
Comparison of Immune Checkpoint Molecules PD-1 and PD-L1 in Paired Primary and Recurrent Glioma: Increasing Trend When Recurrence


Abstract
:1. Introduction
2. Materials and Methods
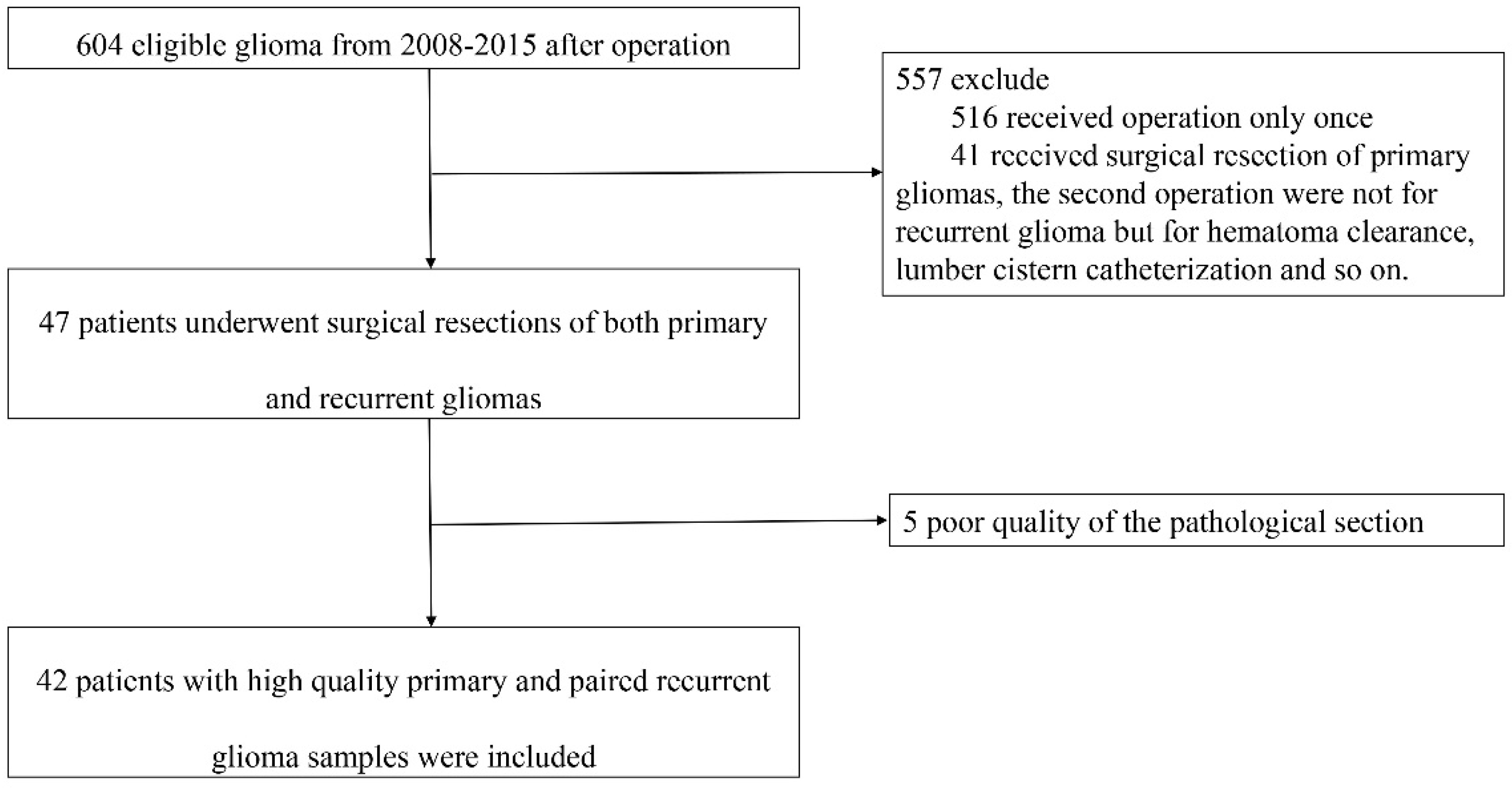
2.1. Patients
2.2. Immunohistochemistry
2.3. Scoring System
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics and Follow-Up
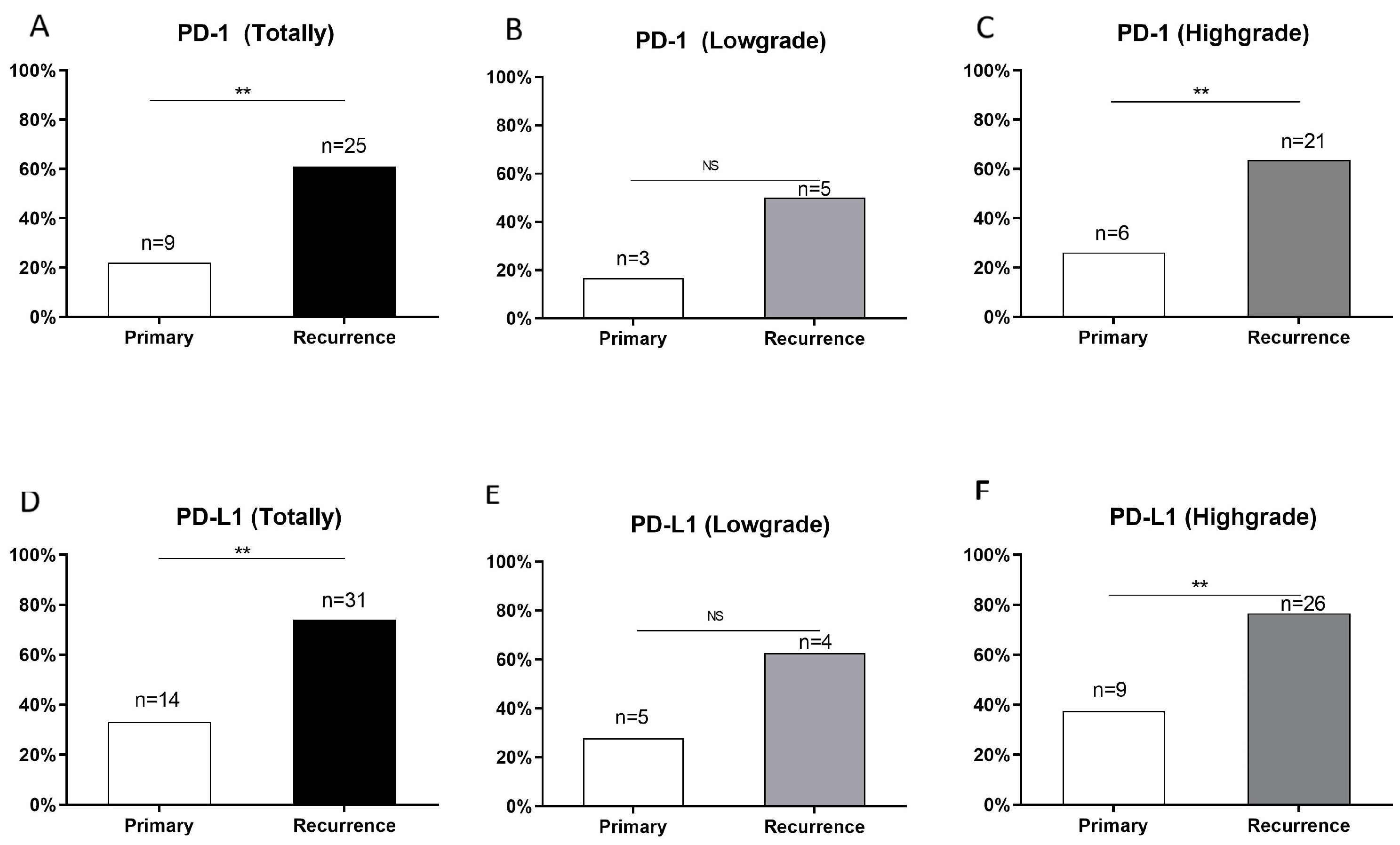
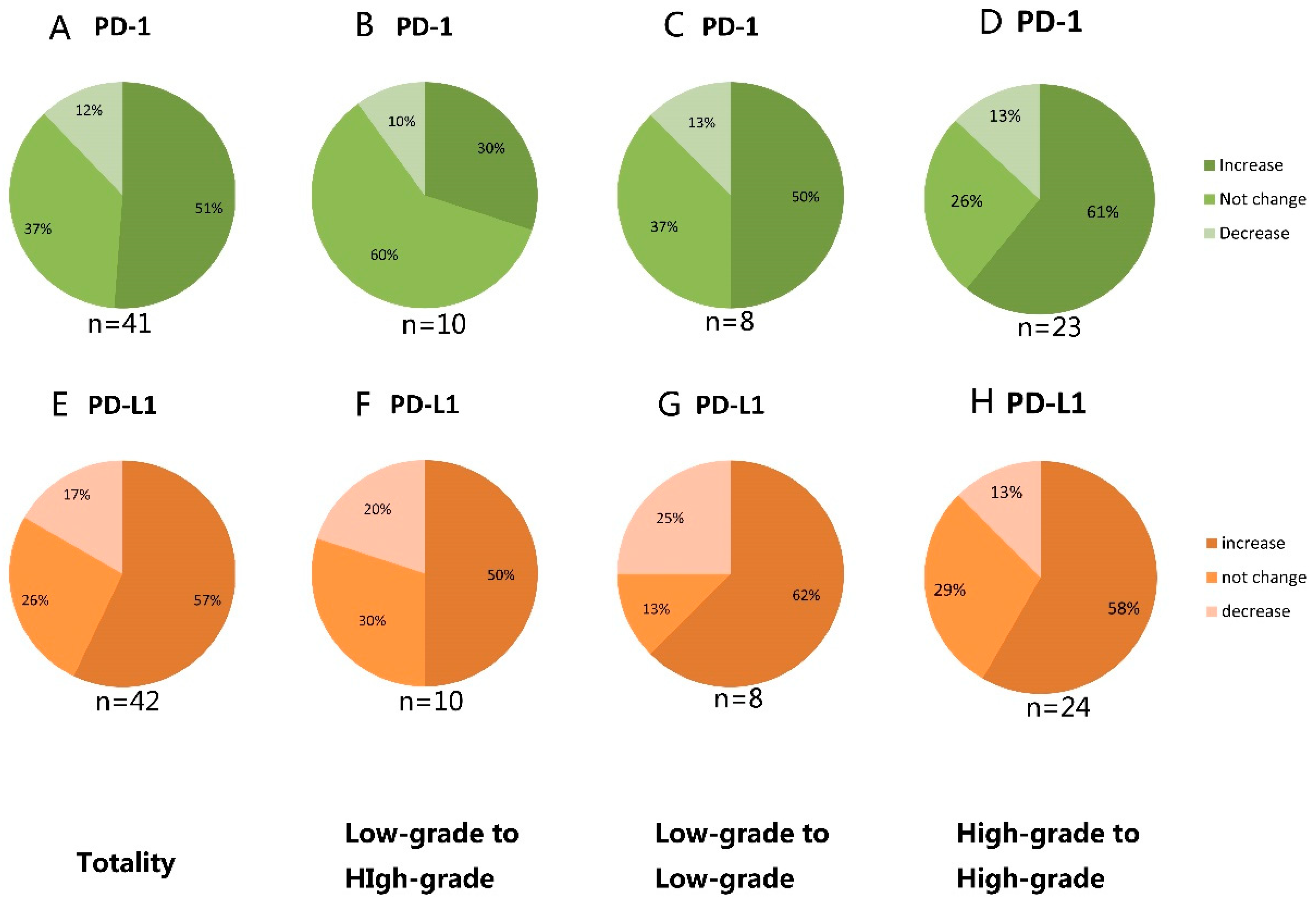
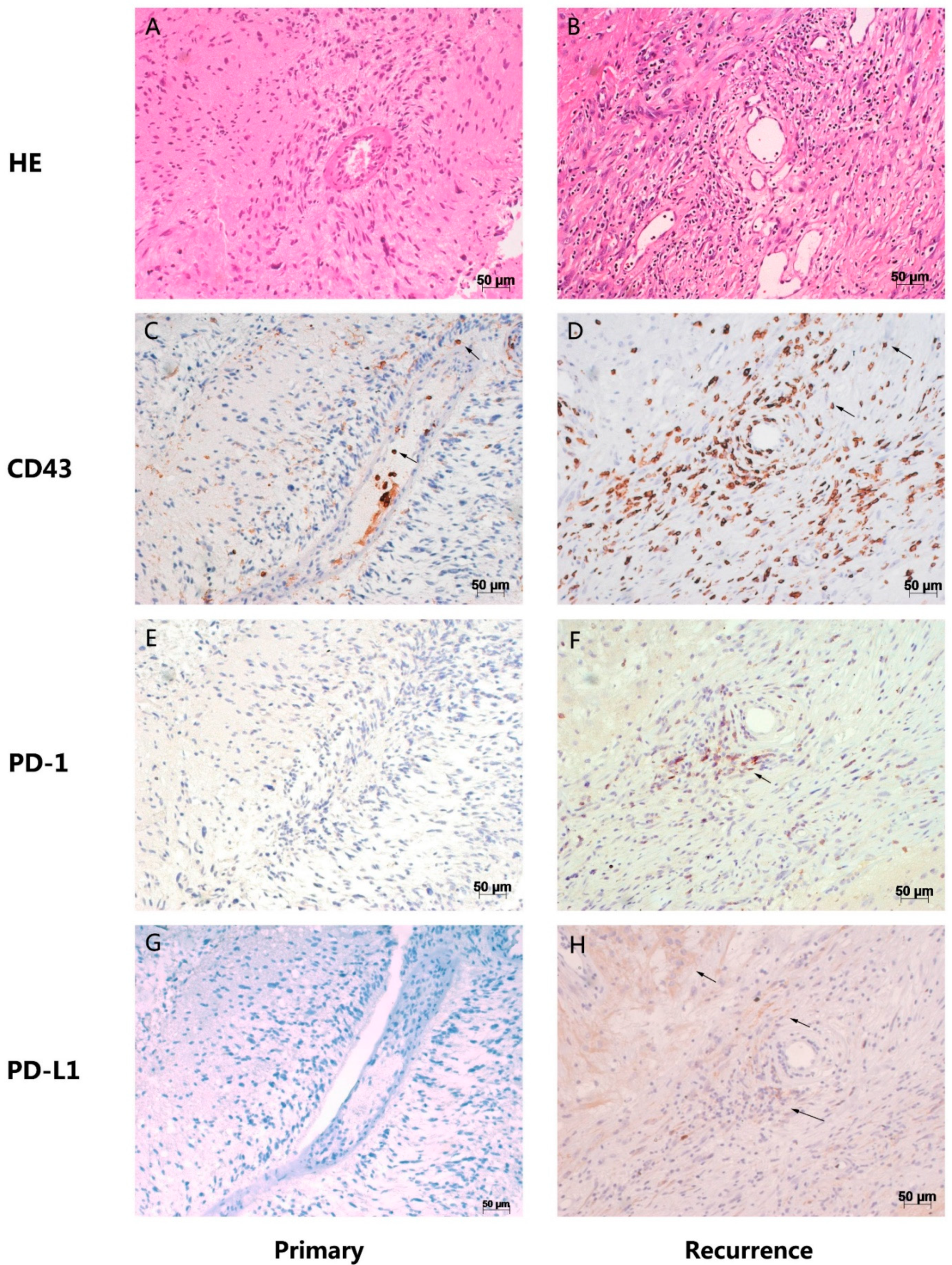
3.2. Increased Protein Expression of PD-1 and PD-L1 in Recurrent Gliomas Compared to Their Corresponding Primary Tumors
3.3. Effect of Postoperative Adjuvant Therapy on the Expression of PD-1, PD-L1
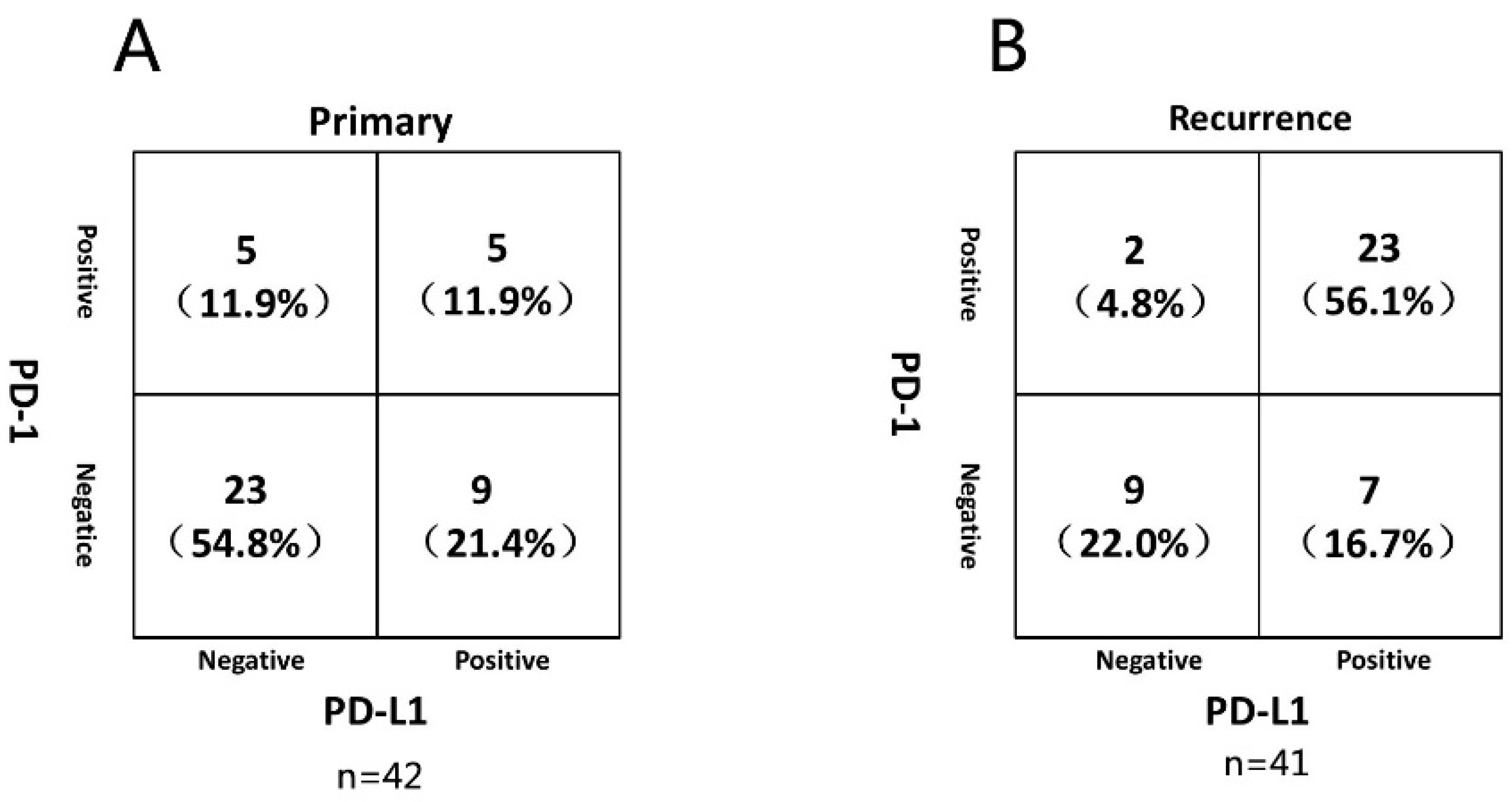
3.4. Correlation between PD-1/PD-L1 Expression
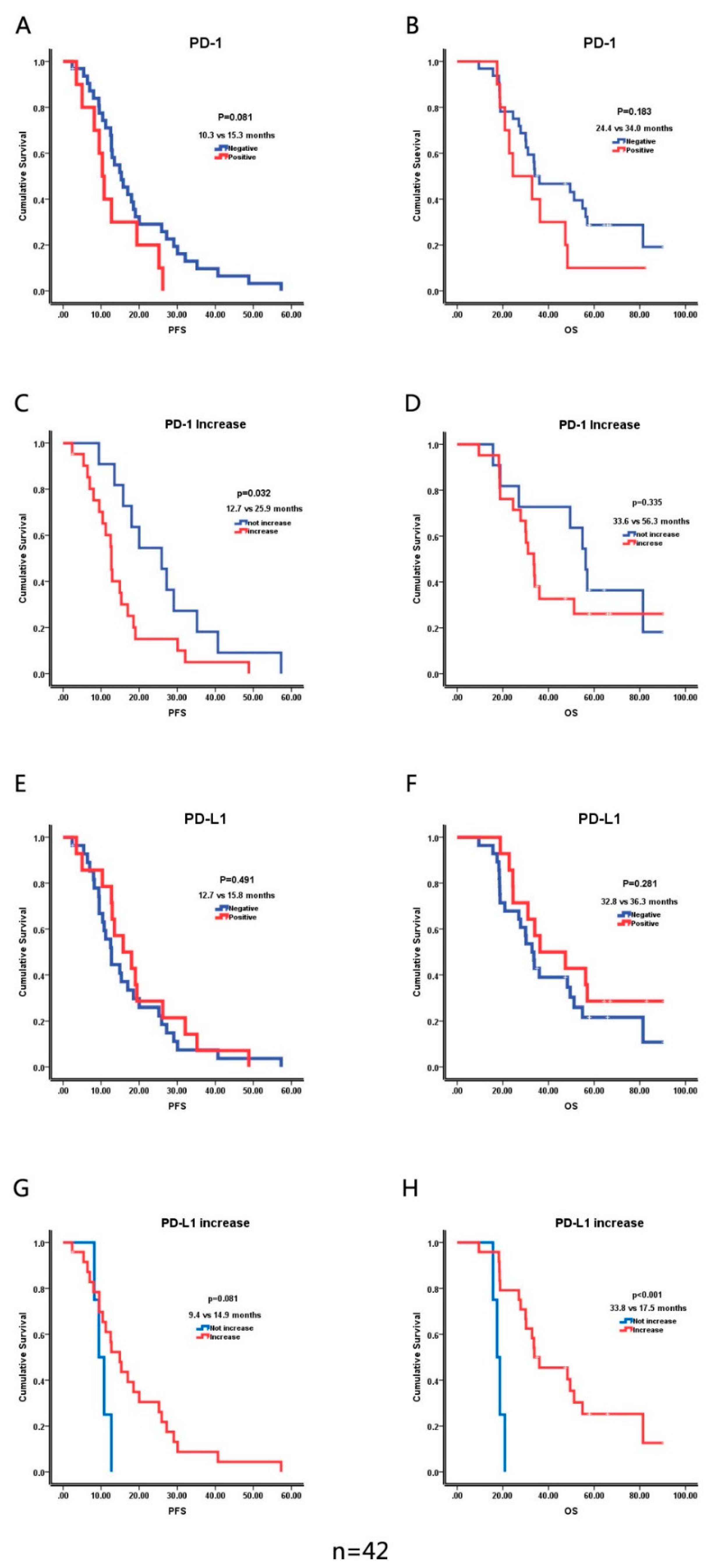
3.5. The Prognostic Value of PD-1 and PD-L1
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kent, W.J. BLAT--the BLAST-like alignment tool. Genome Res. 2002, 12, 656–664. [Google Scholar] [PubMed] [Green Version]
- Pruitt, K.D.; Tatusova, T.; Maglott, D.R. NCBI Reference Sequence (RefSeq): A curated non-redundant sequence database of genomes, transcripts and proteins. Nucleic Acids Res. 2005, 33, D501–D504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Guo, G.; Guan, H.; Yu, Y.; Lu, J.; Yu, J. Challenges and potential of PD-1/PD-L1 checkpoint blockade immunotherapy for glioblastoma. J. Exp. Clin. Cancer Res. 2019, 38, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Caccese, M.; Indraccolo, S.; Zagonel, V.; Lombardi, G. PD-1/PD-L1 immune-checkpoint inhibitors in glioblastoma: A concise review. Crit. Rev. Oncol. Hematol. 2019, 135, 128–134. [Google Scholar] [CrossRef]
- Litak, J.; Mazurek, M.; Grochowski, C.; Kamieniak, P.; Rolinski, J. PD-L1/PD-1 Axis in Glioblastoma Multiforme. Int. J. Mol. Sci 2019, 20, 5347. [Google Scholar] [CrossRef] [Green Version]
