

The Association between High Mobility Group Box 1 and Stroke-Associated Pneumonia in Acute Ischemic Stroke Patients

Abstract
:1. Introduction
2. Materials and Methods
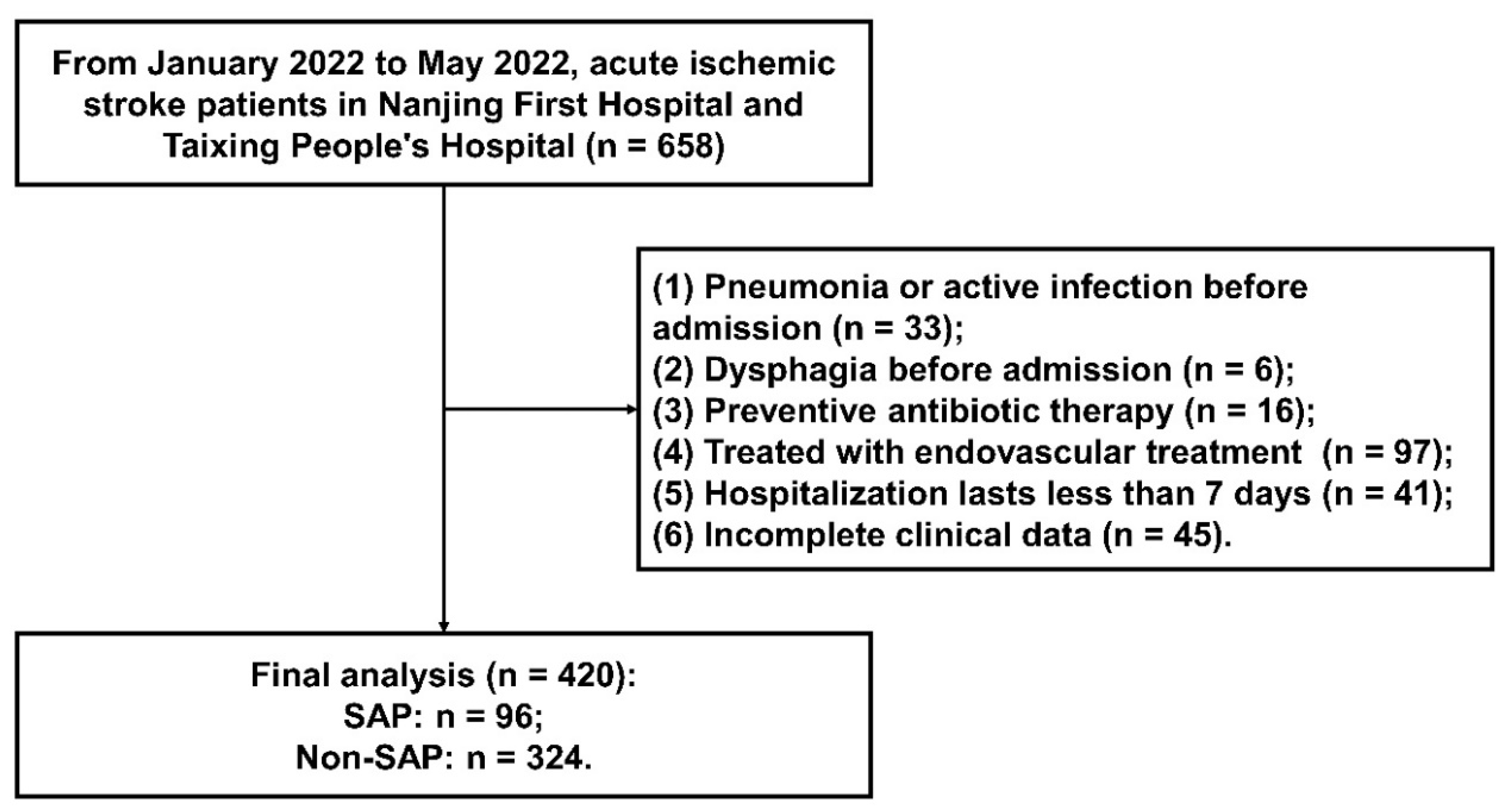
2.1. Study Design and Participants
- (1)
- Admission within 48 h after onset of AIS,
- (2)
- Age 18 years or older.
