
Dimensions of Tinnitus-Related Distress

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
- (1)
- Which sociodemographic and psychological items predict tinnitus-related distress at baseline?
- (2)
- Which factors may underlie these items?
2. Materials and Methods
2.1. Sample
2.2. Questionnaires
- (1)
- Tinnitus-related distress was assessed with the German version of the Tinnitus Questionnaire (TQ) [20]. The TQ [21] is an instrument for measuring tinnitus impairment or tinnitus-related distress (total score). The questionnaire contains 40 items with 3 response categories (2 = “agree”, 1 = “partially agree”, 0 = “disagree”) and the total score (TQ) is used as the dependent variable here;
- (2)
- (3)
- (4)
- The General Depression Scale (ADSL [27] contains 20 items measuring depressive symptoms in the last week, which were included in our model. The questionnaire is the German version of the globally used CES-D—Center for Epidemiological Studies Depression Scale [28]. Each item is rated on a 4-point ordinal scale. Clinically, we used the sum score, which indicates manifest depression from a score of 16;
- (5)
- The Self-Efficacy-Optimism-Pessimism Scale (SWOP [28]) contains 9 items that are rated on a scale from 1 = “agree exactly” to 4 = “disagree”. The 9 individual items were used in the calculation;
- (6)
- The Berlin Mood Questionnaire (BSF [29]) calculates a multidimensional mood model consisting of 30 items with 5 response options: 0 = “not at all”, 1 = “somewhat”, 2 = “quite”, 3 = “mostly”, and 4 = “total”;
- (7)
- The Berlin Complaint Inventory (BI [30]) contains 57 items from the fields of fatigue, upper abdominal symptoms, limb pain, heart problems, and a sum score for total complaint pressure. Responses are on a 5-point ordinal scale with 0 = “not at all”, 1 = “hardly”, 2 = “to some extent”, 3 = “considerably” to 4 = “strongly”. Responses to the 57 individual items were included in the calculation;
- (8)
- The Pain Perception Scale (SES [31]) results in sum scores for affective and sensory pain from 24 items with the 4 response options from 1 = “does not apply” to 4 = “applies exactly”. All 24 items were included in our analysis.
