
Gender Differences in the Correlations between Childhood Trauma, Schizotypy and Negative Emotions in Non-Clinical Individuals



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Self-Report Measures
2.3. Statistical Analysis
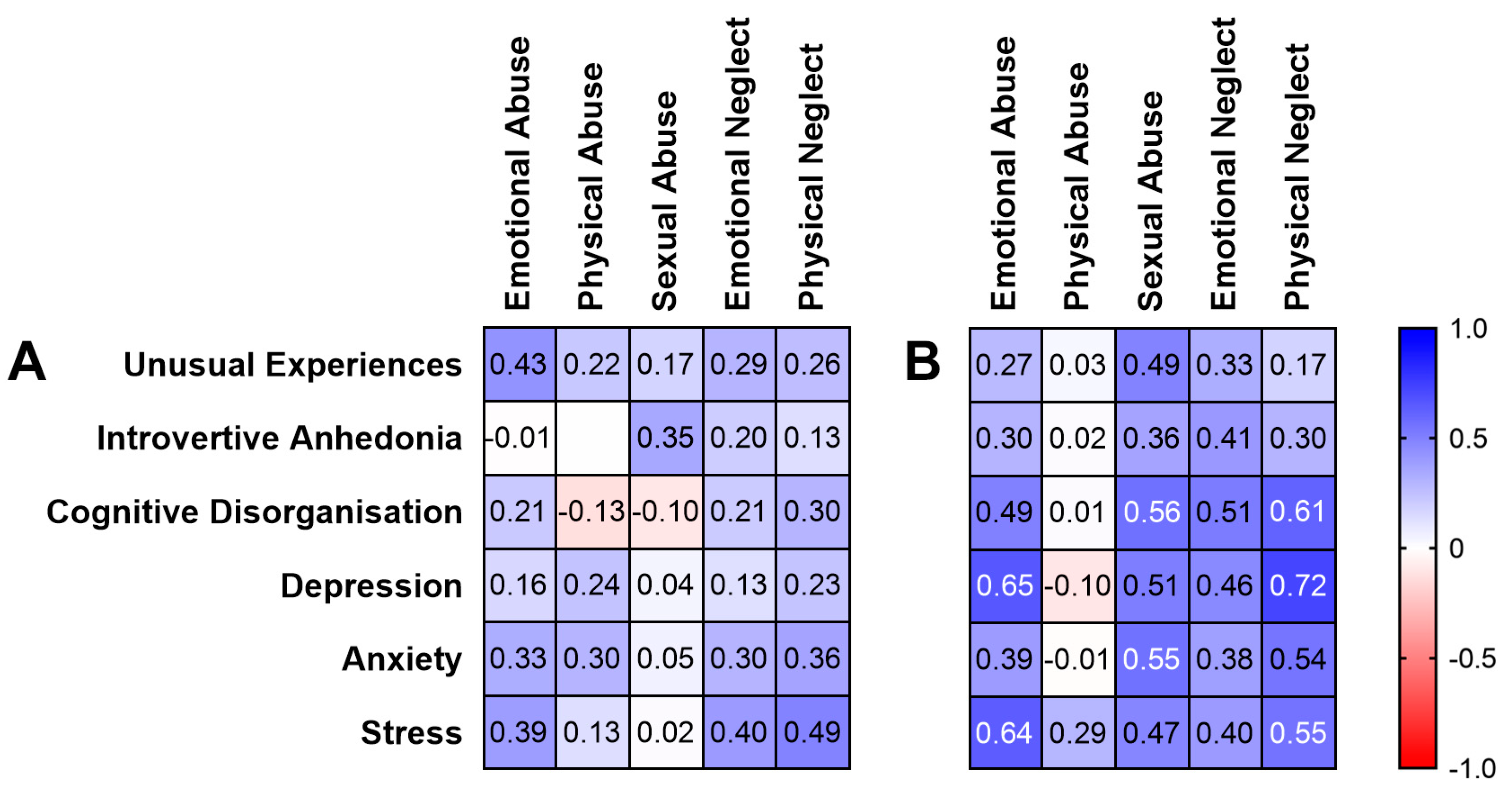
3. Results
4. Discussion
4.1. Childhood Trauma and Disorganised Schizotypy
4.2. Childhood Trauma and Negative Emotions
4.3. Gender Differences in the HPA Axis as an Underlying Mechanism
4.4. Limitations, Future Research and Clinical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, R.; Ma, X.; Wang, G.; Yang, J.; Wang, C. Why sex differences in schizophrenia? J. Transl. Neurosci. 2016, 1, 37. [Google Scholar]
- Riecher-Rössler, A.; Butler, S.; Kulkarni, J. Sex and gender differences in schizophrenic psychoses—a critical review. Arch. Women’s Ment. Health 2018, 21, 627–648. [Google Scholar] [CrossRef] [PubMed]
- Vila-Badia, R.; Butjosa, A.; Del Cacho, N.; Serra-Arumí, C.; Esteban-Sanjusto, M.; Ochoa, S.; Usall, J. Types, prevalence and gender differences of childhood trauma in first-episode psychosis. What is the evidence that childhood trauma is related to symptoms and functional outcomes in first episode psychosis? A systematic review. Schizophr. Res. 2021, 228, 159–179. [Google Scholar] [CrossRef] [PubMed]
- De Bellis, M.D.; Zisk, A. The biological effects of childhood trauma. Child Adolesc. Psychiatr. Clin. 2014, 23, 185–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruessner, M.; Cullen, A.E.; Aas, M.; Walker, E.F. The neural diathesis-stress model of schizophrenia revisited: An update on recent findings considering illness stage and neurobiological and methodological complexities. Neurosci. Biobehav. Rev. 2017, 73, 191–218. [Google Scholar] [CrossRef] [Green Version]
- Weiss, E.L.; Longhurst, J.G.; Mazure, C.M. Childhood sexual abuse as a risk factor for depression in women: Psychosocial and neurobiological correlates. Am. J. Psychiatry 1999, 156, 816–828. [Google Scholar] [CrossRef]
- Sweeney, S.; Air, T.; Zannettino, L.; Shah, S.S.; Galletly, C. Gender differences in the physical and psychological manifestation of childhood trauma and/or adversity in people with psychosis. Front. Psychol. 2015, 6, 1768. [Google Scholar] [CrossRef]
- Pruessner, M.; King, S.; Vracotas, N.; Abadi, S.; Iyer, S.; Malla, A.K.; Shah, J.; Joober, R. Gender differences in childhood trauma in first episode psychosis: Association with symptom severity over two years. Schizophr. Res. 2019, 205, 30–37. [Google Scholar] [CrossRef]
- Garcia, M.; Montalvo, I.; Creus, M.; Cabezas, Á.; Solé, M.; Algora, M.J.; Moreno, I.; Gutiérrez-Zotes, A.; Labad, J. Sex differences in the effect of childhood trauma on the clinical expression of early psychosis. Compr. Psychiatry 2016, 68, 86–96. [Google Scholar] [CrossRef]
- Kudielka, B.M.; Kirschbaum, C. Sex differences in HPA axis responses to stress: A review. Biol. Psychol. 2005, 69, 113–132. [Google Scholar] [CrossRef]