- (1)
- Pneumonia or active infection before admission;
- (2)
- Dysphagia before admission;
- (3)
- Preventive antibiotic therapy;
- (4)
- Received endovascular treatment;
- (5)
- Hospitalization lasts less than 7 days;
- (6)
- Incomplete clinical data.
2.2. Data Acquisition
2.3. Diagnosis of SAP
2.4. Detection of HMGB1 Concentrations
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, M.; Wang, H.; Zeng, X.; Yin, P.; Zhu, J.; Chen, W.; Li, X.; Wang, L.; Wang, L.; Liu, Y.; et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 394, 1145–1158. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Jiang, B.; Sun, H.; Ru, X.; Sun, D.; Wang, L.; Wang, L.; Jiang, Y.; Li, Y.; Wang, Y.; et al. Prevalence, Incidence, and Mortality of Stroke in China: Results from a Nationwide Population-Based Survey of 480 687 Adults. Circulation 2017, 135, 759–771. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Li, R.; Wang, L.; Yin, P.; Wang, Y.; Yan, C.; Ren, Y.; Qian, Z.; Vaughn, M.G.; McMillin, S.E.; et al. Temporal trend and attributable risk factors of stroke burden in China, 1990–2019: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2021, 6, e897–e906. [Google Scholar] [CrossRef]
- Dai, C.; Yan, D.; Xu, M.; Huang, Q.; Ren, W. Geriatric Nutritional Risk Index is related to the risk of stroke-associated pneumonia. Brain Behav. 2022, 12, e2718. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xu, M.; Huang, Y.; He, J.; Ren, W. Low triiodothyronine syndrome is associated with stroke-associated pneumonia. Eur. J. Clin. Investig. 2022, 52, e13840. [Google Scholar] [CrossRef]
- Huang, L.; Zhang, R.; Ji, J.; Long, F.; Wang, Y.; Lu, J.; Xu, G.; Sun, Y. Hypersensitive C-reactive protein-albumin ratio is associated with stroke-associated pneumonia and early clinical outcomes in patients with acute ischemic stroke. Brain Behav. 2022, 12, e2675. [Google Scholar] [CrossRef]
- Guo, Z.; Hou, J.; Yu, S.; Zhang, H.; Yu, S.; Wang, H.; Xu, J.; You, S.; Huang, Z.; Xiao, G.; et al. Eosinophils, Stroke-Associated Pneumonia, and Outcome After Mechanical Thrombectomy for Acute Ischemic Stroke. Front. Aging Neurosci. 2022, 14, 830858. [Google Scholar] [CrossRef]
- Li, Y.M.; Zhao, L.; Liu, Y.G.; Lu, Y.; Yao, J.Z.; Li, C.J.; Lu, W.; Xu, J.H. Novel Predictors of Stroke-Associated Pneumonia: A Single Center Analysis. Front. Neurol. 2022, 13, 857420. [Google Scholar] [CrossRef]
- Lin, G.; Hu, M.; Song, J.; Xu, X.; Liu, H.; Qiu, L.; Zhu, H.; Xu, M.; Geng, D.; Yang, L.; et al. High Fibrinogen to Albumin Ratio: A Novel Marker for Risk of Stroke-Associated Pneumonia? Front. Neurol. 2022, 12, 747118. [Google Scholar] [CrossRef]
- Cun, Y.; Jin, Y.; Wu, D.; Zhou, L.; Zhang, C.; Zhang, S.; Yang, X.; Wang, U.Z.; Zhang, P. Exosome in Crosstalk between Inflammation and Angiogenesis: A Potential Therapeutic Strategy for Stroke. Mediat. Inflamm. 2022, 2022, 7006281. [Google Scholar] [CrossRef]
