
Efficacy of Onabotulinum Toxin A on Obsessive–Compulsive Traits in a Population of Chronic Migraine Patients


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
Sample Enrolled
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hipolito Rodrigues, M.A.; Maitrot-Mantelet, L.; Plu-Bureau, G.; Gompel, A. Migraine, hormones and the menopausal transition. Climacteric 2018, 21, 256–266. [Google Scholar] [CrossRef] [PubMed]
- Viticchi, G.; Falsetti, L.; Paolucci, M.; Altamura, C.; Buratti, L.; Salvemini, S.; Brunelli, N.; Bartolini, M.; Vernieri, F.; Silvestrini, M. Influence of chronotype on migraine characteristics. Neurol. Sci. 2019, 40, 1841–1848. [Google Scholar] [CrossRef] [PubMed]
- Viticchi, G.; Falsetti, L.; Salvemini, S.; Bartolini, M.; Ranghino, A.; Buratti, L.; Silvestrini, M. Headache changes after kidney transplant. Acta Neurol. Belg. 2022, 122, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Di Cosimo, D.; Innamorati, M.; Lester, D.; Tatarelli, R.; Martelletti, P. Psychiatric comorbidity in patients with chronic daily headache and migraine: A selective overview including personality traits and suicide risk. J. Headache Pain 2009, 10, 283–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buse, D.C.; Silberstein, S.D.; Manack, A.N.; Papapetropoulos, S.; Lipton, R.B. Psychiatric comorbidities of episodic and chronic migraine. J. Neurol. 2013, 260, 1960–1969. [Google Scholar] [CrossRef] [PubMed]
- Antonaci, F.; Nappi, G.; Galli, F.; Manzoni, G.C.; Calabresi, P.; Costa, A. Migraine and psychiatric comorbidity: A review of clinical findings. J. Headache Pain 2011, 12, 115–125. [Google Scholar] [CrossRef] [Green Version]
- Lipton, R.B. Tracing transformation: Chronic migraine classification, progression, and epidemiology. Neurology 2009, 72 (Suppl. S5), S3–S7. [Google Scholar] [CrossRef]
