC, et al. Vortioxetine Improves Depressive Symptoms and Cognition in Parkinson’s Disease Patients with Major Depression: An Open-Label Prospective Study. Brain Sciences. 2022; 12(11):1466. https://doi.org/10.3390/brainsci12111466
Chicago/Turabian StyleSantos García, Diego, Maria Gema Alonso Losada, Icíar Cimas Hernando, Iria Cabo López, Rosa Yáñez Baña, Ruben Alonso Redondo, Jose Manuel Paz González, Carlos Cores Bartolomé, Maria José Feal Painceiras, Maria Cristina Íñiguez Alvarado, and et al. 2022. "Vortioxetine Improves Depressive Symptoms and Cognition in Parkinson’s Disease Patients with Major Depression: An Open-Label Prospective Study" Brain Sciences 12, no. 11: 1466. https://doi.org/10.3390/brainsci12111466
APA StyleSantos García, D., Alonso Losada, M. G., Cimas Hernando, I., Cabo López, I., Yáñez Baña, R., Alonso Redondo, R., Paz González, J. M., Cores Bartolomé, C., Feal Painceiras, M. J., Íñiguez Alvarado, M. C., Labandeira, C., & García Díaz, I. (2022). Vortioxetine Improves Depressive Symptoms and Cognition in Parkinson’s Disease Patients with Major Depression: An Open-Label Prospective Study. Brain Sciences, 12(11), 1466. https://doi.org/10.3390/brainsci12111466