- Tatter, S.B. Recurrent malignant glioma in adults. Curr. Treat. Options Oncol. 2002, 3, 509–524. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.A.; Reed, K.; et al. Nivolumab plus ipilimumab in advanced melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef]
- Goldman, J.W.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Ozguroglu, M.; Ji, J.H.; et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): Updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 51–65. [Google Scholar] [CrossRef]
- Waterhouse, D.M.; Garon, E.B.; Chandler, J.; McCleod, M.; Hussein, M.; Jotte, R.; Horn, L.; Daniel, D.B.; Keogh, G.; Creelan, B.; et al. Continuous Versus 1-Year Fixed-Duration Nivolumab in Previously Treated Advanced Non-Small-Cell Lung Cancer: CheckMate 153. J. Clin. Oncol. 2020, 38, 3863–3873. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.F.; Idema, A.J.; Bol, K.F.; Nierkens, S.; Grauer, O.M.; Wesseling, P.; Grotenhuis, J.A.; Hoogerbrugge, P.M.; de Vries, I.J.; Adema, G.J. Regulatory T cells and the PD-L1/PD-1 pathway mediate immune suppression in malignant human brain tumors. Neuro-Oncology 2009, 11, 394–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, G.P.; Dunn, I.F.; Curry, W.T. Focus on TILs: Pro.ognostic significance of tumor infiltrating lymphocytes in human glioma. Cancer Immun. 2007, 7, 12. [Google Scholar] [PubMed]
- Croci, D.O.; Zacarias Fluck, M.F.; Rico, M.J.; Matar, P.; Rabinovich, G.A.; Scharovsky, O.G. Dynamic cross-talk between tumor and immune cells in orchestrating the immunosuppressive network at the tumor microenvironment. Cancer Immunol. Immunother. 2007, 56, 1687–1700. [Google Scholar] [CrossRef] [PubMed]
- Blank, C.; Gajewski, T.F.; Mackensen, A. Interaction of PD-L1 on tumor cells with PD-1 on tumor-specific T cells as a mechanism of immune evasion: Implications for tumor immunotherapy. Cancer Immunol. Immunother. 2005, 54, 307–314. [Google Scholar] [CrossRef]