2.3. Statistics
3. Results
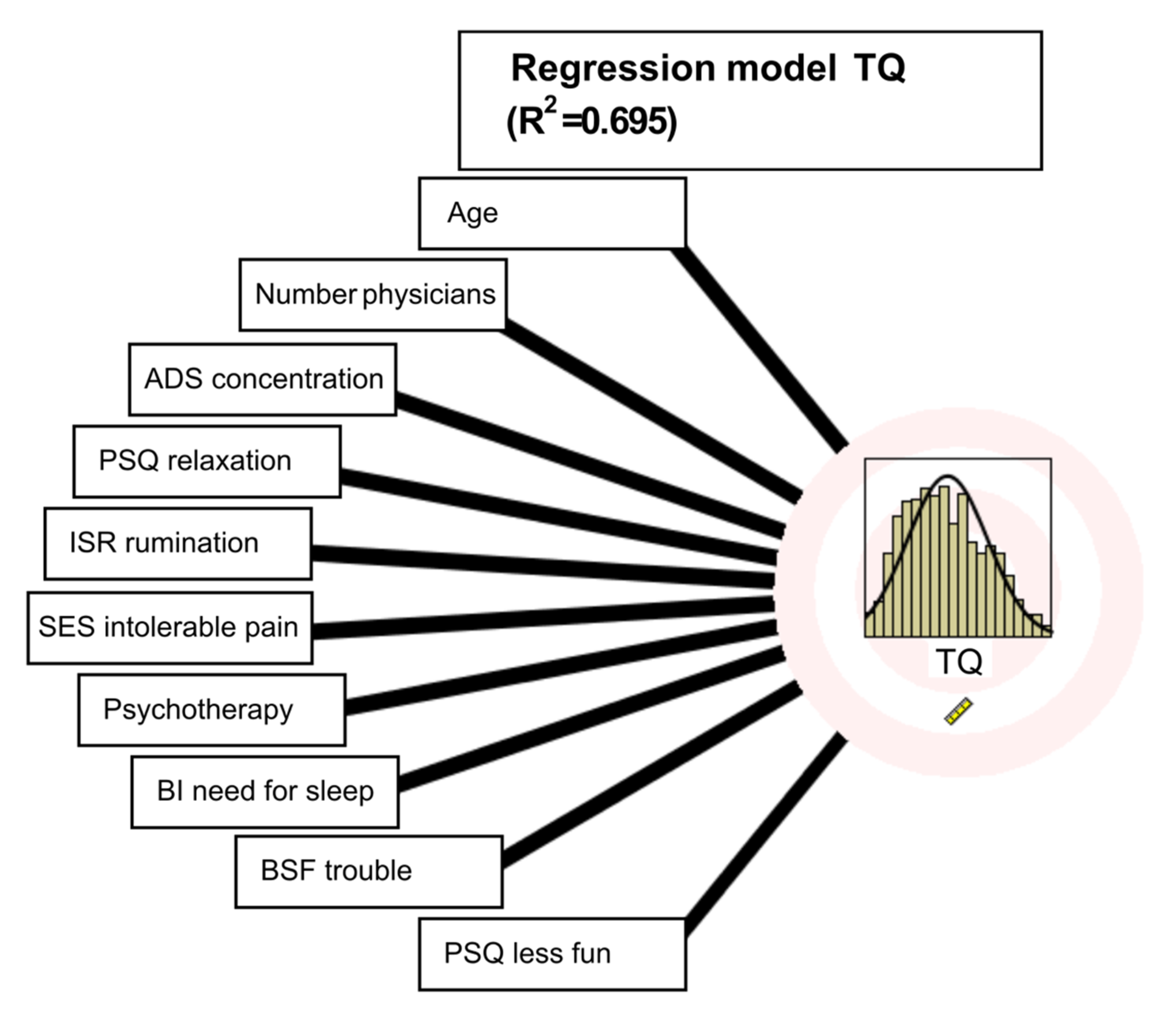
3.1. Predictors of Tinnitus-Related Distress/Regression Model
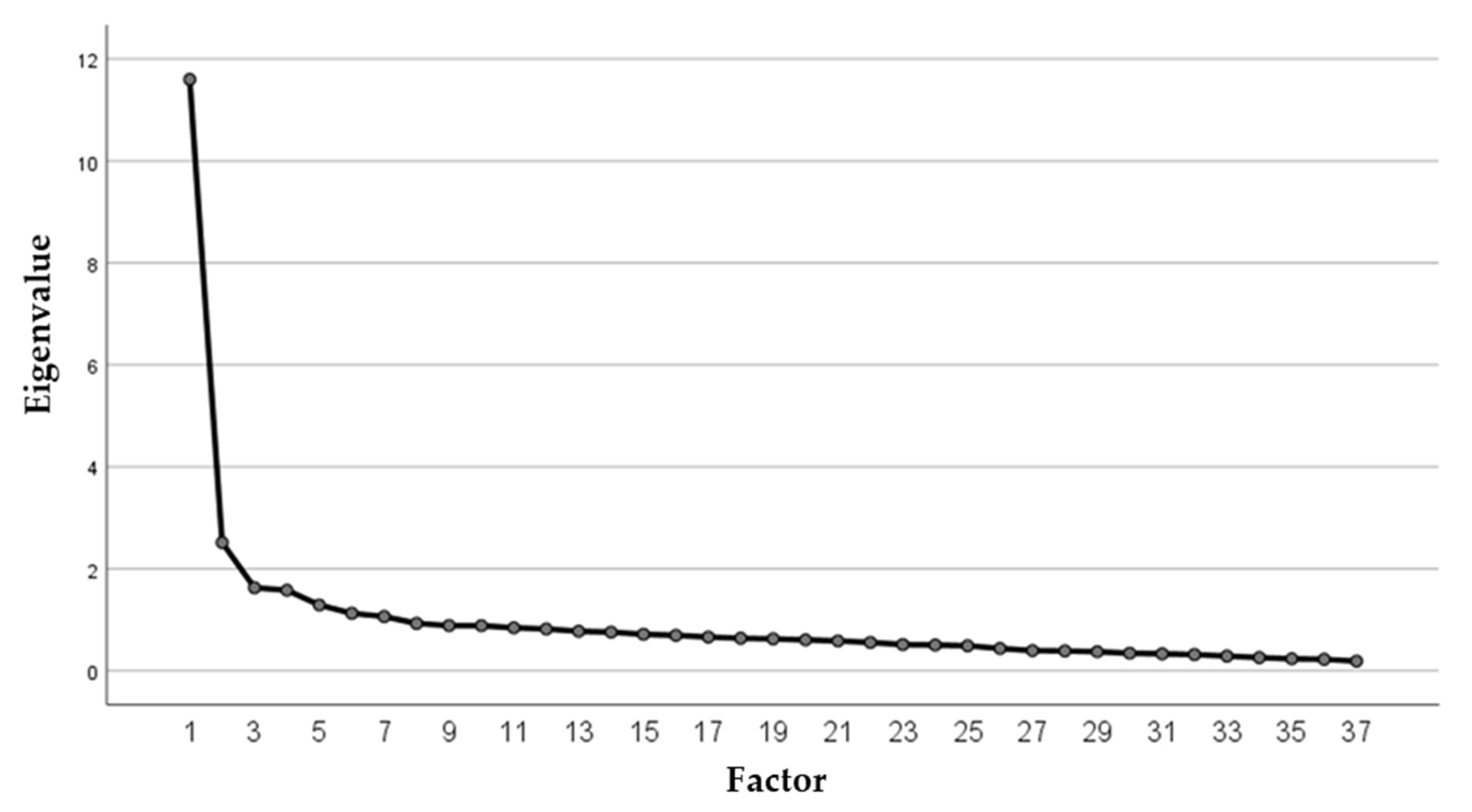
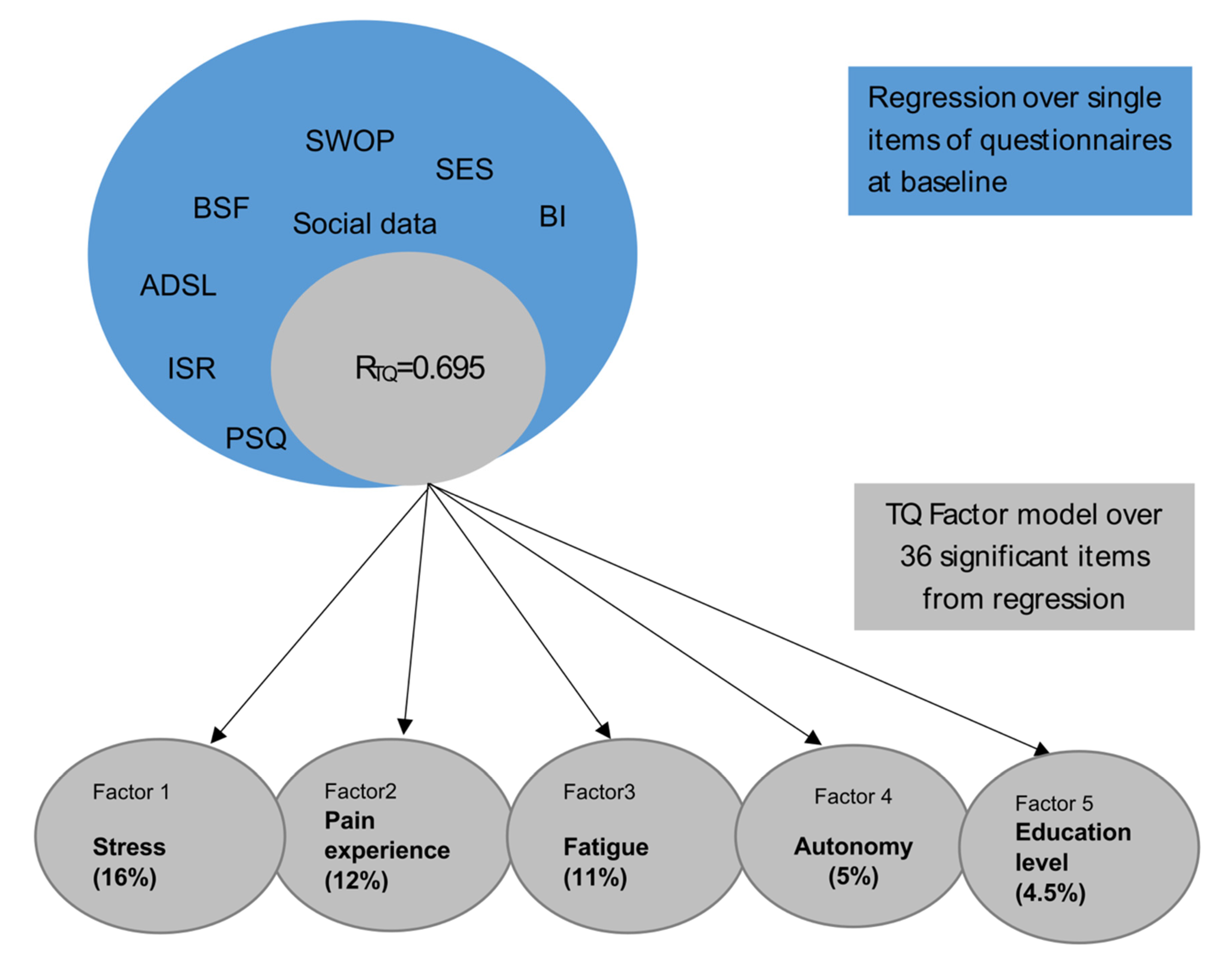
3.2. Dimensional Reduction for Tinnitus-Related Distress via Factorization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zenner, H.P.; Delb, W.; Kroner-Herwig, B.; Jager, B.; Peroz, I.; Hesse, G.; Mazurek, B.; Goebel, G.; Gerloff, C.; Trollmann, R.; et al. On the interdisciplinary S3 guidelines for the treatment of chronic idiopathic tinnitus. Hno 2015, 63, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Zenner, H.P.; Delb, W.; Kroner-Herwig, B.; Jager, B.; Peroz, I.; Hesse, G.; Mazurek, B.; Goebel, G.; Gerloff, C.; Trollmann, R.; et al. A multidisciplinary systematic review of the treatment for chronic idiopathic tinnitus. Eur. Ann. Otorhinolaryngol. 2017, 274, 2079–2091. [Google Scholar] [CrossRef]
- Ivansic, D.; Besteher, B.; Gantner, J.; Guntinas-Lichius, O.; Pantev, C.; Nenadic, I.; Dobel, C. Psychometric assessment of mental health in tinnitus patients, depressive and healthy controls. Psychiat. Res. 2019, 281, 112582. [Google Scholar] [CrossRef] [PubMed]
- Martinez, C.; Wallenhorst, C.; McFerran, D.; Hall, D.A. Incidence Rates of Clinically Significant Tinnitus: 10-Year Trend From a Cohort Study in England. Ear Hearing 2015, 36, E69–E75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cima, R.F.F.; Mazurek, B.; Haider, H.; Kikidis, D.; Lapira, A.; Norena, A.; Hoare, D.J. Amultidisciplinary European guideline for tinnitus: Diagnostics, assessment, and treatment. Hno 2019, 67, S10–S42. [Google Scholar] [CrossRef] [Green Version]
- Jastreboff, P.J. Phantom Auditory-Perception (Tinnitus)—Mechanisms of Generation and Perception. Neurosci. Res. 1990, 8, 221–254. [Google Scholar] [CrossRef]
- Hoare, D.J.; Kowalkowski, V.L.; Kang, S.J.; Hall, D.A. Systematic Review and Meta-Analyses of Randomized Controlled Trials Examining Tinnitus Management. Laryngoscope 2011, 121, 1555–1564. [Google Scholar] [CrossRef] [Green Version]