- Simats, A.; Liesz, A. Systemic inflammation after stroke: Implications for post-stroke comorbidities. EMBO Mol. Med. 2022, 14, e16269. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, Y.; Cui, M.; Zhang, Y.; Shang, X. Prognostic value of the systemic inflammation response index in patients with acute ischemic stroke. Brain Behav. 2022, 12, e2619. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Ma, X.; Zhao, H.; Fan, J.; Liu, T.; Luo, Y.; Guo, Y. Long non-coding RNA H19 promotes leukocyte inflammation in ischemic stroke by targeting the miR-29b/C1QTNF6 axis. CNS Neurosci. Ther. 2022, 28, 953–963. [Google Scholar] [CrossRef]
- Sun, H.; Li, S.; Xu, Z.; Liu, C.; Gong, P.; Deng, Q.; Yan, F. SNHG15 is a negative regulator of inflammation by mediating TRAF2 ubiquitination in stroke-induced immunosuppression. J. Neuroinflammation 2022, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Tröscher, A.R.; Gruber, J.; Wagner, J.N.; Böhm, V.; Wahl, A.S.; von Oertzen, T.J. Inflammation Mediated Epileptogenesis as Possible Mechanism Underlying Ischemic Post-stroke Epilepsy. Front. Aging Neurosci. 2021, 13, 781174. [Google Scholar] [CrossRef]
- Yang, H.; Wang, H.; Andersson, U. Targeting Inflammation Driven by HMGB1. Front. Immunol. 2020, 11, 484. [Google Scholar] [CrossRef] [Green Version]
- Raucci, A.; Di Maggio, S.; Scavello, F.; D’Ambrosio, A.; Bianchi, M.E.; Capogrossi, M.C. The Janus face of HMGB1 in heart disease: A necessary update. Cell. Mol. Life Sci. 2019, 76, 211–229. [Google Scholar] [CrossRef] [Green Version]
- Lei, C.; Li, Y.; Zhu, X.; Li, H.; Chang, X. HMGB1/TLR4 induces autophagy and promotes neuroinflammation after intracerebral hemorrhage. Brain Res. 2022, 1792, 148003. [Google Scholar] [CrossRef]
- Sørensen, M.V.; Pedersen, S.; Møgelvang, R.; Skov-Jensen, J.; Flyvbjerg, A. Plasma high-mobility group box 1 levels predict mortality after ST-segment elevation myocardial infarction. JACC Cardiovasc. Interv. 2011, 4, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, K.; Iwamoto, H.; Sakamoto, S.; Horimasu, Y.; Masuda, T.; Miyamoto, S.; Nakashima, T.; Ohshimo, S.; Fujitaka, K.; Hamada, H.; et al. Serum high-mobility group box 1 is associated with the onset and severity of acute exacerbation of idiopathic pulmonary fibrosis. Respirology 2020, 25, 275–280. [Google Scholar] [CrossRef]
- Shan, W.; Xu, L.; Qiu, Z.; Wang, J.; Shao, J.; Feng, J.; Zhao, J. Increased high-mobility group box 1 levels are associated with depression after acute ischemic stroke. Neurol. Sci. 2022, 43, 3131–3137. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, G.; Chen, W.; Gong, P.; Wang, M.; Zhou, J.; Wang, X.; Guo, M.; Lu, J.; Li, Y.; Feng, H.; et al. The Relationship Between Serum YKL-40 Levels on Admission and Stroke-Associated Pneumonia in Patients with Acute Ischemic Stroke. J. Inflamm. Res. 2021, 14, 4361–4369. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.J.; Kishore, A.K.; Vail, A.; Chamorro, A.; Garau, J.; Hopkins, S.J.; Di Napoli, M.; Kalra, L.; Langhorne, P.; Montaner, J.; et al. Diagnosis of Stroke-Associated Pneumonia: Recommendations from the Pneumonia in Stroke Consensus Group. Stroke 2015, 46, 2335–2340. [Google Scholar] [CrossRef] [PubMed]