- Cupini, L.M.; De Murtas, M.; Costa, C.; Mancini, M.; Eusebi, P.; Sarchielli, P.; Calabresi, P. Obsessive-compulsive disorder and migraine with medication-overuse headache. Headache 2009, 49, 1005–1013. [Google Scholar] [CrossRef]
- Peterlin, B.L.; Rosso, A.L.; Sheftell, F.D.; Libon, D.J.; Mossey, J.M.; Merikangas, K.R. Post-traumatic stress disorder, drug abuse and migraine: New findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia 2011, 31, 235–244. [Google Scholar] [CrossRef] [Green Version]
- Beghi, E.; Bussone, G.; D’Amico, D.; Cortelli, P.; Cevoli, S.; Manzoni, G.C.; Torelli, P.; Tonini, M.C.; Allais, G.; De Simone, R.; et al. Headache, anxiety and depressive disorders: The HADAS study. J. Headache Pain 2010, 11, 141–150. [Google Scholar] [CrossRef]
- Curone, M.; Tullo, V.; Mea, E.; Proietti-Cecchini, A.; Peccarisi, C.; Bussone, G. Psychopathological profile of patients with chronic migraine and medication overuse: Study and findings in 50 cases. Neurol. Sci. 2011, 32 (Suppl. S1), S177–S179. [Google Scholar] [CrossRef]
- Curone, M.; Tullo, V.; Lovati, C.; Proietti-Cecchini, A.; D’Amico, D. Prevalence and profile of obsessive-compulsive trait in patients with chronic migraine and medication overuse. Neurol. Sci. 2014, 35 (Suppl. S1), 185–187. [Google Scholar] [CrossRef]
- Curone, M.; D’Amico, D.; Bussone, G. Obsessive–compulsive aspects as predictors of poor response to treatments in patients with chronic migraine and medication overuse. Neurol. Sci. 2012, 33 (Suppl. S1), S211–S213. [Google Scholar] [CrossRef]
- Bottiroli, S.; De Icco, R.; Vaghi, G.; Pazzi, S.; Guaschino, E.; Allena, M.; Ghiotto, N.; Martinelli, D.; Tassorelli, C.; Sances, G. Psychological predictors of negative treatment outcome with Erenumab in chronic migraine: Data from an open label long-term prospective study. J. Headache Pain 2021, 22, 114. [Google Scholar] [CrossRef]