- Hebert, S.; Canlon, B.; Hasson, D.; Hanson, L.L.M.; Westerlund, H.; Theorell, T. Tinnitus Severity Is Reduced with Reduction of Depressive Mood—A Prospective Population Study in Sweden. PLoS ONE 2012, 7, e37733. [Google Scholar] [CrossRef] [Green Version]
- Goebel, G. Tinnitus and psychiatric comorbidities. Hno 2015, 63, 272–282. [Google Scholar] [CrossRef]
- Moller, A.R. Sensorineural Tinnitus: Its Pathology and Probable Therapies. Int. J. Otolaryngol. 2016, 2016, 2830157. [Google Scholar] [CrossRef] [Green Version]
- Husain, F.T.; Akrofi, K.; Carpenter-Thompson, J.R.; Schmidt, S.A. Alterations to the attention system in adults with tinnitus are modality specific. Brain Res. 2015, 1620, 81–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazurek, B.; Szczepek, A.J.; Hebert, S. Stress and tinnitus. Hno 2015, 63, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Brueggemann, P.; Neff, P.K.A.; Meyer, M.; Riemer, N.; Rose, M.; Mazurek, B. On the relationship between tinnitus distress, cognitive performance and aging. Prog. Brain Res. 2021, 262, 263–285. [Google Scholar] [PubMed]
- Seydel, C.; Haupt, H.; Szczepek, A.J.; Hartmann, A.; Rose, M.; Mazurek, B. Three years later: Report on the state of well-being of patients with chronic tinnitus who underwent modified tinnitus retraining therapy. Audiol. Neurotol. 2015, 20, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Bruggemann, P.; Otto, J.; Lorenz, N.; Schorsch, S.; Szczepek, A.J.; Bocking, B.; Mazurek, B. Long-term changes in multimodal intensive tinnitus therapy: A 5 year follow-up. Hno 2018, 66 (Suppl. S1), 34–38. [Google Scholar] [CrossRef] [PubMed]
- Brüggemann, P.; Szczepek, A.J.; Rose, M.; McKenna, L.; Olze, H.; Mazurek, B. Impact of multiple factors on the degree of tinnitus distress. Front. Hum. Neurosci. 2016, 10, 341. [Google Scholar] [CrossRef] [Green Version]
- Niemann, U.; Brueggemann, P.; Boecking, B.; Mazurek, B.; Spiliopoulou, M. Development and internal validation of a depression severity prediction model for tinnitus patients based on questionnaire responses and socio-demographics. Sci. Rep. 2020, 10, 4664. [Google Scholar] [CrossRef]