- Freeman, G.J.; Long, A.J.; Iwai, Y.; Bourque, K.; Chernova, T.; Nishimura, H.; Fitz, L.J.; Malenkovich, N.; Okazaki, T.; Byrne, M.C.; et al. Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J. Exp. Med. 2000, 192, 1027–1034. [Google Scholar] [CrossRef] [Green Version]
- Martner, A.; Thoren, F.B.; Aurelius, J.; Hellstrand, K. Immunotherapeutic strategies for relapse control in acute myeloid leukemia. Blood Rev. 2013, 27, 209–216. [Google Scholar] [CrossRef]
- Bekiaris, V.; Sedy, J.R.; Macauley, M.G.; Rhode-Kurnow, A.; Ware, C.F. The inhibitory receptor BTLA controls gammadelta T cell homeostasis and inflammatory responses. Immunity 2013, 39, 1082–1094. [Google Scholar] [CrossRef] [Green Version]
- Hebeisen, M.; Baitsch, L.; Presotto, D.; Baumgaertner, P.; Romero, P.; Michielin, O.; Speiser, D.E.; Rufer, N. SHP-1 phosphatase activity counteracts increased T cell receptor affinity. J. Clin. Investig. 2013, 123, 1044–1056. [Google Scholar] [CrossRef]
- Taube, J.M.; Klein, A.; Brahmer, J.R.; Xu, H.; Pan, X.; Kim, J.H.; Chen, L.; Pardoll, D.M.; Topalian, S.L.; Anders, R.A. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin. Cancer Res. 2014, 20, 5064–5074. [Google Scholar] [CrossRef] [Green Version]
- Bloch, O.; Crane, C.A.; Kaur, R.; Safaee, M.; Rutkowski, M.J.; Parsa, A.T. Gliomas promote immunosuppression through induction of B7-H1 expression in tumor-associated macrophages. Clin. Cancer Res. 2013, 19, 3165–3175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Carlsson, R.; Ambjorn, M.; Hasan, M.; Badn, W.; Darabi, A.; Siesjo, P.; Issazadeh-Navikas, S. PD-L1 expression by neurons nearby tumors indicates better prognosis in glioblastoma patients. J. Neurosci. 2013, 33, 14231–14245. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.; See, A.P.; Phallen, J.; Jackson, C.M.; Belcaid, Z.; Ruzevick, J.; Durham, N.; Meyer, C.; Harris, T.J.; Albesiano, E.; et al. Anti-PD-1 blockade and stereotactic radiation produce long-term survival in mice with intracranial gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, S.T.; Hashimoto, Y.; Weathers, S.P.; Xiu, J.; Gatalica, Z.; Verhaak, R.G.; Zhou, S.; Fuller, G.N.; Khasraw, M.; de Groot, J.; et al. Immune checkpoint blockade as a potential therapeutic target: Surveying CNS malignancies. Neuro-Oncology 2016, 18, 1357–1366. [Google Scholar] [CrossRef] [Green Version]
- Gatalica, Z.; Snyder, C.; Maney, T.; Ghazalpour, A.; Holterman, D.A.; Xiao, N.; Overberg, P.; Rose, I.; Basu, G.D.; Vranic, S.; et al. Programmed cell death 1 (PD-1) and its ligand (PD-L1) in common cancers and their correlation with molecular cancer type. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 2965–2970. [Google Scholar] [CrossRef] [Green Version]
- Berghoff, A.S.; Kiesel, B.; Widhalm, G.; Rajky, O.; Ricken, G.; Wohrer, A.; Dieckmann, K.; Filipits, M.; Brandstetter, A.; Weller, M.; et al. Programmed death ligand 1 expression and tumor-infiltrating lymphocytes in glioblastoma. Neuro-Oncology 2015, 17, 1064–1075. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.; Kresak, J.; Yang, C.; Huang, J.; Hiser, W.; Kubilis, P.; Mitchell, D. Analysis of immunobiologic markers in primary and recurrent glioblastoma. J. Neurooncol. 2018, 137, 249–257. [Google Scholar] [CrossRef]
- Nduom, E.K.; Wei, J.; Yaghi, N.K.; Huang, N.; Kong, L.Y.; Gabrusiewicz, K.; Ling, X.; Zhou, S.; Ivan, C.; Chen, J.Q.; et al. PD-L1 expression and prognostic impact in glioblastoma. Neuro-Oncology 2016, 18, 195–205. [Google Scholar] [CrossRef] [Green Version]
- Hao, C.; Chen, G.; Zhao, H.; Li, Y.; Chen, J.; Zhang, H.; Li, S.; Zhao, Y.; Chen, F.; Li, W.; et al. PD-L1 Expression in Glioblastoma, the Clinical and Prognostic Significance: A Systematic Literature Review and Meta-Analysis. Front. Oncol. 2020, 10, 1015. [Google Scholar] [CrossRef]