- Køster, A.; Lajer, M.; Lindhardt, A.; Rosenbaum, B. Gender differences in first episode psychosis. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 940–946. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, S.; Usall, J.; Cobo, J.; Labad, X.; Kulkarni, J. Gender differences in schizophrenia and first-episode psychosis: A comprehensive literature review. Schizophr. Res. Treat. 2012, 2012, 916198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.H.; Rossell, S.L.; Tan, E.J.; Neill, E.; Van Rheenen, T.E.; Carruthers, S.P.; Sumner, P.J.; Louise, S.; Bozaoglu, K.; Gurvich, C. Do schizotypy dimensions reflect the symptoms of schizophrenia? Aust. N. Z. J. Psychiatry 2019, 53, 236–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velikonja, T.; Fisher, H.; Mason, O.; Johnson, S. Childhood trauma and schizotypy: A systematic literature review. Psychol. Med. 2015, 45, 947–963. [Google Scholar] [CrossRef]
- Berenbaum, H.; Thompson, R.J.; Milanak, M.E.; Boden, M.T.; Bredemeier, K. Psychological trauma and schizotypal personality disorder. J. Abnorm. Psychol. 2008, 117, 502. [Google Scholar] [CrossRef] [Green Version]
- Toutountzidis, D.; Gale, T.M.; Irvine, K.; Sharma, S.; Laws, K.R. Sex differences in the association between childhood adversities and schizotypal personality traits. Psychiatry Res. 2018, 269, 31–37. [Google Scholar] [CrossRef]
- Lobbestael, J.; Arntz, A.; Bernstein, D.P. Disentangling the relationship between different types of childhood maltreatment and personality disorders. J. Personal. Disord. 2010, 24, 285–295. [Google Scholar] [CrossRef]
- Powers, A.D.; Thomas, K.M.; Ressler, K.J.; Bradley, B. The differential effects of child abuse and posttraumatic stress disorder on schizotypal personality disorder. Compr. Psychiatry 2011, 52, 438–445. [Google Scholar] [CrossRef]
- Mason, O.; Claridge, G.; Jackson, M. New scales for the assessment of schizotypy. Pers. Individ. Dif. 1995, 18, 7–13. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Pennebaker, J.W.; Susman, J.R. Disclosure of traumas and psychosomatic processes. Soc. Sci. Med. 1988, 26, 327–332. [Google Scholar] [CrossRef]
- Fonseca-Pedrero, E.; Ortuño-Sierra, J.; Sierro, G.; Daniel, C.; Cella, M.; Preti, A.; Mohr, C.; Mason, O.J. The measurement invariance of schizotypy in Europe. Eur. Psychiatry 2015, 30, 837–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, R.; Summers, M.; Summers, A.; Wolf, A.; Summers, J.J. Depression Anxiety Stress Scales-21: Factor structure and test-retest invariance, and temporal stability and uniqueness of latent factors in older adults. J. Psychopathol. Behav. Assess. 2014, 36, 308–317. [Google Scholar] [CrossRef]
- He, J.; Zhong, X.; Gao, Y.; Xiong, G.; Yao, S. Psychometric properties of the Chinese version of the Childhood Trauma Questionnaire-Short Form (CTQ-SF) among undergraduates and depressive patients. Child Abus. Negl. 2019, 91, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Salmond, C.H.; Meiser-Stedman, R.; Glucksman, E.; Thompson, P.; Dalgleish, T.; Smith, P. The nature of trauma memories in acute stress disorder in children and adolescents. J. Child Psychol. Psychiatry 2011, 52, 560–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, F.; Clarke, J.; Heim, C.; Harvey, P.D.; Majer, M.; Nemeroff, C.B. The effects of child abuse and neglect on cognitive functioning in adulthood. J. Psychiatr. Res. 2012, 46, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Gil, A.; Gama, C.S.; de Jesus, D.R.; Lobato, M.I.; Zimmer, M.; Belmonte-de-Abreu, P. The association of child abuse and neglect with adult disability in schizophrenia and the prominent role of physical neglect. Child Abus. Negl. 2009, 33, 618–624. [Google Scholar] [CrossRef]