- Niemann, U.; Brueggemann, P.; Boecking, B.; Mebus, W.; Rose, M.; Spiliopoulou, M.; Mazurek, B. Phenotyping chronic tinnitus patients using self-report questionnaire data: Cluster analysis and visual comparison. Sci. Rep. 2020, 10, 16411. [Google Scholar] [CrossRef]
- Niemann, U.; Boecking, B.; Brueggemann, P.; Mebus, W.; Mazurek, B.; Spiliopoulou, M. Tinnitus-related distress after multimodal treatment can be characterized using a key subset of baseline variables. PLoS ONE 2020, 15, e0228037. [Google Scholar] [CrossRef] [Green Version]
- Goebel, G.; Hiller, W. The tinnitus questionnaire. A standard instrument for grading the degree of tinnitus. Results of a multicenter study with the tinnitus questionnaire. Hno 1994, 42, 166–172. [Google Scholar]
- Hallam, R.S.; Jakes, S.C.; Hinchcliffe, R. Cognitive variables in tinnitus annoyance. Br. J. Clin. Psychol. 1988, 27 Pt 3, 213–222. [Google Scholar] [CrossRef]
- Levenstein, S.; Prantera, C.; Varvo, V.; Scribano, M.L.; Berto, E.; Luzi, C.; Andreoli, A. Development of the Perceived Stress Questionnaire—A New Tool for Psychosomatic Research. J. Psychosom. Res. 1993, 37, 19–32. [Google Scholar] [CrossRef]
- Fliege, H.; Rose, M.; Arck, P.; Levenstein, S.; Klapp, B.F. Validation of the “Perceived Stress Questionnaire” (PSQ) in a German sample. Diagnostica 2001, 47, 142–152. [Google Scholar] [CrossRef]
- Fliege, H.; Rose, M.; Arck, P.; Walter, O.B.; Kocalevent, R.D.; Weber, C.; Klapp, B.F. The Perceived Stress Questionnaire (PSQ) reconsidered: Validation and reference values from different clinical and healthy adult samples. Psychosom. Med. 2005, 67, 78–88. [Google Scholar] [CrossRef]
- Tritt, K.; von Heymann, F.; Zaudig, M.; Zacharias, I.; Sollner, W.; Loew, T. Development of the “ICD-10-Symptom-Rating” (ISR) Questionnaire. Z. Psychosom. Med. Psychother. 2008, 54, 409–418. [Google Scholar]