- Kang, R.; Chen, R.; Zhang, Q.; Hou, W.; Wu, S.; Cao, L.; Huang, J.; Yu, Y.; Fan, X.-G.; Yan, Z.; et al. HMGB1 in health and disease. Mol. Asp. Med. 2014, 40, 1–116. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Takahashi, H.K.; Liu, K.; Wake, H.; Liu, R.; Maruo, T.; Date, I.; Yoshino, T.; Ohtsuka, A.; Mori, S.; et al. Anti-high mobility group box-1 monoclonal antibody protects the blood-brain barrier from ischemia-induced disruption in rats. Stroke 2011, 42, 1420–1428. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Karki, R.; Igwe, O.J. Toll-like receptor 4 signaling: A common pathway for interactions between prooxidants and extracellular disulfide high mobility group box 1 (HMGB1) protein-coupled activation. Biochem. Pharmacol. 2015, 98, 132–143. [Google Scholar] [CrossRef] [Green Version]
- Ye, Y.; Zeng, Z.; Jin, T.; Zhang, H.; Xiong, X.; Gu, L. The Role of High Mobility Group Box 1 in Ischemic Stroke. Front. Cell. Neurosci. 2019, 13, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishibori, M.; Wang, D.; Ousaka, D.; Wake, H. High Mobility Group Box-1 and Blood-Brain Barrier Disruption. Cells 2020, 9, 2650. [Google Scholar] [CrossRef]
- Huang, J.; Zeng, T.; Tian, Y.; Wu, Y.; Yu, J.; Pei, Z.; Tan, L. Clinical significance of high-mobility group box-1 (HMGB1) in subjects with type 2 diabetes mellitus (T2DM) combined with chronic obstructive pulmonary disease (COPD). J. Clin. Lab. Anal. 2019, 33, e22910. [Google Scholar] [CrossRef]
- Biscetti, F.; Tinelli, G.; Rando, M.M.; Nardella, E.; Cecchini, A.L.; Angelini, F.; Straface, G.; Filipponi, M.; Arena, V.; Pitocco, D.; et al. Association between carotid plaque vulnerability and high mobility group box-1 serum levels in a diabetic population. Cardiovasc. Diabetol. 2021, 20, 114. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jiang, Y.; Zeng, D.; Zhou, W.; Hong, X. Prognostic value of plasma HMGB1 in ischemic stroke patients with cerebral ischemia-reperfusion injury after intravenous thrombolysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 105055. [Google Scholar] [CrossRef] [PubMed]
- Le, K.; Mo, S.; Lu, X.; Idriss Ali, A.; Yu, D.; Guo, Y. Association of circulating blood HMGB1 levels with ischemic stroke: A systematic review and meta-analysis. Neurol. Res. 2018, 40, 907–916. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-SAP (n = 324) | SAP (n = 96) | p |
|---|---|---|---|
| Demographics | |||
| Age, years | 65.7 ± 11.9 | 72.8 ± 12.2 | <0.001 |
| Male, n (%) | 222 (68.5) | 64 (66.7) | 0.732 |
| Lower literacy level (primary school or lower), n (%) | 107 (33.0) | 35 (36.5) | 0.532 |
| Vascular risk factors, n (%) | |||
| Hypertension | 217 (67.0) | 68 (70.8) | 0.477 |
| Diabetes mellitus | 98 (30.2) | 33 (34.4) | 0.443 |
| Atrial fibrillation | 33 (10.2) | 25 (26.0) | <0.001 |
| Coronary heart disease | 33 (10.2) | 17 (17.7) | 0.046 |
| Previous stroke | 54 (16.7) | 27 (28.1) | 0.012 |
| Clinical characteristics | |||