- Lorenc, Z.P.; Kenkel, J.M.; Fagien, S.; Hirmand, H.; Nestor, M.S.; Sclafani, A.P.; Sykes, J.M.; Waldorf, H.A. A review of onabotulinumtoxinA (Botox). Aesthet. Surg. J. 2013, 33 (Suppl. S1), 9S–12S. [Google Scholar]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Sica, C.; Ghisi, M.; Altoè, G.; Chiri, L.R.; Franceschini, S.; Coradeschi, D.; Melli, G. The Italian version of Obsessive Compulsive Inventory: Its psychometric properties on community and clinical samples. J. Anxiety Disord. 2009, 23, 204–211. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef]
- Tassorelli, C.; Tedeschi, G.; Sarchielli, P.; Pini, L.A.; Grazzi, L.; Geppetti, P.; De Tommaso, M.; Aguggia, M.; Cortelli, P.; Martelletti, P. Optimizing the long-term management of chronic migraine with onabotulinumtoxinA in real life. Expert Rev. Neurother. 2018, 18, 167–176. [Google Scholar] [CrossRef]
- Altamura, C.; Costa, C.; Fofi, L.; Viticchi, G.; Fallacara, A.; Brunelli, N.; Egeo, G.; Aurilia, C.; Migliore, S.; Barbanti, P.; et al. Migraineurs’ psychological traits do not influence response to erenumab. Neurol. Sci. 2020, 41 (Suppl. S2), 467–468. [Google Scholar] [CrossRef]
- Radat, F.; Lanteri-Minet, M. What is the role of dependence-related behavior in medication-overuse headache? Headache 2010, 50, 1597–1611. [Google Scholar] [CrossRef] [PubMed]
- Rouw, C.; Munksgaard, S.B.; Engelstoft, I.M.S.; Nielsen, M.; Westergaard, M.L.; Jensen, R.H.; Bendtsen, L.; Carlsen, L.N. Dependence-like behaviour in patients treated for medication overuse headache: A prospective open-label randomized controlled trial. Eur. J. Pain 2021, 25, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Radat, F.; Creac’h, C.; Guegan-Massardier, E.; Mick, G.; Guy, N.; Fabre, N.; Giraud, P.; Nachit-Ouinekh, F.; Lanteri-Minet, M. Behavioral dependence in patients with medication overuse headache: A cross-sectional study in consulting patients using the DSM-IV criteria. Headache 2008, 48, 1026–1036. [Google Scholar] [CrossRef] [PubMed]
- Remijnse, P.L.; Nielen, M.M.; van Balkom, A.J.; Cath, D.C.; van Oppen, P.; Uylings, H.B.; Veltman, D.J. Reduced orbitofrontal-striatal activity on a reversal learning task in obsessive-compulsive disorder. Arch. Gen. Psychiatry 2006, 63, 1225–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fumal, A.; Laureys, S.; Di Clemente, L.; Boly, M.; Bohotin, V.; Vandenheede, M. Orbito-frontal cortex involvement in chronic analgesic- overuse headache evolving from episodic migraine. Brain 2006, 129, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.I.; Liu, M.N.; Chen, W.H.; Walsh, V.; Wang, S.J. Clinical and biobehavioral perspectives: Is medication overuse headache a behavior of dependence? Prog. Brain Res. 2020, 255, 371–402. [Google Scholar]
- Moorman, D.E. The role of the orbitofrontal cortex in alcohol use, abuse, and dependence. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 87, 85–107. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.S.; Stark, R.J.; Freeman, M.C.; Orejudos, A.; Manack Adams, A. Long-term study of the efficacy and safety of onabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J. Headache Pain 2018, 19, 13. [Google Scholar] [CrossRef] [Green Version]