- Fischer, H.F.; Schirmer, N.; Tritt, K.; Klapp, B.F.; Fliege, H. Retest-Reliability and Sertsitivity to Change of the ICD-10-Symptom-Rating (ISR) in Different Samples. Psychother. Psychosom. Med. Psychol. 2011, 61, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Hautzinger, M.; Welz, S. Short- and long-term efficacy of psychological intervention for depression in older adults. Z. Klin. Psychol. Psychother. 2008, 37, 52–60. [Google Scholar] [CrossRef]
- Scholler, G.; Fliege, H.; Klapp, B.F. Questionnaire for self-efficacy optimism and pessimism: Reconstruction, selection of items, and validation of an instrument by means of examinations of clinical samples. Psychother. Psychosom. Med. Psychol. 1999, 49, 275–283. [Google Scholar]
- Horhold, M.; Bolduan, D.; Klapp, C.; Volger, H.; Scholler, G.; Klapp, B. Testing a screening strategy for identifying psychosomatic patients in gynecologic practice. Psychother. Psychosom. Med. Psychol. 1997, 47, 156–162. [Google Scholar]
- Brahler, E.; Scheer, J.W. Scaling of psychosomatic by means of the Giessen inventory (GBB) (author’s transl). Psychother. Med. Psychol. 1979, 29, 14–27. [Google Scholar]
- Geissner, E. The Pain Perception Scale--a differentiated and change-sensitive scale for assessing chronic and acute pain. Rehabilitation 1995, 34, 35–43. [Google Scholar]
- Holgers, K.M.; Erlandsson, S.I.; Barrenas, M.L. Predictive factors for the severity of tinnitus. Audiology 2000, 39, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, B.; Boecking, B.; Brueggemann, P. Association Between Stress and Tinnitus-New Aspects. Otol. Neurotol. 2019, 40, e467–e473. [Google Scholar] [CrossRef] [PubMed]
- Boecking, B.; von Sass, J.; Sieveking, A.; Schaefer, C.; Brueggemann, P.; Rose, M.; Mazurek, B. Tinnitus-related distress and pain perceptions in patients with chronic tinnitus—Do psychological factors constitute a link? PLoS ONE 2020, 15, e0234807. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables/Sociodemographic Information | Mean (st.dev.)/Percent |
|---|---|
| Sex | women: 50% |
| Age | 49.4 (11.8) |
| Partnership | yes: 72% |
| Graduation | low: 11% middle: 39% high: 49% |