- Hirano, F.; Kaneko, K.; Tamura, H.; Dong, H.; Wang, S.; Ichikawa, M.; Rietz, C.; Flies, D.B.; Lau, J.S.; Zhu, G.; et al. Blockade of B7-H1 and PD-1 by monoclonal antibodies potentiates cancer therapeutic immunity. Cancer Res. 2005, 65, 1089–1096. [Google Scholar]
- Wainwright, D.A.; Chang, A.L.; Dey, M.; Balyasnikova, I.V.; Kim, C.K.; Tobias, A.; Cheng, Y.; Kim, J.W.; Qiao, J.; Zhang, L.; et al. Durable therapeutic efficacy utilizing combinatorial blockade against IDO, CTLA-4, and PD-L1 in mice with brain tumors. Clin. Cancer Res. 2014, 20, 5290–5301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filley, A.C.; Henriquez, M.; Dey, M. Recurrent glioma clinical trial, CheckMate-143: The game is not over yet. Oncotarget 2017, 8, 91779–91794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, E.; Mao, T.; Dong, H.; Boisserand, L.S.B.; Antila, S.; Bosenberg, M.; Alitalo, K.; Thomas, J.L.; Iwasaki, A. VEGF-C-driven lymphatic drainage enables immunosurveillance of brain tumours. Nature 2020, 577, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Campian, J.; Butt, O.; Ghinaseddin, A.; Rahman, M.; Chheda, M.; Johanns, T.; Ansstas, G.; Huang, J.; Liu, J.; Talcott, G.; et al. CTIM-26. PHASE I/II STUDY OF THE COMBINATION OF PEMBROLIZUMAB (MK-3475) AND LASER INTERSTITIAL THERMAL THERAPY (LITT) IN RECURRENT GLIOBLASTOMA. Neuro-Oncology 2021, 23, vi56. [Google Scholar] [CrossRef]
- Hwang, H.; Huang, J.; Khaddour, K.; Butt, O.H.; Ansstas, G.; Chen, J.; Katumba, R.G.; Kim, A.H.; Leuthardt, E.C.; Campian, J.L. Prolonged response of recurrent IDH-wild-type glioblastoma to laser interstitial thermal therapy with pembrolizumab. CNS Oncol. 2022, CNS81. [Google Scholar] [CrossRef] [PubMed]
- Pembrolizumab and Reirradiation in Bevacizumab Naïve and Bevacizumab Resistant Recurrent Glioblastoma. Available online: https://clinicaltrials.gov/ct2/show/NCT03661723?term=NCT03661723&draw=2&rank=1 (accessed on 7 September 2018).