- Schulze, J.; Neumann, I.; Magid, M.; Finzi, E.; Sinke, C.; Axel Wollmer, M.; Krüger, T.H.C. Botulinum toxin for the management of depression: An updated review of the evidence and meta-analysis. J. Psychiatr. Res. 2021, 135, 332–340. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Tepper, S.J.; Robbins, L.D.; Manack Adams, A.; Buse, D.C.; Orejudos, A.; Silberstein, S.D. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J. Neurol. Neurosurg. Psychiatry 2019, 90, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, M.T.; McHugh, M.J.; Pariyadath, V.; Stein, E.A. Resting state functional connectivity in addiction: Lessons learned and a road ahead. Neuroimage 2012, 62, 2281–2295. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| T0 | T1 | p | |
|---|---|---|---|
| Age | 50.8 (±11.1) | -- | -- |
| Female Sex, (n, %) | 55 (70.5%) | -- | -- |
| Clinical Improvement, (n, %) | -- | 48 (61.5%) | -- |
| MIDAS Score (±SD) | 77.43 (±52.8) | 41.16 (±39.4) | 0.0001 |
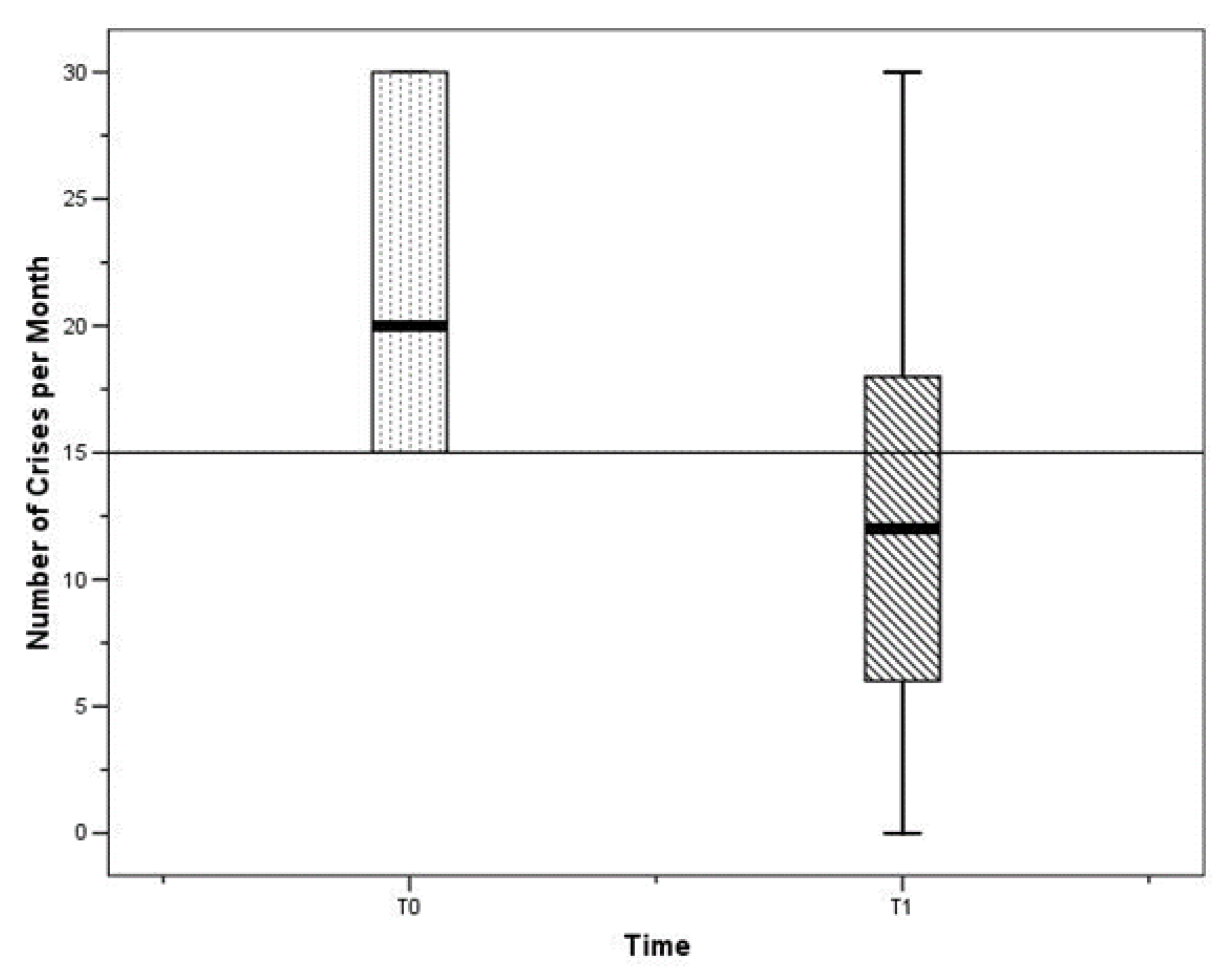
| Crises per Month (±SD) | 21.51 (±6.59) | 12.65 (±8.31) | 0.001 |
| Migraine Type: | |||
|
|
| 0.0001 |
| BS-11 (±SD) | 9.17 (±1.36) | 7.53 (±2.02) | 0.0001 |
| PPI (±SD) | 4.16 (±0.81) | 3.17 (±1.15) | 0.0001 |
| BRS-6 (±SD) | 4.36 (±0.75) | 3.39 (±1.25) | 0.0001 |
| HIT-6 (±SD) | 18.04 (±2.99) | 14.67 (±4.06) | 0.0001 |
| Drug Prophylaxis at T0 (n, %) | |||
|
| -- | -- |
| Drug Treatment of Attacks (n,%) | |||
|
| -- | -- |
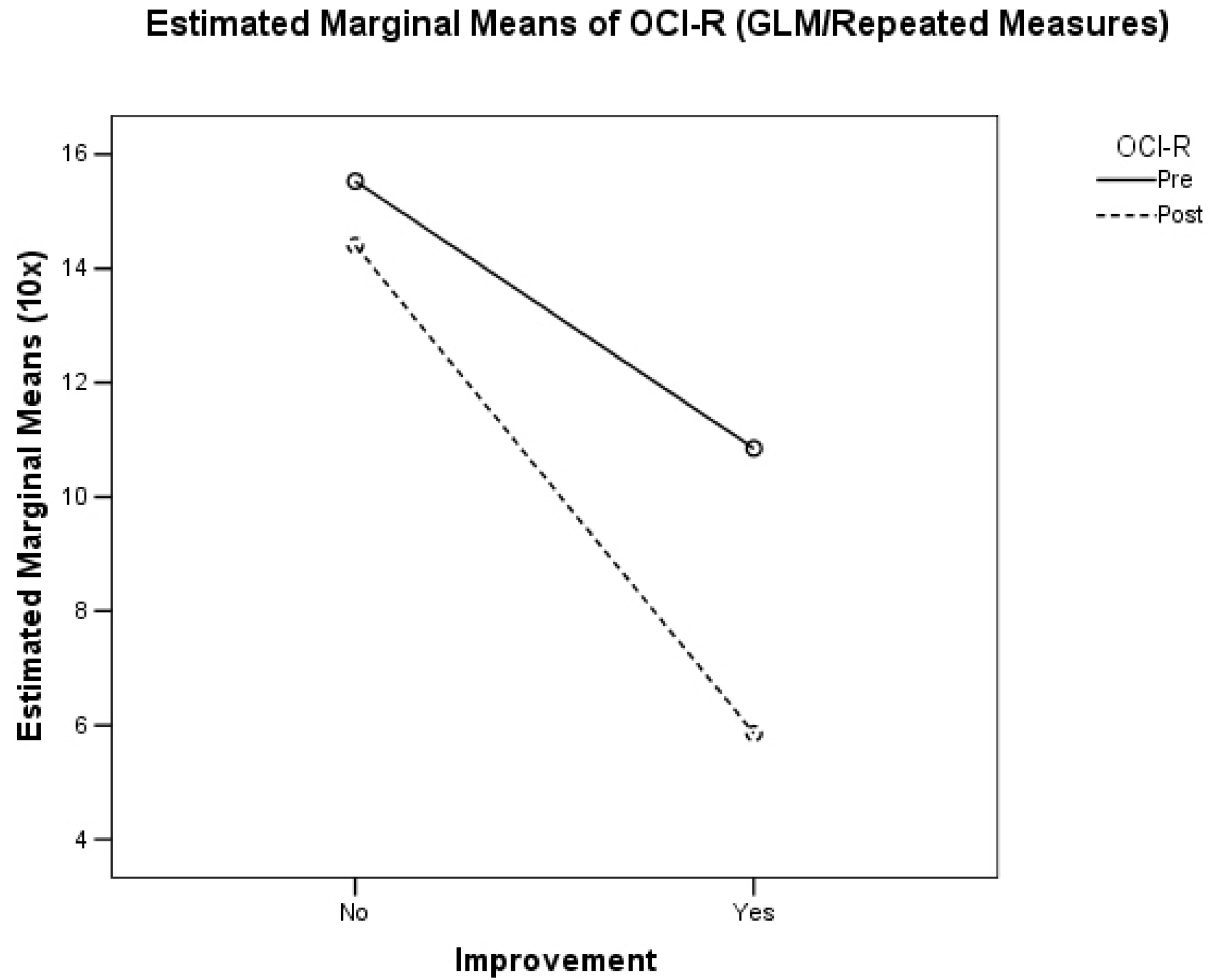
| OCI-R (IQR) | 1 (2) | 0 (2) | 0.0001 |
| OCI-R | |||
|
|
| 0.0001 |
| Responder | Non-Responder | p | |
|---|---|---|---|
| MIDAS Score at T0 (IQR) | 70 (84) | 55 (36) | 0.233 |
| MIDAS Score at T1 (IQR( | 20 (20) | 58 (61) | 0.0001 |
| Number of Crises at T0 (IQR) | 18.5 (15) | 20 (15) | 0.871 |
| Number of Crises at T1 (IQR) | 20 (12) | 0.871 | |
| OCI-R at T0 (IQR) | 2 (3) | 1 (2) | 0.065 |
| OCI-R at T1 (IQR) | 2 (3) | 0 (1) | 0.001 |
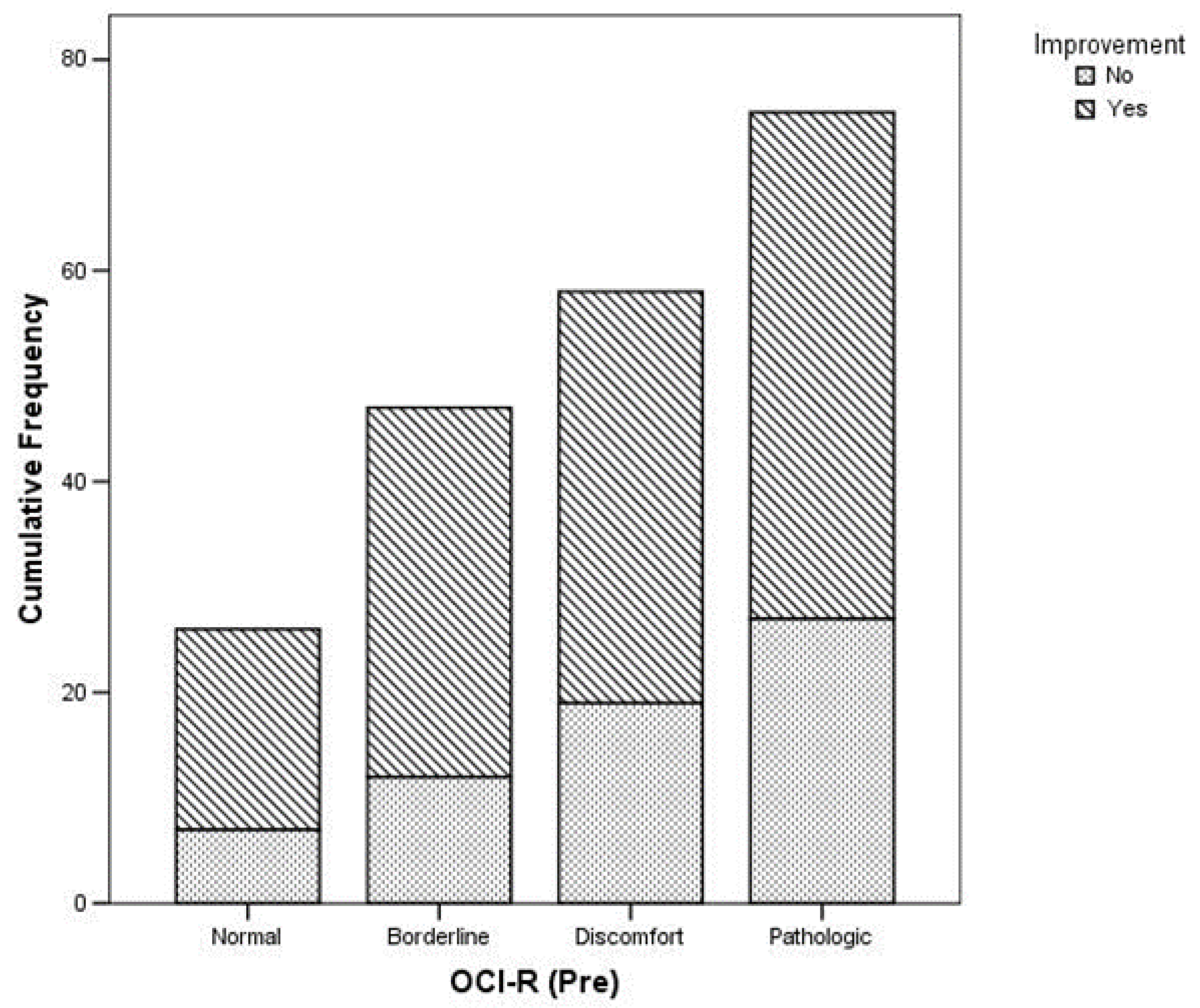
| OCI-R at T0 (n, %) | |||