- Kelly, M.M.; Tyrka, A.R.; Price, L.H.; Carpenter, L.L. Sex differences in the use of coping strategies: Predictors of anxiety and depressive symptoms. Depress. Anxiety 2008, 25, 839–846. [Google Scholar] [CrossRef] [Green Version]
- Huh, H.J.; Kim, K.H.; Lee, H.-K.; Chae, J.-H. The relationship between childhood trauma and the severity of adulthood depression and anxiety symptoms in a clinical sample: The mediating role of cognitive emotion regulation strategies. J. Affect. Disord. 2017, 213, 44–50. [Google Scholar] [CrossRef]
- Whatley, S.L.; Foreman, A.C.; Richards, S. The relationship of coping style to dysphoria, anxiety, and anger. Psychol. Rep. 1998, 83, 783–791. [Google Scholar] [CrossRef]
- Matud, M.P. Gender differences in stress and coping styles. Pers. Individ. Dif. 2004, 37, 1401–1415. [Google Scholar] [CrossRef]
- Sigurdardottir, S.; Halldorsdottir, S.; Bender, S.S. Consequences of childhood sexual abuse for health and well-being: Gender similarities and differences. Scand. J. Public Health 2014, 42, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Hinkelmann, K.; Moritz, S.; Botzenhardt, J.; Riedesel, K.; Wiedemann, K.; Kellner, M.; Otte, C. Cognitive impairment in major depression: Association with salivary cortisol. Biol. Psychiatry 2009, 66, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Walder, D.J.; Walker, E.F.; Lewine, R.J. Cognitive functioning, cortisol release, and symptom severity in patients with schizophrenia. Biol. Psychiatry 2000, 48, 1121–1132. [Google Scholar] [CrossRef]
- Cherian, K.; Schatzberg, A.F.; Keller, J. HPA axis in psychotic major depression and schizophrenia spectrum disorders: Cortisol, clinical symptomatology, and cognition. Schizophr. Res. 2019, 213, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Gomez, R.G.; Fleming, S.H.; Keller, J.; Flores, B.; Kenna, H.; DeBattista, C.; Solvason, B.; Schatzberg, A.F. The neuropsychological profile of psychotic major depression and its relation to cortisol. Biol. Psychiatry 2006, 60, 472–478. [Google Scholar] [CrossRef]
- Powers, S.I.; Laurent, H.K.; Gunlicks-Stoessel, M.; Balaban, S.; Bent, E. Depression and anxiety predict sex-specific cortisol responses to interpersonal stress. Psychoneuroendocrinology 2016, 69, 172–179. [Google Scholar] [CrossRef]
- Gobinath, A.R.; Mahmoud, R.; Galea, L.A. Influence of sex and stress exposure across the lifespan on endophenotypes of depression: Focus on behavior, glucocorticoids, and hippocampus. Front. Neurosci. 2015, 8, 420. [Google Scholar] [CrossRef]
- Goodwill, H.L.; Manzano-Nieves, G.; Gallo, M.; Lee, H.-I.; Oyerinde, E.; Serre, T.; Bath, K.G. Early life stress leads to sex differences in development of depressive-like outcomes in a mouse model. Neuropsychopharmacology 2019, 44, 711–720. [Google Scholar] [CrossRef]