- Nivolumab With Radiation Therapy and Bevacizumab for Recurrent MGMT Methylated Glioblastoma. Available online: https://clinicaltrials.gov/ct2/show/NCT03743662?term=NCT03743662&draw=2&rank=1 (accessed on 16 November 2018).
- Pembrolizumab and Standard Therapy in Treating Patients With Glioblastoma. Available online: https://clinicaltrials.gov/ct2/show/NCT03197506?term=NCT03197506&draw=2&rank=1 (accessed on 23 June 2017).
- Trial of Anti-PD-1 Immunotherapy and Stereotactic Radiation in Patients With Recurrent Glioblastoma. Available online: https://clinicaltrials.gov/ct2/show/NCT04977375?term=NCT04977375&draw=2&rank=1 (accessed on 26 July 2021).
- Intra-tumoral Ipilimumab Plus Intravenous Nivolumab Following the Resection of Recurrent Glioblastoma (GlitIpNi). Available online: https://clinicaltrials.gov/ct2/show/NCT03233152?term=NCT03233152&draw=2&rank=1 (accessed on 28 July 2017).
- Fenstermaker, R.A.; Ciesielski, M.J. Challenges in the development of a survivin vaccine (SurVaxM) for malignant glioma. Expert Rev. Vaccines 2014, 13, 377–385. [Google Scholar] [CrossRef]
- Schalper, K.A.; Rodriguez-Ruiz, M.E.; Diez-Valle, R.; Lopez-Janeiro, A.; Porciuncula, A.; Idoate, M.A.; Inoges, S.; de Andrea, C.; Lopez-Diaz de Cerio, A.; Tejada, S.; et al. Neoadjuvant nivolumab modifies the tumor immune microenvironment in resectable glioblastoma. Nat. Med. 2019, 25, 470–476. [Google Scholar] [CrossRef]
- Cloughesy, T.F.; Mochizuki, A.Y.; Orpilla, J.R.; Hugo, W.; Lee, A.H.; Davidson, T.B.; Wang, A.C.; Ellingson, B.M.; Rytlewski, J.A.; Sanders, C.M.; et al. Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma. Nat. Med. 2019, 25, 477–486. [Google Scholar] [CrossRef]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Primary (n = 42) | Recurrence (n = 42) |
|---|---|---|
| Age(year) | ||
| Mean (range) | 43.2 (11–61) | 44.9 (12–64) |
| Sex | ||
| Male | 27 | 27 |
| Female | 15 | 15 |
| Tumor location—side | ||
| Left | 22 | 19 |
| Right | 20 | 22 |
| Middle | 0 | 1 |
| Pathological Type | ||