| NIHSS at admission | 3 (2, 4) | 9 (5, 16) | <0.001 |
| Dysphagia at admission, n (%) | 21 (6.5) | 51 (53.1) | <0.001 |
| SBP, mmHg | 143.7 ± 19.7 | 144.5 ± 24.0 | 0.720 |
| DBP, mmHg | 85.9 ± 12.6 | 85.4 ± 13.1 | 0.769 |
| Ventilator during hospitalization, n (%) | 1 (0.3) | 13 (13.5) | <0.001 |
| BMI, kg/m2 | 24.8 ± 3.3 | 23.9 ± 4.1 | 0.045 |
| Pulse, /min | 78 (70, 80) | 78 (69, 89) | 0.223 |
| Intravenous thrombolysis, n (%) | 78 (24.1) | 31 (32.3) | 0.107 |
| TOAST subtype, n (%) | 0.013 | ||
| LAA | 146 (45.1) | 42 (43.8) | |
| CE | 43 (13.3) | 27 (28.1) | |
| SAO | 113 (34.9) | 22 (22.9) | |
| SOE | 12 (3.7) | 3 (3.1) | |
| SUE | 10 (3.1) | 2 (2.1) | |
| Laboratory data | |||
| WBC, 10^9/L | 7.29 (5.95, 8.93) | 9.92 (7.04, 12.91) | <0.001 |
| FBG, mmol/L | 5.42 (4.77, 6.63) | 6.25 (5.22, 7.80) | <0.001 |
| TC, mmol/L | 4.43 ± 1.14 | 4.41 ± 1.17 | 0.834 |
| TG, mmol/L | 1.34 (0.98,1.78) | 1.25 (0.80, 1.70) | 0.122 |
| HDL, mmol/L | 1.05 (0.90, 1.29) | 1.16 (0.86, 1.49) | 0.115 |
| LDL, mmol/L | 2.56 (1.93, 3.24) | 2.49 (1.90, 3.16) | 0.573 |
| Uric acid, ng/mL | 307.5 (252.0, 369.8) | 314.5 (254.0, 397.8) | 0.263 |
| HMGB1 as a Categorical Variable | HMGB1 as a Continuous Variable | ||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||
| Case, n (%) | 14 (13.3) | 18 (17.1) | 26 (24.8) | 38 (36.2) | 96 (22.9) |
| Unadjusted model | 1.00 (reference) | 1.345 (0.630–2.869) | 2.139 (1.045–4.378) | 3.687 (1.851–7.344) | 1.132 (1.069–1.199) |
| Age- and sex-adjusted | 1.00 (reference) | 1.344 (0.618–2.924) | 2.025 (0.967–4.241) | 3.511 (1.725–7.147) | 1.131 (1.066–1.200) |
| Multivariable-adjusted * | 1.00 (reference) | 1.139 (0.409–3.169) | 1.019 (0.360–2.886) | 2.701 (1.045–6.981) | 1.096 (1.011–1.188) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
E, Y.; Deng, Q.; Shi, G.; Li, Z.; Liu, C.; Wang, S.; Lian, H.; Cao, H.; Zhang, X.; Zhang, Y.; et al. The Association between High Mobility Group Box 1 and Stroke-Associated Pneumonia in Acute Ischemic Stroke Patients. Brain Sci. 2022, 12, 1580. https://doi.org/10.3390/brainsci12111580
E Y, Deng Q, Shi G, Li Z, Liu C, Wang S, Lian H, Cao H, Zhang X, Zhang Y, et al. The Association between High Mobility Group Box 1 and Stroke-Associated Pneumonia in Acute Ischemic Stroke Patients. Brain Sciences. 2022; 12(11):1580. https://doi.org/10.3390/brainsci12111580
Chicago/Turabian StyleE, Yan, Qiwen Deng, Guomei Shi, Zhongyuan Li, Chengfang Liu, Siyu Wang, Huiwen Lian, Haiming Cao, Xiaohao Zhang, Yingdong Zhang, and et al. 2022. "The Association between High Mobility Group Box 1 and Stroke-Associated Pneumonia in Acute Ischemic Stroke Patients" Brain Sciences 12, no. 11: 1580. https://doi.org/10.3390/brainsci12111580
APA StyleE, Y., Deng, Q., Shi, G., Li, Z., Liu, C., Wang, S., Lian, H., Cao, H., Zhang, X., Zhang, Y., Gong, P., & Jiang, T. (2022). The Association between High Mobility Group Box 1 and Stroke-Associated Pneumonia in Acute Ischemic Stroke Patients. Brain Sciences, 12(11), 1580. https://doi.org/10.3390/brainsci12111580