| Employment Duration of tinnitus Number of physicians consulted | yes: 74.7% 2.7 years (1.9) 2.95 (1.6) |
| Variables | Mean (st.dev.) |
| Total TQ: tinnitus-related distress Emotional distress Cognitive distress Psychological distress Intrusiveness Auditory perceptual difficulties Sleep disturbances Somatic complaints | 35.2 (17.2) 9.5 (5.6) 5.9 (4.1) 15.4 (9.3) 9.6 (3.8) 4.8 (3.6) 3.3 (2.5) 2.1 (1.9) |
| PSQ-20 total: perceived stress Worries Tension Joy Demand | 44.8 (18.3) 27.7 (22.7) 55.9 (22.6) 49.5 (23.2) 48.8 (22.2) |
| SWOP Self-efficacy Optimism Pessimism | 28.0 (5.8) 27.7 (7.6) 21.2 (7.2) |
| ADSL total depression | 15.6 (11.3) |
| BSF berlin mood questionnaire Elevated mood Positive mindset Anger Anxious depression Fatigue Apathy BI Berlin complaint inventory Overall complaints Fatigue Abdominal symptoms Limb pain Heart symptoms | 1.6 (1.0) 2.2 (0.77) 0.7 (0.71) 1.08 (0.92) 1.49 (1.01) 0.56 (0.67) 22.69 (15.32) 8.53 (5.89) 2.76 (3.39) 8.40 (5.39) 3.00 (3.68) |
| SES pain perception scale Affective pain Sensoric pain | 23.34 (9.86) 13.57 (4.95) |
| ISR ICD-10 Symptom Rating: total score Depression Anxiety Obsessive–compulsive syndrome Somatoform syndrome Eating disorder syndrome Additional items score | 0.78 (0.58) 1.10 (0.92) 0.91 (0.90) 0.79 (0.85) 0.59 (0.78) 0.66 (0.81) 0.71 (0.55) |
| Sociodemographic Items that Significantly Predict TQ | ||
|---|---|---|
| Age | ||
| Number of physicians consulted | ||
| Psychotherapy | ||
| Graduation | ||
| Employment | ||
| Psychological Questionnaire Items that Significantly Predict TQ | ||
| Questionnaire | Item Number | Item Text |
| PSQ | 03 | You feel that too many demands are being made on you. |
| PSQ | 06 | You fear that you will not be able to achieve your goals. |
| PSQ | 20 | You feel discouraged. |
| PSQ | 21 | You are having fun (-). |
| PSQ | 22 | You are afraid of the future |
| PSQ | 26 | You feel mentally exhausted. |
| PSQ | 27 | You have trouble relaxing. |
| PSQ | 29 | You have enough time for yourself (-). |
| SWOP | 03 | I have no trouble achieving my intentions and goals. |
| SWOP | 06 | Things never turn out the way I want them to. |