| Pilocytic astrocytoma | 2 | 1 |
| Astrocytoma, IDH1-mutant | 8 | 9 |
| Astrocytoma, IDH1-wildtype | 15 | 10 |
| Oligodendroglioma, NOS | 3 | 4 |
| Glioblastoma, IDH1-wildtype | 12 | 18 |
| Ganglioglioma | 1 | 0 |
| Pleomorphic xanthoastrocytoma | 1 | 0 |
| IDH1 status | 9 (mutant)/33 (wildtype) | 11 (mutant)/31 (wildtype) |
| WHO grade | ||
| 1 | 2 | 1 |
| 2 | 16 | 7 |
| 3 | 12 | 11 |
| 4 | 12 | 23 |
| Residual after first surgery | ||
| Yes | 21 | 31 |
| No | 21 | 11 |
| Adjuvant therapy after first surgery | ||
| Radiotherapy alone | 6 | 1 |
| Chemotherapy alone | 1 | 8 |
| chemoradiotherapy | 15 | 9 |
| No adjuvant therapy | 20 | 24 |
| Type of recurrence | ||
| Recurrence in situ | 38 | |
| Distant relapse in the brain | 4 | |
| Median PFS (month) | 13.5 | |
| Median OS (month) | 33.8 | 14.1 |
| Group (n) | Primary (%) | Recurrence (%) | ||||
|---|---|---|---|---|---|---|
| Positive | Negative | Positive | Negative | p | ||
| PD-1 | No adjuvant therapy (20) | 3 | 17 | 10 | 10 | p < 0.05 |
| Adjuvant therapy (21) | 6 | 15 | 15 | 6 | 0.05 < p < 0.1 | |
| PD-L1 | No adjuvant therapy (20) | 8 | 12 | 13 | 7 | p > 0.25 |
| Adjuvant therapy (22) | 6 | 16 | 18 | 4 | p < 0.005 | |
| Characteristics | PD-1 Negative (n = 32) | PD-1 Positive (n = 10) | p-Value |
|---|---|---|---|
| Age(year) | |||
| Mean (range) | 43 (11–61) | 44 (12–61) | 0.887 |
| Sex | |||
| Male | 20 | 7 | - |
| Female | 12 | 3 | 1.000 |
| WHO grade | |||
| 1 | 2 | 0 | - |
| 2 | 13 | 3 | - |
| 3 | 10 | 2 | - |
| 4 | 7 | 5 | 0.135 |
| IDH1 status | 9 (mutant)/23 (wildtype) | 10 (wildtype) | 0.086 |
| Resection type | |||
| Total gross resection | 15 | 6 | - |
| Subtotal resection | 17 | 4 | 0.719 |
| Adjuvant therapy after first surgery | |||
| Yes | 15 | 7 | - |
| No | 17 | 3 | 0.284 |
| Type of recurrence | |||
| Local recurrence | 30 | 8 | - |
| Distant recurrence | 2 | 2 | 0.236 |
| Median PFS (month) | 15.3 | 10.3 | 0.081 |
| Median OS (month) | 34.0 | 24.4 | 0.183 |