|
|
| 0.0001 |
| OCI-R at T1 (n, %) | |||
|
|
| 0.002 |
| BS-11 at T0 (±SD) | 9.33 (±0.93) | 8.89 (±1.89) | 0.176 |
| BS-11 at T1 (±SD) | 6.79 (±1.81) | 8.85 (±1.68) | 0.0001 |
| PPI at T0 (±SD) | 4.25 (±0.73) | 4.00 (±0.92) | 0.199 |
| PPI at T1 (±SD) | 2.77 (±1.08) | 3.89 (±0.93) | 0.0001 |
| BRS-6 at T0 (±SD) | 4.42 (±0.71) | 4.26 (±0.81) | 0.385 |
| BRS-6 at T1 (±SD) | 2.90 (±1.19) | 4.26 (±0.81) | 0.0001 |
| HIT-6 at T0 (±SD) | 18.44 (±3.29) | 17.33 (±2.27) | 0.126 |
| HIT-6 at T1 (±SD) | 13.48 (±4.24) | 16.78 (±2.69) | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viticchi, G.; Falsetti, L.; Salvemini, S.; Bartolini, M.; Paolucci, S.; Buratti, L.; Silvestrini, M. Efficacy of Onabotulinum Toxin A on Obsessive–Compulsive Traits in a Population of Chronic Migraine Patients. Brain Sci. 2022, 12, 1563. https://doi.org/10.3390/brainsci12111563
Viticchi G, Falsetti L, Salvemini S, Bartolini M, Paolucci S, Buratti L, Silvestrini M. Efficacy of Onabotulinum Toxin A on Obsessive–Compulsive Traits in a Population of Chronic Migraine Patients. Brain Sciences. 2022; 12(11):1563. https://doi.org/10.3390/brainsci12111563
Chicago/Turabian StyleViticchi, Giovanna, Lorenzo Falsetti, Sergio Salvemini, Marco Bartolini, Silvia Paolucci, Laura Buratti, and Mauro Silvestrini. 2022. "Efficacy of Onabotulinum Toxin A on Obsessive–Compulsive Traits in a Population of Chronic Migraine Patients" Brain Sciences 12, no. 11: 1563. https://doi.org/10.3390/brainsci12111563
APA StyleViticchi, G., Falsetti, L., Salvemini, S., Bartolini, M., Paolucci, S., Buratti, L., & Silvestrini, M. (2022). Efficacy of Onabotulinum Toxin A on Obsessive–Compulsive Traits in a Population of Chronic Migraine Patients. Brain Sciences, 12(11), 1563. https://doi.org/10.3390/brainsci12111563