| ADS | 05 | During the last week, I had trouble concentrating. |
| ADS | 06 | During the last week, I have been depressed. |
| ADS | 11 | During the last week, I slept poorly. |
| ADS | 14 | During the last week, I felt lonely. |
| BSF | 12 | I feel troubled. |
| BSF | 29 | I feel exhausted. |
| ISR | 02 | I no longer really enjoy things that I normally like to do. |
| ISR | 10 | I resist repetitive, nonsensical thoughts or actions, even if I don’t always succeed. |
| ISR | 18 | I have difficulty concentrating. |
| ISR | 20 | I have problems sleeping. |
| ISR | 24 | I have psychological problems due to severe everyday stresses (e.g., serious illness, loss of job, or separation from partner). |
| ISR | 27 | I feel impaired in the exercise of my sexuality. |
| BI | 07 | Excessive need for sleep |
| BI | 10 | Dizziness |
| BI | 27 | Headache |
| SES | 01 | I experience my pain as tortourus. |
| SES | 02 | I experience my pain as horrible. |
| SES | 07 | I experience my pain as dreadful. |
| SES | 09 | I experience my pain as heavy. |
| SES | 13 | I experience my pain as intolerable. |
| SES | 17 | I experience my pain as burning. |
| Component | Initial Eigenvalues | Total% of Variance | Cumulated% |
|---|---|---|---|
| 1 | 11.597 | 31.342 | 31.342 |
| 2 | 2.514 | 6.794 | 38.136 |
| 3 | 1.626 | 4.395 | 42.536 |
| 4 | 1.578 | 4.264 | 46.795 |
| 5 | 1.287 | 3.479 | 50.275 |
| Extraction method: principal component analysis | |||
| Sums of Squared Factor Loadings for Extraction | |||
| Total | % of variance | Cumulated% | |
| 11,597 | 31.342 | 31.342 | |
| 2514 | 6.794 | 38.136 | |
| 1626 | 4.395 | 42.531 | |
| 1578 | 4.264 | 46.795 | |
| 1287 | 3.479 | 50.274 | |
| Rotated sum of squared loadings. | |||
| Total | % of variance | Cumulated% | |
| 6040 | 16.324 | 16.324 | |
| 4565 | 12.338 | 28.662 | |
| 4130 | 11.163 | 39.825 | |
| 1806 | 4.882 | 4.,707 | |
| 1646 | 4.449 | 49.156 | |
| Rotated Component Matrices | |||||
|---|---|---|---|---|---|
| Component | 1 | 2 | 3 | 4 | 5 |
| PSQ 20 | 0.745 | ||||
| PSQ 22 | 0.686 | ||||
| PSQ 21 | −0.679 | ||||