- Read, J.; Perry, B.D.; Moskowitz, A.; Connolly, J. The contribution of early traumatic events to schizophrenia in some patients: A traumagenic neurodevelopmental model. Psychiatry Interpers. Biol. Process. 2001, 64, 319–345. [Google Scholar] [CrossRef] [Green Version]
- Young, E.A.; Haskett, R.F.; Murphy-Weinberg, V.; Watson, S.J.; Akil, H. Loss of glucocorticoid fast feedback in depression. Arch. Gen. Psychiatry 1991, 48, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Boiko, A.S.; Mednova, I.A.; Kornetova, E.G.; Bokhan, N.A.; Semke, A.V.; Loonen, A.J.; Ivanova, S.A. Cortisol and DHEAS related to metabolic syndrome in patients with schizophrenia. Neuropsychiatr. Dis. Treat. 2020, 16, 1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Men | Women | Test Statistic | ||||
|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | Mean (SD) | Median (IQR) | U | p | |
| Age | 24.76 (4.35) | 23.00 (6.00) | 23.18 (4.04) | 22.50 (4.00) | 375.50 | 0.21 |
| CTQ measures | ||||||
| Emotional Abuse | 6.24 (1.82) | 5.00 (2.00) | 8.11 (3.63) | 7.00 (4.00) | 315.00 | 0.03 |
| Physical Abuse | 5.55 (1.03) | 5.00 (1.00) | 6.18 (2.29) | 5.00 (1.75) | 425.00 | 0.51 |
| Sexual Abuse | 5.45 (1.50) | 5.00 (0.00) | 5.96 (2.01) | 5.00 (1.00) | 398.50 | 0.20 |
| Emotional Neglect | 8.27 (3.30) | 7.00 (4.00) | 8.81 (3.86) | 8.00 (6.00) | 417.00 | 0.67 |
| Physical Neglect | 6.41 (2.11) | 5.00 (2.00) | 6.32 (1.63) | 5.00 (2.75) | 437.00 | 0.86 |
| Schizotypy measures | ||||||
| Unusual Experiences | 6.55 (6.29) | 5.00 (8.50) | 8.71 (6.43) | 7.50 (11.50) | 363.50 | 0.15 |
| Introvertive Anhedonia | 6.67 (5.01) | 6.00 (6.00) | 5.96 (4.09) | 5.50 (6.75) | 439.50 | 0.74 |
| Cognitive Disorganisation | 7.69 (5.47) | 7.00 (7.50) | 12.04 (5.76) | 14.00 (10.00) | 258.00 | 0.005 * |
| Negative emotion measures | ||||||
| Depression | 2.85 (4.40) | 1.00 (3.00) | 2.39 (2.38) | 2.00 (2.75) | 431.00 | 0.65 |
| Anxiety | 2.91 (3.19) | 2.00 (3.00) | 3.36 (3.46) | 2.50 (4.75) | 429.50 | 0.63 |
| Stress | 3.88 (3.69) | 3.00 (3.50) | 4.43 (3.39) | 4.00 (5.75) | 404.50 | 0.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, E.H.X.; Rossell, S.L.; Gurvich, C. Gender Differences in the Correlations between Childhood Trauma, Schizotypy and Negative Emotions in Non-Clinical Individuals. Brain Sci. 2022, 12, 186. https://doi.org/10.3390/brainsci12020186
Thomas EHX, Rossell SL, Gurvich C. Gender Differences in the Correlations between Childhood Trauma, Schizotypy and Negative Emotions in Non-Clinical Individuals. Brain Sciences. 2022; 12(2):186. https://doi.org/10.3390/brainsci12020186
Chicago/Turabian StyleThomas, Elizabeth H. X., Susan L. Rossell, and Caroline Gurvich. 2022. "Gender Differences in the Correlations between Childhood Trauma, Schizotypy and Negative Emotions in Non-Clinical Individuals" Brain Sciences 12, no. 2: 186. https://doi.org/10.3390/brainsci12020186
APA StyleThomas, E. H. X., Rossell, S. L., & Gurvich, C. (2022). Gender Differences in the Correlations between Childhood Trauma, Schizotypy and Negative Emotions in Non-Clinical Individuals. Brain Sciences, 12(2), 186. https://doi.org/10.3390/brainsci12020186