| Characteristics | PD-L1 Negative (n = 28) | PD-L1 Positive (n = 14) | p-Value |
|---|---|---|---|
| Age(year) | |||
| Mean (range) | 46 (11–61) | 38 (12–52) | 0.073 |
| Sex | |||
| Male | 17 | 10 | - |
| Female | 11 | 4 | 0.734 |
| WHO grade | |||
| 1 | 2 | 0 | - |
| 2 | 11 | 5 | - |
| 3 | 7 | 5 | - |
| 4 | 8 | 4 | 0.573 |
| IDH1 status | 7 (mutant)/21 (wildtype) | 2 (mutant)/12 (wildtype) | 0.692 |
| Resection type | |||
| Total gross resection | 16 | 5 | - |
| Subtotal resection | 12 | 9 | 0.326 |
| Adjuvant therapy after first surgery | |||
| Yes | 16 | 6 | - |
| No | 12 | 8 | 0.515 |
| Type of recurrence | |||
| Local recurrence | 25 | 13 | - |
| Distant recurrence | 3 | 1 | 1.000 |
| Median PFS (month) | 12.7 | 15.8 | 0.491 |
| Median OS (month) | 32.8 | 36.3 | 0.284 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, W.; Shao, A.; Ren, X.; Chen, Z.; Xu, J.; Wei, Q. Comparison of Immune Checkpoint Molecules PD-1 and PD-L1 in Paired Primary and Recurrent Glioma: Increasing Trend When Recurrence. Brain Sci. 2022, 12, 266. https://doi.org/10.3390/brainsci12020266
Yu W, Shao A, Ren X, Chen Z, Xu J, Wei Q. Comparison of Immune Checkpoint Molecules PD-1 and PD-L1 in Paired Primary and Recurrent Glioma: Increasing Trend When Recurrence. Brain Sciences. 2022; 12(2):266. https://doi.org/10.3390/brainsci12020266
Chicago/Turabian StyleYu, Wei, Anwen Shao, Xiaoqiu Ren, Zexin Chen, Jinghong Xu, and Qichun Wei. 2022. "Comparison of Immune Checkpoint Molecules PD-1 and PD-L1 in Paired Primary and Recurrent Glioma: Increasing Trend When Recurrence" Brain Sciences 12, no. 2: 266. https://doi.org/10.3390/brainsci12020266
APA StyleYu, W., Shao, A., Ren, X., Chen, Z., Xu, J., & Wei, Q. (2022). Comparison of Immune Checkpoint Molecules PD-1 and PD-L1 in Paired Primary and Recurrent Glioma: Increasing Trend When Recurrence. Brain Sciences, 12(2), 266. https://doi.org/10.3390/brainsci12020266