| ISR 02 | 0.634 | 0.361 | |||
| ISR 24 | 0.632 | ||||
| ADSL 06 | 0.622 | 0.417 | |||
| ADSL 14 | 0.609 | ||||
| BSF 12 | 0.595 | 0.390 | |||
| PSQ 06 | 0.574 | 0.332 | |||
| PSQ 26 | 0.559 | 0.463 | |||
| ISR 27 | 0.557 | ||||
| SWOP 06 | 0.513 | ||||
| SWOP 03 | −0.481 | ||||
| PSQ 03 | 0.455 | ||||
| social item 24 (psychotherapy) | 0.429 | ||||
| ISR 10 | 0.323 | ||||
| SES 02 | 0.831 | ||||
| SES 13 | 0.806 | ||||
| SES 09 | 0.799 | ||||
| SES 07 | 0.789 | ||||
| SES 01 | 0.764 | ||||
| SES 17 | 0.584 | ||||
| BI 27 | 0.437 | 0.435 | |||
| ADSL 11 | 0.796 | ||||
| ISR 20 | 0.780 | ||||
| BSF 29 | 0.457 | 0.626 | |||
| BI 07 | 0.573 | ||||
| ADSL 05 | 0.401 | 0.571 | |||
| PSQ 27 | 0.392 | 0.508 | |||
| ISR 18 | 0.464 | 0.505 | |||
| BI 10 | 0.322 | 0.372 | |||
| social item 18 (employment) | 0.648 | ||||
| PSQ 29 | 0.620 | ||||
| social item 10 (profession, foreman) | 0.707 | ||||
| age | −0.505 | 0.515 | |||
| social item 09 (graduation) | 0.483 | ||||
| social item 25 (number of physicians consulted) | −0.379 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brueggemann, P.; Mebus, W.; Boecking, B.; Amarjargal, N.; Niemann, U.; Spiliopoulou, M.; Dobel, C.; Rose, M.; Mazurek, B. Dimensions of Tinnitus-Related Distress. Brain Sci. 2022, 12, 275. https://doi.org/10.3390/brainsci12020275
Brueggemann P, Mebus W, Boecking B, Amarjargal N, Niemann U, Spiliopoulou M, Dobel C, Rose M, Mazurek B. Dimensions of Tinnitus-Related Distress. Brain Sciences. 2022; 12(2):275. https://doi.org/10.3390/brainsci12020275
Chicago/Turabian StyleBrueggemann, Petra, Wilhelm Mebus, Benjamin Boecking, Nyamaa Amarjargal, Uli Niemann, Myra Spiliopoulou, Christian Dobel, Matthias Rose, and Birgit Mazurek. 2022. "Dimensions of Tinnitus-Related Distress" Brain Sciences 12, no. 2: 275. https://doi.org/10.3390/brainsci12020275
APA StyleBrueggemann, P., Mebus, W., Boecking, B., Amarjargal, N., Niemann, U., Spiliopoulou, M., Dobel, C., Rose, M., & Mazurek, B. (2022). Dimensions of Tinnitus-Related Distress. Brain Sciences, 12(2), 275. https://doi.org/10.3390/brainsci12020275